Simple Summary
Tumors of the small bowel are rarely encountered and difficult to diagnose; the symptoms are nonspecific until the late stages. The introduction of videocapsule endoscopy and balloon- or spiral-assisted enteroscopy has improved the diagnosis, although many large tumors are still diagnosed by CT scan and in emergency settings. The most frequent malignant small bowel tumors are adenocarcinoma, lymphoma, GIST, and neuroendocrine tumors. We present a 7-year study of 80 small bowel tumors admitted to our clinic, of which 62.2% were primary malignant tumors and 10.3% were metastases. Adenocarcinoma represents the most frequent malignant tumor; two squamous carcinomas were diagnosed. The 5-year survival rate was 41%.
Abstract
(1) Background: Tumors of the small bowel represent 3–6% of gastrointestinal neoplasms and 3–6% of GI malignancies. The difficulties regarding the diagnosis are associated with larger tumors at the moment of the diagnosis and with advanced forms of malignant tumors, associated with a dismal prognosis. (2) Methods: We performed an observational, retrospective, cohort study that included patients with small bowel tumors admitted to the Craiova County Emergency Clinic Hospital between 1 January 2017 and 31 December 2023. The data were collected from the analysis of the patient’s discharge documents from the Hippocrates computer system of the hospital and the evaluation of endoscopy databases. Patients under 16 years of age, those with no pathological confirmation of the malignancy, and those with insufficient data were excluded. (3) Results: A total of 80 cases of small bowel tumors were diagnosed; 72.5% were malignant, of which 10.3% were metastases. The most frequent primary malignant small bowel tumor was adenocarcinoma; two squamous cell carcinomas were noted. CT scans and upper digestive endoscopy represent the most frequent imaging methods for the diagnosis. The prognosis for malignant tumors was poor, with a 41% 5-year survival rate. (4) Conclusions: Small bowel tumors are rarely encountered, with 72.5% being malignant, and were diagnosed at large dimensions and in advanced stages for malignant tumors, with a dismal prognosis.
1. Introduction
Tumors of the small bowel are relatively rare forms, accounting for 3–6% of gastrointestinal (GI) neoplasms [1,2,3,4]. An increased prevalence was noted in the last several decades, possibly associated with the progress in diagnostic procedures [5].
Several pathological types have been described in small bowel tumors (SBTs) [6]. Malignant tumors are more frequent [2] and include carcinomas (most frequently adenocarcinomas and rarely squamous cell carcinomas), neuroendocrine tumors, lymphomas, and sarcomas; intestinal stromal tumors and mesenchymal tumors are also often described [1,3,5,7,8,9,10,11]. Rare cases of primary squamous carcinomas [12,13,14,15,16,17,18,19,20,21,22,23] and leiomyosarcomas [24] have been noted. Metastatic small bowel tumors originating from colon, prostate, breast, and lung cancers, or from skin melanoma, have also been recorded [1,3,7,13].
The symptoms of patients with SBT are variable and sometimes correlated with the pathological type [7]. The most frequent complaints are nausea and/or vomiting, abdominal pain, bleeding, and weight loss [1,5,25,26]. Bleeding may be either overt (melena) or occult (anemia). Bowel obstruction (by the tumor or by intussusception), or sometimes perforations, are seen frequently [3,4,27,28,29]. This can sometimes even occur in benign SBT [30,31,32,33,34]. Emergency surgery may be needed; one study from Turkey found a rate of 17.6% for emergency procedures [5]. SBT represents the second cause of obscure gastrointestinal bleeding [4], and in various studies of patients with iron-deficient anemia, the rate of SBT after negative bidirectional endoscopy was reported in up to 8.9% of cases [3], with a pooled frequency of 1.25% in a systematic review [35]. Jejunal tumors are associated more frequently with bleeding, and ileal tumors with abdominal pain [2]. Nonspecific symptoms are usually associated with a six- to nine-month delay in diagnosis [1].
Survival rates for malignant SBT are hard to estimate because of the high variability of the tumor types. Some models involving Deep Learning or other types of artificial intelligence were studied [36].
The diagnosis can be difficult, especially in the mid-segment of the small bowel. Duodenal and sometimes jejunal tumors can be diagnosed by upper digestive endoscopy, while ileo-colonoscopy can be used for SBT in the terminal ileum. Enteroscopy (spiral, single-, or double-balloon enteroscopy) is very useful [4,37,38,39,40,41,42,43,44,45,46,47,48,49], as well as videocapsule enteroscopy (VCE). Anterograde combined with retrograde balloon enteroscopy can assess 70% of the small bowel [4], while motorized spiral enteroscopy can frequently evaluate the entire small bowel, sometimes by using only the anterograde (oral) route [4]. VCE introduction has revolutionized small bowel pathology diagnosis and foremost gastrointestinal bleeding with unclear etiology [50], as it is easy to perform, non-invasive, and does not need sedation. However, the rate of entire small bowel examinations ranges between 67 and 76.6% [51,52,53], and it cannot perform biopsies or therapeutic maneuvers [3]. Some lesions (especially gastrointestinal stromal tumors—GISTs, and tumors located in the duodenum or Treitz area) may be missed [48,54]. In two studies of 79 and 16 patients with SBT, 16.7% were missed by VCE [55,56]. Even large subepithelial lesions as large as 3 cm can be missed [57]. Capsule retention represents another disadvantage; even if rates of 3% are usually seen in normal investigations [53], in SBT, the retention rates go up to 10 or even 20% [54]. A meta-analysis comparing enteroscopy with VCE found a good sensitivity and specificity for enteroscopy (89% and 97%, respectively) [58]. The main advantage of enteroscopy is represented by the possibility of both biopsies and tattooing the lesions, which can help the surgeons to find the lesion [4]. Transabdominal ultrasound can sometimes visualize the tumor, but the sensitivity is only 50.5%, with 100% specificity [59]; in tumors above 2 cm in diameter, with circumferential extension or ulcerative pattern, the sensitivity increases above 90% [59]. Computed tomography (CT) scans or magnetic resonance imaging (MRI) have a higher accuracy; however, small tumors can be easily missed [1]. In a study of 79 SBTs, including 9 missed by VCE, the accuracy for CT scans was 55.8%, and for small bowel follow-through was 46.1% [55]. In another study of 16 neuroendocrine tumors, the detection rate for CT scans was 62.5% [56]. The use of CT or MRI enteroclysis [1,60] significantly increased the accuracy of SBT detection. Digital angiography can be useful in small SBTs with active bleeding [61].
Because subepithelial lesions of the small bowel tract can be missed on VCE examination, a score named SPICE (Smooth, Protruding Lesion Index of Capsule Endoscopy) was proposed, which includes four criteria: mass with ill-defined boundaries, with a diameter larger than its height, non-visible lumen, and mass image visible for less than 10 min [4,48]. Another score proposed for the probability of a mass lesion at VCE examination includes bleeding, mucosal disruption, irregular surface, white villi, and color [62]; a score of four or more was associated with a high probability of a small bowel mass lesions, while a score of two or less was associated with a low likelihood [62]. Artificial intelligence may aid VCE accuracy for SBT detection [63,64], with a significantly reduced time for examination (average 4.5 min), a sensitivity as high as 98–99%, and an error in diagnosis below 3% [64].
Our study was designed to fill the existing literature gaps regarding small bowel tumors in Romania by assessing the prevalence, diagnosis, pathological types, and prognosis of benign and malignant small bowel tumors in patients admitted between January 2017 and December 2023 in a tertiary care hospital. Several studies in Eastern and Southern Europe have assessed the prevalence of small bowel tumors [5,10,29,37,65,66,67], but some included only small series [66], only surgical cases [10,29,65,66,67], or were limited to malignant tumors [5,10,66]. Given the paucity of data regarding small bowel tumors in Eastern and Southern Europe, a study presenting an analysis of both benign and malignant small bowel tumors in Romania helps to describe the epidemiology of SBT, and by including cases without surgical management, we can better estimate survival analysis in malignant small bowel tumors.
