
Efficacy and Safety of Chemotherapy Combined with Hormonal Therapy in Heavily Pretreated Advanced Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer (ELSA/KGOG3049): A Multicenter Pilot Study


 , , , , , ,
, , , , , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Outcomes
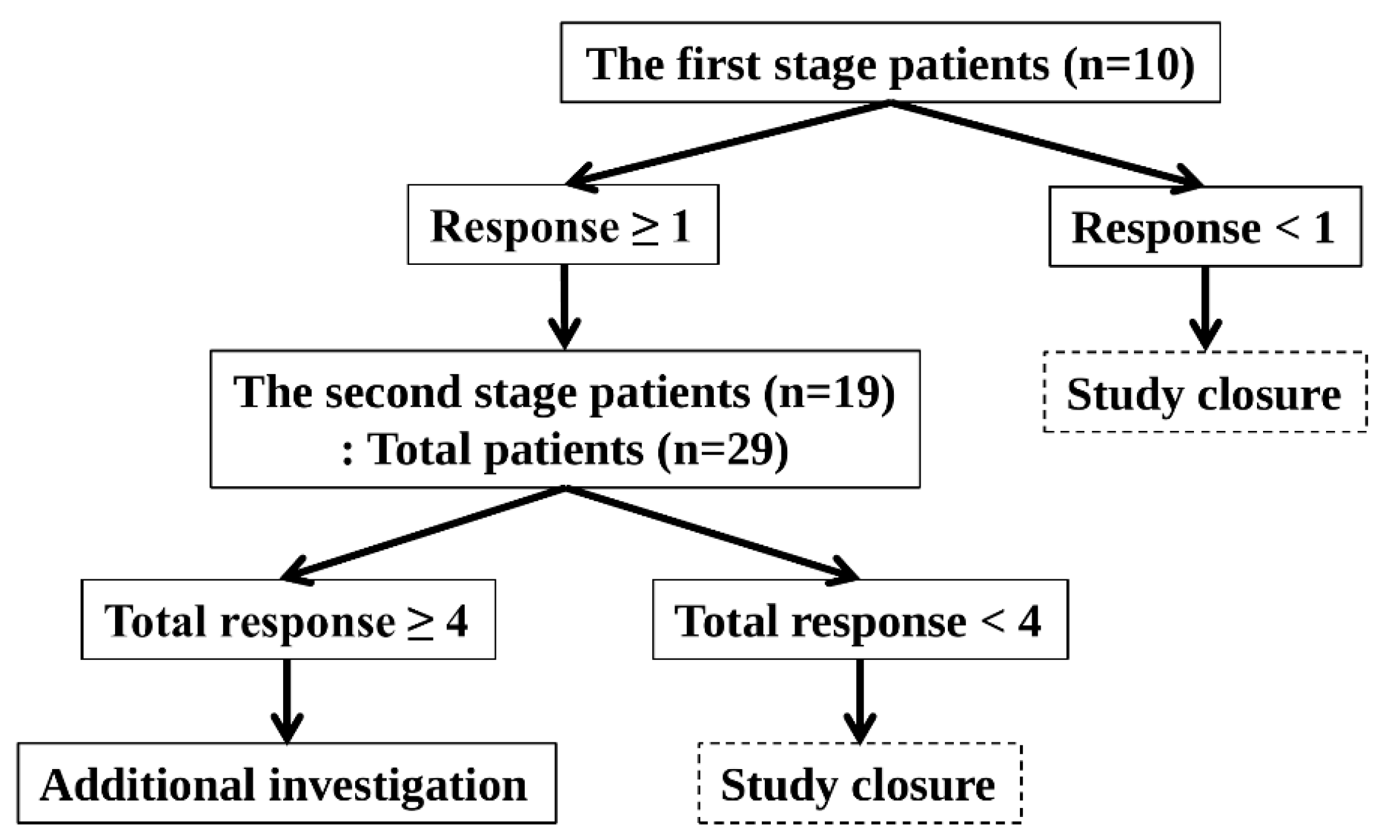
2.4. Sample Size
2.5. Statistics
3. Results
3.1. Baseline Characteristics
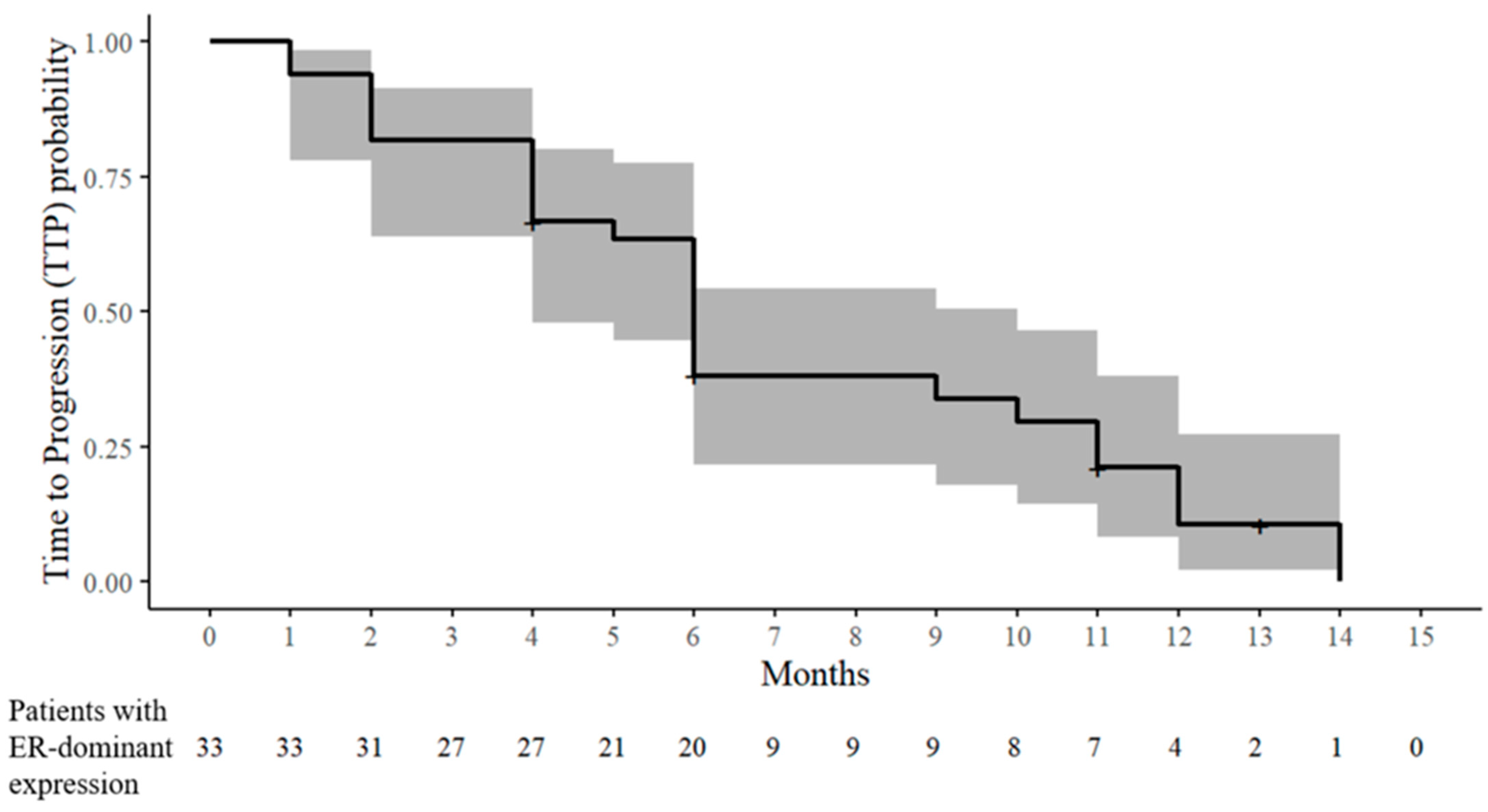
3.2. Response Assessment in Patients with ER-Dominant Expression
3.3. Response Assessment in Patients with PRa-Dominant Expression
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Hennessy, B.T.; Coleman, R.L.; Markman, M. Ovarian cancer. Lancet 2009, 374, 1371–1382. [Google Scholar] [CrossRef]
- Foley, O.W.; Rauh-Hain, J.A.; Del Carmen, M.G. Recurrent epithelial ovarian cancer: An update on treatment. Oncology (Williston Park) 2013, 27, 288–294, 298. [Google Scholar] [PubMed]
- Hanker, L.C.; Loibl, S.; Burchardi, N.; Pfisterer, J.; Meier, W.; Pujade-Lauraine, E.; Ray-Coquard, I.; Sehouli, J.; Harter, P.; du Bois, A. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann. Oncol. 2012, 23, 2605–2612. [Google Scholar] [CrossRef] [PubMed]
- Sieh, W.; Köbel, M.; Longacre, T.A.; Bowtell, D.D.; Defazio, A.; Goodman, M.T.; Høgdall, E.; Deen, S.; Wentzensen, N.; Moysich, K.B.; et al. Hormone-receptor expression and ovarian cancer survival: An Ovarian Tumor Tissue Analysis consortium study. Lancet Oncol. 2013, 14, 853–862. [Google Scholar] [CrossRef] [PubMed]
- van Kruchten, M.; van der Marel, P.; de Munck, L.; Hollema, H.; Arts, H.; Timmer-Bosscha, H.; de Vries, E.; Hospers, G.; Reyners, A. Hormone receptors as a marker of poor survival in epithelial ovarian cancer. Gynecol. Oncol. 2015, 138, 634–639. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Bi, R.; Ju, X.; Chen, X.; Yang, W.; Wu, X. A clinically applicable molecular classification for high-grade serous ovarian cancer based on hormone receptor expression. Sci. Rep. 2016, 6, 25408. [Google Scholar] [CrossRef]
