
Synergistic Efficacy of WST11-VTP and P-Selectin-Targeted Nanotherapy in a Preclinical Prostate Cancer Model

 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simple Summary
Abstract
1. Introduction
2. Methodology
2.1. Ethical Aspects
2.2. Cell Culture
2.3. Preparation of Nanoparticles Loaded with Enzalutamide or Paclitaxel
2.4. In Vivo Studies
2.4.1. Vascular-Targeted Photodynamic Therapy (VTP)
2.4.2. Radiation Therapy (RT)
2.4.3. Nanoparticles Administration
2.4.4. Imaging
2.4.5. Tumor Monitoring
2.5. Statistical Analysis
3. Results
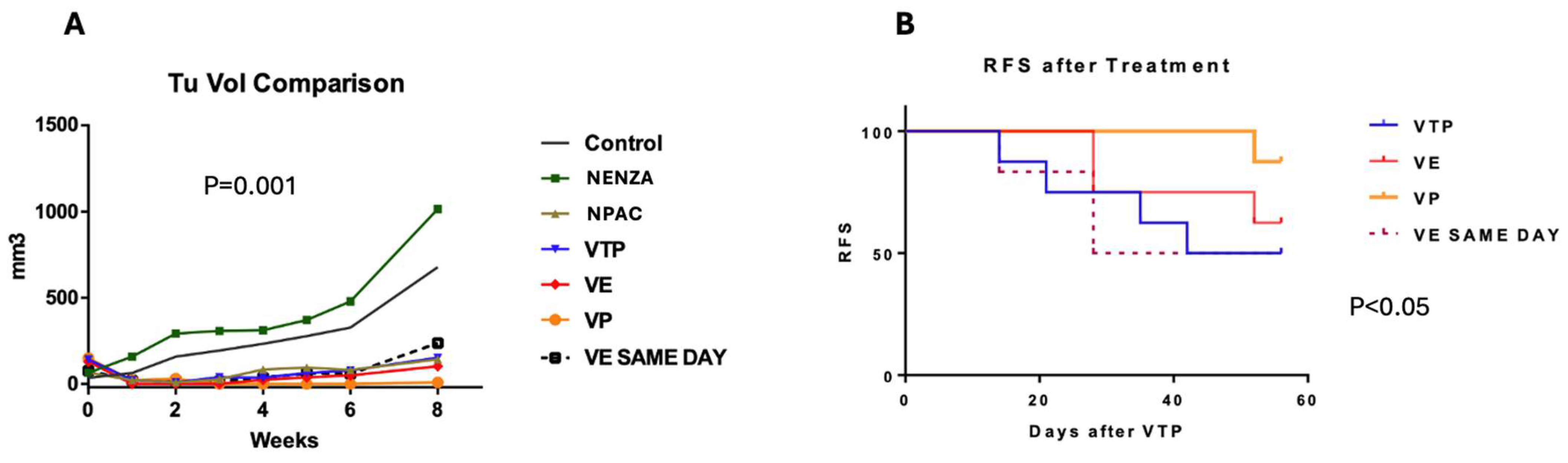
3.1. The Evaluation of the Oncological Effect of the Association Between VTP and Nanoparticles Carrying Paclitaxel or Enzalutamide, Including the Administration Time
3.2. The Evaluation of the Intra-Tumor Concentration Time of Nanoparticles Carrying Paclitaxel or Enzalutamide
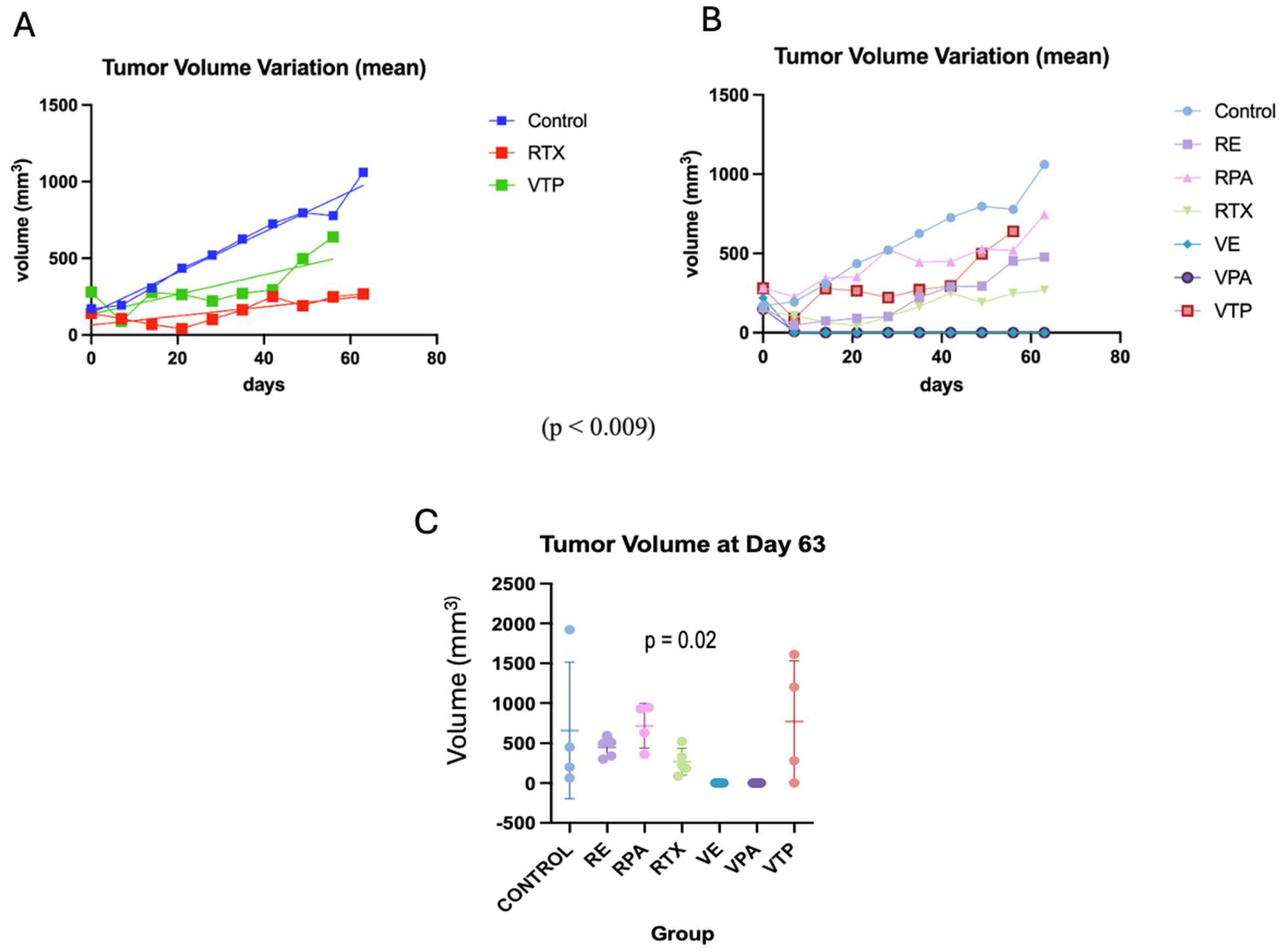
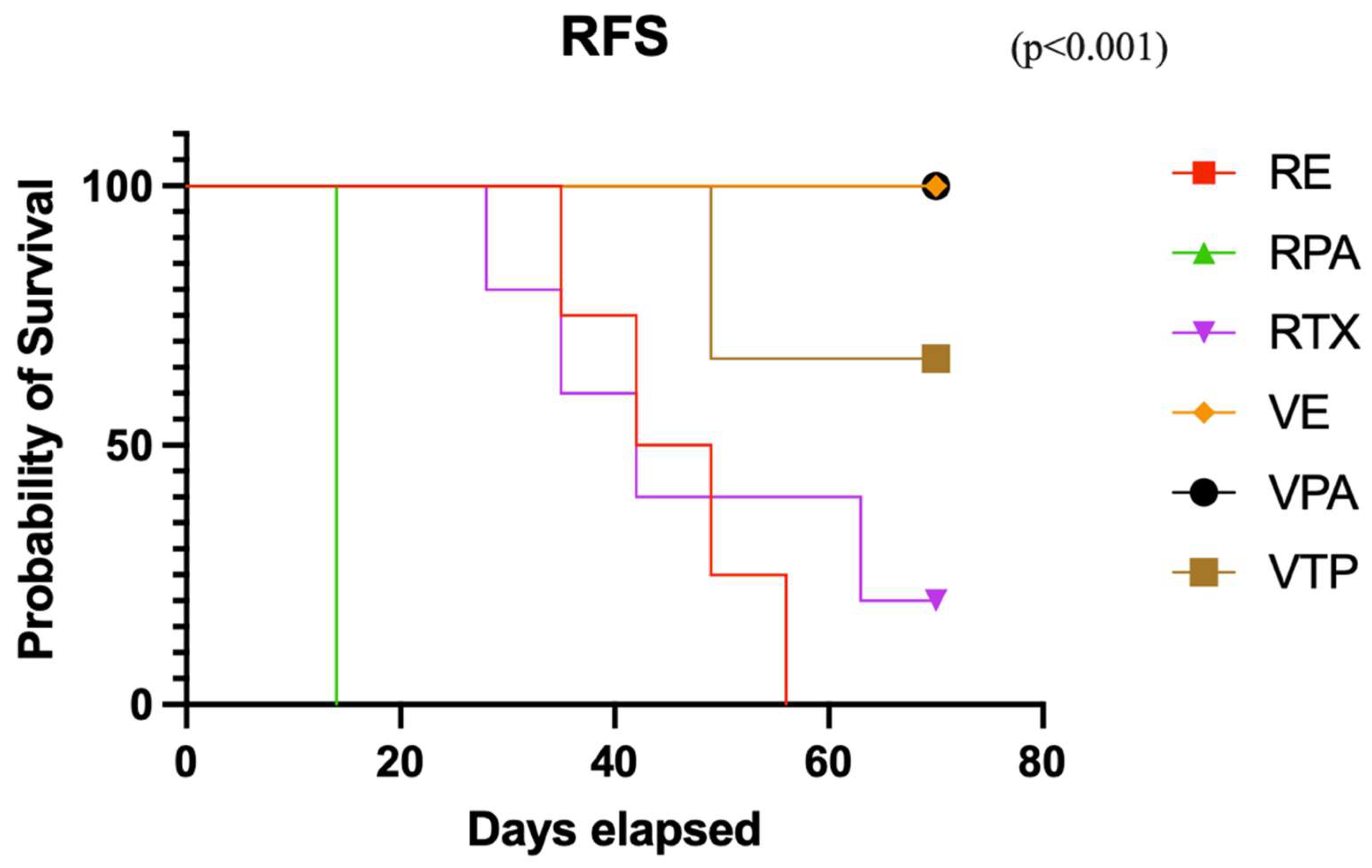
3.3. An Evaluation and Comparison of the Oncological Effects Between VTP and Radiation Therapy
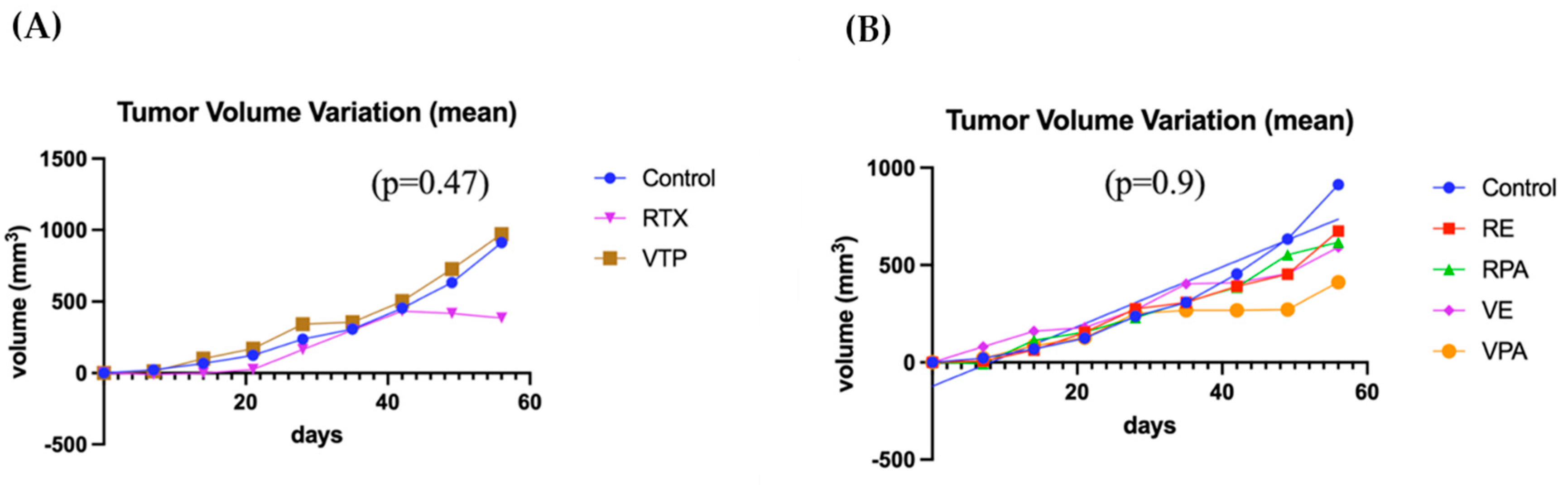
3.4. Evaluation of Induction and Oncological Efficacy of VTP and Radiotherapy in Synchronous Untreated Contralateral Tumors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Corsini, C.; Bergengren, O.; Carlsson, S.; Garmo, H.; Hjelm-Eriksson, M.; Fransson, P.; Kindblom, J.; Robinson, D.; Westerberg, M.; Stattin, P.; et al. Patient-reported Side Effects 1 Year After Radical Prostatectomy or Radiotherapy for Prostate Cancer: A Register-based Nationwide Study. Eur. Urol. Oncol. 2024, 7, 605–613. [Google Scholar] [CrossRef]
