Simple Summary
Basaloid thymic carcinoma (BTC) is an extremely rare tumor, and very little data are available on its clinical behavior, drug sensibility, and patients’ outcome. We retrospectively collected demographical, clinical, and pathological data of all consecutive patients previously diagnosed with BTC at TYME-referral institutes from 2008 to 2023. Twenty-eight patients with BTC were identified. A total of 22/28 patients were included in this analysis. BTC is generally diagnosed as a localized disease, and no alterations in actionable targets or microsatellite instability were identified. Patients with stage I–III BTC can achieve long-term DFS, and efforts should be made to perform radical surgical resection, combined with perioperative treatment when appropriate. Patients with advanced disease progression have shown a high response rate to systemic treatments, but they have a poor prognosis.
Abstract
Background: thymic basaloid carcinoma (BTC) is an extremely rare tumor, and very little data are available on BTC’s biology, clinical behavior, drug sensitivity, and patient outcomes. Methods: We performed a retrospective observational study on patients diagnosed with BTC in 11 referral centers of TYME. All BTC diagnoses were reviewed by the referring pathologist. Results: Twenty-eight patients were identified. A total of 22/28 patients were included. Eighteen patients had TNM stage I–III disease, and all underwent surgery; three patients received preoperative chemotherapy, and 10 patients received adjuvant radiotherapy. With a median follow-up of 46 (1–133) months, median overall survival (mOS) and median relapse-free survival were not reached. At 48 months, OS was 77% (95%CI 43–92), and DFS was 63% (95%CI 30–83). The median OS of the 4 patients diagnosed with metastatic disease was 7 months. Six patients received first-line systemic treatment for metastatic disease, and all showed tumor responses. Anti-tumor activity was also observed with an anti-VEGFR TKI and a multi-TKI inhibitor combined with an anti-PD1 antibody. Next-generation sequencing performed in three tumor samples did not identify actionable alterations or microsatellite instability. Conclusions: BTC is an extremely rare tumor that usually presents as a localized disease. Patients diagnosed with stage I–III disease can achieve long-term DFS, and efforts should be made to perform radical surgical resection combined with perioperative treatment whenever appropriate. Patients with advanced disease progression have a poor prognosis despite a high response rate to systemic treatments.
1. Introduction
Thymic epithelial tumors (TETs) are a heterogeneous group of rare neoplasms arising from thymic epithelial cells with a complex histopathologic classification.
The World Health Organization (WHO) classifies TETs into two main subgroups: thymomas (TMs) and thymic carcinomas (TCs) [1,2,3]. TMs include five subtypes (A, AB, B1, B2, and B3), which are distinguished by the morphology of the epithelial cells and the percentage of non-neoplastic lymphocytes. The prognosis is best for type A, progressively worse for the other subtypes, and worst for type B3 [4,5,6,7].
Thymic carcinoma (TC) is a rare malignancy accounting for approximately 10–12% of all TETs. It is the most aggressive TET subtype, with a more aggressive behavior and a higher propensity for widespread metastasis [8,9]. Patients with advanced TC are usually treated with systemic therapies, including platinum-based chemotherapy such as cisplatin/cyclophosphamide/doxorubicin or carboplatinum/paclitaxel combinations and anti-angiogenic agents, such as sunitinib and lenvatinib, achieving a 5-year overall survival rate of approximately 30–55% [10,11,12,13,14,15].
In addition, immunotherapy has shown robust clinical activity both as a monotherapy [16,17,18,19] and in combination [20], and it is considered one of the standard treatment options in many international guidelines.