2. Materials and Methods
2.1. Patient Selection
We conducted an observational, retrospective, cohort study that included patients with small bowel tumors admitted to the Craiova County Emergency Clinic Hospital between 1 January 2017 and 31 December 2023. Data were collected from the Hippocrates (Romanian Soft Company, Bucharest, Romania) digital registration system of the hospital with diagnostic codes of definite or possible small bowel tumors (C17.0—malignant duodenal tumor; C17.1—malignant jejunal tumor; C17.2—malignant ileal tumor; C17.8—malignant tumor surpassing small bowel; C17.9—malignant small bowel tumors, unprecise; D01.7—carcinoma in situ of other specified digestive organs; D13.3—benign small bowel tumors; D37.2—small bowel tumors with unspecified and unknown evolution; D37.7 and D37.9—other digestive tumors with unspecified and unknown evolution), as well as K56 (paralytic ileus and intestinal obstruction without hernia), and were supplemented as needed by analyzing the patient medical records. Patients under 16 years of age, with no pathological confirmation of the malignancy, or incomplete records were excluded.
The diagnosis of small bowel tumors was based on clinical data; digestive endoscopy—upper digestive endoscopy, push enteroscopy, or ileo-colonoscopy performed exclusively on an Olympus Exera III system (Olympus Europe, Hamburg, Germany) and videocapsule endoscopy (Olympus EndoCapsule, Olympus Europe, Hamburg, Germany); and imaging—CT scan (Siemens Somatom go. TOP 128 slice reconstructed, Siemens Healthineers, Erlangen, Germany), MR imaging (Siemens—Magnetom Symphony 1,5T, Siemens Healthineers, Erlangen, Germany), or incidentally during abdominal surgery. It was then confirmed by pathology examination of endoscopically resected tumors (performed in the Gastroenterology Department) or surgically resected specimens, or by intraoperative biopsy in one of the three surgery departments of the hospital (in case of inoperable lesions). Only small bowel tumors with confirmed histopathology were included. The symptoms, along with the presence of complications, were recorded. The CT scan and MR imaging noted the dimensions of the lesion (if the lesion was seen), the parietal thickening, the retrograde dilation of the small bowel or the stomach, and the presence or absence of invaded lymph nodes, as well as distant metastases.
The diagnosis was confirmed in all patients by histopathological exam (with detailed information related to the benign or malignant type of tumor and also to the epithelial or mesenchymal origin, grading, lymphovascular or perineural invasion, and pTNM classification in malignant tumors); immunohistochemical evaluation was performed in a subgroup of the patients. The tumor stage was evaluated using the 8th edition of the “TNM Malignant Tumor Classification” from the International Cancer Control Union [68]. The immunohistochemical panel applied includes markers for squamous cell carcinoma, malignant melanoma (Melan A, HIMB45), the evaluation of endothelial differentiation (CD31, CD34), or the tumor proliferation index Ki-67. Final TNM staging, grading, and vascular and perineural invasion were also analyzed.
This study was approved by the Clinical County Emergency Hospital of Craiova Ethics Committee (Approval Number 17886/24 April 2024) on the following information: (1) data were collected within a retrospective, observational study; (2) the study did not interfere with current medical care; (3) data were collected and analyzed anonymously so that the patient data confidentiality would not be breached.
2.2. Data Collection and Statistical Analysis
The extracted data were processed in Microsoft Excel (Microsoft Corp., Redmond, WA, USA), with the XLSTAT 2016 add-on for MS Excel (Addinsoft SARL, Paris, France). The frequencies are presented as absolute numbers of cases and percentages. Survival analysis was performed using R software (version 4.3) with the survival and survminer packages. Survival analysis was performed using the Kaplan–Meier method to estimate survival probabilities, and differences between groups were assessed with the log-rank test. Cox proportional hazards regression models were used to evaluate the association between potential risk factors and survival outcomes. The multivariate Cox model included variables with a p-value < 0.05 in univariate analysis or clinical relevance. Hazard ratios (HRs) with 95% confidence intervals (CIs) are reported to quantify effect sizes.
3. Results
3.1. Main Characteristics of Patients
During the study period, 80 cases of small bowel tumors were admitted; 58 were malignant tumors and 22 were benign tumors (Figure 1). Mean age was similar for benign and malignant tumors (63.1 for benign and 64 for malignant tumors, p = 0.7614); male gender was predominant for both benign and malignant SBT. There was an almost equal distribution to the duodenum, jejunum, and ileum; five cases presented multiple tumors located in the small bowel.
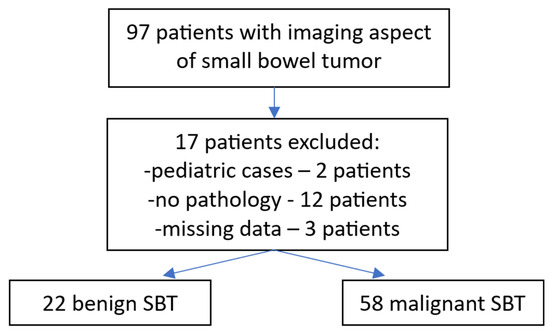
Figure 1.
A diagram showing the inclusion of patients and tumor types.
The most frequent symptoms at admission were abdominal pain and nausea with or without vomiting; complications were noted in 46.2% of cases (intestinal occlusion, bleeding, invagination, and perforation). In-hospital death was recorded in 10 cases (12.5%), being related to complications and advanced malignant diseases (Table 1).

Table 1.
Baseline characteristics of the studied cohort.
CT scans represent the most used investigation for the diagnosis of SBT (60%). In 81.3% of cases, the tumor was visible at the CT scan (Figure 2, Figure 3, Figure 4 and Figure 5); the mean diameter was 59.8 mm. The presence of lymph nodes was noted in one-third of malignant SBT cases, while metastases were present in 25.6%. Upper digestive endoscopy was performed in 34 cases (Figure 6 and Figure 7), with endoscopic resection in 6 cases; lower digestive diagnostic endoscopy was used in 12 cases. Transabdominal ultrasound was used in 21 cases; however, it detected SBT in only 19%. Videocapsule endoscopy was performed in only four cases, all with a negative CT scan and endoscopy.

Figure 2.
CT scan post-contrast with heterogeneous uptake and central necrosis, vascular peripheral enhancement, and regular contour, with no loco-regional extension. The pathology exam revealed an intestinal stromal tumor.
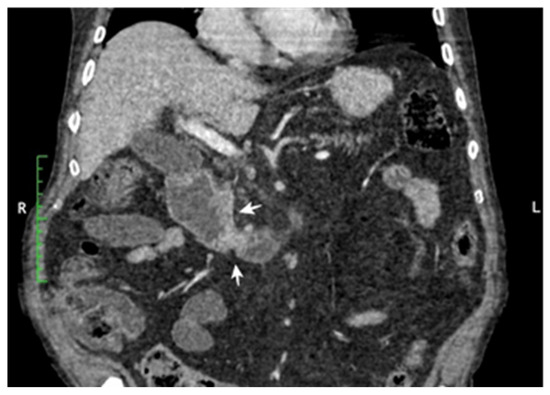
Figure 3.
Coronal CT reconstruction post-contrast: infiltrative tumor located on the upper part of the small bowel, with circumferential distribution. Small lymph nodes are visible. Pathology revealed duodenal adenocarcinoma.
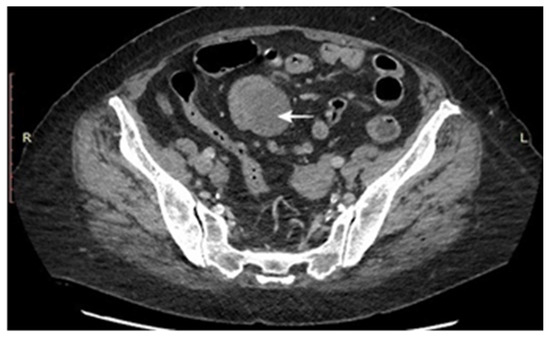
Figure 4.
CT scan: tumoral mass with ileal location and predominant extraluminal extension, ileal luminal stenosis and upstream dilation of the small bowel, moderate enhancement, and mesenteric fat infiltration. Several mesenteric lymph nodes up to 1.4 cm.

