
Inter-Institutional Comparison of Personalized Risk Assessments for Second Malignant Neoplasms for a 13-Year-Old Girl Receiving Proton versus Photon Craniospinal Irradiation

Abstract
:1. Introduction
2. Methods and Materials
2.1. Patient and Treatment Objectives
2.1.1. Proton CSI

{kind=link}
{kind=link}
{kind=link}
| Proton CSI | LPA | MPA | UPA | RPO | LPO |
|---|---|---|---|---|---|
| Monitor Units | 2493 | 2594 | 2577 | 1349 | 1323 |
| Nominal injection beam energy (MeV) | 180 | 160 | 160 | 200 | 200 |
| Range in patient (cm H2O) | 14.2 | 10.9 | 11.4 | 15.3 | 15.8 |
| Nominal SOBP width (cm) | 7 | 6 | 5 | 16 | 16 |
| Gantry angle (°) | 180 | 180 | 180 | 255 | 105 |
| Couch rotation angle (°) | 0 | 0 | 0 | 2 | 358 |
| Air gap (cm) | 23 | 25 | 26 | 38 | 39 |
| Aperture block thickness (cm) | 6 | 4 | 4 | 6 | 6 |
| Pre-collimated field size (cm × cm) | 25 × 25 | 25 × 25 | 25 × 25 | 25 × 25 | 25 × 25 |
| Collimated field, major axis (cm) | 22.7 | 13.4 | 11.9 | 21.1 | 20.7 |
| Collimated field, minor axis (cm) | 6.1 | 4.8 | 5.5 | 16.7 | 16.9 |
2.1.2. Photon CSI
2.2. In-Field Equivalent Dose in Organs and Tissues
| Photon CSI | LPA | UPA | RL | LL |
|---|---|---|---|---|
| Monitor Units | 3008 | 2785 | 1245 | 1268 |
| Gantry angle (°) | 180 | 180 | 270 | 90 |
| Collimator angle (°) | 0 | 0 | 11 | 349 |
| X1 jaw (cm) | −4.4 | −2.9 | −9.3 | −10.9 |
| X2 jaw (cm) | 3.7 | 2.6 | 10.9 | 9.3 |
| Y1 jaw (cm) | −4.1 | −9.0 | −10.0 | −10.0 |
| Y2 jaw (cm) | 10.0 | 19.0 | 10.5 | 10.5 |
| Depth of calculation point (cm H2O) | 6.7 | 5.1 | 7.6 | 8.1 |
| Effective square (cm) | 8.5 | 7.4 | 17.3 | 17.3 |
| Source-to-skin distance (cm) | 100 | 100 | 92.9 | 92.7 |
2.3. Stray Radiation Equivalent Dose in Organs and Tissues from Proton CSI
2.4. Equivalent Dose in Organs and Tissues for Photon CSI
2.4.1. Approach 1: TPS Calculations
2.4.2. Approach 2: Volume-Weighted Average
2.4.3. Approach 3: Model-Based Estimate
2.5. Risks of SMN Incidence and Mortality
| Cancer Site | IT/HT (%/Sv) | MT/HT (%/Sv) |
|---|---|---|
| Stomach | 0.98 | 0.55 |
| Colon | 2.15 | 1.00 |
| Liver | 0.26 | 0.23 |
| Lung | 6.78 | 5.96 |
| Breast | 9.25 | 2.17 |
| Uterus | 0.49 | 0.11 |
| Ovary | 0.98 | 0.54 |
| Bladder | 2.07 | 0.58 |
| Thyroid | 3.25 | 0.33 |
| Leukemia | 0.80 | 0.52 |
| NMSC | 17.77 | 0.04 |
| Other solid | 6.82 | 2.93 |
3. Results
3.1. Absorbed Dose, RBE-Weighted Absorbed Dose, and Equivalent Dose