- Hoffman, K.E.; Penson, D.F.; Zhao, Z.; Huang, L.-C.; Conwill, R.; Laviana, A.A.; Joyce, D.D.; Luckenbaugh, A.N.; Goodman, M.; Hamilton, A.S.; et al. Patient-Reported Outcomes Through 5 Years for Active Surveillance, Surgery, Brachytherapy, or External Beam Radiation With or Without Androgen Deprivation Therapy for Localized Prostate Cancer. JAMA 2020, 323, 149–163. [Google Scholar] [CrossRef]
- Bagheri, H.; Mahdavi, S.R.; Geramifar, P.; Neshasteh-Riz, A.; Rad, M.S.; Dadgar, H.; Arabi, H.; Zaidi, H. An Update on the Role of mpMRI and (68) Ga-PSMA PET Imaging in Primary and Recurrent Prostate Cancer. Clin. Genitourin. Cancer 2024, 22, 102076. [Google Scholar] [CrossRef] [PubMed]
- Kurohane, K.; Tominaga, A.; Sato, K.; North, J.R.; Namba, Y.; Oku, N. Photodynamic therapy targeted to tumor-induced angiogenic vessels. Cancer Lett. 2001, 167, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Pogue, B.W.; Hoopes, P.J.; Hasan, T. Vascular and cellular targeting for photodynamic therapy. Crit. Rev. Eukaryot. Gene Expr. 2006, 16, 279–305. [Google Scholar] [CrossRef]
- Madar-Balakirski, N.; Tempel-Brami, C.; Kalchenko, V.; Brenner, O.; Varon, D.; Scherz, A.; Salomon, Y.; Secomb, T.W. Permanent occlusion of feeding arteries and draining veins in solid mouse tumors by vascular targeted photodynamic therapy (VTP) with Tookad. PLoS ONE 2010, 5, e10282. [Google Scholar] [CrossRef]
- Nogueira, L.; Tracey, A.T.; Alvim, R.; Reisz, P.; Scherz, A.; Coleman, J.A.; Kim, K. Developments in Vascular-Targeted Photodynamic Therapy for Urologic Malignancies. Molecules 2020, 25, 5417. [Google Scholar] [CrossRef]
