
Perspectives of Molecularly Imprinted Polymer-Based Drug Delivery Systems in Ocular Therapy


 ,
,  ,
,  , and
, and 
Abstract
:
1. Introduction
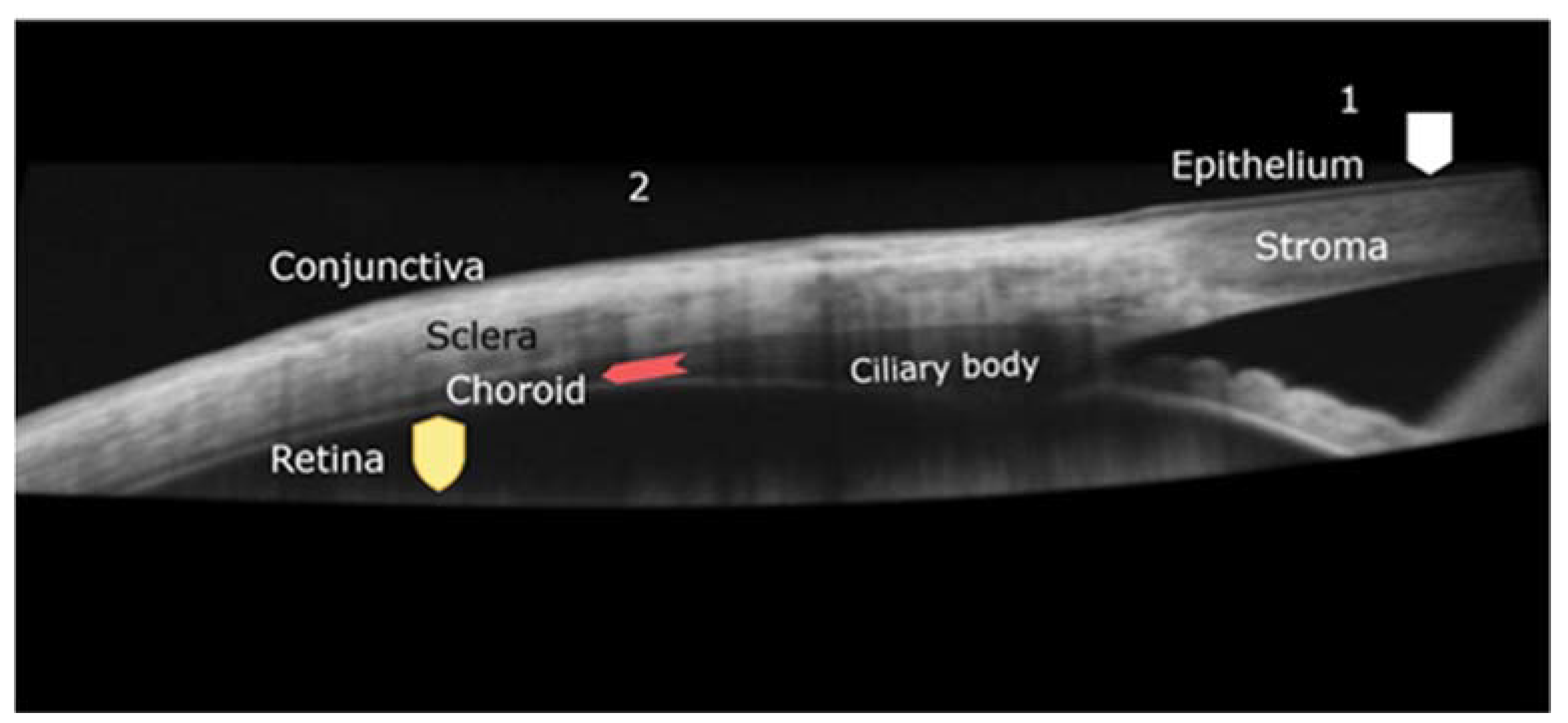
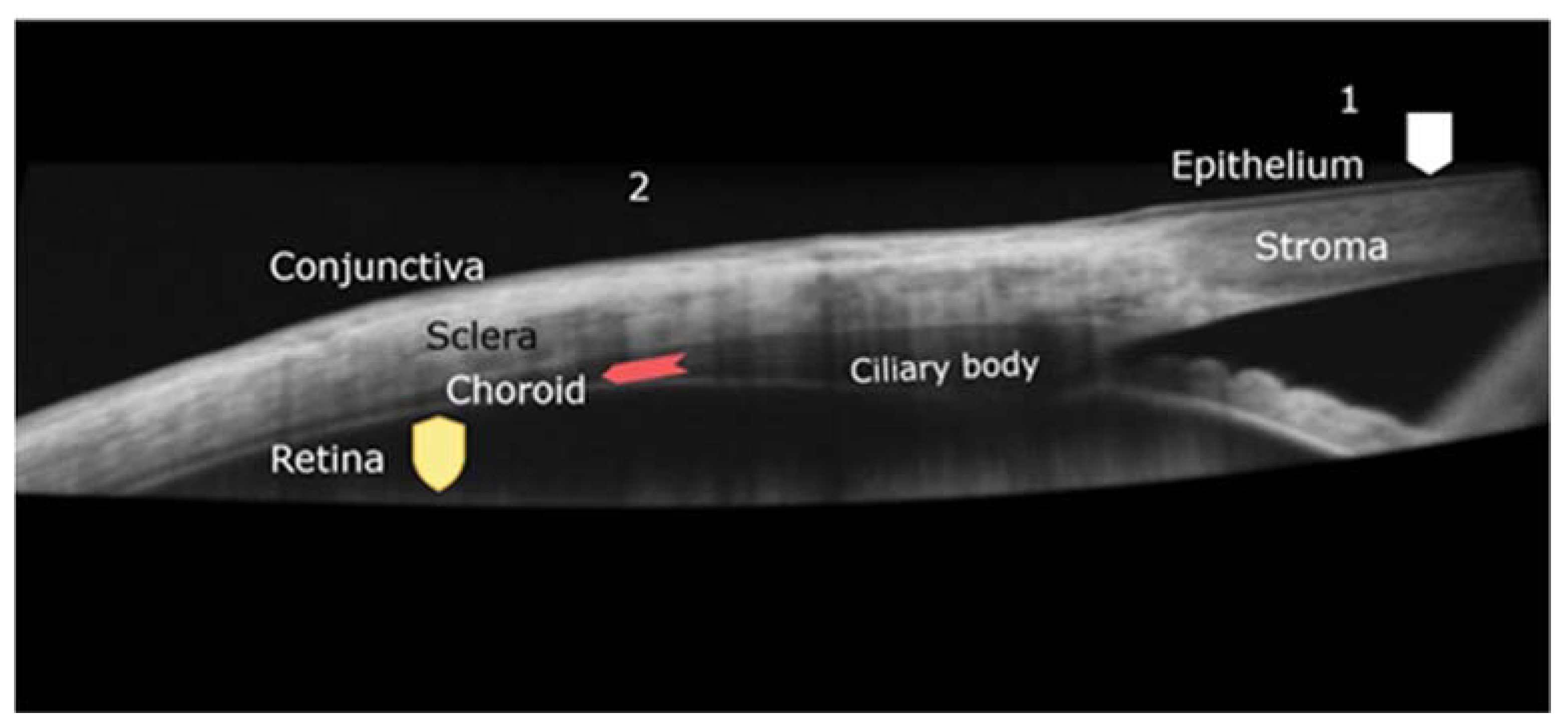
2. Eye’s Structure and Therapeutical Approaches for Its Treatment
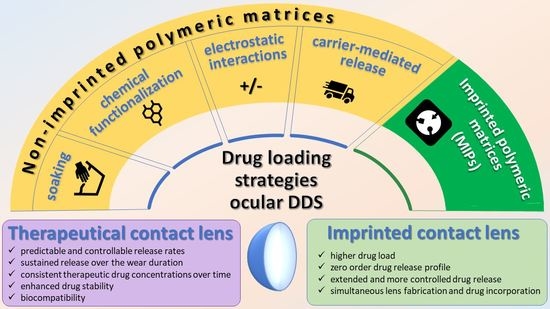
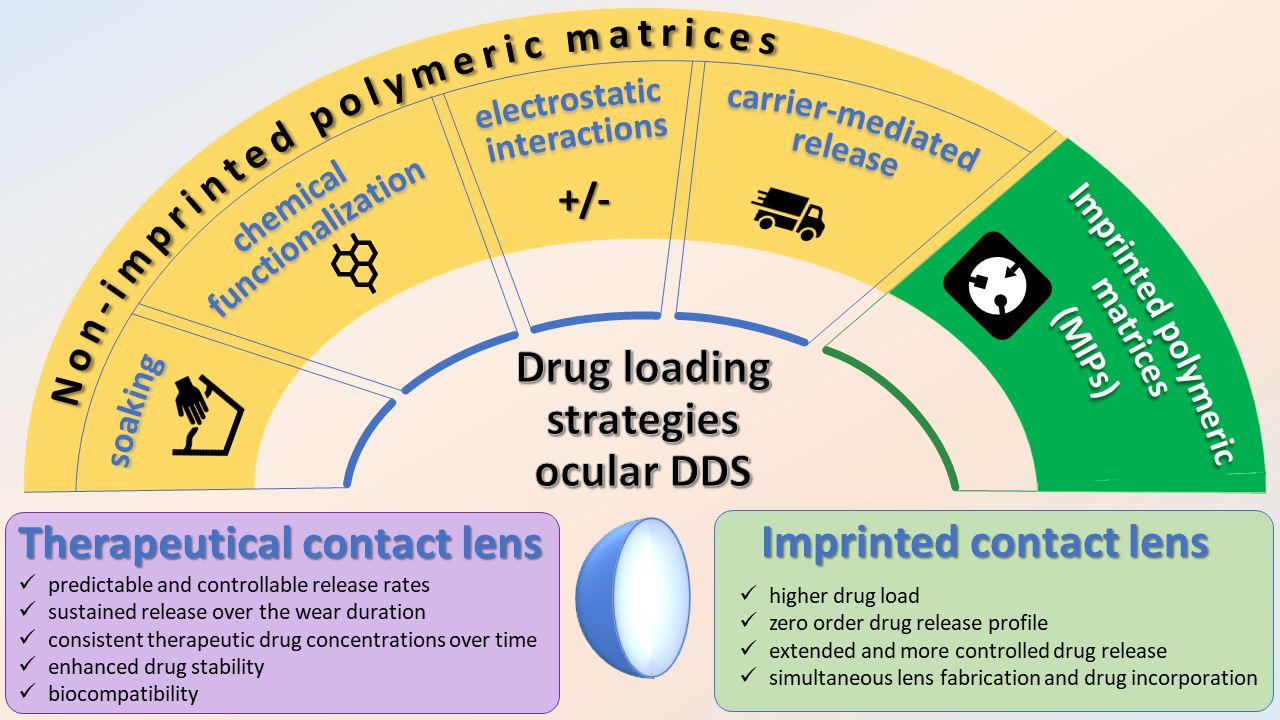
3. Drug Loading Strategies in Polymeric Matrices for Extended Drug Delivery
3.1. Hydrogels
3.2. Molecularly Imprinted Polymer (MIP)-Based as Drug Reservoirs
4. MIP-Based Systems Intended for Ocular Drug Delivery
4.1. Advantages and Limitations of Molecular Imprinting in Ocular DDS Development
4.1.1. Advantages
4.1.2. Challenges
4.2. Balancing between Flexibility of CLs and Imprinting Efficiency
4.3. Computer Modeling
4.4. Loading/Release Efficiency
4.5. Contact Lenses as Promising MIP-Based DDS for Ocular Treatment
5. Challenges and Perspectives of MIPs as Ocular DDS
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Resnikoff, S.; Kocur, I. Non-communicable eye diseases: Facing the future. Community Eye Health J. 2014, 27, 41–43. [Google Scholar]
- WHO World report on vision. World Health Organ. 2019, 214, 1–160.