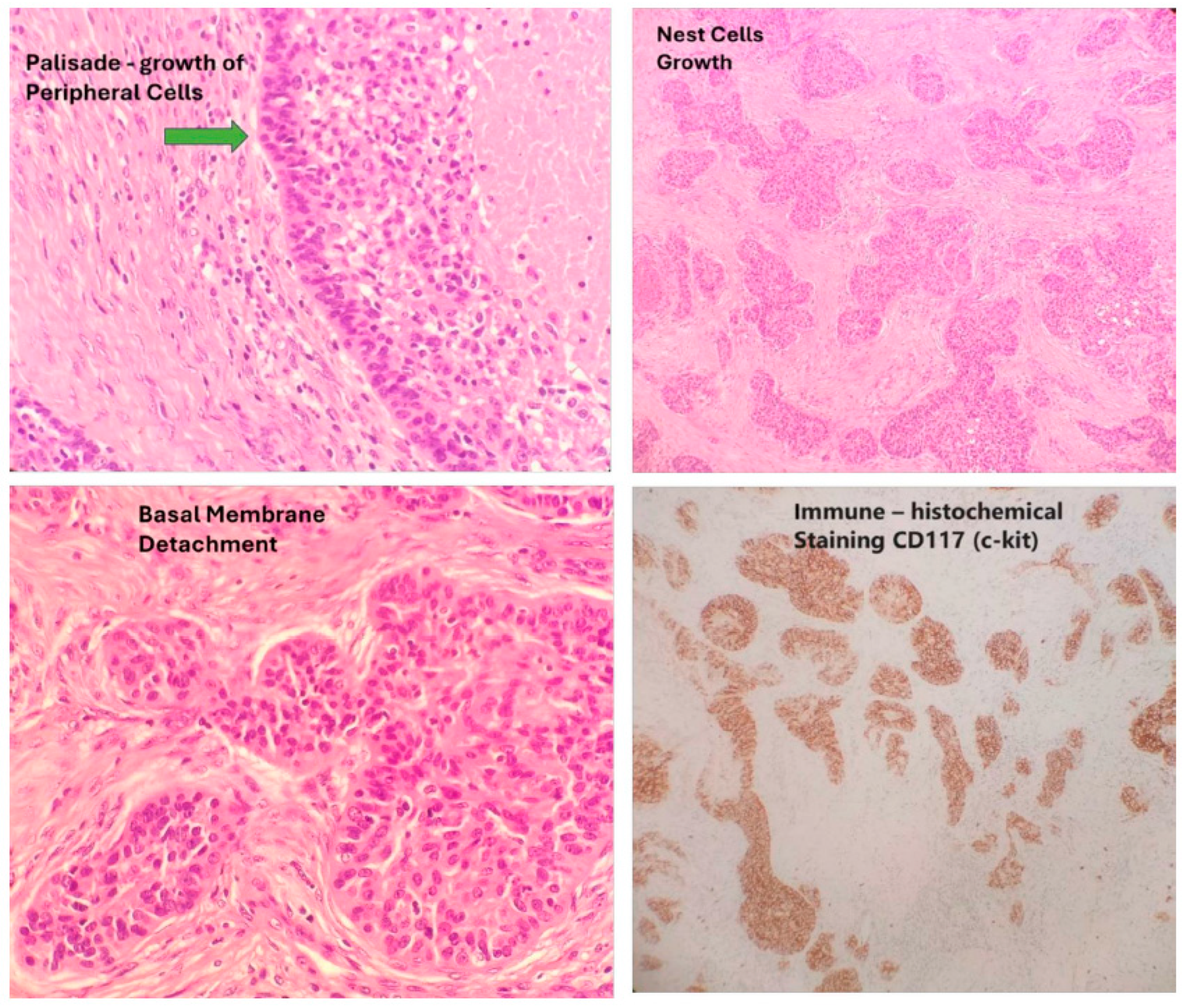
Basaloid thymic carcinoma (BTC) is an extremely rare subtype of TC that is well recognized in the WHO classification. After the identification of squamous cell marker expression in BTC, this tumor became a rare subtype of squamous cell thymic carcinoma (STC), reclassifying STC into keratinizing, non-keratinizing, and basaloid subtypes. Tumors are classified as BTC when more than 50% of the tumor is basaloid. Tumors with 50% or less basaloid component may be included in the diagnosis “with basaloid features”. The differential diagnosis includes poorly differentiated squamous cell carcinoma and metastatic tumor, with CD-117 being a useful marker in differential diagnosis [21] (Figure 1).
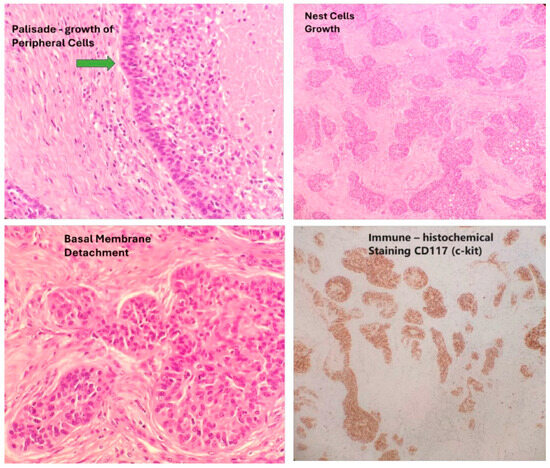
Figure 1.