Figure 5.
CT post-contrast axial scan: heterogeneous mass at the level of jejunal loops, round-shaped, with regular contours. The pathology exam revealed a mesenchymal angiomatous tumor.
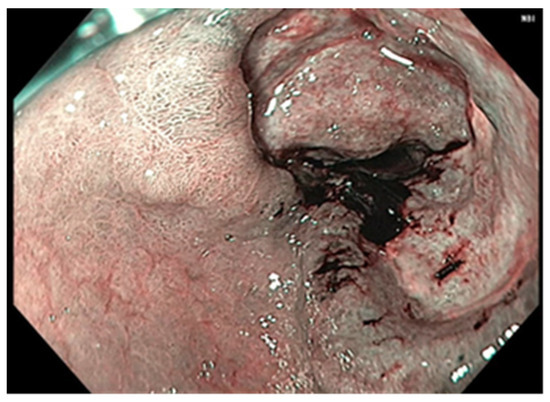
Figure 6.
Upper digestive endoscopy: duodenal carcinoma visible through the dilated pyloric orifice.
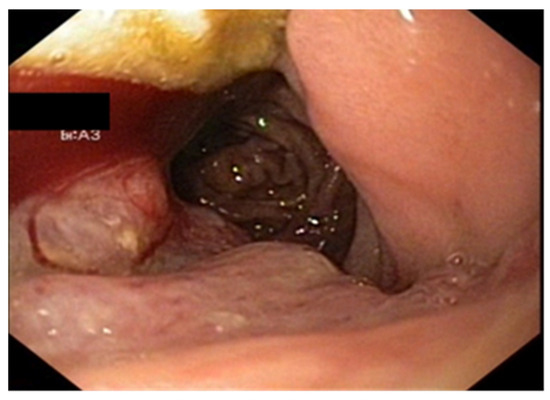
Figure 7.
Upper digestive endoscopy: visible carcinoma located on the second part of the duodenum.
Of 58 malignant tumors, 89.7% were primitive and 10.3% were metastases. Carcinoma represented the most frequent primitive malignant SBT (48.3%), with adenocarcinoma being the most encountered subtype, although we recorded two cases of squamous cell carcinomas of the small bowel. Lymphoma was the second primitive malignant SBT (13.8%), followed in equal proportion by neuroendocrine tumors and GISTs (10.3%).
3.2. Treatment Particularities
Endoscopic resections was performed in 7 cases of benign tumors (Figure 8 and Figure 9), while surgical resection was performed in 47 cases (Figure 10, Figure 11, Figure 12 and Figure 13). Internal or external derivations were needed in 10 cases; laparotomy with biopsy for confirmation was performed in 16 cases.
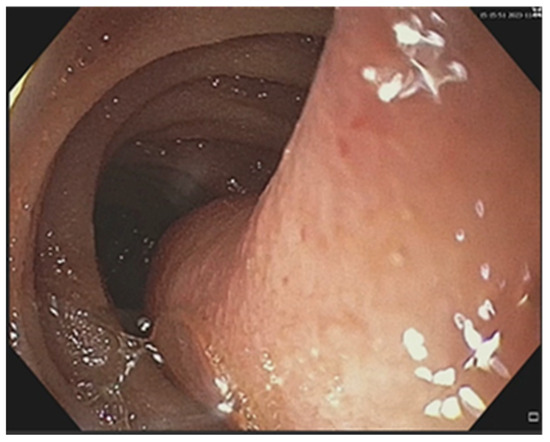
Figure 8.
Upper digestive endoscopy: pedunculated lipoma of the third part of the duodenum.
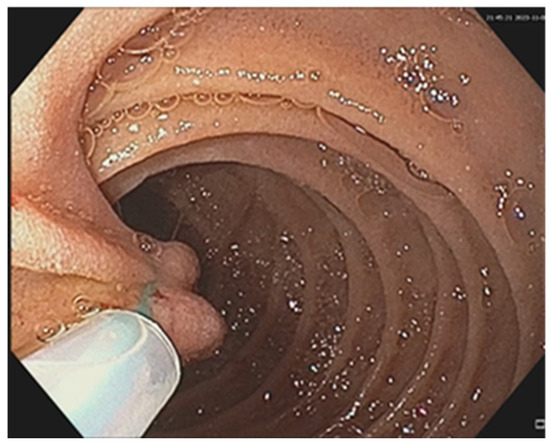
Figure 9.
Upper digestive endoscopy: same duodenal lipoma and the placement of an endoloop to the pedunculum, followed by resection.
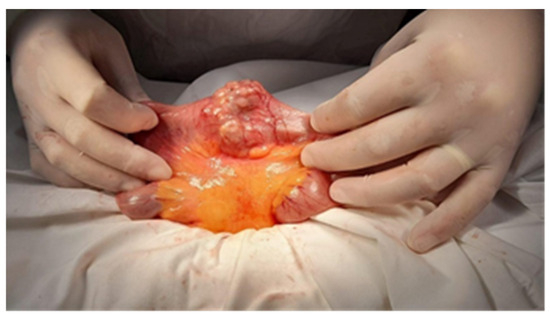
Figure 10.
Surgical intraoperative aspect: jejunal metastasis. The pathology exam revealed an ileal lymphoma.
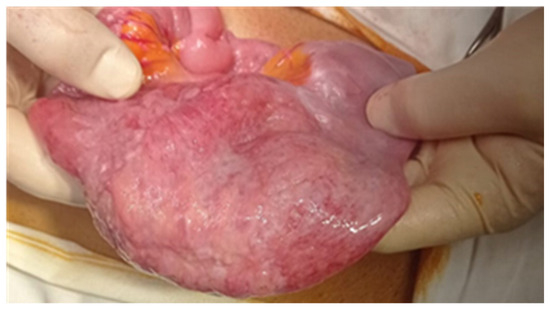
Figure 11.
Surgical intraoperative aspect of an ileal tumor.
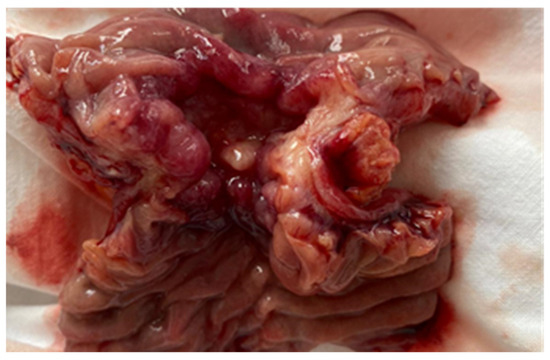
Figure 12.
The surgical intraoperative aspect of a jejunal stenosing tumor. Pathology examination revealed an adenocarcinoma.
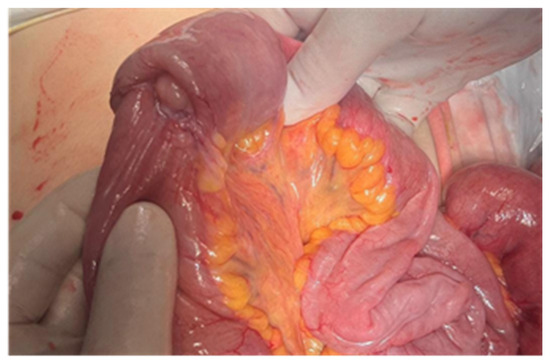
Figure 13.
Surgical intraoperative aspect of jejunal tumor complicated with invagination. Pathology examination has shown a carcinosarcoma.
3.3. Immunohistochemistry
Immunohistochemistry was performed in all gastrointestinal stromal tumors and revealed the presence of CD117, CD34, and DOG1 in all cases; alpha-actin was present as a vascular marker in one case and had a zonal distribution in another. Ki-67 was used for GIST classification according to the criterion of malignant potential. The diagnosis of intestinal lymphomas was confirmed by immunohistochemistry in dedicated hematological centers. For carcinomas, immunohistochemistry was performed in seven cases; two adenocarcinomas had both CD19 and CA 19-9 positivity, with CD10, S100, P53, CAIX positivity, and vimentin, tyrosine-kinase, and CD56 negativity in one case. CDX2 positivity was noted in all adenocarcinomas, while P63 positivity was noted in all squamous cell carcinomas and focally positive in adenocarcinomas with squamous differentiation (Figure 14, Figure 15, Figure 16, Figure 17, Figure 18 and Figure 19).