- Bourne, R.R.A.; Steinmetz, J.D.; Saylan, M.; Mersha, A.M.; Weldemariam, A.H.; Wondmeneh, T.G.; Sreeramareddy, C.T.; Pinheiro, M.; Yaseri, M.; Yu, C.; et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, Y.; Li, X.; Kebebe, D.; Zhang, B.; Ren, J.; Lu, J.; Li, J.; Du, S.; Liu, Z. Research progress of in-situ gelling ophthalmic drug delivery system. Asian J. Pharm. Sci. 2019, 14, 1–15. [Google Scholar] [CrossRef]
- Zhou, R.; Caspi, R.R. Ocular immune privilege. F1000 Biol. Rep. 2010, 2, 3. [Google Scholar] [CrossRef] [PubMed]
- Mantelli, F.; Mauris, J.; Argüeso, P. The ocular surface epithelial barrier and other mechanisms of mucosal protection: From allergy to infectious diseases. Curr. Opin. Allergy Clin. Immunol. 2013, 13, 563–568. [Google Scholar] [CrossRef] [Green Version]
- Eghrari, A.O.; Riazuddin, S.A.; Gottsch, J.D. Overview of the Cornea: Structure, Function, and Development. Prog. Mol. Biol. Transl. Sci. 2015, 134, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, K.M.; Kananen, K.; Auriola, S.; Kontturi, K.; Urtti, A. Characterization of paracellular and aqueous penetration routes in cornea, conjunctiva, and sclera. Investig. Ophthalmol. Vis. Sci. 1997, 38, 627–634. [Google Scholar] [PubMed]
- Prausnitz, M.R. Permeability of cornea, sciera, and conjunctiva: A literature analysis for drug delivery to the eye. J. Pharm. Sci. 1998, 87, 1479–1488. [Google Scholar] [CrossRef]
- Morrison, P.W.J.; Khutoryanskiy, V.V. Advances in ophthalmic drug delivery. Ther. Deliv. 2014, 5, 1297–1315. [Google Scholar] [CrossRef] [Green Version]
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Barar, J.; Javadzadeh, A.R.; Omidi, Y. Ocular novel drug delivery: Impacts of membranes and barriers. Expert Opin. Drug Deliv. 2008, 5, 567–581. [Google Scholar] [CrossRef]
- Almeida, H.; Amaral, M.H.; Lobão, P.; Lobo, J.M.S. In situ gelling systems: A strategy to improve the bioavailability of ophthalmic pharmaceutical formulations. Drug Discov. Today 2014, 19, 400–412. [Google Scholar] [CrossRef]
- Karla, P.K.; Earla, R.; Boddu, S.H.; Johnston, T.P.; Pal, D.; Mitra, A. Molecular expression and functional evidence of a drug efflux pump (BCRP) in human corneal epithelial cells. Curr. Eye Res. 2009, 34, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Maulvi, F.A.; Soni, T.G.; Shah, D.O. A review on therapeutic contact lenses for ocular drug delivery. Drug Deliv. 2016, 23, 3017–3026. [Google Scholar] [CrossRef]
- Kuno, N.; Fujii, S. Recent Advances in Ocular Drug Delivery Systems. Polymers 2011, 3, 193–221. [Google Scholar] [CrossRef]
- Patel, A. Ocular drug delivery systems: An overview. World J. Pharmacol. 2013, 2, 47. [Google Scholar] [CrossRef] [PubMed]
- Daull, P.; Amrane, M.; Garrigue, J.-S. Novasorb® Cationic Nanoemulsion and Latanoprost: The Ideal Combination for Glaucoma Management? Journal of Eye Diseases and Disorders. J. Eye Dis. Disord 2017, 2, 1. [Google Scholar] [CrossRef]
- Souto, E.B.; Dias-Ferreira, J.; López-Machado, A.; Ettcheto, M.; Cano, A.; Espuny, A.C.; Espina, M.; Garcia, M.L.; Sánchez-López, E. Advanced formulation approaches for ocular drug delivery: State-of-the-art and recent patents. Pharmaceutics 2019, 11, 460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Hao, L.; Wang, H.; Yang, X.; Zhang, G.; Wang, G.; Zhang, X. Hydrogel contact lens for extended delivery of ophthalmic drugs. Int. J. Polym. Sci. 2011, 2011, 814163. [Google Scholar] [CrossRef]
- Zhang, X.; Cao, X.; Qi, P. Therapeutic contact lenses for ophthalmic drug delivery: Major challenges. J. Biomater. Sci. Polym. Ed. 2020, 31, 549–560. [Google Scholar] [CrossRef]
- Peral, A.; Martinez-Aguila, A.; Pastrana, C.; Huete-Toral, F.; Carpena-Torres, C.; Carracedo, G. Contact Lenses as Drug Delivery System for Glaucoma: A Review. Appl. Sci. 2020, 10, 5151. [Google Scholar] [CrossRef]
- Weng, Y.; Liu, J.; Jin, S.; Guo, W.; Liang, X.; Hu, Z. Nanotechnology-based strategies for treatment of ocular disease. Acta Pharm. Sin. B 2017, 7, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- del Amo, E.M.; Rimpelä, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic aspects of retinal drug delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702. [Google Scholar] [CrossRef] [Green Version]
- Bisht, R.; Mandal, A.; Jaiswal, J.K.; Rupenthal, I.D. Nanocarrier mediated retinal drug delivery: Overcoming ocular barriers to treat posterior eye diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2018, 10, 1473. [Google Scholar] [CrossRef]
- Saw, S.M.; Gazzard, G.; Friedman, D.S. Interventions for angle-closure glaucoma: An evidence-based update. Ophthalmology 2003, 110, 1869–1879. [Google Scholar] [CrossRef]
- Bodoki, A.E.; Iacob, B.-C.; Bodoki, E. Perspectives of molecularly imprinted polymer-based drug delivery systems in cancer therapy. Polymers 2019, 11, 2085. [Google Scholar] [CrossRef] [Green Version]
- Bodoki, A.E.; Iacob, B.-C.; Gliga, L.E.; Oprean, S.L.; Spivak, D.A.; Gariano, N.A.; Bodoki, E. Improved Enantioselectivity for Atenolol Employing Pivot Based Molecular Imprinting. Molecules 2018, 23, 1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Lorenzo, C.; Hiratani, H.; Gómez-Amoza, J.L.; Martínez-Pacheco, R.; Souto, C.; Concheiro, A. Soft contact lenses capable of sustained delivery of timolol. J. Pharm. Sci. 2002, 91, 2182–2192. [Google Scholar] [CrossRef] [PubMed]
- Hiratani, H.; Alvarez-Lorenzo, C. Timolol uptake and release by imprinted soft contact lenses made of N,N-diethylacrylamide and methacrylic acid. J. Control. Release 2002, 83, 223–230. [Google Scholar] [CrossRef]