Typical histological features and CD117 staining of BTC (primary tumor specimens).
Choosing an appropriate treatment strategy for patients with BTC is often challenging because of its extreme rarity and the very limited data available on its clinical behavior, drug sensitivity, and patient outcomes. To our knowledge, only about 30 cases of BTC have been published in the English literature, and most of them are single-case reports [22,23,24,25,26,27,28,29,30].
In order to provide a basis for clinical decision making in this subgroup of patients, the referral centers of the Italian Collaborative Group for ThYmic MalignanciEs (TYME) retrospectively identified patients diagnosed with BTC, reviewed the pathological diagnosis, and analyzed all available clinical data.
The study was approved by the TYME research group, by the Scientific Ethics Committee of the coordinating institute (CE Humanitas Prot. GAV 312/23 on 23 Maj 2023), and by all the other involved centers.
2. Material and Methods
We performed a multicenter retrospective observational study of patients diagnosed with TET from 2008 to 2023 within the referral centers of the TYME network.
TYME (ThyYmic MalignanciEs) is a network established in Italy in 2014 with the aim of promoting collaboration among Italian centers with specific multidisciplinary expertise in TETs. Currently, 23 centers are members of the network. As of December 2024, the first 11 of them have participated in the Italian Registry on Thymic Epithelial Tumors (TETs), and all these centers participated in this retrospective analysis.
Medical records were reviewed to extract data from all patients previously diagnosed with BTC. Inclusion criteria included tumor location in the anterior mediastinum, an absence of other primary tumors, and the presence of basaloid morphologic and histochemical features, specifically a histologic diagnosis of thymic carcinoma, positive immunohistochemical staining for CD117, and a basaloid component of more than 50% of the tumor. Tumors with 50% or less basaloid component, so-called “tumors with basaloid features”, were excluded.
All selected cases were reviewed by the center’s referring pathologist and oncologist to confirm the diagnosis of BTC.
Tumors were defined as localized (stage I–III) or metastatic (stage IV) according to 8th TNM.
Descriptive analyses were performed for all BTC-confirmed patients. Disease-free survival (DFS) and overall survival (OS) functions were estimated using the Kaplan–Meier method on the number of patients with available survival data. DFS was calculated from the date of surgery to the date of relapse or death, whichever occurred first. OS was calculated from the date of diagnosis to the date of death or last follow-up. Tumor response was assessed according to the RECIST 1.1 criteria [31].
3. Results
Twenty-eight patients with BTC diagnosed between 2008 and 2023 were identified by 11 centers. A total of 22/28 patients were included in this analysis. Six patients were excluded because of concomitant second primary tumor (one patient), insufficient data (one patient), or unconfirmed diagnosis of BTC at pathological review (four patient).
Patient characteristics are summarized in Table 1.

Table 1.
Characteristics of patients.
The median age of the patients at the time of diagnosis was 58 years (range: 33–76). A total of 11/22 patients were male.
The majority of patients had early stage disease at the time of diagnosis (stage I: 9 pts, stage II: 6 pts). Three patients were diagnosed with stage III and four patients with stage IV disease.
All 18 patients with localized disease at diagnosis underwent surgery. Three patients received preoperative chemotherapy, while no patient received preoperative radiotherapy. Ten patients also received postoperative radiation.
All six patients with metastatic disease received first-line chemotherapy, and five received additional systemic therapies.
No patient had autoimmune disease.
3.1. Patients with Localized Disease
Eighteen patients out of twenty-two were diagnosed with localized disease (TNM stage I: eight patients, stage II: five patients, stage III: three patients, and not available: two patients).
All 18 patients with localized BTC underwent surgery. Three patients received platinum-containing preoperative chemotherapy consisting of a CAP (cisplatin, doxorubicin, and cyclophosphamide) regimen (two patients) and a carboplatin plus paclitaxel combination (one patient).
According to the RECIST 1.1 criteria, two patients (one patient treated with CAP, and one patient treated with CBDCA plus paclitaxel) achieved a partial response (PR) and remained disease-free after surgery at 10+ and 70+ months. The best response of the remaining patient was stable disease.
Ten patients received adjuvant radiotherapy.