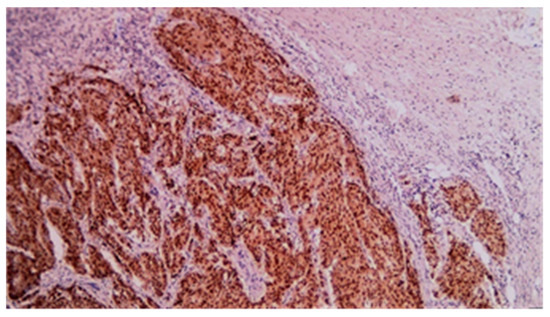
Figure 14.
CDX2 immunohistochemical staining of mixed adenocarcinoma–squamous carcinoma of the small bowel (20×).
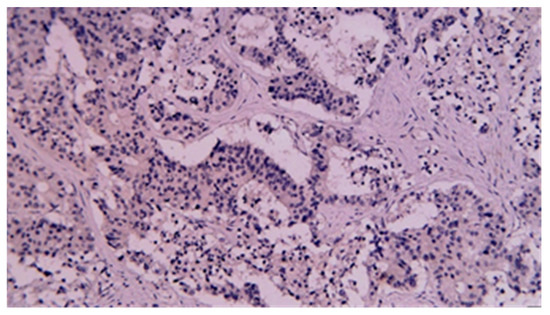
Figure 15.
P63 immunohistochemical staining of mixed adenocarcinoma–squamous carcinoma of the small bowel (20×).
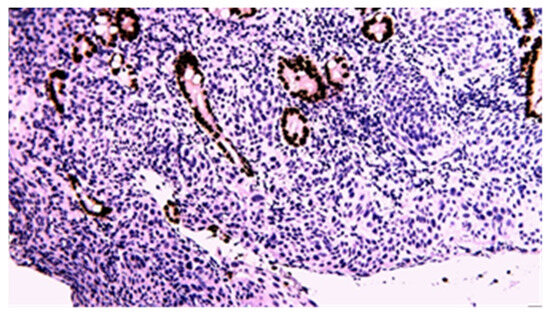
Figure 16.
CDX2 immunohistochemical staining of squamous carcinoma of the small bowel (20×).
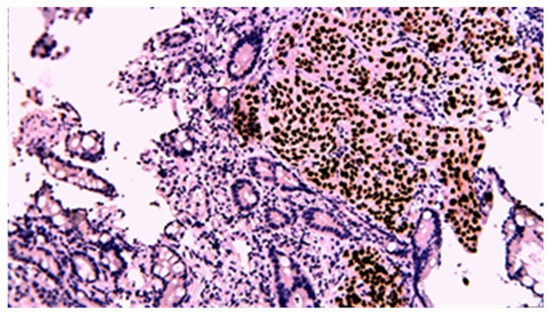
Figure 17.
P63 immunohistochemical staining of squamous cell carcinoma of the small bowel (20×).
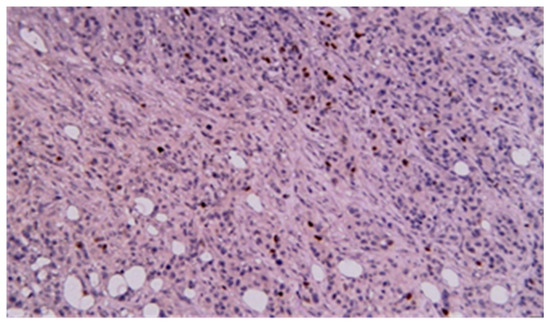
Figure 18.
CDX2 immunohistochemical staining of poorly differentiated carcinoma of the small bowel (20×).
Figure 19.
P63 immunohistochemical staining of poorly differentiated carcinoma of the small bowel (40×).
Of 28 patients with small bowel carcinoma, 3 died soon after surgery; 14 of 23 remaining patients had postoperative chemotherapy, and none had preoperative chemotherapy or radiotherapy. We had no therapeutic data regarding the other two cases of carcinoma, as well as for lymphomas, NETs, GISTs, and sarcomas.
3.4. Survival Analysis
Because carcinomas represented the most frequent malignant SBT, we evaluated the prognosis for all malignant SBT and among the three histological categories of small bowel tumors (carcinoma, metastases, and other tumors including lymphoma, sarcoma, GIST, and NET) by constructing the Kaplan–Meier curve (Figure 20 and Figure 21).
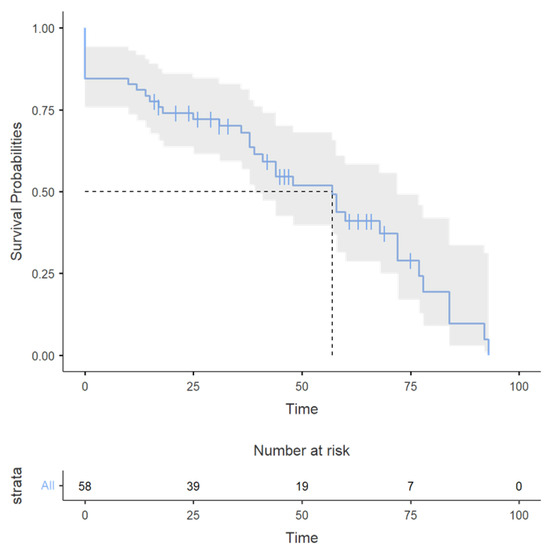
Figure 20.
The Kaplan–Meier curve for all SBT; the X-axis represents the time (months).
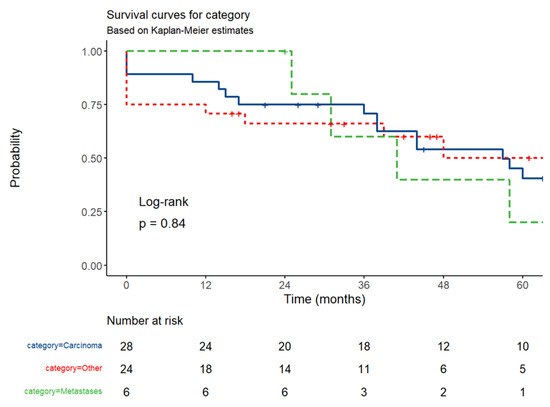
Figure 21.
The Kaplan–Meier curve for carcinomas, SB metastases, and other tumors (NET, lymphoma, sarcoma, GIST). The X-axis represents the time (months).
The number of survivors decreased over time in all categories (Figure 21); the decline was more gradual for carcinomas, steeper in later time points for NET, GISTs, lymphoma, and sarcoma, and faster after the third time-point for small bowel metastases. Despite these trends, the survival curves remained statistically indistinguishable. For carcinoma patients, 12-month survival was 86% (95%CI, 73.69–99.71%), 36-month survival was 71% (55.64–90.18%), and 60-month survival was 41% (25.03–65.93%). For patients with small bowel metastases, 12-month survival was 100%, 36-month survival was 60% (29.33–100%), and 60-month survival was 20% (3.46–100%). For the group of patients with lymphoma, sarcoma, NET, and GISTs, 12-month survival was 71% (54.80–91.57%), 36-month survival was 66% (49.46–88.37%), and 60-month survival was 50% (30.46–82.34%). The log-rank test revealed no statistically significant difference in survival between the groups (p = 0.84), possibly because of the small number of patients. Compared to carcinoma patients, patients with lymphomas, GISTs, and neuroendocrine tumors had a hazard ratio (HR) of 0.96 (95% CI: 0.47–1.93; p = 0.902), and those with small bowel metastases from other tumors had an HR of 1.29 (95% CI: 0.43–3.85; p = 0.648) relative to carcinoma patients, indicating no significant difference in risk.
