
Defining the Role of Adjuvant Radiotherapy for Biliary Tract Cancers: A Site-Specific Propensity-Matched Analysis

 , , , , , ,
, , , , , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
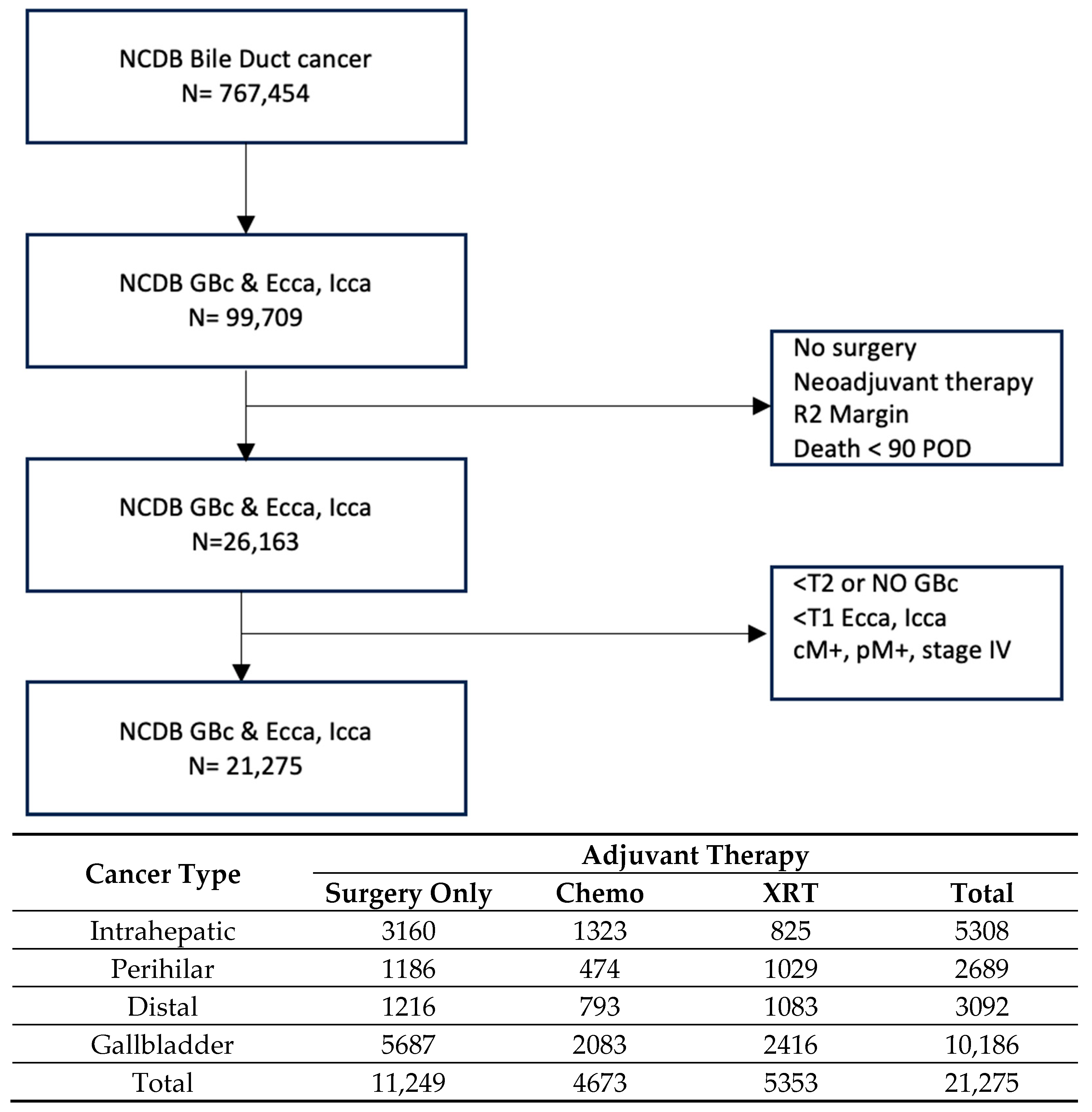
2.2. Patient Selection
2.3. Propensity Matching and Survival Analysis
3. Results
4. Subset Analyses
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, L.S.; Zhang, X.F.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Recurrence Patterns and Timing Courses Following Curative-Intent Resection for Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2019, 26, 2549–2557. [Google Scholar] [CrossRef] [PubMed]
- Groot Koerkamp, B.; Wiggers, J.K.; Allen, P.J.; Besselink, M.G.; Blumgart, L.H.; Busch, O.R.; Coelen, R.J.; D’Angelica, M.I.; DeMatteo, R.P.; Gouma, D.J.; et al. Recurrence Rate and Pattern of Perihilar Cholangiocarcinoma after Curative Intent Resection. J. Am. Coll. Surg. 2015, 221, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Komaya, K.; Ebata, T.; Shirai, K.; Ohira, S.; Morofuji, N.; Akutagawa, A.; Yamaguchi, R.; Nagino, M.; Aoba, T.; Kaneoka, Y.; et al. Recurrence after resection with curative intent for distal cholangiocarcinoma. Br. J. Surg. 2017, 104, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Komaya, K.; Ebata, T.; Yokoyama, Y.; Igami, T.; Sugawara, G.; Mizuno, T.; Yamaguchi, J.; Nagino, M. Recurrence after curative-intent resection of perihilar cholangiocarcinoma: Analysis of a large cohort with a close postoperative follow-up approach. Surgery 2018, 163, 732–738. [Google Scholar] [CrossRef]
- Sahara, K.; Tsilimigras, D.I.; Kikuchi, Y.; Ethun, C.G.; Maithel, S.K.; Abbott, D.E.; Poultsides, G.A.; Hatzaras, I.; Fields, R.C.; Weiss, M.; et al. Defining and Predicting Early Recurrence after Resection for Gallbladder Cancer. Ann. Surg. Oncol. 2021, 28, 417–425. [Google Scholar] [CrossRef]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R., Jr.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef]
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Anaya, D.A.; Anders, R.; Are, C.; Bachini, M.; Borad, M.; Brown, D.; Burgoyne, A.; et al. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 541–565. [Google Scholar] [CrossRef]
- Boffa, D.J.; Rosen, J.E.; Mallin, K.; Loomis, A.; Gay, G.; Palis, B.; Thoburn, K.; Gress, D.; McKellar, D.P.; Shulman, L.N.; et al. Using the National Cancer Database for Outcomes Research: A Review. JAMA Oncol. 2017, 3, 1722–1728. [Google Scholar] [CrossRef]
- Ramaswamy, A.; Ostwal, V.S.; Engineer, R.; Parulekar, M.; Mandavkar, S.; Aier, N.; Bhargava, P.G.; Srinivas, S.; Patkar, S.; Krishnatry, R.; et al. A multicenter, open-label, randomized phase II study evaluating adjuvant gemcitabine plus cisplatin (GC) and capecitabine with concurrent capecitabine radiotherapy (CAPE-RT) in patients with operated gallbladder adenocarcinoma (GBC): The GECCOR-GB trial. J. Clin. Oncol. 2023, 41, 4017. [Google Scholar] [CrossRef]