- Tracey, A.T.; Nogueira, L.M.; Alvim, R.G.; Coleman, J.A.; Murray, K.S. Focal therapy for primary and salvage prostate cancer treatment: A narrative review. Transl. Androl. Urol. 2021, 10, 3144–3154. [Google Scholar] [CrossRef]
- Murray, K.S.; Winter, A.G.; Corradi, R.B.; LaRosa, S.; Jebiwott, S.; Somma, A.; Takaki, H.; Srimathveeravalli, G.; Lepherd, M.; Monette, S.; et al. Treatment Effects of WST11 Vascular Targeted Photodynamic Therapy for Urothelial Cell Carcinoma in Swine. J. Urol. 2016, 196, 236–243. [Google Scholar] [CrossRef]
- Corradi, R.B.; LaRosa, S.; Jebiwott, S.; Murray, K.S.; Rosenzweig, B.; Somma, A.J.; Gomez, R.S.; Scherz, A.; Kim, K.; Coleman, J.A. Effectiveness of the combination of vascular targeted photodynamic therapy and anti-cytotoxic T-lymphocyte-associated antigen 4 in a preclinical mouse model of urothelial carcinoma. Int. J. Urol. 2019, 26, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.; Sjoberg, D.; Nogueira, L.; Tracey, A.; Alvim, R.; Reisz, P.; Demac, Q.; Benfante, N.; Nagar, K.; Thomas, J.; et al. Final Results of a Phase I Trial of WST-11 (TOOKAD Soluble) Vascular-targeted Photodynamic Therapy for Upper Tract Urothelial Carcinoma. J. Urol. 2023, 209, 863–871. [Google Scholar] [CrossRef]
- Margulis, V.; Kaufman, R.P.; Marcq, G.; Shore, N.D.; Colombel, M.; Uchio, E.M.; Psutka, S.P.; Aller, M.; Rausch, S.; Raventos, C.; et al. ENLIGHTED phase 3 study: Efficacy and safety of padeliporfin vascular targeted photodynamic therapy (VTP) for treatment of low-grade upper tract urothelial cancer (LG UTUC). J. Clin. Oncol. 2024, 42 (Suppl. S16), TPS4622. [Google Scholar] [CrossRef]