- Hiratani, H.; Fujiwara, A.; Tamiya, Y.; Mizutani, Y.; Alvarez-Lorenzo, C. Ocular release of timolol from molecularly imprinted soft contact lenses. Biomaterials 2005, 26, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Guidi, G.; Korogiannaki, M.; Sheardown, H. Modification of Timolol Release From Silicone Hydrogel Model Contact Lens Materials Using Hyaluronic Acid. Eye Contact Lens Sci. Clin. Pract. 2014, 40, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, S.; Sizemore, S.P.; Byrne, M.E. Biomimetic hydrogels for enhanced loading and extended release of ocular therapeutics. Biomaterials 2007, 28, 717–724. [Google Scholar] [CrossRef]
- Ali, M.; Horikawa, S.; Venkatesh, S.; Saha, J.; Hong, J.W.; Byrne, M.E. Zero-order therapeutic release from imprinted hydrogel contact lenses within in vitro physiological ocular tear flow. J. Control. Release 2007, 124, 154–162. [Google Scholar] [CrossRef]
- Tieppo, A.; White, C.J.; Paine, A.C.; Voyles, M.L.; McBride, M.K.; Byrne, M.E. Sustained in vivo release from imprinted therapeutic contact lenses. J. Control. Release 2012, 157, 391–397. [Google Scholar] [CrossRef]
- Hui, A.; Sheardown, H.; Jones, L. Acetic and Acrylic Acid Molecular Imprinted Model Silicone Hydrogel Materials for Ciprofloxacin-hcl Delivery. Materials 2012, 5, 85–107. [Google Scholar] [CrossRef] [Green Version]
- Hui, A.; Willcox, M.; Jones, L. In vitro and in vivo evaluation of novel ciprofloxacin-releasing silicone hydrogel contact lenses. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4896–4904. [Google Scholar] [CrossRef]
- Kioomars, S.; Heidari, S.; Malaekeh-Nikouei, B.; Shayani Rad, M.; Khameneh, B.; Mohajeri, S.A. Ciprofloxacin-imprinted hydrogels for drug sustained release in aqueous media. Pharm. Dev. Technol. 2017, 22, 122–129. [Google Scholar] [CrossRef]
- Silva, D.; de Sousa, H.C.; Gil, M.H.; Santos, L.F.; Oom, M.S.; Alvarez-Lorenzo, C.; Saramago, B.; Serro, A.P. Moxifloxacin-imprinted silicone-based hydrogels as contact lens materials for extended drug release. Eur. J. Pharm. Sci. 2021, 156, 105591. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; de Sousa, H.C.; Gil, M.H.; Santos, L.F.; Amaral, R.A.; Saraiva, J.A.; Salema-Oom, M.; Alvarez-Lorenzo, C.; Serro, A.P.; Saramago, B. Imprinted hydrogels with LbL coating for dual drug release from soft contact lenses materials. Mater. Sci. Eng. C 2021, 120, 111687. [Google Scholar] [CrossRef] [PubMed]
- Topete, A.; Barahona, I.; Santos, L.F.; Pinto, C.A.; Saraiva, J.A.; Paula Serro, A.; Saramago, B. The effects of addition of functional monomers and molecular imprinting on dual drug release from intraocular lens material. Int. J. Pharm. 2021, 600, 120513. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, B.; Dalgakiran, D.; Inan, T.; Kurkcuoglu, O.; Güner, F.S. A computational and experimental approach to develop minocycline-imprinted hydrogels and determination of their drug delivery performances. J. Polym. Res. 2018, 25, 1–10. [Google Scholar] [CrossRef]
- Malakooti, N.; Alexander, C.; Alvarez-Lorenzo, C. Imprinted Contact Lenses for Sustained Release of Polymyxin B and Related Antimicrobial Peptides. J. Pharm. Sci. 2015, 104, 3386–3394. [Google Scholar] [CrossRef] [PubMed]
- Abouelatta, S.M.; Sheta, A.I.; Ibrahim, R.R. Optimized molecular imprints in gamma-irradiated collagen shields of an antifungal drug: In vitro characterization, in-vivo bioavailability enhancement. Eur. J. Pharm. Biopharm. 2021, 166, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Varela-Garcia, A.; Gomez-Amoza, J.L.; Concheiro, A.; Alvarez-Lorenzo, C. Imprinted contact lenses for ocular administration of antiviral drugs. Polymers 2020, 12, 2026. [Google Scholar] [CrossRef] [PubMed]
- Tieppo, A.; Pate, K.M.; Byrne, M.E. In vitro controlled release of an anti-inflammatory from daily disposable therapeutic contact lenses under physiological ocular tear flow. Eur. J. Pharm. Biopharm. 2012, 81, 170–177. [Google Scholar] [CrossRef]
- Malaekeh-Nikouei, B.; Ghaeni, F.A.; Motamedshariaty, V.S.; Mohajeri, S.A. Controlled release of prednisolone acetate from molecularly imprinted hydrogel contact lenses. J. Appl. Polym. Sci. 2012, 126, 387–394. [Google Scholar] [CrossRef]
- White, C.J.; Di Pasquale, S.A.; Byrne, M.E. Controlled release of multiple therapeutics from silicone hydrogel contact lenses. Optom. Vis. Sci. 2016, 93, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Raesian, P.; Rad, M.S.; Khodaverdi, E.; Motamedshariaty, V.S.; Mohajeri, S.A. Preparation and characterization of fluorometholone molecular imprinted soft contact lenses as ocular controlled drug delivery systems. J. Drug Deliv. Sci. Technol. 2021, 64, 102591. [Google Scholar] [CrossRef]
- Yan, F.; Liu, Y.; Han, S.; Zhao, Q.; Liu, N. Bimatoprost Imprinted Silicone Contact Lens to Treat Glaucoma. AAPS PharmSciTech 2020, 21, 63. [Google Scholar] [CrossRef]
- Omranipour, H.; Sajadi Tabassi, S.; Kowsari, R.; Rad, M.; Mohajeri, S. Brimonidine Imprinted Hydrogels and Evaluation of Their Binding and Releasing Properties as New Ocular Drug Delivery Systems. Curr. Drug Deliv. 2015, 12, 717–725. [Google Scholar] [CrossRef]
- Ribeiro, A.; Veiga, F.; Santos, D.; Torres-Labandeira, J.J.; Concheiro, A.; Alvarez-Lorenzo, C. Bioinspired Imprinted PHEMA-Hydrogels for ocular delivery of carbonic anhydrase inhibitor drugs. Biomacromolecules 2011, 12, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.; Veiga, F.; Santos, D.; Torres-Labandeira, J.J.; Concheiro, A.; Alvarez-Lorenzo, C. Receptor-based biomimetic NVP/DMA contact lenses for loading/eluting carbonic anhydrase inhibitors. J. Memb. Sci. 2011, 383, 60–69. [Google Scholar] [CrossRef]