- Choi, S.H.; Rim, C.H.; Shin, I.S.; Yoon, W.S.; Koom, W.S.; Seong, J. Benefit of adjuvant radiotherapy for gallbladder cancer: A comparability-based meta-analysis. Hepatol. Int. 2022, 16, 712–727. [Google Scholar] [CrossRef] [PubMed]
- Beuzit, L.; Edeline, J.; Brun, V.; Ronot, M.; Guillygomarc’h, A.; Boudjema, K.; Gandon, Y.; Garin, E.; Rolland, Y. Comparison of Choi criteria and Response Evaluation Criteria in Solid Tumors (RECIST) for intrahepatic cholangiocarcinoma treated with glass-microspheres Yttrium-90 selective internal radiation therapy (SIRT). Eur. J. Radiol. 2016, 85, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Moole, H.; Tathireddy, H.; Dharmapuri, S.; Moole, V.; Boddireddy, R.; Yedama, P.; Dharmapuri, S.; Uppu, A.; Bondalapati, N.; Duvvuri, A. Success of photodynamic therapy in palliating patients with nonresectable cholangiocarcinoma: A systematic review and meta-analysis. World J. Gastroenterol. 2017, 23, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.W.; Yang, X.H.; Wu, B.Q.; Jiang, Y.; Qu, Z. Progress in diagnosis and surgical treatment of perihilar cholangiocarcinoma. Gastroenterol. Hepatol. 2019, 42, 271–279. [Google Scholar] [CrossRef]
- Rea, D.J.; Heimbach, J.K.; Rosen, C.B.; Haddock, M.G.; Alberts, S.R.; Kremers, W.K.; Gores, G.J.; Nagorney, D.M. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann. Surg. 2005, 242, 451–458; discussion 458–461. [Google Scholar] [CrossRef]
- Edeline, J.; Touchefeu, Y.; Guiu, B.; Farge, O.; Tougeron, D.; Baumgaertner, I.; Ayav, A.; Campillo-Gimenez, B.; Beuzit, L.; Pracht, M.; et al. Radioembolization Plus Chemotherapy for First-line Treatment of Locally Advanced Intrahepatic Cholangiocarcinoma: A Phase 2 Clinical Trial. JAMA Oncol. 2020, 6, 51–59. [Google Scholar] [CrossRef]
- Dominguez, D.A.; Wong, P.; Chen, Y.J.; Singh, G.P.; Fong, Y.; Li, D.; Ituarte, P.H.G.; Melstrom, L.G. Adjuvant Chemoradiation in Resected Biliary Adenocarcinoma: Evaluation of SWOG S0809 with a Large National Database. Ann. Surg. Oncol. 2024. [Google Scholar] [CrossRef]
- Kobayashi, S.; Tomokuni, A.; Gotoh, K.; Takahashi, H.; Akita, H.; Marubashi, S.; Yamada, T.; Teshima, T.; Fukui, K.; Fujiwara, Y.; et al. A retrospective analysis of the clinical effects of neoadjuvant combination therapy with full-dose gemcitabine and radiation therapy in patients with biliary tract cancer. Eur. J. Surg. Oncol. 2017, 43, 763–771. [Google Scholar] [CrossRef]