| HT (Sv) | ||||
|---|---|---|---|---|
| Organ or Tissue | Primary Protons | External Neutrons | Internal Neutrons | Total |
| Stomach | 0.01 | 0.34 | 0.14 | 0.49 |
| Colon | 0.08 | 0.27 | 0.11 | 0.46 |
| Liver | 0.39 | 0.38 | 0.12 | 0.89 |
| Lungs | 1.82 | 0.48 | 0.17 | 2.47 |
| Breasts | 0.00 | 0.32 | 0.07 | 0.39 |
| Uterus | 0.00 | 0.21 | 0.08 | 0.29 |
| Ovaries | 0.00 | 0.18 | 0.07 | 0.25 |
| Bladder | 0.00 | 0.13 | 0.06 | 0.19 |
| Thyroid | 0.45 | 0.44 | 0.31 | 1.20 |
| Red bone marrow | 4.41 | 0.24 | 0.14 | 4.79 |
| Skin | 2.40 | 0.27 | 0.12 | 2.79 |
| Remainder | 2.84 | 0.27 | 0.16 | 3.27 |
| Whole body | 2.52 | 0.27 | 0.15 | 2.94 |
| HT (Sv) | |||
|---|---|---|---|
| Organ or Tissue | TPS Only | Volume-Weighted Averaging Technique | TPS in-Field & Model Out-of-Field |
| Stomach | 9.48 | 9.48 | 9.73 |
| Colon | 6.12 | 6.12 | 6.82 |
| Liver | 4.64 | 4.64 | 5.33 |
| Lungs | 4.78 | 4.78 | 5.59 |
| Breasts | 0.72 | 0.72 | 1.57 |
| Uterus | 0.02 | 0.60 | 1.11 |
| Ovaries | 0.02 | 0.60 | 1.70 |
| Bladder | 0.03 | 0.60 | 1.10 |
| Thyroid | 16.75 | 16.75 | 16.75 |
| Red bone marrow | 5.49 | 5.49 | 5.88 |
| Skin | 2.58 | 2.58 | 2.80 |
| Remainder | 4.77 | 4.77 | 4.91 |
| Whole body | 4.53 | 4.53 | 4.64 |
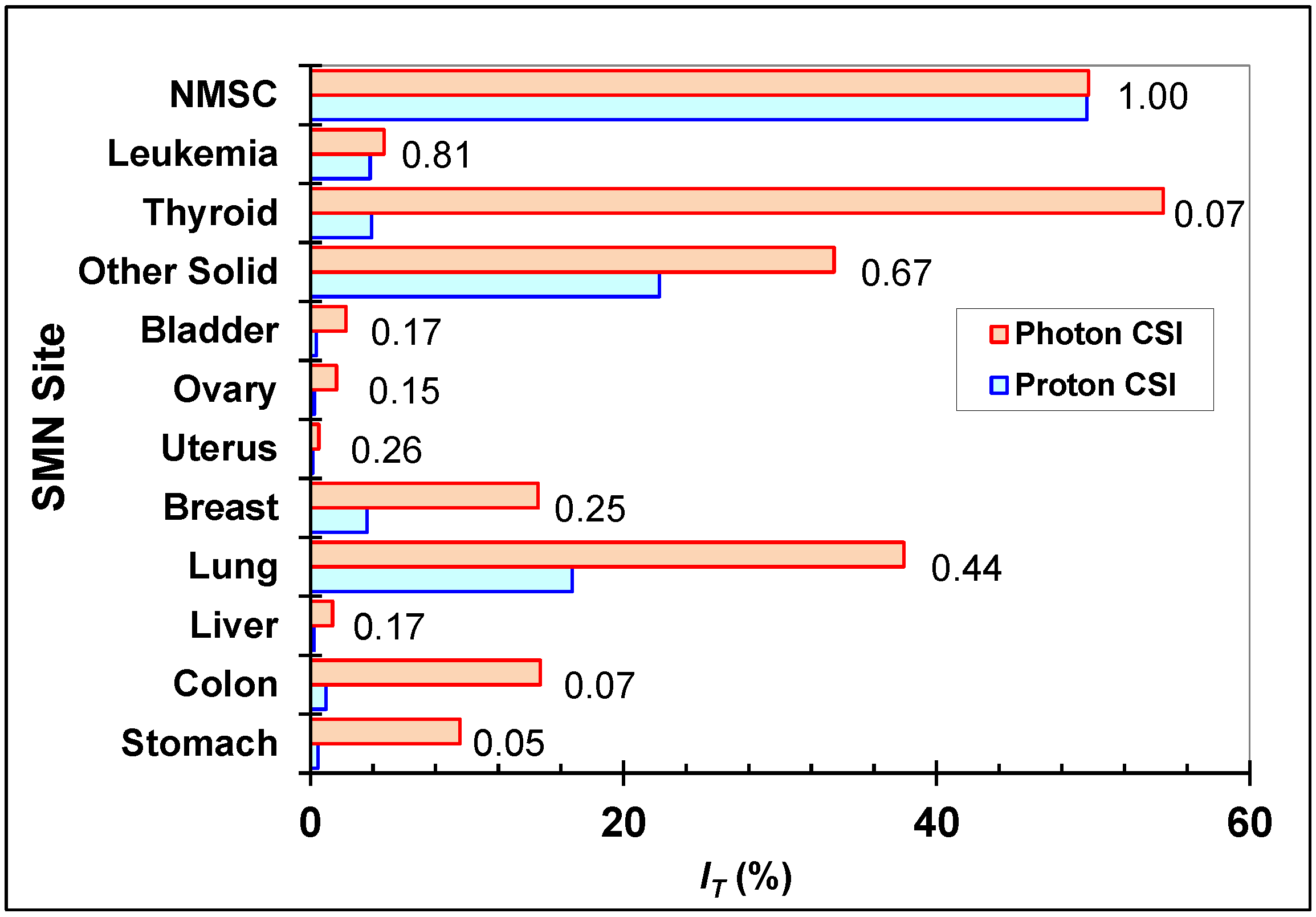
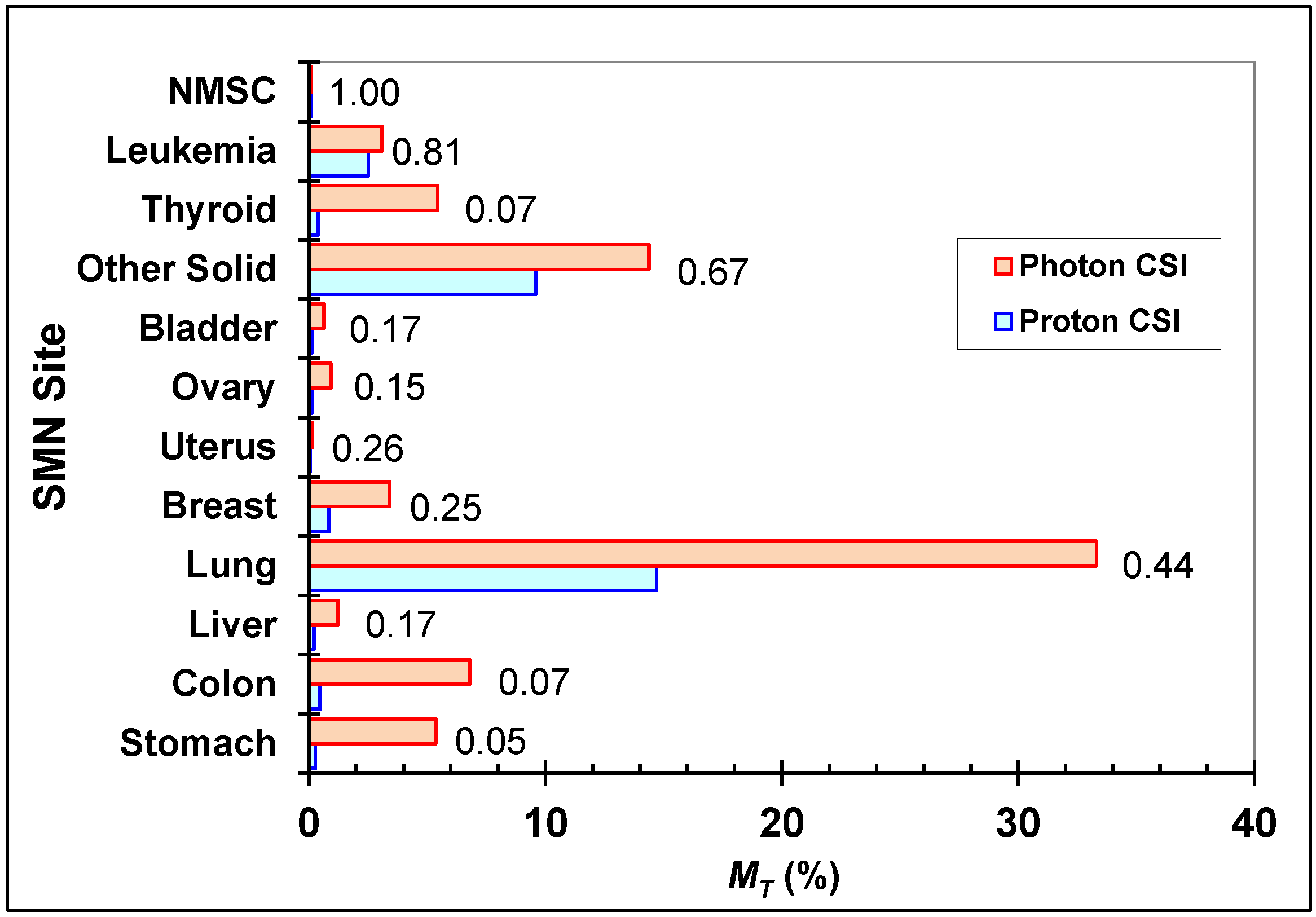
3.2. Risk of SMN Incidence and Mortality
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- Garcia, M.; Jemal, A.; Ward, E.M.; Center, M.M.; Hao, Y.; Siegel, R.L.; Thun, M.J. Global Cancer Facts & Figures 2007; American Cancer Society: Atlanta, GA, USA, 2007. [Google Scholar]
- Mahajan, A. Normal tissue complications from low-dose proton therapy. Health Phys. 2012, 103, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Merchant, T.E.; Farr, J.B. Proton beam therapy: A fad or a new standard of care. Curr. Opin. Pediatr. 2014, 26, 3–8. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2012; ACS: Atlanta, GA, USA, 2012. [Google Scholar]
- Mertens, A.C.; Liu, Q.; Neglia, J.P.; Wasilewski, W.; Armstrong, G.T.; Robison, L.L.; Yasui, Y. Cause-specific late mortality among 5-year survivors of childhood cancer: The Childhood Cancer Survivor Study. J. Natl. Cancer Inst. 2008, 100, 1368–1379. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.L.; Yock, T.I.; Mahajan, A.; Hill-Kaiser, C.; Keole, S.; Loredo, L.; Cahlon, O.; McMullen, K.P.; Hartsell, W.; Indelicato, D.J. Pediatric proton therapy: Patterns of care across the United States. Int. J. Part Ther. 2014, 1, 357–367. [Google Scholar] [CrossRef]