- Nikouei, B.M.-; Vahabzadeh, S.A.; Mohajeri, S.A. Preparation of a Molecularly Imprinted Soft Contact Lens as a New Ocular Drug Delivery System for Dorzolamide. Curr. Drug Deliv. 2013, 10, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Da-mota, A.F.; Vivero-Lopez, M.; Topete, A.; Serro, A.P.; Concheiro, A.; Alvarez-Lorenzo, C. Atorvastatin-eluting contact lenses: Effects of molecular imprinting and sterilization on drug loading and release. Pharmaceutics 2021, 13, 606. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Byrne, M.E. Controlled Release of High Molecular Weight Hyaluronic Acid from Molecularly Imprinted Hydrogel Contact Lenses. Pharm. Res. 2009, 26, 714–726. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; McBride, M.K.; Pate, K.M.; Tieppo, A.; Byrne, M.E. Extended release of high molecular weight hydroxypropyl methylcellulose from molecularly imprinted, extended wear silicone hydrogel contact lenses. Biomaterials 2011, 32, 5698–5705. [Google Scholar] [CrossRef] [PubMed]
- Yañez, F.; Chauhan, A.; Concheiro, A.; Alvarez-Lorenzo, C. Timolol-imprinted soft contact lenses: Influence of the template: Functional monomer ratio and the hydrogel thickness. J. Appl. Polym. Sci. 2011, 122, 1333–1340. [Google Scholar] [CrossRef]
- Sibrian-Vazquez, M.; Spivak, D.A. Improving the Strategy and Performance of Molecularly Imprinted Polymers Using Cross-Linking Functional Monomers. J. Org. Chem. 2003, 68, 9604–9611. [Google Scholar] [CrossRef]
- Tashakori-Sabzevar, F.; Mohajeri, S.A. Development of ocular drug delivery systems using molecularly imprinted soft contact lenses. Drug Dev. Ind. Pharm. 2015, 41, 703–713. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Hiratani, H.; Concheiro, A. Contact lenses for drug delivery: Achieving sustained release with novel systems. Am. J. Drug Deliv. 2006, 4, 131–151. [Google Scholar] [CrossRef]
- Byrne, M.E.; Salian, V. Molecular imprinting within hydrogels II: Progress and analysis of the field. Int. J. Pharm. 2008, 364, 188–212. [Google Scholar] [CrossRef] [PubMed]
- Van Beek, M.; Weeks, A.; Jones, L.; Sheardown, H. Immobilized hyaluronic acid containing model silicone hydrogels reduce protein adsorption. J. Biomater. Sci. Polym. Ed. 2008, 19, 1425–1436. [Google Scholar] [CrossRef]
- Hiratani, H.; Alvarez-Lorenzo, C. The nature of backbone monomers determines the performance of imprinted soft contact lenses as timolol drug delivery systems. Biomaterials 2004, 25, 1105–1113. [Google Scholar] [CrossRef]
- Momose, T.; Ito, N.; Kanai, A.; Watanabe, Y.; Shibata, M. Adsorption of levocabastine eye drops by soft contact lenses and its effects in rabbit eyes. CLAO J. 1997, 23, 96–99. [Google Scholar]
- Cope, J.R.; Collier, S.A.; Rao, M.M.; Chalmers, R.; Mitchell, G.L.; Richdale, K.; Wagner, H.; Kinoshita, B.T.; Lam, D.Y.; Sorbara, L.; et al. Contact Lens Wearer Demographics and Risk Behaviors for Contact Lens-Related Eye Infections–United States, 2014. MMWR. Morb. Mortal. Wkly. Rep. 2015, 64, 865–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musgrave, C.S.A.; Fang, F. Contact Lens Materials: A Materials Science Perspective. Materials 2019, 12, 261. [Google Scholar] [CrossRef] [Green Version]
- Donshik, P.C. Extended wear contact lenses. Ophthalmol. Clin. 2003, 16, 305–309. [Google Scholar] [CrossRef]
- Silva, D.; Sousa, H.C.d.; Gil, M.H.; Santos, L.F.; Moutinho, G.M.; Serro, A.P.; Saramago, B. Antibacterial layer-by-layer coatings to control drug release from soft contact lenses material. Int. J. Pharm. 2018, 553, 186–200. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Active Pharmaceutical Ingredient | Imprinting Approach Polymerization Mixture (Functional Monomer/CROSSLINKER/INITIATOR) | Polymeric Scaffold Characteristics | Drug Load | Drug Release | Development Stage | Key Observations | References |
|---|---|---|---|---|---|---|---|
| Timolol maleate | Non-covalent imprinting; MAA/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly-HEMA hydrogel/CL (700 μm) Water uptake: 108% | 12 mg/g hydrogel for MIP vs. 4 mg/g hydrogel for NIP IF = 3 | Sustained release (complete release in 12 h; slowest release in artificial lacrimal fluid, pH = 8) | Material characterization In vitro release studies: method–sink model; medium–0.9% NaCl (pH = 5.5), PBS (pH = 7.4), artificial lacrimal fluid (pH = 8), 37 °C | [30] | |
| Timolol maleate | Non-covalent imprinting; MAA/EGDMA/Darocur 1173; UV, 50 min, room temperature | Poly–DEAA hydrogel/CL (300 μm) Water uptake: not reported | IF: approx. 2 | Sustained release for 48 h | Material characterization In vitro release studies: method–sink model; medium–0.9% NaCl (pH = 7), 37 °C | [31] | |
| Timolol maleate | Non-covalent imprinting; MAA/EGDMA/Darocur 1173; UV, 20 min, room temperature | Poly–DEAA hydrogel/CL (80 μm) Water uptake: 35–36% | 34.7 μg/lens for MIP vs. 21.2 μg/lens for NIP IF = 1.63 | In-vivo release studies–sustained release: initial pulse release (up to Cmax = 330 μM for MIP vs. Cmax = 183 μM for NIP) followed by exponential decrease | Material characterization In vitro release studies: method–sink model; medium–0.9% NaCl (pH = 7), 37 °C In vivo release studies: Nippon albino rabbits | In vivo release studies: Timolol detected in the tear fluid for 180 min for MIP vs. 90 min and 60 min for NIP and eye drop solution, respectively; MRT-12 min. for MIP and NIP vs. 5.32 min and 6.35 min for 0.068% and 0.25% eye drop solution, respectively | [32] |
| Timolol maleate | Non-covalent imprinting; -/EGDMA/Irgacure 184; UV, 15 min, room temperature | Poly (HEMA-co-TRIS) and Poly (DMA-co-TRIS) hydrogels/CL (1000 μm) Water uptake: 26.5% and 32.3% | Not reported | Sustained release for 48 h; Combined strategy, MI and addition of hyaluronic acid-highest mass of released drug | Material characterization In vitro release studies: method–sink model; medium–PBS (pH = 7.4), 37 °C | Hyaluronic acid–negatively charged wetting agent used as a functional additive instead of functional monomers to increase loading capacity | [33] |