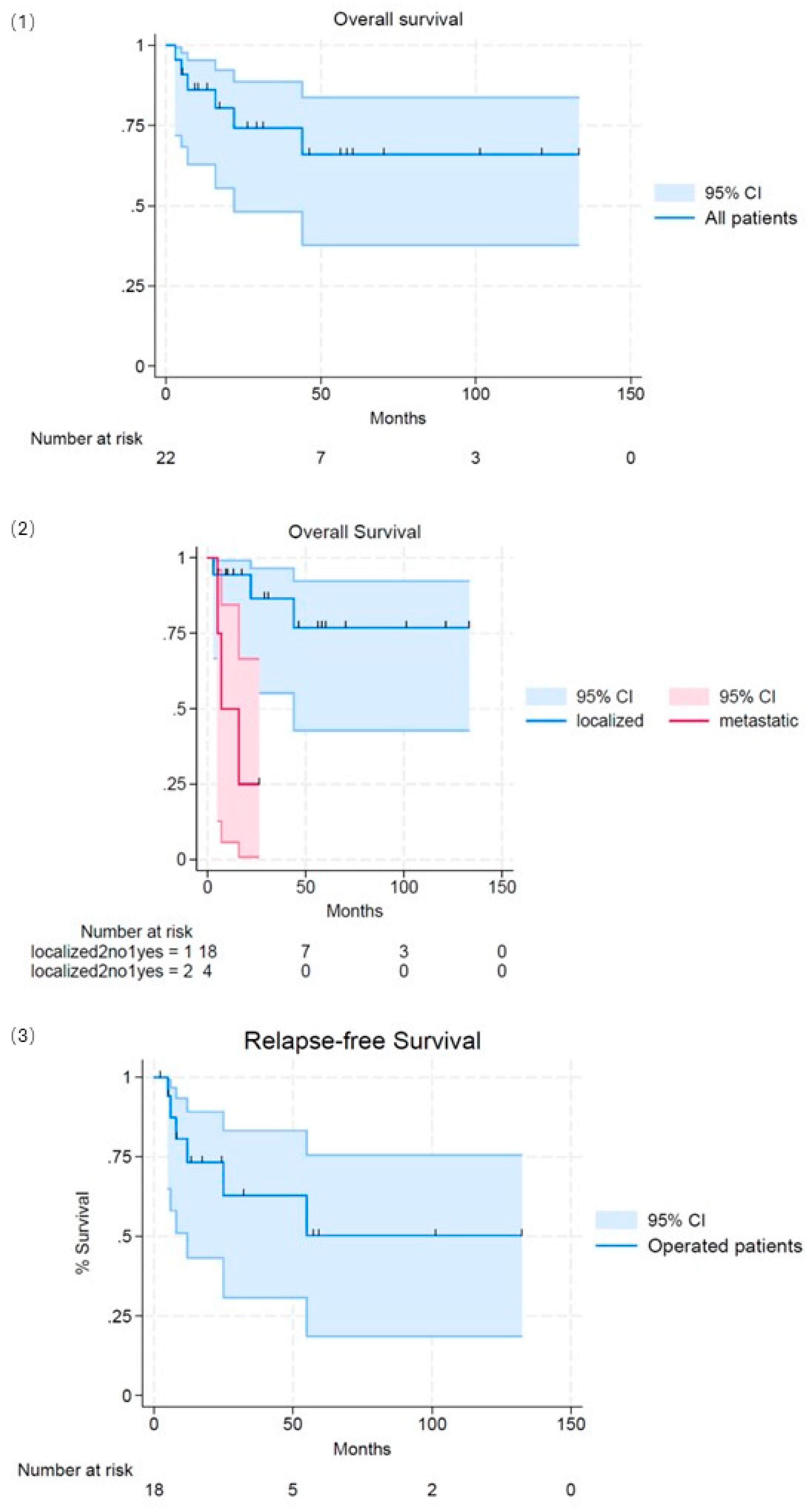
At a median follow-up of 46 (1–133) months, six out of eighteen patients relapsed (two locoregional and four distant). Median overall survival and median relapse-free survival were not reached. At 48 months, OS was 77% (95%CI 43–92), and DFS was 63% (95%CI 30–83) (Figure 2).