- Abe, Y.; Itano, O.; Takemura, Y.; Minagawa, T.; Ojima, H.; Shinoda, M.; Kitago, M.; Obara, H.; Shigematsu, N.; Kitagawa, Y. Phase I study of neoadjuvant S-1 plus cisplatin with concurrent radiation for biliary tract cancer (Tokyo Study Group for Biliary Cancer: TOSBIC02). Ann. Gastroenterol. Surg. 2023, 7, 808–818. [Google Scholar] [CrossRef]
- Oh, D.Y.; Ruth He, A.; Qin, S.; Chen, L.T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Ah Lee, M.; Kitano, M.; et al. Durvalumab plus Gemcitabine and Cisplatin in Advanced Biliary Tract Cancer. NEJM Evid. 2022, 1, EVIDoa2200015. [Google Scholar] [CrossRef]
- Kelley, R.K.; Ueno, M.; Yoo, C.; Finn, R.S.; Furuse, J.; Ren, Z.; Yau, T.; Klumpen, H.J.; Chan, S.L.; Ozaka, M.; et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2023, 401, 1853–1865. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All Biliary Tumors | Matched Group 1 (n = 8394) | Matched Group 2 (n = 7252) | ||||||
|---|---|---|---|---|---|---|---|---|
| Surgery Only (n = 4197) | XRT (n = 4197) | Chemo (n = 3626) | XRT (n = 3626) | |||||
| n | Col % | n | Col % | n | Col % | n | Col % | |
| SEX | ||||||||
| Male | 1824 | 43.5% | 1866 | 44.5% | 1562 | 43.1% | 1578 | 43.5% |
| Female | 2373 | 56.5% | 2331 | 55.5% | 2064 | 56.9% | 2048 | 56.5% |
| Age | ||||||||
| ≤65 | 1813 | 43.2% | 1811 | 43.1% | 1743 | 48.1% | 1725 | 47.6% |
| >65 | 2384 | 56.8% | 2386 | 56.9% | 1883 | 51.9% | 1901 | 52.4% |
| Race | ||||||||
| White | 3067 | 73.1% | 3009 | 71.7% | 2616 | 72.1% | 2562 | 70.7% |
| Black | 421 | 10.0% | 480 | 11.4% | 389 | 10.7% | 432 | 11.9% |
| Hispanic | 382 | 9.1% | 392 | 9.8% | 324 | 8.9% | 364 | 10.0% |
| Asian/Pacific Islander | 275 | 6.6% | 240 | 5.7% | 224 | 6.2% | 214 | 5.9% |
| Others | 52 | 1.2% | 55 | 1.3% | 52 | 1.4% | 48 | 1.3% |
| Margin | ||||||||
| R0 | 2782 | 66.3% | 2788 | 66.4% | 2434 | 67.1% | 2430 | 67.0% |
| R1 | 684 | 16.3% | 691 | 16.5% | 548 | 15.1% | 563 | 15.5% |
| RX | 731 | 17.4% | 718 | 17.1% | 644 | 17.8% | 633 | 17.5% |
| Pathologic T Stage | ||||||||
| T1 | 281 | 6.7% | 321 | 7.6% | 212 | 5.8% | 233 | 6.4% |
| T2 | 1594 | 38.0% | 1548 | 36.9% | 1225 | 33.8% | 1243 | 34.3% |
| T3 | 1436 | 34.2% | 1405 | 33.5% | 1379 | 38.0% | 1353 | 37.3% |
| T4 | 82 | 2.0% | 88 | 2.1% | 79 | 2.2% | 65 | 1.8% |
| Unknown | 804 | 19.2% | 835 | 19.9% | 731 | 20.2% | 739 | 20.4% |
| Pathologic N Stage | ||||||||
| N0 | 1853 | 44.2% | 1852 | 44.1% | 1406 | 38.8% | 1441 | 39.7% |
| N1 | 1509 | 35.9% | 1512 | 36.0% | 1511 | 41.7% | 1496 | 40.4% |
| NX | 833 | 19.8% | 833 | 19.8% | 709 | 19.6% | 699 | 19.3% |
| Lymph nodes positive | ||||||||
| Negative | 1562 | 37.2% | 1552 | 37.0% | 1195 | 33.0% | 1233 | 34.0% |
| Positive | 1506 | 35.9% | 1515 | 35.8% | 1494 | 41.2% | 1479 | 40.7% |
| No LN examined | 1107 | 26.4% | 1114 | 26.6% | 911 | 25.1% | 897 | 24.7% |