After stratifying survival by tumor type, subgroup analysis revealed significant heterogeneity in median survival across tumor types. SARs had a numerically higher median survival (72 months) but with a CI spanning 0–NA, implying potential outliers or small sample size. Carcinoma had a median survival (57 months, 95% CI: 38–78). GIST and lymphoma showed intermediate outcomes (both 48 months), although lymphoma’s wide CI (0–NA) suggests uncertainty due to limited events. Small bowel metastases (41 months, CI: 31–NA) and NET (39 months, CI: 18–NA) had the poorest survival, with lower bounds of CIs indicating early risk. The median survival was 89 months for stage II carcinoma, 58 months for stage III, and 38 months for stage IV.
4. Discussion
In our study, malignant tumors represent 75% of the cases; primitive carcinomas were the most frequent malignant tumors (48.1%), followed by lymphomas, neuroendocrine tumors, stromal tumors, and six cases of metastatic small bowel tumors (three from melanoma, two from urothelial tumor, and one from pulmonary carcinoma). Most primitive carcinomas were adenocarcinomas (24/28 cases). In the literature, adenocarcinoma was the most frequent malignant SBT in most studies [2,5,10,69,70,71], whereas in other studies, small bowel stromal tumors were the most frequent [2,5,65], while lymphoma was almost equal to carcinoma in two studies [26,72]. Most of the small bowel tumors included were malignant, similar to the literature data [2,5,37,49,65,66]; some studies based on balloon-assisted enteroscopy have, however, shown a predominance of benign tumors [55]. Detailed data are provided in Supplementary Table S1.
The mean age was similar for benign and malignant tumors (63.1 for benign lesions and 64 years for malignant tumors, respectively); ages as young as 47 for benign tumors and 35 for malignant tumors were noted. The age distribution was also influenced by excluding pediatric patients, because cases of SBT, almost all benign, can also be encountered in patients under 18 years. Male gender was predominant in both benign (61.9%) and malignant small bowel tumors (62.3%). Most published studies have also noted a male predisposition for small bowel tumors [37,38,39,40,42,55], but others have not confirmed this [7,25,27,72].
Most patients with SBT have undergone radical or palliative surgery; endoscopic resection was performed in 7 cases. Perioperative death was noted in 10 cases (12.5%), 7 cases being associated with complications (4 with intestinal occlusion and 3 with severe bleeding), and the other 3 cases had advanced, unresectable malignant tumors. The most frequent causes for the lack of surgery were consent denial by the patient (10 cases), advanced diseases (8 cases, 7 with distant metastases and 1 with locally advanced disease), 2 cases with a diagnosis of lymphoma, and 1 case with acute cerebrovascular disease. Due to the presence of nonspecific symptoms, the diagnosis was frequently made in the advanced stages. An abdominal CT scan represents the main imaging method used for diagnosis in our patients, with a high detection rate (81.3%); most tumors were large at the moment of diagnosis, with only five cases having tumors between 20 and 30 mm. Upper and lower digestive endoscopy proved useful for tumors located in the duodenum and terminal ileum, respectively.
In our study, the survival of patients with small bowel malignant tumors and also of those with small bowel carcinoma was low, with a 41% 5-year overall survival rate (between 20 and 50% according to the tumor type). In the literature, 5-year survival rates of 20–30% are reported [1,6,26,73,74,75], but rates as low as 9% [76] and as high as 57.2% [70] have also been reported. In Romania, a study on operated patients with small bowel primitive carcinomas and 25 months’ median surveillance has shown a median survival of 13 months, and a 5-year survival of 30%, with an insufficient number of cases for statistically accurate differentiation between patients who received radical surgery and those with palliative treatment [10]. The mean overall survival and 5-year overall survival were lower in adenocarcinoma compared to NET and GIST [2,6,7,26,70]. The median overall survival in our study was 57 months for small bowel carcinomas, 48 months for GISTs and lymphomas, 72 months for sarcomas, and 57 months for all malignant SBT. The low 5-year survival rate in our study may be explained by the high rate of advanced disease (9/26 carcinomas, 3/6 NETs, 1/3 sarcomas, and 1/6 GISTs were stage IV tumors, while six cases were metastatic SBTs). Advanced small bowel carcinoma is associated with a dismal prognosis, with a median overall survival of 13.8 months and a 14.7% one-year survival rate [77].
Out of 28 patients with carcinoma, 2 had a primary squamous cell carcinoma of the small bowel (one being purely squamous cell carcinoma and the other having a mixed adenocarcinoma–squamous cell carcinoma type); another metastasis originated from a urothelial squamous cell carcinoma. Primitive squamous cell carcinomas of the small bowel are rarely encountered; a 2016 literature review found 22 cases [15]. WHO defined adenosquamous small bowel tumors as tumors including at least 10% adenocarcinoma and squamous cell carcinoma components [22]. Several possible patterns are described in the literature: aberrant differentiation of pluripotent stem cells to malignant squamous cells, the previous existence of a local ectopic squamous epithelium or squamous metaplasia with subsequent malignant transformation favored by chronic mucosal lesions [15,17,22,23]. Collision tumors or partial transformation from adenocarcinoma may explain the appearance of adenosquamous carcinoma [22]. It is difficult to differentiate between primary or metastatic squamous cell small bowel tumors. There are several criteria such as apparent atypia and nested distribution, the formation of a keratinized pearl, the lack of glandular components and glandular epithelium, and no evidence of involvement of primary SCC of other organs [17,18]. The presence of squamous metaplasia of the glandular epithelium favors the primary small bowel tumor if most of the cancer cells are deep in the wall of the SI, whereas in cases with little involvement of the mucosa, the metastatic nature of the lesion is more likely, especially if tumoral cells reach mucosal surfaces [18]. Both our patients were operated on and survived more than 5 years (one died at 78 months and another is still alive at 63 months); neither patient has followed postoperative chemotherapy. Clinicopathological characteristics, standardized therapy, and survival were hard to evaluate because of the rarity of the cases [15,22]; in one study, 66.7% of the squamous SB carcinomas died within one year after diagnosis (4/9 being metastatic tumors) [22], whereas in another review, from 22 patients, 16 cases were operated on, 4 and 3 were treated by chemotherapy and radiotherapy, and 54.5% died during follow-up [15].
There are several limitations to our study. Because of the rarity of SBT, our patient group was relatively small, which partially impaired the statistical analysis; the diverse type of tumors (benign or malignant, primitive or metastatic, carcinoma, lymphoma, sarcoma, NET, or GIST) further fragmented the patient groups and consequently impacted the statistical power of our analysis. While being difficult to conduct, a multicentric study may overcome the issues related to the small size; an extended timeframe may also be desired. However, changes in diagnostic and therapeutic modalities may render the study unsound for survival analysis. Two pediatric cases were excluded, both with benign tumors; most small bowel tumors in children are benign (infantile polyps, hamartoma, Peutz–Jeghers polyposis). Data related to lymphoma treatment were not available. Long-term survival (five years after the diagnosis) was impossible for patients admitted in the last three years of our study.
5. Conclusions
We diagnosed 80 small bowel tumors during the 7-year study period; 72.5% of small bowel tumors were malignant, the most frequent carcinoma, followed by lymphoma, GIST, and neuroendocrine tumors. Two squamous cell carcinomas were also noted. CT scans and upper digestive endoscopy were the main imaging investigations for the diagnosis. We found that 58.8% of tumors were resected surgically, and 9% by endoscopy. Survival was poor, with 5-year rates of 41% for carcinomas. Despite technical progress regarding diagnosis by videocapsule endoscopy, CT scan, and MRI, the early diagnosis and treatment of small bowel tumors is still difficult to achieve because of their nonspecific symptoms and the limitations of imaging methods for the diagnosis.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers17091465/s1, Table S1: Studies describing small bowel tumors.
Author Contributions
Conceptualization, S.M.C., M.M.F. and L.S.; methodology, S.M.C., V.M.S. and D.C.; software, D.C., B.S.U. and S.M.C.; validation, V.F.I., S.M. and V.M.S.; formal analysis, S.M.C. and D.C.; investigation, M.P., B.S.U., V.F.I. and M.C.; resources, M.P., L.S., C.S.M., V.M.S. and S.M.; data curation, S.M.C., L.S., C.S.M. and M.M.F.; writing—original draft preparation, S.M.C., D.C., M.P., L.S. and M.M.F.; writing—review and editing, S.M.C., D.C., C.S.M. and M.M.F.; visualization, S.M.C., M.C. and M.M.F.; supervision, L.S., V.M.S. and M.M.F.; project administration, S.M.C., L.S., and M.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
The article processing charges were funded by the University of Medicine and Pharmacy of Craiova, Romania.