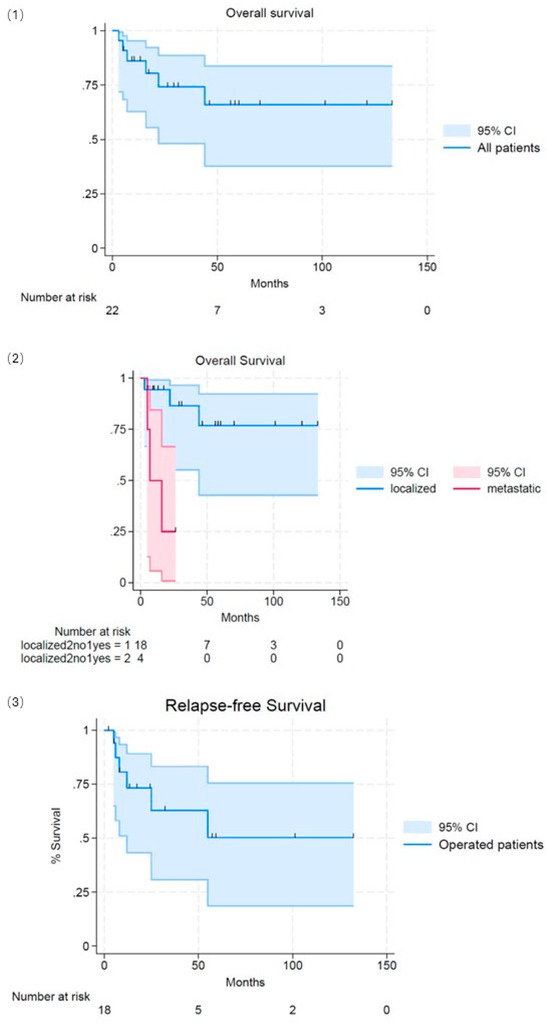
Figure 2.
Survival. (1): Overall survival of the entire population. (2): Overall survival split (localized/metastatic tumor at diagnosis). (3): Relapse-free survival split (localized/metastatic tumor at diagnosis).
3.2. Patients with Upfront Metastatic Disease
Four out of twenty-two patients were diagnosed with sincronous metastatic lesions, mostly localized to the lungs, liver, and bones. Four out of twenty-two patients were diagnosed with sinusoidal metastatic lesions, mostly localized to the lungs, liver, and bones. Three patients died, and one patient was alive for 24 months. Median OS was 7 months (Figure 2).
3.3. Response to Systemic Treatments
Six patients received first-line systemic treatment for metastatic disease, all with platinum-containing chemotherapy: carboplatin plus paclitaxel (five patients) and carboplatin plus etoposide (one patient). Five patients had a partial response, and one patient had a complete response (CR). Five out of six also received a second-line treatment. Two out of five were treated with sunitinib, and one of them achieved a PR lasting 7 months; one patient received a pembrolizumab/lenvatinib combination with a complete response lasting 7+ months.
3.4. Molecular Analysys
Next-generation sequencing was performed in three tumor samples, and no KIT mutations, other actionable alterations, or microsatellite instability were identified.
4. Discussion
This retrospective analysis, performed by 11 centers of the TYME network, identified 22 patients with BTC diagnosed over a 15-year period, confirmed by a pathological and oncological internal review.
Thymic basaloid carcinoma appeared to be an extremely rare tumor, usually diagnosed between 50 and 70 years of age, with an equal distribution between men and women.
Of particular interest, BTC was diagnosed in most cases as localized WHO stage I–III disease. All patients underwent radical surgery with or without perioperative treatment. With a median follow-up of 46 (1–133) months, 12/18 patients remained disease-free with a 48 mOS and DFS of 77% and 63%, respectively. These data suggest a similar outcome for patients with localized BTC compared to that reported for patients with stage I–III thymic carcinoma [29].
The lack of adequate studies in this patient setting, due to the extreme rarity of this tumor, makes it impossible to make an adequate comparison between our results and those reported in the literature for patients with BTC. In addition to some case reports [22,23,24,25,26,27,28,29], we can only refer to the clinicopathologic study of 12 cases of BTC by Jeffrey G. Brown et al. reported long-term data in eight patients diagnosed with localized/metastatic BTC [30]. In this report, five out of eight patients died of their disease at an average of 34 months from the time of diagnosis.
The small number of patients treated with preoperative chemotherapy does not allow for definitive conclusions to be drawn about its role in determining patient outcomes. In light of the activity demonstrated in the three patients treated in this series, its use can be considered and deemed useful for an adequate multimodal approach. Three patients were treated with induction carboplatin plus paclitaxel or the CAP regimen, achieving a partial response (two patients) or disease stabilization (one patient). The limited sample size and retrospective nature of this analysis do not allow for the evaluation of the efficacy of adjuvant radiotherapy, which was administered to 10/18 patients with no major side effects.
The response to systemic treatments in patients with advanced BTC appears to be higher than expected when compared with the available data on TC. Tumor responses were observed in all six patients treated with a platinum-containing regimen and in one of the two patients treated with sunitinib. Interestingly, one patient treated with a pembrolizumab/lenvatinib combination achieved a complete response lasting 7+ months.