| Unknown | 22 | 0.5% | 22 | 0.5% | 26 | 0.7% | 17 | 0.5% |
| Surgical approach | ||||||||
| Open | 1491 | 35.5% | 1472 | 35.1% | 1320 | 36.4% | 1275 | 35.2% |
| Minimally Invasive | 940 | 22.4% | 945 | 22.5% | 874 | 24.1% | 891 | 24.6% |
| No data before 2010 | 1265 | 30.2% | 1269 | 30.2% | 719 | 19.7% | 735 | 20.3% |
| Unknown after 2010 | 501 | 11.9% | 511 | 12.2% | 713 | 19.8% | 725 | 20.4% |
| N | 5-yr Survival (%) | Median Survival (mo.) | p Value | |
|---|---|---|---|---|
| Matched Intrahepatic (IHC) | ||||
| Group 1 | 0.319 | |||
| Surgery Only | 723 | 41.2 | 44.8 | |
| XRT | 723 | 38.8 | 38.9 | |
| Group 2 | 0.445 | |||
| Chemo | 691 | 38.5 | 43.3 | |
| XRT | 691 | 37.7 | 38.7 | |
| Matched Perihilar (PHC) | ||||
| Group 1 | 0.003 | |||
| Surgery Only | 693 | 24.7 | 26.3 | |
| XRT | 693 | 31.0 | 31.2 | |
| Group 2 | 0.557 | |||
| Chemo | 445 | 27.0 | 26.5 | |
| XRT | 445 | 29.7 | 30.3 | |
| Matched Distal (DCC) | ||||
| Group 1 | 0.015 | |||
| Surgery Only | 726 | 30.7 | 27.0 | |
| XRT | 726 | 33.4 | 33.7 | |
| Group 2 | 0.298 | |||
| Chemo | 722 | 35.2 | 33.4 | |
| XRT | 722 | 31.8 | 32.9 | |
| Matched Gallbladder (GBC) | ||||
| Group 1 | 0.05 | |||
| Surgery Only | 2055 | 33.8 | 26.6 | |
| XRT | 2055 | 32.5 | 30.2 | |
| Group 2 | 0.001 | |||
| Chemo | 1768 | 31.5 | 24.6 | |
| XRT | 1768 | 32.6 | 30.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, Y.D.; Acidi, B.; Newton, A.; Haddad, A.; Chiang, Y.-J.; Coelho, R.; Newhook, T.E.; Tzeng, C.-W.D.; Chun, Y.S.; Ludmir, E.B.; et al. Defining the Role of Adjuvant Radiotherapy for Biliary Tract Cancers: A Site-Specific Propensity-Matched Analysis. Cancers 2025, 17, 494. https://doi.org/10.3390/cancers17030494
Seo YD, Acidi B, Newton A, Haddad A, Chiang Y-J, Coelho R, Newhook TE, Tzeng C-WD, Chun YS, Ludmir EB, et al. Defining the Role of Adjuvant Radiotherapy for Biliary Tract Cancers: A Site-Specific Propensity-Matched Analysis. Cancers. 2025; 17(3):494. https://doi.org/10.3390/cancers17030494
Chicago/Turabian StyleSeo, Yongwoo David, Belkacem Acidi, Andrew Newton, Antony Haddad, Yi-Ju Chiang, Rainna Coelho, Timothy E. Newhook, Ching-Wei D. Tzeng, Yun Shin Chun, Ethan B. Ludmir, and et al. 2025. "Defining the Role of Adjuvant Radiotherapy for Biliary Tract Cancers: A Site-Specific Propensity-Matched Analysis" Cancers 17, no. 3: 494. https://doi.org/10.3390/cancers17030494
APA StyleSeo, Y. D., Acidi, B., Newton, A., Haddad, A., Chiang, Y.-J., Coelho, R., Newhook, T. E., Tzeng, C.-W. D., Chun, Y. S., Ludmir, E. B., Koay, E. J., Javle, M., Vauthey, J. N., & Cao, H. S. T. (2025). Defining the Role of Adjuvant Radiotherapy for Biliary Tract Cancers: A Site-Specific Propensity-Matched Analysis. Cancers, 17(3), 494. https://doi.org/10.3390/cancers17030494