Institutional Review Board Statement
This study was approved on 19 April 2023 by the Institutional Review Board (IRB) at the Clinical County Emergency Hospital of Craiova (Comisia de Etica a Spitalului Clinic Judetean de Urgentă Craiova) (Approval No. 18690/19.04.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cheung, D.Y.; Choi, M.-G. Current Advance in Small Bowel Tumors. Clin. Endosc. 2011, 44, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Kye, B.H.; Lee, J.I.; Kim, S.H.; Kim, H.J.; Kang, W.K.; Oh, S.T. Clinicopathological Features of Primary Jejunoileal Tumors. J. Korean Soc. Coloproctology 2010, 26, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, J.W. Small Bowel Malignancies in Patients Undergoing Capsule Endoscopy for Iron Deficiency Anemia. Diagnostics 2021, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- Safatle-Ribeiro, A.V.; Ribeiro, U., Jr. Impact of enteroscopy on diagnosis and management of small bowel tumors. Chin. J. Cancer Res. 2020, 32, 319–333. [Google Scholar] [CrossRef]
- Sahin, E. Emergent approach to small bowel tumors: Diagnosis and treatment. Turk. J. Trauma Emerg. Surg. 2024, 30, 155–159. [Google Scholar] [CrossRef]
- Pan, S.Y. Epidemiology of cancer of the small intestine. World J. Gastrointest. Oncol. 2011, 3, 33–42. [Google Scholar] [CrossRef]
- Cardoso, H.; Rodrigues, J.T.; Marques, M.; Ribeiro, A.; Vilas-Boas, F.; Santos-Antunes, J.; Rodrigues-Pinto, E.; Silva, M.; Maia, J.C.; Macedo, G. Malignant Small Bowel Tumors: Diagnosis, Management and Prognosis. Acta Medica Port. 2015, 28, 448–456. [Google Scholar] [CrossRef]
- Shah, P.P.; Kothari, S. Jejunal Adenocarcinoma—A Case Report with Review. Indian J. Surg. 2011, 75, 82–85. [Google Scholar] [CrossRef][Green Version]
- Krishnamurthy, P.; Varghese, S.E.; Gopalswamy, N.; Hillman, N.; Ali, S.A. Small-bowel adenocarcinoma: Case report and review of literature on diagnosis of small-bowel tumors. Gastroenterol. Hepatol. 2007, 3, 129–135. [Google Scholar]
- Obleagă, C.V.; Streba, C.T.; Mirea, C.S.; Vîlcea, I.D.; Florescu, D.N.; Ciorbagiu, M.C.; Turcu, T.; Florescu, M.M.; Șerbănescu, M.S.; Mehedințeanu, A.-M.; et al. Primitive Resectable Small Bowel Cancer Clinical–Pathological Analysis: A 10-Year Retrospective Study in a General Surgery Unit. Cancers 2024, 16, 3713. [Google Scholar] [CrossRef]
- Mirea, C.S.; Ciorbagiu, M.C.; Obleaga, C.V.; Moraru, E.; Mogoanta, S.S.; Ciurea, R.N.; Foarfa, M.C.; Vilcea, A.M.; Vilcea, I.D. Stage IV duodenal GIST requiring emergency pancreaticoduodenectomy—Diagnosis difficulties and therapeutic options. Rom. J. Morphol. Embryol. 2018, 59, 543–548. [Google Scholar] [PubMed]
- Nandedkar, S.; Trivedi, K.; Malukani, K.; Kk, T. Primary squamous cell carcinoma of the small intestine. J. Cancer Res. Ther. 2013, 9, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Terada, T. Malignant tumors of the small intestine: A histopathologic study of 41 cases among 1,312 consecutive specimens of small intestine. Int. J. Clin. Exp. Pathol. 2012, 5, 203–209. [Google Scholar] [PubMed]
- Mumtaz, S.; Ahmad, Z.; Fatima, S.; Qureshi, A. Squamous cell carcinoma in the small intestine. BMJ Case Rep. 2011, 2011, bcr0120113762. [Google Scholar] [CrossRef]
- Wang, F.-D.; Wang, Z.-W.; Xue, H.-D.; Wu, H.-W.; Zhang, Y.; Yu, J.-C.; Jin, Z.-Y. Primary Squamous Cell Carcinoma of the Small Intestine. Chin. Med. J. 2016, 129, 2131–2133. [Google Scholar] [CrossRef]
- Platt, C.C.; Haboubi, N.Y.; Schofield, P.F. Primary squamous cell carcinoma of the terminal ileum. J. Clin. Pathol. 1991, 44, 253–254. [Google Scholar] [CrossRef]
- Xiao, L.; Sun, L.; Zhang, J.-X.; Pan, Y.-S. Rare squamous cell carcinoma of the jejunum causing perforated peritonitis: A case report. World J. Gastrointest. Oncol. 2022, 14, 2295–2301. [Google Scholar] [CrossRef]
- Sun, D.S.; Shin, O.R.; Ku, Y.M.; Kim, Y.-S.; Seo, K.-J. Squamous cell carcinoma of the small bowel manifesting as a jejunal perforation: A case report. Int. J. Clin. Exp. Pathol. 2014, 7, 6345–6349. [Google Scholar]
- Soni, S.; Elhence, P.; Varshney, V.K.; Suman, S. Primary squamous cell carcinoma of the ampulla of Vater: Management and review of the literature. BMJ Case Rep. 2021, 14, e236477. [Google Scholar] [CrossRef]
- Bolanaki, H.; Giatromanolaki, A.; Sivridis, E.; Karayiannakis, A.J. Primary squamous cell carcinoma of the ampulla of Vater. JOP 2014, 15, 42–45. [Google Scholar] [CrossRef]
- Battal, M.; Bostancı, O.; Basak, T.; Kartal, K.; Ekiz, F. Pure Squamous Cell Carcinoma of the Duodenum. Case Rep. Surg. 2015, 2015, 714640. [Google Scholar] [CrossRef] [PubMed]
- Funamizu, N.; Nakabayashi, Y.; Dairaku, K.; Tomori, K.; Hiramoto, Y.; Kurihara, K. Intestinal obstruction caused by primary adenosquamous cell carcinoma of the small intestine: A case report and review of the literature. Mol. Clin. Oncol. 2018, 10, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Kumar, A.; Gowda, V.; Sahai, R.; Kumar, S.; Kishore, S. An adding up of an exceptionally rare case report: Primary Squamous cell carcinoma of Jejunum from North India. J. Cancer Res. Ther. 2023, 19, S451–S453. [Google Scholar] [CrossRef]
- Jadhav, M.; Nivash, T.H. Unveiling a Jejunal Leiomyosarcoma Presenting as a Gastrointestinal Stromal Tumor: A Case Report. Cureus 2024, 16, e66973. [Google Scholar] [CrossRef]
- Mitchell, K.J.; Williams, E.S.; Leffall, L.D. Primary malignant small bowel tumors: An atypical abdominal emergency. J. Natl. Med. Assoc. 1995, 87, 276–279. [Google Scholar]
- Farhat, M.H.; Shamseddine, A.I.; Barada, K.A. Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcome in 33 Patients in a Tertiary Care Center. J. Oncol. 2008, 2008, 212067. [Google Scholar] [CrossRef]
- Beltran, M.A.; Cruces, K.S. Primary tumors of jejunum and ileum as a cause of intestinal obstruction: A case control study. Int. J. Surg. 2007, 5, 183–191. [Google Scholar] [CrossRef]
- Kogo, H.; Shimanuki, K.; Iwao, T.; Yoshida, H. Small bowel GIST with hemorrhagic shock diagnosed by capsule endoscopy and double-balloon endoscopy, angiography-guided hemostasis, and laparoscopic-assisted resection. Clin. Case Rep. 2021, 9, e04240. [Google Scholar] [CrossRef]