- Chan, K.K.L.; Siu, M.K.Y.; Jiang, Y.X.; Wang, J.J.; Wang, Y.; Leung, T.H.Y.; Liu, S.S.; Cheung, A.N.Y.; Ngan, H.Y.S. Differential expression of estrogen receptor subtypes and variants in ovarian cancer: Effects on cell invasion, proliferation and prognosis. BMC Cancer 2017, 17, 606. [Google Scholar] [CrossRef]
- Voutsadakis, I.A. Hormone Receptors in Serous Ovarian Carcinoma: Prognosis, Pathogenesis, and Treatment Considerations. Clin. Med. Insights Oncol. 2016, 10, 17–25. [Google Scholar] [CrossRef]
- Zheng, H.; Kavanagh, J.; Hu, W.; Liao, Q.; Fu, S. Hormonal therapy in ovarian cancer. Int. J. Gynecol. Cancer 2006, 17, 325–338. [Google Scholar] [CrossRef]
- Modugno, F.; Laskey, R.; Smith, A.L.; Andersen, C.L.; Haluska, P.; Oesterreich, S. Hormone response in ovarian cancer: Time to reconsider as a clinical target? Endocr. Relat. Cancer 2012, 19, R255–R279. [Google Scholar] [CrossRef]
- Panici, P.B.; Greggi, S.; Amoroso, M.; Scambia, G.; Battaglia, F.A.; Gebbia, V.; Salerno, G.; Paratore, M.P.; Mancuso, S. A combination of platinum and tamoxifen in advanced ovarian cancer failing platinum-based chemotherapy: Results of a Phase II study. Int. J. Gynecol. Cancer 2001, 11, 438–444. [Google Scholar] [CrossRef]
- Niwa, K.; Onogi, K.; Wu, Y.; Mori, H.; Harrigan, R.C.; Tamaya, T. Clinical implication of medroxyprogesterone acetate against advanced ovarian carcinoma: A pilot study. Eur. J. Gynaecol. Oncol. 2008, 29, 252–255. [Google Scholar] [PubMed]
- Schwartz, P.E.; Chambers, J.T.; Kohorn, E.I.; Chambers, S.K.; Weitzman, H.; Voynick, I.M.; MacLusky, N.; Naftolin, F. Tamoxifen in combination with cytotoxic chemotherapy in advanced epithelial ovarian cancer. A prospective randomized trial. Cancer 1989, 63, 1074–1078. [Google Scholar] [CrossRef]
- Senn, H.J.; Lei, D.; Castaño-Almendral, A.; Brunner, K.W.; Martz, G.; Obrecht, P.; Melchert, F.; Rhomberg, W. Chemo-(hormonal)-therapy of advanced ovarian neoplasms in FIGO stages III and IV. Prospective SAKK-study 20/71. Schweiz. Med. Wochenschr. 1980, 110, 1202–1208. [Google Scholar] [PubMed]