Despite good drug sensitivity, the prognosis of patients diagnosed with synchronous metastases seems to be poor, with an observed mOS of 7 months in the small sample size analyzed. Unfortunately, no KIT mutations, other actionable target alterations, or microsatellite instability were identified to suggest possible targeted approaches.
The limitations of this study are due to its retrospective nature, the absence of a centralized review, and the limited number of cases analyzed.
5. Conclusions
Basaloid thymic carcinoma is an extremely rare tumor, usually presenting as localized disease, and no actionable targets have been found in the few cases analyzed by NGS. Patients diagnosed with stage I–III disease can achieve long-term DFS, and efforts should be made to perform radical surgical resection, combined with perioperative treatment whenever appropriate. Patients with advanced disease have a poor prognosis despite a high response rate to systemic treatments. This experience also demonstrates the potential of collaborative networks to contribute to the knowledge of ultra-rare diseases. A major collaborative effort should be undertaken to better understand the preclinical and clinical basis of BTC in order to improve the treatment of this extremely rare tumor.
Author Contributions
C.C. and T.D.P. contributed to the conception of the work, the acquisition, analysis, the interpretation of data for this work, drafting this work, and final approval of the version to be published; the authors confirmed their agreement to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All the other authors contributed to the acquisition, analysis, interpretation of data for this work, drafting this work, and the final approval of the version to be published; the authors confirmed their agreement to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Funding
Cliniche Humanitas Gavazzeni (Via Mauro Gavazzeni 21, 24125, Bergamo, Italy) supported the publication fee for this work.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Comitato Etico Humanitas (protocol code GAV 312/23 date of approval: 23 May 2023).
Informed Consent Statement
Since this is a retrospective study and we have EC approval, informed consent was not required.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
Chiara Catania: outside the submitted work, personal fees for speaker and meeting support from Astra Zeneca. Paolo Zucali: outside the submitted work, personal fees for his advisory role, speaker engagements, and travel and accommodation expenses from Merck Sharp and Dohme (MSD), Astellas, Janssen, Sanofi, Ipsen, Pfizer, Novartis, Bristol Meyer Squibb, Amgen, Astra Zeneca, Roche, and Bayer. Enrico Ruffini: outside the submitted work, personal fees for speaker engagements and travel and accommodation expenses from Astra Zeneca and Roche. Giuseppe Lo Russo: outside the submitted work, personal fees for his advisory role, travel accommodations, speaker fees, writing fees, consultancies, honoraria, and pi for profit trials from MSD, Regeneron, Roche, Lilly, BMS, Amgen, Astra Zeneca, Johnson and Johnson, Merck, Novartis, Pierre Fabre, Bayer, Beigene, Pfizer, GSK, DAlICHi, Takeda, and Sanofi. Marina Garassino: outside the submitted work, she reports to AstraZeneca, Abion, MSD International, Bayer, BMS, Boehringer Ingelheim Italia S.p.A, Celgene, Eli Lilly, Incyte, Novartis, Pfizer, Roche, Takeda, Seattle Genetics, Mirati, Daiichi Sankyo, Regeneron, Merck, Blueprint, Janssen, Sanofi, AbbVie, BeiGenius, Oncohost, and Medscape. Giulia Pasello: outside the submitted work: advisor/consultant/speaker fee: AstraZeneca, BMS, MSD, Lilly, Novartis, Amgen, Pfizer, J&J, Roche. unconditioned research support: Astra Zeneca, Roche, and MSD Guido Rindi: outside the submitted work, speakers fee for IPSEN and a consulting role for Bracco Imaging Suisse. Tommaso De Pas: outside the submitted work, personal fees for trial support, meeting support, advisory role, speaker engagements, and travel and accommodation expenses from GSK Boehringer Ingelheim, Pfizer, Blueprint Medicines, Gilead, Amgen, Merck, and GSK.