- Turan, M.; Karadayi, K.; Duman, M.; Ozer, H.; Arici, S.; Yildirir, C.; Koçak, O.; Sen, M. Small bowel tumors in emergency surgery. Ulus. Travma Acil Cerrahi Derg. 2010, 16, 327–333. [Google Scholar]
- Chou, J.-W.; Feng, C.-L.; Lai, H.-C.; Tsai, C.-C.; Chen, S.-H.; Hsu, C.-H.; Cheng, K.-S.; Peng, C.-Y.; Chung, P.-K. Obscure Gastrointestinal Bleeding Caused by Small Bowel Lipoma. Intern. Med. 2008, 47, 1601–1603. [Google Scholar] [CrossRef]
- Al-Swaiti, G.T.; Al-Qudah, M.H.; Al-Doud, M.A.; Al-Bdour, A.R.; Al-Nizami, W. Spontaneous perforation of jejunal gastrointestinal stromal tumor: A case report. Int. J. Surg. Case Rep. 2020, 73, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Livengood, J.C.; Fenoglio, M.E. Gastrointestinal Hemorrhage from a Small Bowel Polypoid Hemangioma. JSLS J. Soc. Laparoendosc. Surg. 2002, 6, 179–180. [Google Scholar]
- Gil Heo, T. Solitary jejunal cavernous hemangioma causing intermittent melena: A case report. Int. J. Surg. Case Rep. 2021, 84, 106121. [Google Scholar] [CrossRef]
- Abboud, B. Vanek’s tumor of the small bowel in adults. World J. Gastroenterol. 2015, 21, 4802–4808. [Google Scholar] [CrossRef]
- Rockey, D.C.; Altayar, O.; Falck-Ytter, Y.; Kalmaz, D. AGA Technical Review on Gastrointestinal Evaluation of Iron Deficiency Anemia. Gastroenterology 2020, 159, 1097–1119. [Google Scholar] [CrossRef]
- Yin, M.; Lin, J.; Liu, L.; Gao, J.; Xu, W.; Yu, C.; Qu, S.; Liu, X.; Qian, L.; Xu, C.; et al. Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study. Diagnostics 2022, 12, 1247. [Google Scholar] [CrossRef]
- Dolu, S.; Onem, S.; Htway, Z.; Hajıyev, F.; Bilgen, A.; Binicier, H.C.; Kalemoglu, E.; Sagol, O.; Akarsu, M. Endoscopic and histological characteristics of small bowel tumors diagnosed by double-balloon enteroscopy. Clin. Endosc. 2023, 56, 83–91. [Google Scholar] [CrossRef]
- Zhang, C.; Hong, L.; Zhang, T.; Sun, P.; Sun, J.; Zhou, J.; Wang, L.; Fan, R.; Wang, Z.; Cheng, S.; et al. Clinical characteristics of small bowel tumors diagnosed by double-balloon endoscopy: Experience from a Chinese tertiary hospital. Turk. J. Gastroenterol. 2020, 31, 30–35. [Google Scholar] [CrossRef]
- Robles, E.P.-C.; Delgado, P.E.; Conesa, P.B.; Andrés, B.M.; Guggiana, M.F.; Mateos, E.A.; Caballero, M.F.; Agudo, J.L.R.; Martínez, S.C.; Latorre, R.; et al. Role of double-balloon enteroscopy in malignant small bowel tumors. World J. Gastrointest. Endosc. 2015, 7, 652–658. [Google Scholar] [CrossRef]
- Chung, C.-S.; Tai, C.-M.; Huang, T.-Y.; Chang, C.-W.; Chen, K.-C.; Tseng, C.-M.; Wang, H.-Y.; Chu, C.-H.; Wu, J.-M.; Chen, Y.; et al. Small bowel tumors: A digestive endoscopy society of Taiwan (DEST) multicenter enteroscopy-based epidemiologic study. J. Formos. Med. Assoc. 2018, 117, 705–710. [Google Scholar] [CrossRef]
- Ko, M.; Yen, C.; Yen, H. Obscure gastrointestinal bleeding with negative abdominal computed tomography study: The importance of enteroscopy for early diagnosis of small bowel malignancy. JGH Open 2019, 4, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, J.S.; Song, J.H.; Nam, K.; Kim, S.-E.; Jeong, E.S.; Kim, J.H.; Jeon, S.R. Discordance Rate and Risk Factor of Other Diagnostic Modalities for Small Bowel Tumors Detected by Device-Assisted Enteroscopy: A Korean Association for the Study of Intestinal Disease (KASID) Multicenter Study. Gut Liver 2024, 18, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Yin, A.; Yin, A.; Hu, W.; Hu, W.; Zhao, L.; Zhao, L.; Ding, Y.; Ding, Y.; Yu, H.; Yu, H. Diagnosis and therapy using double-balloon endoscopy for small bowel disease: Experience from a Chinese tertiary hospital. J. Int. Med. Res. 2020, 48, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B. Application of double-balloon enteroscopy for small bowel tumors. Clin. Endosc. 2023, 56, 53–54. [Google Scholar] [CrossRef]
- Nishimura, N.; Mizuno, M.; Shimodate, Y.; Doi, A.; Mouri, H.; Matsueda, K.; Yamamoto, H. The Role of Double-balloon Enteroscopy in the Diagnosis and Surgical Treatment of Metastatic Small Bowel Tumors. Intern. Med. 2018, 57, 1209–1212. [Google Scholar] [CrossRef]
- Banciu, C.; Munteanu, A.; Aprotosoaie, A.; Fabian, R.; Dobrescu, A.; Vaduva, A.; Fabian, A.; Soica, I.; Ivan, V.; Sima, L. Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review. Diagnostics 2024, 14, 904. [Google Scholar] [CrossRef]
- Chen, W.-G. Double-balloon enteroscopy in small bowel tumors: A Chinese single-center study. World J. Gastroenterol. 2013, 19, 3665–3671. [Google Scholar] [CrossRef]
- Fantasia, S.; Valdivia, P.C.; Kayali, S.; Koulaouzidis, G.; Pennazio, M.; Koulaouzidis, A. The Role of Capsule Endoscopy in the Diagnosis and Management of Small Bowel Tumors: A Narrative Review. Cancers 2024, 16, 262. [Google Scholar] [CrossRef]
- Vere, C.C.; Foarfă, C.; Streba, C.T.; Cazacu, S.; Pârvu, D.; Ciurea, T. Videocapsule endoscopy and single balloon enteroscopy: Novel diagnostic techniques in small bowel pathology. Rom. J. Morphol. Pathol. 2009, 50, 467–474. [Google Scholar]
- Pongprasobchai, S.; Chitsaeng, S.; Tanwandee, T.; Manatsathit, S.; Kachintorn, U. Yield, etiologies and outcomes of capsule endoscopy in Thai patients with obscure gastrointestinal bleeding. World J. Gastrointest. Endosc. 2013, 5, 122–127. [Google Scholar] [CrossRef]
- Zagorowicz, E.S. Small bowel tumors detected and missed during capsule endoscopy: Single center experience. World J. Gastroenterol. 2013, 19, 9043–9048. [Google Scholar] [CrossRef] [PubMed]
- Cheung, D.Y.; Kim, J.S.; Shim, K.-N.; Choi, M.-G.; Korean Gut Image Study Group. The Usefulness of Capsule Endoscopy for Small Bowel Tumors. Clin. Endosc. 2016, 49, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.J.; Lee, O.Y.; Jeen, Y.T.; Lim, C.Y.; Cheung, D.Y.; Cheon, J.H.; Ye, B.D.; Song, H.J.; Do, J.H.; Lee, K.J.; et al. Indications for Detection, Completion, and Retention Rates of Small Bowel Capsule Endoscopy Based on the 10-Year Data from the Korean Capsule Endoscopy Registry. Clin. Endosc. 2015, 48, 399–404. [Google Scholar] [CrossRef]