- Emons, G.; Gorchev, G.; Sehouli, J.; Wimberger, P.; Stähle, A.; Hanker, L.; Hilpert, F.; Sindermann, H.; Gründker, C.; Harter, P. Efficacy and safety of AEZS-108 (INN: Zoptarelin Doxorubicin Acetate) an LHRH agonist linked to doxorubicin in women with platinum refractory or resistant ovarian cancer expressing LHRH receptors: A multicenter Phase II trial of the ago-study group (AGO GYN 5). Gynecol. Oncol. 2014, 133, 427–432. [Google Scholar] [CrossRef]
- Manning-Geist, B.L.; Gordhandas, S.B.; Giri, D.D.; Iasonos, A.; Zhou, Q.; Girshman, J.; O’CEarbhaill, R.E.; Zamarin, D.; Lichtman, S.M.; Sabbatini, P.J.; et al. Phase II study of enzalutamide in androgen receptor positive, recurrent, high- and low-grade serous ovarian cancer. Gynecol. Oncol. 2021, 164, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.; Pervez, S. Allred scoring for ER reporting and it’s impact in clearly distinguishing ER negative from ER positive breast cancers. J. Pak. Med. Assoc. 2010, 60, 350–353. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE). 2021. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 1 December 2019).
- Bruchim, I.; Jarchowsky-Dolberg, O.; Fishman, A. Advanced (>second) line chemotherapy in the treatment of patients with recurrent epithelial ovarian cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 166, 94–98. [Google Scholar] [CrossRef]
- Moore, K.N.; Angelergues, A.; Konecny, G.E.; García, Y.; Banerjee, S.; Lorusso, D.; Lee, J.-Y.; Moroney, J.W.; Colombo, N.; Roszak, A.; et al. Mirvetuximab Soravtansine in FRα-Positive, Platinum-Resistant Ovarian Cancer. N. Engl. J. Med. 2023, 389, 2162–2174. [Google Scholar] [CrossRef]
- Matulonis, U.A.; Lorusso, D.; Oaknin, A.; Pignata, S.; Dean, A.; Denys, H.; Colombo, N.; Van Gorp, T.; Konner, J.A.; Marin, M.R.; et al. Efficacy and Safety of Mirvetuximab Soravtansine in Patients With Platinum-Resistant Ovarian Cancer With High Folate Receptor Alpha Expression: Results From the SORAYA Study. J. Clin. Oncol. 2023, 41, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.-Y.; Banerjee, S.; González-Martín, A.; Jung, K.H.; Ługowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J. Clin. Oncol. 2024, 42, 47–58. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G. Morphological subtypes of ovarian carcinoma: A review with emphasis on new developments and pathogenesis. Pathology 2011, 43, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Peres, L.C.; Cushing-Haugen, K.L.; Köbel, M.; Harris, H.R.; Berchuck, A.; Rossing, M.A.; Schildkraut, J.M.; Doherty, J.A. Invasive Epithelial Ovarian Cancer Survival by Histotype and Disease Stage. J. Natl. Cancer Inst. 2019, 111, 60–68. [Google Scholar] [CrossRef]