- Particle Therapy Co-Operative Group Website. Available online: http://ptcog.web.psi.ch/ptcentres.html (accessed on 20 January 2015).
- Taddei, P.J.; Mirkovic, D.; Fontenot, J.D.; Giebeler, A.; Zheng, Y.; Kornguth, D.; Mohan, R.; Newhauser, W.D. Stray radiation dose and second cancer risk for a pediatric patient receiving craniospinal irradiation with proton beams. Phys. Med. Biol. 2009, 54, 2259–2275. [Google Scholar] [CrossRef] [PubMed]
- Taddei, P.J.; Mahajan, A.; Mirkovic, D.; Zhang, R.; Giebeler, A.; Kornguth, D.; Harvey, M.; Woo, S.; Newhauser, W.D. Predicted risks of second malignant neoplasm incidence and mortality due to secondary neutrons in a girl and boy receiving proton craniospinal irradiation. Phys. Med. Biol. 2010, 55, 7067–7080. [Google Scholar] [CrossRef] [PubMed]
- Athar, B.S.; Paganetti, H. Comparison of second cancer risk due to out-of-field doses from 6-MV IMRT and proton therapy based on 6 pediatric patient treatment plans. Radiother. Oncol. 2011, 98, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Taddei, P.J.; Howell, R.M.; Krishnan, S.; Scarboro, S.B.; Mirkovic, D.; Newhauser, W.D. Risk of second malignant neoplasm following proton versus intensity-modulated photon radiotherapies for hepatocellular carcinoma. Phys. Med. Biol. 2010, 55, 7055–7065. [Google Scholar] [CrossRef]
- Zacharatou Jarlskog, C.; Paganetti, H. Risk of developing second cancer from neutron dose in proton therapy as a function of field characteristics, organ, and patient age. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 228–235. [Google Scholar]
- Newhauser, W.D.; Fontenot, J.D.; Mahajan, A.; Kornguth, D.; Stovall, M.; Zheng, Y.; Taddei, P.J.; Mirkovic, D.; Mohan, R.; Cox, J.D.; et al. The risk of developing a second cancer after receiving craniospinal proton irradiation. Phys. Med. Biol. 2009, 54, 2277–2291. [Google Scholar] [CrossRef]