References
- Masaoka, A.; Monden, Y.; Nakahara, K.; Tanioka, T. Follow-up study of thymomas with special reference to their clinical stages. Cancer 1981, 48, 2485–2492. [Google Scholar] [CrossRef] [PubMed]
- Koga, K.; Matsuno, Y.; Noguchi, M.; Mukai, K.; Asamura, H.; Goya, T.; Shimosato, Y. A review of 79 thymomas: Modification of staging system and reappraisal of conventional division into invasive and non-invasive thymoma. Pathol. Int. 1994, 44, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.A. Epidemiology of thymoma and associated malignancies. J. Thorac. Oncol. 2010, 5 (Suppl. S4), S260–S265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ströbel, P.; Hohenberger, P.; Marx, A. Thymoma and thymic carcinoma: Molecular pathology and targeted therapy. J. Thorac. Oncol. 2010, 5 (Suppl. S4), S286–S290. [Google Scholar] [CrossRef] [PubMed]
- Marx, A.; Ströbel, P.; Badve, S.S.; Chalabreysse, L.; Chan, J.K.; Chen, G.; de Leval, L.; Detterbeck, F.; Girard, N.; Huang, J.; et al. ITMIG consensus statement on the use of the WHO histological classification of thymoma and thymic carcinoma: Refined definitions, histological criteria, and reporting. J. Thorac. Oncol. 2014, 9, 596–611. [Google Scholar] [CrossRef] [PubMed]
- den Bakker, M.A.; Roden, A.C.; Marx, A.; Marino, M. Histologic classification of thymoma: A practical guide for routine cases. J. Thorac. Oncol. 2014, 9 (Suppl. S2), S125–S130. [Google Scholar] [CrossRef] [PubMed]
- Chalabreysse, L.; Roy, P.; Cordier, J.F.; Loire, R.; Gamondes, J.P.; Thivolet-Bejui, F. Correlation of the WHO schema for the classification of thymic epithelial neoplasms with prognosis: A retrospective study of 90 tumors. Am. J. Surg. Pathol. 2002, 26, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Weis, C.A.; Yao, X.; Deng, Y.; Detterbeck, F.C.; Marino, M.; Nicholson, A.G.; Huang, J.; Ströbel, P.; Antonicelli, A.; Marx, A. Contributors to the ITMIG Retrospective Database. The impact of thymoma histotype on prognosis in a worldwide database. J. Thorac. Oncol. 2015, 10, 367–372. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roden, A.C.; Yi, E.S.; Jenkins, S.M.; Edwards, K.K.; Donovan, J.L.; Cassivi, S.D.; Marks, R.S.; Garces, Y.I.; Aubry, M.C. Modified Masaoka stage and size are independent prognostic predictors in thymoma and modified Masaoka stage is superior to histopathologic classifications. J. Thorac. Oncol. 2015, 10, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, U. The eighth edition TNM stage classification for thymic tumors: What do I need to know? J. Thorac. Cardiovasc. Surg. 2021, 161, 1524–1529. [Google Scholar] [CrossRef]
- Ruffini, E.; Fang, W.; Guerrera, F.; Huang, J.; Okumura, M.; Kim, D.K.; Girard, N.; Billè, A.; Boubia, S.; Cangir, A.K.; et al. The international association for the study of lung cancer thymic tumors staging project: The impact of the eighth edition of the union for international cancer control and American Joint Committee on cancer TNM stage classification of thymic tumors. J. Thorac. Oncol. 2020, 15, 436e47. [Google Scholar] [CrossRef] [PubMed]
- Sato, J.; Satouchi, M.; Itoh, S.; Okuma, Y.; Niho, S.; Mizugaki, H.; Murakami, H.; Fujisaka, Y.; Kozuki, T.; Nakamura, K.; et al. Lenvatinib in patients with advanced or metastatic thymic carcinoma(REMORA): A multicentre, phase 2 trial. Lancet Oncol. 2020, 21, 843e50. [Google Scholar] [CrossRef] [PubMed]
- Proto, C.; Ganzinelli, M.; Manglaviti, S.; Imbimbo, M.; Galli, G.; Marabese, M.; Zollo, F.; Alvisi, M.F.; Perrino, M.; Cordua, N.; et al. Efficacy and safety of ramucirumab plus carboplatin and paclitaxel in untreated metastatic thymic carcinoma: RELEVENT phase II trial (NCT03921671). Ann. Oncol. 2024, 35, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Antonarelli, G.; Corti, C.; Zucali, P.A.; Perrino, M.; Manglaviti, S.; Lo Russo, G.; Varano, G.M.; Salvini, P.; Curigliano, G.; Catania, C.; et al. Continuous sunitinib schedule in advanced platinum refractory thymic epithelial neoplasms: A retrospective analysis from the ThYmic MalignanciEs (TYME) Italian collaborative group. Eur. J. Cancer 2022, 174, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; De Pas, T.; He, Y.; Giaccone, G. Investigational drugs for the treatment of thymic cancer: A focus on phase 1 and 2 clinical trials. Expert. Opin. Investig. Drugs 2022, 31, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Giaccone, G.; Kim, C.; Thompson, J.; McGuire, C.; Kallakury, B.; Chahine, J.J.; Manning, M.; Mogg, R.; Blumenschein, W.M.; Tan, M.T.; et al. Pembrolizumab in patients with thymic carcinoma: A single-arm, single-centre, phase 2 study. Lancet Oncol. 2018, 19, 347–355. [Google Scholar] [CrossRef]