- Azzouzi, A.R.; Vincendeau, S.; Barret, E.; Cicco, A.; Kleinclauss, F.; van der Poel, H.G.; Stief, C.G.; Rassweiler, J.; Salomon, G.; Solsona, E.; et al. Padeliporfin vascular-targeted photodynamic therapy versus active surveillance in men with low-risk prostate cancer (CLIN1001 PCM301): An open-label, phase 3, randomised controlled trial. Lancet Oncol. 2017, 18, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Flegar, L.; Buerk, B.; Proschmann, R.; Propping, S.; Groeben, C.; Baunacke, M.; Herout, R.; Huber, J.; Thomas, C.; Borkowetz, A. Vascular-targeted Photodynamic Therapy in Unilateral Low-risk Prostate Cancer in Germany: 2-yr Single-centre Experience in a Real-world Setting Compared with Radical Prostatectomy. Eur. Urol. Focus 2022, 8, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Laubli, H.; Borsig, L. Selectins promote tumor metastasis. Semin. Cancer Biol. 2010, 20, 169–177. [Google Scholar] [CrossRef]
- Bonfanti, R.; Furie, B.C.; Furie, B.; Wagner, D.D. PADGEM (GMP140) is a component of Weibel-Palade bodies of human endothelial cells. Blood 1989, 73, 1109–1112. [Google Scholar] [CrossRef]
- Hallahan, D.E.; Virudachalam, S. Accumulation of P-selectin in the lumen of irradiated blood vessels. Radiat. Res. 1999, 152, 6–13. [Google Scholar] [CrossRef]