- Brodin, N.P.; Munck Af Rosenschold, P.; Aznar, M.C.; Kiil-Berthelsen, A.; Vogelius, I.R.; Nilsson, P.; Lannering, B.; Bjork-Eriksson, T. Radiobiological risk estimates of adverse events and secondary cancer for proton and photon radiation therapy of pediatric medulloblastoma. Acta Oncol. 2011, 50, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Howell, R.M.; Taddei, P.J.; Giebeler, A.; Mahajan, A.; Newhauser, W.D. A comparative study on the risks of radiogenic second cancers and cardiac mortality in a set of pediatric medulloblastoma patients treated with photon or proton craniospinal irradiation. Radiother. Oncol. 2014, 113, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Miralbell, R.; Lomax, A.; Cella, L.; Schneider, U. Potential reduction of the incidence of radiation-induced second cancers by using proton beams in the treatment of pediatric tumors. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Stokkevag, C.H.; Engeseth, G.M.; Ytre-Hauge, K.S.; Rohrich, D.; Odland, O.H.; Muren, L.P.; Brydoy, M.; Hysing, L.B.; Szostak, A.; Palmer, M.B.; et al. Estimated risk of radiation-induced cancer following paediatric cranio-spinal irradiation with electron, photon and proton therapy. Acta Oncol. 2014, 53, 1048–1057. [Google Scholar] [CrossRef]
- Zhang, R.; Howell, R.M.; Giebeler, A.; Taddei, P.J.; Mahajan, A.; Newhauser, W.D. Comparison of risk of radiogenic second cancer following photon and proton craniospinal irradiation for a pediatric medulloblastoma patient. Phys. Med. Biol. 2013, 58, 807–823. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A. Proton craniospinal radiation therapy: Rationale and clinical evidence. Int. J. Part Ther. 2014, 1, 399–407. [Google Scholar] [CrossRef]
- Giebeler, A.; Newhauser, W.D.; Amos, R.A.; Mahajan, A.; Homann, K.; Howell, R.M. Standardized treatment planning methodology for passively scattered proton craniospinal irradiation. Radiat. Oncol. 2013, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Atlas of Global Development: A Visual Guide to the World’s Greatest Challenges, 4th Ed. ed; Collins: Glasgow, UK, 2013. [Google Scholar]
- Newhauser, W.; Fontenot, J.; Zheng, Y.; Polf, J.; Titt, U.; Koch, N.; Zhang, X.; Mohan, R. Monte Carlo simulations for configuring and testing an analytical proton dose-calculation algorithm. Phys. Med. Biol. 2007, 52, 4569–4584. [Google Scholar] [CrossRef] [PubMed]
- Howell, R.M.; Giebeler, A.; Koontz-Raisig, W.; Mahajan, A.; Etzel, C.J.; D’Amelio, A.M., Jr.; Homann, K.L.; Newhauser, W.D. Comparison of therapeutic dosimetric data from passively scattered proton and photon craniospinal irradiations for medulloblastoma. Radiat. Oncol. 2012, 7, 116. [Google Scholar] [CrossRef]