- Giaccone, G.; Kim, C. Durable Response in Patients with Thymic Carcinoma Treated with Pembrolizumab After Prolonged Follow-Up. J. Thorac. Oncol. 2021, 16, 483–485. [Google Scholar] [CrossRef]
- Cho, J.; Kim, H.S.; Ku, B.M.; Choi, Y.-L.; Cristescu, R.; Han, J.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; Park, K.; et al. Pembrolizumab for patients with refractory or relapsed thymic epithelial tumor: An open-label phase II trial. J. Clin. Oncol. 2019, 37, 2162–2170. [Google Scholar] [CrossRef]
- Wang, W.; Lin, G.; Hao, Y.; Guan, Y.; Zhang, Y.; Xu, C.; Wang, Q.; Wang, D.; Jiang, Z.; Cai, J.; et al. Treatment outcomes and prognosis of immune checkpoint inhibitors therapy in patients with advanced thymic carcinoma: A multicentre retrospective study. Eur. J. Cancer 2022, 174, 21–30. [Google Scholar] [CrossRef]
- Conforti, F.; Zucali, P.A.; Pala, L.; Catania, C.; Bagnardi, V.; Sala, I.; Della Vigna, P.; Perrino, M.; Zagami, P.; Corti, C.; et al. Avelumab plus axitinib in unresectable or metastatic type B3 thymomas and thymic carcinomas (CAVEATT): A single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022, 23, 1287–1296. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. WHO Panel. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Manthri, S.; Rehman, H.H.; Costello, P.N.; Chakraborty, K. Thymic basaloid carcinoma: A rare clinical entity. BMJ Case Rep. 2019, 12, e231980. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.H.; Gorton, A.; Tully, A.; Podbielski, F.J. Surgical management of locally invasive basaloid carcinoma of thymic gland. J. Surg. Case Rep. 2021, 2021, rjab531. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Phen, S.; Wang, M.X.; Kelling, M.; Bhattal, G.K. Metastatic basaloid squamous cell carcinoma of thymic origin. BMJ Case Rep. 2019, 12, e228860. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Buero, A.; Quadrelli, S.; Pankl, L.G.; Vigovich, F. Two-year disease remission of an unresectable basaloid thymic carcinoma with second line chemotherapy drugs: Report of a case. Pan Afr. Med. J. 2019, 33, 53. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Su, C.; Zhu, X.; Wang, Q.; Zhang, J. A basaloid carcinoma with multilocular thymic cyst mimicking a mediastinal teratoma. J. Cardiothorac. Surg. 2024, 19, 198. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Siddiqui, S.; Connelly, T.; Keita, L.; Blazkova, S.; Veerasingam, D. Thymic carcinoma presenting as atypical chest pain. BMJ Case Rep. 2015, 2015, bcr2015211374. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Suemitsu, R.; Takeo, S.; Momosaki, S.; Furuya, K. Thymic basaloid carcinoma with aggressive invasion of the lung and pericardium: Report of a case. Surg. Today 2011, 41, 986–988. [Google Scholar] [CrossRef] [PubMed]
- Bhora, F.Y.; Chen, D.J.; Detterbeck, F.C.; Asamura, H.; Falkson, C.; Filosso, P.L.; Giaccone, G.; Huang, J.; Kim, J.; Kondo, K.; et al. Staging and Prognostic Factors Committee; Advisory Boards. The ITMIG/IASLC Thymic Epithelial Tumors Staging Project: A Proposed Lymph Node Map for Thymic Epithelial Tumors in the Forthcoming 8th Edition of the TNM Classification of Malignant Tumors. J. Thorac. Oncol. 2014, 9 (Suppl. S2), S88–S96. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.G.; Familiari, U.; Papotti, M.; Rosai, J. Thymic basaloid carcinoma: A clinicopathologic study of 12 cases, with a general discussion of basaloid carcinoma and its relationship with adenoid cystic carcinoma. Am. J. Surg. Pathol. 2009, 33, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).