| Ketotifen fumarate | Non-covalent imprinting; AA, AM, NVP/PEG200DMA/AIBN; UV, 10 min, 36 °C | Poly-HEMA hydrogel/CL (400 µm and 700 µm) Water uptake: 40–50% | 4.9 × 10−2 mmol/g hydrogel for MIP | Artificial lacrimal fluid-prolonged release profile for 5 days (2200 µg cumulative release, 80% drug released in 4 days) Lysozyme (1mg/mL) in artificial lacrimal fluid–5-fold increase in the duration of release | Material characterization In vitro release studies: method–sink model; medium–artificial lacrimal fluid (pH = 80), and lysozyme (1mg/mL) in artificial lacrimal fluid | Receptor-inspired hydrogel (microdomains that resemble histamine H1-receptors) | [34] |
| Ketotifen fumarate | Non-covalent imprinting; AA, AM, NVP/PEG200DMA/AIBN; UV, 10 min, 36 °C | Poly-HEMA hydrogel/CL (thickness not reported) Water uptake: not reported | 20.85 mg/g hydrogel for MIP | Infinite sink model: Fickian kinetics, prolonged release for 5 days (1200 µg cumulative release, 80% drug released in 4 days) Physiological flow model: Zero-order kinetics, sustained release for 3.5 days (45 µg cumulative release, constant rate of 12.9 µg/day) | Material characterization In vitro release studies: method–sink model, and physiological flow model (microfluidic device); medium–artificial lacrimal fluid (pH = 8) | Zero-order release under physiological volumetric flow rates | [35] |
| Ketotifen fumarate | Non-covalent imprinting; AA, AM, NVP/PEG200DMA/AIBN; UV, 9 min, 35 °C | Poly-HEMA hydrogel/CL (100 μm) Water uptake: not reported | 115 μg/lens for MIP vs. 39 μg/lens for NIP IF = 2.95 | In vitro release studies: prolonged release for 72 h (85% of drug released in 24 h for MIP vs. 100% drug released in 6 h for NIP) In vivo release studies: initial pulse release (up to Cmax = 214 μg/mL) followed by a sustained release for MIP vs. initial pulse release (up to Cmax = 140 μg/mL) followed by an exponential decrease for NIP | Material characterization In vitro release studies: method–sink model; medium–artificial lacrimal fluid (pH = 8), 34 °C In vivo release studies: New Zealand white rabbits | In vivo release studies: MRT–12.47 h for MIP, 3.75 and 50 times greater than for NIP and 0.035% eye drops, respectively; sustained, extended release (average constant tear film concentration of 170 μg/mL up to 26 h) | [36] |
| Ciprofloxacin | Non-covalent imprinting; AA/EGDMA/Irgacure; UV, 20 min and 50 °C overnight | Poly (HEMA-co-TRIS) hydrogel/CL (1000 μm) Water uptake: approx. 15% | Not reported | Sustained release for up to 14 days | Material characterization In vitro release studies: method–sink model; medium–artificial lacrimal fluid (pH = 8) | [37] | |
| Ciprofloxacin | Non-covalent imprinting; AA/EGDMA/AIBN, Irgacure 1173; UV, 5 min, room temperature | Poly (HEMA-co-TRIS-co-NVP) hydrogel/CL (64 μm) Water uptake: 36.2% | 1509 μg/lens for MIP vs. 1383 μg/lens for NIP IF = 1.09 | Sustained release for up to 8 h | Material characterization In vitro release studies: method–sink model; medium–PBS (pH = 8) In vitro antibacterial activity (P. aeruginosa) In vivo testing of antimicrobial activity–Rabbit scratch model (white New Zealand rabbits) | In-vivo study: the imprinted SCL have similar performance to conventional antibiotic eye drops | [38] |
| Ciprofloxacin | Non-covalent imprinting; MAA/EGDMA/AIBN; 50 °C, 24 h | Poly-HEMA hydrogel/CL (400 μm) Water uptake: 34% | 170–210 μg/disc for MIP vs. 120–160 μg/disc for NIP IF = 1.31–1.41 | Sustained release (60% released in the first 5 h followed by a sustained release profile for 50 h) | Material characterization In vitro release studies: method–sink model; medium–NaCl 0.9%, and artificial lacrimal fluid (pH = 8), 37 °C In vitro antibacterial activity (P. aeruginosa, S. aureus) | [39] | |
| Moxifloxacin | Non-covalent imprinting; AA/EGDMA/AIBN; 60 °C, 24 h | Poly (HEMA-co-TRIS-co-NVP) hydrogel/CL (300 μm) Water uptake: 130% | 64.9 μg/mg hydrogel for MIP vs. 44.1 μg/mg hydrogel for NIP IF = 1.47 | Sustained release (60% release in the first 8 h followed by a sustained release of effective concentrations for 13 days; 45 μg/mg hydrogel cumulative release) | Material characterization In vitro release studies: methods–sink model and physiological flow model using a microfluidic device; medium–artificial lacrimal fluid (pH = 8), 36 °C In vitro antibacterial activity (S. aureus and S. epidermidis) | [40] | |
| Moxifloxacin | Non-covalent imprinting; AA/EGDMA/AIBN; 60 °C, 24 h | Poly (HEMA-co-TRIS-co-NVP) LbL coated hydrogel/CL (300 μm) Water uptake: 119% | 44 μg/mg hydrogel for LbL MIP vs. 9 μg/mg hydrogel for LbL NIP IF = 4.88 | Sustained release (23% release in the first 1 h followed by a sustained release of effective concentrations for 10 days; 20–25 μg/mg hydrogel cumulative release) | Material characterization In vitro release studies: methods –sink model, and the physiological flow model (microfluidic device); medium–130 mM NaCl (pH = 6.9), 36 °C In vitro antibacterial activity (S. aureus and S. epidermidis) | The combination of MI and LbL coating-sustained double release of moxifloxacin and diclofenac | [41] |
| Moxifloxacin and Diclofenac | Non-covalent imprinting; MAA/EGDMA/AIBN; 60 °C, 18 h | CI26Y hydrogel/IOL Water uptake: approx. 25% | Diclofenac: 16 μg/mg hydrogel for MIP vs. 12.2 μg/mg hydrogel for NIP IF = 1.31 Moxifloxacin: 28 μg/mg hydrogel for both MIP and NIP. | Diclofenac–sustained release up to 14 days (71% for MIP and 81% for NIP cumulative release) Moxifloxacin–sustained release for up to 14 days (83% for MIP and 81% for NIP cumulative release) | Material characterization In vitro release studies: method–sink model; medium–PBS (pH = 8), 36 °C Mathematical model for the prediction of the In vivo therapeutic efficacy In vitro irritability tests, cytotoxicity tests and antibacterial tests | MI Intraocular lens material for the simultaneous delivery of diclofenac and moxifloxacin | [42] |