- Zheng, Y.; Newhauser, W.; Fontenot, J.; Taddei, P.; Mohan, R. Monte Carlo study of neutron dose equivalent during passive scattering proton therapy. Phys. Med. Biol. 2007, 52, 4481–4496. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Fontenot, J.; Taddei, P.; Mirkovic, D.; Newhauser, W. Monte Carlo simulations of neutron spectral fluence, radiation weighting factor and ambient dose equivalent for a passively scattered proton therapy unit. Phys. Med. Biol. 2008, 53, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Giebeler, A.; Langen, K.M.; Mirkovic, D.; Mohan, R. Can megavoltage computed tomography reduce proton range uncertainties in treatment plans for patients with large metal implants? Phys. Med. Biol. 2008, 53, 2327–2344. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Fontenot, J.D.; Mirkovic, D.; Hendricks, J.S.; Newhauser, W.D. Advantages of MCNPX-based lattice tally over mesh tally in high-speed Monte Carlo dose reconstruction for proton radiotherapy. Nucl. Technol. 2013, 183, 101–106. [Google Scholar] [PubMed]
- Pelowitz, D.B. MCNPX™ User’s Manual, Version 2.7.0.; Los Alamos National Laboratory: Los Alamos, NM, USA, 2011. [Google Scholar]
- Stankovskiy, A.; Kerhoas-Cavata, S.; Ferrand, R.; Nauraye, C.; Demarzi, L. Monte Carlo modelling of the treatment line of the Proton Therapy Center in Orsay. Phys. Med. Biol. 2009, 54, 2377–2394. [Google Scholar] [CrossRef] [PubMed]
- Newhauser, W.D.; Rechner, L.; Mirkovic, D.; Yepes, P.; Koch, N.C.; Titt, U.; Fontenot, J.D.; Zhang, R. Benchmark measurements and simulations of dose perturbations due to metallic spheres in proton beams. Radiat. Measur. 2013, 58, 37–44. [Google Scholar] [CrossRef]
- Law, M.Y.; Liu, B. Informatics in radiology: DICOM-RT and its utilization in radiation therapy. Radiographics 2009, 29, 655–667. [Google Scholar] [CrossRef] [PubMed]
- DICOM Standards Committee; Working Group 18 Clinical Trials. Digital Imaging and Communications in Medicine (DICOM) Supplement 142: Clinical Trial De-identification Profiles; National Electrical Manufacturers Association: Rosslyn, VA, USA, 2011. [Google Scholar]
- Newhauser, W.; Jones, T.; Swerdloff, S.; Newhauser, W.; Cilia, M.; Carver, R.; Halloran, A.; Zhang, R. Anonymization of DICOM electronic medical records for radiation therapy. Comput. Biol. Med. 2014, 53, 134–140. [Google Scholar] [CrossRef] [PubMed]