- Markman, M.; Webster, K.; Zanotti, K.; Peterson, G.; Kulp, B.; Belinson, J. Phase 2 trial of carboplatin plus tamoxifen in platinum-resistant ovarian cancer and primary carcinoma of the peritoneum. Gynecol. Oncol. 2004, 94, 404–408. [Google Scholar] [CrossRef]
- Velden, J.; Gitsch, G.; Wain, G.; Friedlander, M.; Hacker, N. Tamoxifen in patients with advanced epithelial ovarian cancer. Int. J. Gynecol. Cancer 1995, 5, 301–305. [Google Scholar] [CrossRef]
- Mangioni, C.; Franceschi, S.; Vecchia, C.; D’Incalci, M. High-dose medroxyprogesterone acetate (MPA) in advanced epithelial ovarian cancer resistant to first- or second-line chemotherapy. Gynecol. Oncol. 1981, 12, 314–318. [Google Scholar] [CrossRef]
- Malfetano, J.; Beecham, J.B.; Bundy, B.N.; Hatch, K.D. A Phase II Trial of Medroxyprogesterone Acetate in Epithelial Ovarian Cancers. Am. J. Clin. oncology 1993, 16, 149–151. [Google Scholar] [CrossRef]
- van Weelden, W.J.; Birkendahl, P.B.; Lalisang, R.I.; IntHout, J.; Kruitwagen, R.F.P.M.; Romano, A.; Pijnenborg, J.M.A. The effect of progestin therapy in advanced and recurrent endometrial cancer: A systematic review and meta-analysis. Int. J. Obstet. Gynaecol. 2022, 130, 143–152. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Ju, X.; Bi, R.; Chen, X.; Yang, W.; Wu, X. Hormone receptor expression profiles differ between primary and recurrent high-grade serous ovarian cancers. Oncotarget 2017, 8, 32848–32855. [Google Scholar] [CrossRef]
- Vetter, M.; Stadlmann, S.; Bischof, E.; Margarint, E.L.G.; Schötzau, A.; Singer, G.; Heinzelmann-Schwarz, V.; Montavon, C. Hormone Receptor Expression in Primary and Recurrent High-Grade Serous Ovarian Cancer and Its Implications in Early Maintenance Treatment. Int. J. Mol. Sci. 2022, 23, 14242. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Age | Stage | Histology | Previous Chemotherapeutic Line | Current Chemotherapeutic Line | Method for Obtaining Tissue for Testing HR Expression | Tissue Used for Testing HR Expression | Status of HR Expression (Allred Scores) | Status of HR Expression | Hormonal Agent | Chemotherapeutic Agent | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 65 | 3C | HGSC | 2nd | 3rd | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 5) | ER-dominant | Tamoxifen | Belotecan |
| Case 2 | 63 | 4B | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 8, PRa: 3) | ER-dominant | Tamoxifen | Weekly paclitaxel |
| Case 3 | 55 | 3A | HGSC | 7th | 8th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 0) | ER-dominant | Tamoxifen | Cyclophosphamide |
| Case 4 | 66 | 3C | HGSC | 7th | 8th | Primary surgery | Ovary | ER-dominant (ER: 4, PRa: 0) | ER-dominant | Tamoxifen | Vinorelbine |
| Case 5 | 44 | 3B | HGSC | 8th | 9th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 2) | ER-dominant | Tamoxifen | Cyclophosphamide |
| Case 6 | 62 | 3C | HGSC | 7th | 8th | Primary surgery | Fallopian tube | ER-dominant (ER: 7, PRa: 3) | ER-dominant | Tamoxifen | Cyclophosphamide |
| Case 7 | 70 | 3C | HGSC | 5th | 6th | Primary surgery | Peritoneum | ER-dominant (ER: 5, PRa: 4) | ER-dominant | Tamoxifen | Vinorelbine |
| Case 8 | 59 | 3A | HGSC | 8th | 9th | Surgery at 1st recurrence | Pelvic lymph node | ER-dominant (ER: 7, PRa: 5) | ER-dominant | Tamoxifen | Cyclophosphamide |
| Case 9 | 57 | 4B | HGSC | 5th | 6th | Primary surgery | Ovary | ER-dominant (ER: 8, PRa: 4) | ER-dominant | Tamoxifen | Cyclophosphamide |
| Case 10 | 48 | 3C | HGSC | 6th | 7th | Primary surgery | Omentum | ER-dominant (ER: 7, PRa: 6) | ER-dominant | Tamoxifen | Docetaxel/carboplatin |
| Case 11 | 74 | 3C | HGSC | 7th | 8th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 5) | ER-dominant | Tamoxifen | Vinorelbine |
| Case 12 | 53 | 3C | HGSC | 2nd | 3rd | Primary surgery | Ovary | ER-dominant (ER: 5, PRa: 5) | ER-dominant | Tamoxifen | Weekly gemcitabine |
| Case 13 | 66 | 4B | HGSC | 6th | 7th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 0) | ER-dominant | Tamoxifen | Vinorelbine |