| Minocycline | Non-covalent imprinting; AA/EGDMA/ 2,2’-Azobis(2,4-dimethyl-valeronitrile); 45 °C, 24 h | Poly-HEMA hydrogel/- Water uptake: 40% MIP vs. 35% NIP | 0.243 μg/mg hydrogel for MIP vs. 0.082 μg/mg hydrogel for NIP IF = 2.9 | Sustained release for 48 h (2.294 μg/mg hydrogel for MIP and 1.696 μg/mg hydrogel for NIP cumulative release) | Material characterization In vitro release studies: method–sink model; medium–NaCl 0.9%, 37 °C | Molecular dynamics simulations to select the suitable monomer and the optimum amount of crosslinker | [43] |
| Polymyxin B | Non-covalent imprinting; AA/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly-HEMA hydrogel/CL (400 μm) Water uptake: 37% | Approx. 90 mg/g disc | Sustained release for up to 14 days (41% drug released in 7 days; 40 mg/g disc cumulative release) | Material characterization In vitro release studies: method–sink model; medium–NaCl 0.9% In vitro antibacterial activity (P. aeruginosa) | [44] | |
| Voriconazole | Non-covalent imprinting; AM, MMA/EGDMA/ benzoyl peroxide; 70 °C, 24 h | Collagen shield | Binding capacity: 82.79% for MIP vs. 20.65% for NIP IF = 4.01 | In vitro release studies: Sustained release-73.5% after 24 h, and 85.39% after 48 h In vivo release studies: initial drug release up to Cmax = 62.3 ng/mL (24 h), for collagen-MIP vs. burst drug release up to Cmax = 47.38 ng/mL (3 h) followed by an exponential decrease for the voriconazole solution | Material characterization In vitro release studies: method-sink model; medium-artificial lacrimal fluid (32 °C) In vitro antifungal activity Ex vivo cornea permeation study In vivo studies on albino rabbits | In vivo release studies: 29.09 h MRT for collagen-MIP vs. 6.86 h MRT for voriconazole solution; sustained release with a 7.53-fold increase in bioavailability as compared to the voriconazole solution | [45] |
| Valacyclovir or Acyclovir | Non-covalent imprinting; MAA/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly-HEMA hydrogel/CL (450 μm) Water uptake: 90% | Valacyclovir: approx. 4.5 mg/g disc for MIP Acyclovir: approx. 2 mg/g disc for MIP | Valacyclovir: sustained release for 10 h (3.5–4 mg/g disc cumulative release) Acyclovir–0.6 mg/g disc accumulative release (irreversible binding of significant amount of template) | Material characterization In vitro eye compatibility test In vitro release studies: medium–artificial lacrimal fluid In vitro drug permeability studies (bovine and porcine cornea and sclera) | Computational modeling to elucidate drug–functional monomer interactions In vitro drug permeability studies–accumulation in the cornea and penetration through the sclera for valacyclovir | [46] |
| Diclofenac | Non-covalent imprinting; DEAEM/PEG200DMA/AIBN; UV, 8 min, 35 °C | Poly-HEMA hydrogel/CL (105 μm) wollen polymer volume fractions: 1.535 | 0.015–0.02 mg/mg hydrogel | Sink model: sustained release for 72 h Physiological flow model: Zero-order kinetics, linear release profile up to 48 h, (release rate 6.75 µg/h) | Material characterization In vitro release studies: methods– infinite sink model and physiological flow model (microfluidic device); medium–artificial lacrimal fluid (34 °C) | Zero-order release under physiological volumetric flow rates | [47] |
| Prednisolone acetate | Non-covalent imprinting; MAA/EGDMA/AIBN; 60 °C, 24 h | Poly-HEMA hydrogels/CL (400 μm) Water uptake: 62–63% | 58 μg/disc for MIP vs. 39 μg/disc for NIP IF = 1.49 | Sustained release for 48 h (64% drug in 48 h for MIP vs. 78% drug release within 8 h for NIP) | Material characterization In vitro release studies: methods–sink model, medium-0.9% NaCl and artificial lacrimal fluid (pH = 8), 37 °C | [48] | |
| HPMC, trehalose, ibuprofen, prednisolone | Non-covalent imprinting; AA, 4VPh/EGDMA, PEG200DMA/Darocur 1173; UV, 1.5 min., room temperature | Poly (TRIS-co-DMA-co-DMS-R11)/CL (100 μm) Water uptake: not reported | HPMC and trehalose: 500 μg/lens Ibuprofen and prednisolone: 150 μg/lens | Sustained release HPMC: 20% drug release in 7 days (release rate 14–18 μg/day), and complete release in 36 days Trehalose: 90% drug release/24 h (linear release, 17 μg/h) Ibuprofen and prednisolone: 30% drug release in 1 day (release rate 45 μg/day) | Material characterization In vitro release studies: methods–sink model, and physiological flow model (microfluidic device); medium–water, NaCl 0.9%, NaCl 5%, PBS (pH = 7.4), artificial lacrimal fluid (pH = 8), 34 °C | Simultaneous load and release of HPMC, trehalose, ibuprofen and prednisolone | [49] |
| Fluorometholone | Non-covalent imprinting; MAA/EGDMA/AIBN; UV, 40 min, room temperature | Poly-HEMA hydrogels/CL (200 μm) Water uptake: 53.75–57.25% | 61 μg/lens for MIP vs. 40 μg/lens for NIP IF = 1.53 | Sustained release-59.7% and 92.8% of drug was released from MIP and NIP, respectively, within the first 8 h | Material characterization In vitro release studies: method–sink model; medium-0.9% NaCl (pH = 5.5), artificial lacrimal fluid (pH = 8), 37 °C | [50] | |
| Bimatoprost | Non-covalent imprinting; MAA/EGDMA/Irgacure; UV, 15 min, room temperature | Poly (HEMA-co-DMA-co-siloxane) hydrogel/CL (thickness not reported) Water uptake: 88% MIP vs. 92% NIP | 14.76 μg/lens for MIP vs. 10.75 μg/lens for NIP IF = 1.37 | In vivo release study: sustained release up to 36–60 h-Cmax (5 min)-56.26 μg/mL for MIP vs. 62.35 μg/mL for NIP and 145.26 μg/mL for 0.03% bimatoprost eye drop solution | Material characterization In vitro release studies: method-sink model; medium–artificial lacrimal fluid (pH = 8), 34 °C In vivo release studies: white New Zealand rabbits | The in-vivo study-low burst release and increase in bimatoprost MRT for MIP-SCL vs. conventional soaked SCL (NIP) and 0.03% bimatoprost eye drop solution | [51] |