- ICRP. Relative biological effectiveness (RBE), quality factor (Q), and radiation weighting factor (wR): Publication 92. In Ann ICRP; Pergamon: New York, NY, USA, 2003; Volume 33. [Google Scholar]
- ICRP. Recommendations of the International Commission on Radiological Protection: Publication 60. In Ann ICRP; Pergamon Press: New York, NY, USA, 1991; Volume 21. [Google Scholar]
- ICRU. ICRU Report 49: Stopping Powers and Ranges for Protons and Alpha Particles; International Commission on Radiation Units and Measurements, Inc.: Bethesda, MD, USA, 1993. [Google Scholar]
- Howell, R.M.; Scarboro, S.B.; Kry, S.F.; Yaldo, D.Z. Accuracy of out-of-field dose calculations by a commercial treatment planning system. Phys. Med. Biol. 2010, 55, 6999–7008. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Followill, D.S.; Wang, X.A.; Kry, S.F. Accuracy and sources of error of out-of field dose calculations by a commercial treatment planning system for intensity-modulated radiation therapy treatments. J. Appl. Clin. Med. Phys. 2013, 14. [Google Scholar] [CrossRef]
- Spruijt, K.H.; Dahele, M.; Cuijpers, J.P.; Jeulink, M.; Rietveld, D.; Slotman, B.J.; Verbakel, W.F. Flattening filter free vs. flattened beams for breast irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Taddei, P.J.; Jalbout, W.; Howell, R.M.; Khater, N.; Geara, F.; Homann, K.; Newhauser, W.D. Analytical model for out-of-field dose in photon craniospinal irradiation. Phys. Med. Biol. 2013, 58, 7463–7479. [Google Scholar] [CrossRef] [PubMed]
- Howell, R.M.; Scarboro, S.B.; Taddei, P.J.; Krishnan, S.; Kry, S.F.; Newhauser, W.D. Methodology for determining doses to in-field, out-of-field and partially in-field organs for late effects studies in photon radiotherapy. Phys. Med. Biol. 2010, 55, 7009–7023. [Google Scholar] [CrossRef] [PubMed]
- NRCNAS. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII—Phase 2; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Meadows, A.T.; Friedman, D.L.; Neglia, J.P.; Mertens, A.C.; Donaldson, S.S.; Stovall, M.; Hammond, S.; Yasui, Y.; Inskip, P.D. Second neoplasms in survivors of childhood cancer: Findings from the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2009, 27, 2356–2362. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A. Why is IMPT a smart treatment option for pediatric patients? Avaliable online: http://www.proton-therapy.org/impt.html (accessed on 20 January 2015).