- Shamay, Y.; Elkabets, M.; Li, H.; Shah, J.; Brook, S.; Wang, F.; Adler, K.; Baut, E.; Scaltriti, M.; Jena, P.V.; et al. P-selectin is a nanotherapeutic delivery target in the tumor microenvironment. Sci. Transl. Med. 2016, 8, 345ra87. [Google Scholar] [CrossRef]
- Venkatesan, J.; Murugan, S.S.; Seong, G.H. Fucoidan-based nanoparticles: Preparations and applications. Int. J. Biol. Macromol. 2022, 217, 652–667. [Google Scholar] [CrossRef] [PubMed]
- Koshrovski-Michael, S.; Ajamil, D.R.; Dey, P.; Kleiner, R.; Tevet, S.; Epshtein, Y.; Buzhor, M.G.; Khoury, R.; Pozzi, S.; Shenbach-Koltin, G.; et al. Two-in-one nanoparticle platform induces a strong therapeutic effect of targeted therapies in P-selectin-expressing cancers. Sci. Adv. 2024, 10, eadr4762. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.; Sriram, V.; Xu, Z.; Harris, G.M.; Lee, J.-Y. Fucoidan-Doxorubicin Nanoparticles Targeting P-Selectin for Effective Breast Cancer Therapy. Carbohydr. Polym. 2020, 249, 116837. [Google Scholar] [CrossRef] [PubMed]
- Shastry, M.; Gupta, A.; Chandarlapaty, S.; Young, M.; Powles, T.; Hamilton, E. Rise of Antibody-Drug Conjugates: The Present and Future. Am. Soc. Clin. Oncol. Educ. Book 2023, 43, e390094. [Google Scholar] [CrossRef]
- Fu, Z.; Li, S.; Han, S.; Shi, C.; Zhang, Y. Antibody drug conjugate: The “biological missile” for targeted cancer therapy. Signal Transduct. Target. Ther. 2022, 7, 93. [Google Scholar] [CrossRef]
- Kim, K.; Watson, P.A.; Lebdai, S.; Jebiwott, S.; Somma, A.J.; La Rosa, S.; Mehta, D.; Murray, K.S.; Lilja, H.; Ulmert, D.; et al. Androgen Deprivation Therapy Potentiates the Efficacy of Vascular Targeted Photodynamic Therapy of Prostate Cancer Xenografts. Clin. Cancer Res. 2018, 24, 2408–2416. [Google Scholar] [CrossRef]