| Brimonidine | Non-covalent imprinting; MAA/EGDMA/AIBN; 50 °C, 24 h | Poly-HEMA hydrogel/CL (400 μm) Water uptake: 47% | 3 μg/mg hydrogel for MIP vs. 1.75 μg/mg hydrogel for NIP IF = 1.71 | Sustained release for 48 h(39-50% drug released from MIPs vs. 70% drug released from NIP in the first 30 min) | Material characterization In vitro release studies: medium–NaCl 0.9%, and artificial lacrimal fluid, pH = 8, 37 °C | [52] | |
| Acetazolamide | Pivot based imprinting; Zn(II) methacrylate, 4VI, HEAA/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly-HEMA hydrogel/CL (900 μm) Water uptake: 80–85% | Acetazolamide: 3.28 mg/g hydrogel for MIP vs. 3.15 mg/g for NIP Ethoxzolamide: 1.71 mg/g hydrogel for MIP vs. 1.55 mg/g for NIP | Sustained release for 2 weeks (Acetazolamide: 20% released in 6 h and 50% released in 192 h; Ethozxolamide: 15% released in 6 h and 25% released in 192 h) | Material characterization In vitro release studies: method–sink model; medium–0.9% NaCl, room temperature Cytocompatibility tests (Balb/3T3 Clone A31 cell line) | Receptor-inspired hydrogel Highest affinity and better control of release for the non-imprinted networks; the use of functional monomers that best mimic carbonic anhydrase receptors is critical | [53] |
| Acetazolamide | Pivot based imprinting; Zn(II) nitrate hexahydrate, 4VI, HEAA/Zn(II)/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly (DMA-co-NVP) hydrogel/CL (900 μm) Water uptake: 80–85% | Acetazolamide: 4.11 mg/g hydrogel for MIP vs. 3.81 mg/g hydrogel for NIP Ethoxzolamide: 1.34 mg/g hydrogel for MIP vs. 1.47 mg/g hydrogel for NIP | Sustained release for 9–12 h (Acetazolamide: 50% drug release in the first hour; Ethoxzolamide: 50–70% drug released in 12 h) | Material characterization In vitro release studies: method–sink model; medium–0.9% NaCl, room temperature Cytocompatibility tests (Balb/3T3 Clone A31 cell line) | Receptor-inspired hydrogel The use of functional monomers that best mimic carbonic anhydrase receptors is critical | [54] |
| Dorzolamide | Non-covalent imprinting; MAA/EGDMA/AIBN; 50 °C, 24 h | Poly-HEMA hydrogel/CL (400 μm) Water uptake: approx. 47% | 105 μg/disc for MIP vs. 77 μg/disc for NIP IF = 1.36 | Sustained drug release for 48 h (24% drug released from MIP vs. 62% drug released from NIP in the first 0.5 h, and 51% drug released from MIP vs. 80% drug released from NIP in 3 h) | Material characterization In vitro release studies: method –sink model; medium–0.9% NaCl and artificial lacrimal fluid (pH = 8), 37 °C | [55] | |
| Atorvastatin | Non-covalent imprinting; EGPEM, AEMA, APMA/EGDMA/AIBN; 50 °C, 12 h and 70 °C, 24 h | Poly-HEMA hydrogel/CL (300 μm) Water content: 90% | 6.69 mg/g hydrogel for MIP vs. 5.81 mg/g hydrogel for NIP IF = 1.15 | Sustained release for 7 days; (~7 mg/g for MIP vs. ~6 mg/g for NIP after 1 week) | Material characterization In vitro release studies: method–sink model; medium-artificial lacrimal fluid (pH = 7.4), 37 °C Ocular irritancy test (hen’s egg test chorioallantoic membrane) Cytocompatibility tests (Balb/3T3 fibroblasts cells) Ex vivo cornea and sclera permeability and accumulation of atorvastatin | Computational modeling docking to elucidate drug–functional monomer interactions | [56] |
| Hyaluronic acid | Non-covalent imprinting; AM, NVP, DEAEM/Nelfilcon A/Irgacure 2959; UV, 45 s | PVA-based commercial formulation/CL (127 μm) Swollen polymer volume fractions: 0.23–0.29 | Not reported | Sustained release for 48 h (release rate: 12 μg/h in the first 6–10 h, and nearly liner release profile at a rate of 4 μg/h in the next 10 to 30 h) | Material characterization In vitro release studies: method–sink method, medium-artificial lacrimal solution (pH = 8), 35 °C | Receptor-inspired hydrogel (microdomains that resemble the binding sites in the cell-surface glycoprotein CD44) Hyaluronic acid diffusion coefficients and release profiles can be significantly altered by the changes in mass content and by the relative proportions of functional monomers | [57] |
| HPMC | Non-covalent imprinting; AA/PEG200DMA, EGDMA/Darocur 1173; UV, 1.5 min | Lotrafilcon B, commercial silicone hydrogel lens (Silicon hydrogel macromer, TRIS and DMA)/CL (350 μm) Water content: 33% | Not reported | Sustained release - 1000 μg of HPMC over a period of up to 60 days in a constant manner at a rate of 16 μg/day | Material characterization In vitro release studies: method–sink method, medium-deionized water (pH = 6.4), 34 °C | [58] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bodoki, A.E.; Iacob, B.-C.; Dinte, E.; Vostinaru, O.; Samoila, O.; Bodoki, E. Perspectives of Molecularly Imprinted Polymer-Based Drug Delivery Systems in Ocular Therapy. Polymers 2021, 13, 3649. https://doi.org/10.3390/polym13213649
Bodoki AE, Iacob B-C, Dinte E, Vostinaru O, Samoila O, Bodoki E. Perspectives of Molecularly Imprinted Polymer-Based Drug Delivery Systems in Ocular Therapy. Polymers. 2021; 13(21):3649. https://doi.org/10.3390/polym13213649
Chicago/Turabian StyleBodoki, Andreea E., Bogdan-C. Iacob, Elena Dinte, Oliviu Vostinaru, Ovidiu Samoila, and Ede Bodoki. 2021. "Perspectives of Molecularly Imprinted Polymer-Based Drug Delivery Systems in Ocular Therapy" Polymers 13, no. 21: 3649. https://doi.org/10.3390/polym13213649
APA StyleBodoki, A. E., Iacob, B.-C., Dinte, E., Vostinaru, O., Samoila, O., & Bodoki, E. (2021). Perspectives of Molecularly Imprinted Polymer-Based Drug Delivery Systems in Ocular Therapy. Polymers, 13(21), 3649. https://doi.org/10.3390/polym13213649