- Kim, E.R. Roles of Capsule Endoscopy and Device-Assisted Enteroscopy in the Diagnosis and Treatment of Small-Bowel Tumors. Clin. Endosc. 2020, 53, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Han, J.W.; Hong, S.N.; Jang, H.J.; Jeon, S.R.; Cha, J.M.; Park, S.J.; Byeon, J.S.; Ko, B.M.; Kim, E.R.; Choi, H.; et al. Clinical Efficacy of Various Diagnostic Tests for Small Bowel Tumors and Clinical Features of Tumors Missed by Capsule Endoscopy. Gastroenterol. Res. Pr. 2015, 2015, 623208. [Google Scholar] [CrossRef]
- Shyung, M.G.; Green, J.; Min, M.; Schlieve, C.R.; Patel, K.; Cahan, M.; Cave, D. Carcinoids and Capsules: A Case Series Highlighting the Utility of Capsule Endoscopy in Patients With Small Bowel Carcinoids. Gastroenterol. Res. 2017, 10, 347–351. [Google Scholar] [CrossRef]
- Ribeiro, I.; Pinho, R.; Rodrigues, A.; Fernandes, C.; Silva, J.; Ponte, A.; Tente, D.; Carvalho, J. The Importance of Alternative Diagnostic Modalities in the Diagnosis of Small Bowel Tumors After a Negative Capsule Endoscopy. GE Port. J. Gastroenterol. 2015, 22, 112–116. [Google Scholar] [CrossRef]
- Sulbaran, M.; de Moura, E.; Bernardo, W.; Morais, C.; Oliveira, J.; Bustamante-Lopez, L.; Sakai, P.; Mönkemüller, K.; Safatle-Ribeiro, A. Overtube-assisted enteroscopy and capsule endoscopy for the diagnosis of small-bowel polyps and tumors: A systematic review and meta-analysis. Endosc. Int. Open 2016, 04, E151–E163. [Google Scholar] [CrossRef]
- Fujita, M.; Manabe, N.; Honda, K.; Murao, T.; Osawa, M.; Kawai, R.; Akiyama, T.; Shiotani, A.; Haruma, K.; Hata, J. Usefulness of Ultrasonography for Diagnosis of Small Bowel Tumors. Medicine 2015, 94, e1464. [Google Scholar] [CrossRef]
- Faggian, A.; Fracella, M.R.; D’Alesio, G.; Alabiso, M.E.; Berritto, D.; Feragalli, B.; Miele, V.; Iasiello, F.; Grassi, R. Small-Bowel Neoplasms: Role of MRI Enteroclysis. Gastroenterol. Res. Pr. 2015, 2016, 9686815. [Google Scholar] [CrossRef]
- Chen, Y.-T.; Sun, H.-L.; Luo, J.-H.; Ni, J.-Y.; Chen, D.; Jiang, X.-Y.; Zhou, J.-X.; Xu, L.-F. Interventional digital subtraction angiography for small bowel gastrointestinal stromal tumors with bleeding. World J. Gastroenterol. 2014, 20, 17955–17961. [Google Scholar] [CrossRef] [PubMed]
- Shyung, L.-R.; Lin, S.-C.; Shih, S.-C.; Chang, W.-H.; Chu, C.-H.; Wang, T.-E. Proposed Scoring System to Determine Small Bowel Mass Lesions Using Capsule Endoscopy. J. Formos. Med. Assoc. 2009, 108, 533–538. [Google Scholar] [CrossRef]
- Yang, Y.J. The Future of Capsule Endoscopy: The Role of Artificial Intelligence and Other Technical Advancements. Clin. Endosc. 2020, 53, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Alemanni, L.V.; Fabbri, S.; Rondonotti, E.; Mussetto, A. Recent developments in small bowel endoscopy: The “black box” is now open! Clin. Endosc. 2022, 55, 473–479. [Google Scholar] [CrossRef]
- Mărgăritescu, N.D.; Ciobanu, M.O.; Nemeş, R.N.; Ghelase, Ş.M.; Pleşea, R.M.; Georgescu, I.; Voinea, B.; Pleşea, I.E.; Chiuțu, L.C. The morphological profile of small bowel tumors—Our experience. Rom. J. Morphol. Embryol. 2016, 57, 1241–1252. [Google Scholar]
- Tarcoveanu, E.; Georgescum, S.; Vasilescu, A.; Danila, N.; Lupascu, C.; Dimofte, G.; Neacsu, C.N.; Moldovanu, R. Small bowel tumours from barium meal to capsule endoscopy and from open to laparoscopic approach. Chirurgia 2011, 106, 451–464. [Google Scholar]
- Negoi, I.; Paun, S.; Hostiuc, S.; Stoica, B.; Tanase, I.; Negoi, R.I.; Beuran, M. Most small bowel cancers are revealed by a complication. Einstein 2015, 13, 500–505. [Google Scholar] [CrossRef]
- Oweira, H.; Abdel-Rahman, O.; Mehrabi, A.; Reissfelder, C. Assessment of the external validity of the AJCC 8th staging system for small intestinal adenocarcinoma: A time to reconsider the role of tumor location? J. Gastrointest. Oncol. 2019, 10, 421–428. [Google Scholar] [CrossRef]
- Sánchez-Ramón, A.; Cerino-Palomino, V.; Medina-Franco, H. Tumores de intestino delgado: Experiencia en el Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”. Rev. Gastroenterol. Mex. 2012, 77, 181–185. [Google Scholar] [CrossRef][Green Version]
- Zhang, S.; Zheng, C.; Chen, Y.; Xu, Q.; Ma, J.; Yuan, W.; Jiang, Q.; Zhao, Y.; Zhang, J.; Che, X.; et al. Clinicopathologic features, surgical treatments, and outcomes of small bowel tumors: A retrospective study in China. Int. J. Surg. 2017, 43, 145–154. [Google Scholar] [CrossRef]
- Rondonotti, E.; Pennazio, M.; Toth, E.; Menchen, P.; Riccioni, M.E.; De Palma, G.D.; Scotto, F.; De Looze, D.; Pachofsky, T.; Tacheci, I.; et al. Small-bowel neoplasms in patients undergoing video capsule endoscopy: A multicenter European study. Endoscopy 2008, 40, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Yoo, A.Y.; Lee, B.J.; Kim, W.S.; Kim, S.M.; Kim, S.H.; Joo, M.K.; Kim, H.J.; Park, J.-J. Clinicopathological Features of Small Bowel Tumors Diagnosed by Video Capsule Endoscopy and Balloon-Assisted Enteroscopy: A Single Center Experience. Clin. Endosc. 2021, 54, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Dabaja, B.S.; Suki, D.; Pro, B.; Bonnen, M.; Ajani, J. Adenocarcinoma of the small bowel: Presentation, prognostic factors, and outcome of 217 patients. Cancer 2004, 101, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Han, S.L.; Cheng, J.; Zhou, H.Z.; Guo, S.C.; Jia, Z.R.; Wang, P.F. Surgically treated primary malignant tumor of small bowel: A clinical analysis. World J. Gastroenterol. 2010, 16, 1527–1532. [Google Scholar] [CrossRef]
- Teufel, A.; Meindl-Beinker, N.M.; Hösel, P.; Gerken, M.; Roig, A.; Ebert, M.P.; Herr, W.; Scheiter, A.; Pauer, A.; Schlitt, H.J.; et al. Characteristics and outcome of patients with small bowel adenocarcinoma (SBA). J. Cancer Res. Clin. Oncol. 2023, 149, 4579–4590. [Google Scholar] [CrossRef]
- Tian, J.; Liu, J.; Guo, C.; Yang, X.; Yang, Y.; Gou, H.; Qiu, M.; Cao, D. Prognostic factors and treatment outcomes in patients with non-ampullary small bowel adenocarcinoma: Long-term analysis. Medicine 2019, 98, e15381. [Google Scholar] [CrossRef]
- Li, X.; Ying, H.; Cheng, Y.; Zhao, L.; Zhao, S.; Bai, C.; Zhou, J. Clinicopathological features and treatment outcomes of metastatic or locally unresectable small bowel adenocarcinoma. J. BUON 2019, 24, 2539–2545. [Google Scholar]





















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).