- Siva, S.; MacManus, M.P.; Martin, R.F.; Martin, O.A. Abscopal effects of radiation therapy: A clinical review for the radiobiologist. Cancer Lett. 2015, 356, 82–90. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, L.; Alvim, R.; Baker, H.; Nagar, K.; Thomas, J.; Alvim, L.; Kim, K.; Heller, D.A.; Reis, A.; Scherz, A.; et al. Synergistic Efficacy of WST11-VTP and P-Selectin-Targeted Nanotherapy in a Preclinical Prostate Cancer Model. Cancers 2025, 17, 2361. https://doi.org/10.3390/cancers17142361
Nogueira L, Alvim R, Baker H, Nagar K, Thomas J, Alvim L, Kim K, Heller DA, Reis A, Scherz A, et al. Synergistic Efficacy of WST11-VTP and P-Selectin-Targeted Nanotherapy in a Preclinical Prostate Cancer Model. Cancers. 2025; 17(14):2361. https://doi.org/10.3390/cancers17142361
Chicago/Turabian StyleNogueira, Lucas, Ricardo Alvim, Hanan Baker, Karan Nagar, Jasmine Thomas, Laura Alvim, Kwanghee Kim, Daniel A. Heller, Augusto Reis, Avigdor Scherz, and et al. 2025. "Synergistic Efficacy of WST11-VTP and P-Selectin-Targeted Nanotherapy in a Preclinical Prostate Cancer Model" Cancers 17, no. 14: 2361. https://doi.org/10.3390/cancers17142361
APA StyleNogueira, L., Alvim, R., Baker, H., Nagar, K., Thomas, J., Alvim, L., Kim, K., Heller, D. A., Reis, A., Scherz, A., & Coleman, J. (2025). Synergistic Efficacy of WST11-VTP and P-Selectin-Targeted Nanotherapy in a Preclinical Prostate Cancer Model. Cancers, 17(14), 2361. https://doi.org/10.3390/cancers17142361