- Perkins, J.L.; Liu, Y.; Mitby, P.A.; Neglia, J.P.; Hammond, S.; Stovall, M.; Meadows, A.T.; Hutchinson, R.; Dreyer, Z.E.; Robison, L.L.; et al. Nonmelanoma skin cancer in survivors of childhood and adolescent cancer: A report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2005, 23, 3733–3741. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.T.; Liu, W.; Leisenring, W.; Yasui, Y.; Hammond, S.; Bhatia, S.; Neglia, J.P.; Stovall, M.; Srivastava, D.; Robison, L.L. Occurrence of multiple subsequent neoplasms in long-term survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2011, 29, 3056–3064. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.; Elliston, C.; Hall, E.; Berdon, W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am. J. Roentgenol. 2001, 176, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Pierce, D.A.; Shimizu, Y.; Preston, D.L.; Vaeth, M.; Mabuchi, K. Studies of the mortality of atomic bomb survivors. Report 12, Part I. Cancer: 1950–1990. Radiat Res. 1996, 146, 1–27. [Google Scholar] [CrossRef]
- UNSCEAR. Report of the United Nations Scientific Committee on the Effects of Atomic Radiation: Sixtieth Session (27–31 May 2013); New York, NY, USA, 2013. [Google Scholar]
- Department of Health; Public Health England; NHS England (including NHS Improving Quality). Improving Outcomes: A Strategy for Cancer-Third Annual Report; Crown: London, UK, 2010. [Google Scholar]
- Fontenot, J.D.; Bloch, C.; Followill, D.; Titt, U.; Newhauser, W.D. Estimate of the uncertainties in the relative risk of secondary malignant neoplasms following proton therapy and intensity-modulated photon therapy. Phys. Med. Biol. 2010, 55, 6987–6998. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J. The impact of protons on the incidence of second malignancies in radiotherapy. Technol. Cancer Res. Treat. 2007, 6, 31–34. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taddei, P.J.; Khater, N.; Zhang, R.; Geara, F.B.; Mahajan, A.; Jalbout, W.; Pérez-Andújar, A.; Youssef, B.; Newhauser, W.D. Inter-Institutional Comparison of Personalized Risk Assessments for Second Malignant Neoplasms for a 13-Year-Old Girl Receiving Proton versus Photon Craniospinal Irradiation. Cancers 2015, 7, 407-426. https://doi.org/10.3390/cancers7010407
Taddei PJ, Khater N, Zhang R, Geara FB, Mahajan A, Jalbout W, Pérez-Andújar A, Youssef B, Newhauser WD. Inter-Institutional Comparison of Personalized Risk Assessments for Second Malignant Neoplasms for a 13-Year-Old Girl Receiving Proton versus Photon Craniospinal Irradiation. Cancers. 2015; 7(1):407-426. https://doi.org/10.3390/cancers7010407
Chicago/Turabian StyleTaddei, Phillip J., Nabil Khater, Rui Zhang, Fady B. Geara, Anita Mahajan, Wassim Jalbout, Angélica Pérez-Andújar, Bassem Youssef, and Wayne D. Newhauser. 2015. "Inter-Institutional Comparison of Personalized Risk Assessments for Second Malignant Neoplasms for a 13-Year-Old Girl Receiving Proton versus Photon Craniospinal Irradiation" Cancers 7, no. 1: 407-426. https://doi.org/10.3390/cancers7010407
APA StyleTaddei, P. J., Khater, N., Zhang, R., Geara, F. B., Mahajan, A., Jalbout, W., Pérez-Andújar, A., Youssef, B., & Newhauser, W. D. (2015). Inter-Institutional Comparison of Personalized Risk Assessments for Second Malignant Neoplasms for a 13-Year-Old Girl Receiving Proton versus Photon Craniospinal Irradiation. Cancers, 7(1), 407-426. https://doi.org/10.3390/cancers7010407