| Case 14 | 50 | 4B | HGSC | 4th | 5th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 6) | ER-dominant | Tamoxifen | Topotecan/carboplatin |
| Case 15 | 61 | 2A | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 6, PRa: 3) | ER-dominant | Tamoxifen | Gemcitabine |
| Case 16 | 65 | 4B | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 3) | ER-dominant | Tamoxifen | Weekly paclitaxel |
| Case 17 | 71 | 3B | HGSC | 3rd | 4th | Primary surgery | Mesentery | ER-dominant (ER: 7, PRa: 5) | ER-dominant | Tamoxifen | Topotecan |
| Case 18 | 50 | 4A | HGSC | 3rd | 4th | Primary surgery | Colon | ER-dominant (ER: 7, PRa: 6) | ER-dominant | Tamoxifen | Topotecan/carboplatin |
| Case 19 | 51 | 3C | HGSC | 5th | 6th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 4) | ER-dominant | Tamoxifen | Docetaxel triweekly |
| Case 20 | 63 | 3C | HGSC | 2nd | 3rd | Primary surgery | Ovary | ER-dominant (ER: 8, PRa: 4) | ER-dominant | Tamoxifen | Topotecan/cisplatin |
| Case 21 | 55 | 4B | HGSC | 2nd | 3rd | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 4) | ER-dominant | Tamoxifen | Pegylated liposomal doxorubicin |
| Case 22 | 41 | 3B | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 6, PRa: 4) | ER-dominant | Tamoxifen | Weekly topotecan |
| Case 23 | 49 | 3C | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 4, PRa: 3) | ER-dominant | Tamoxifen | Topotecan |
| Case 24 | 67 | 4B | HGSC | 2nd | 3rd | Primary surgery | Salpinx | ER-dominant (ER: 6, PRa: 0) | ER-dominant | Tamoxifen | Pegylated liposomal doxorubicin |
| Case 25 | 50 | 3C | HGSC | 2nd | 3rd | Primary surgery | Ovary | ER-dominant (ER: 5, PRa: 4) | ER-dominant | Tamoxifen | Topotecan/cisplatin |
| Case 26 | 51 | 3C | HGSC | 5th | 6th | Surgery at the 5th recurrence | Spleen | ER-dominant (ER: 8, PRa: 7) | ER-dominant | Tamoxifen | Pegylated liposomal doxorubicin |
| Case 27 | 60 | 3C | HGSC | 5th | 6th | Surgery at the 5th recurrence | Paraaortic lymph node | ER-dominant (ER: 8, PRa: 2) | ER-dominant | Tamoxifen | Gemcitabine/carboplatin |
| Case 28 | 65 | 3C | HGSC | 2nd | 3rd | Biopsy at the 2nd recurrence | Supraclavicular lymph node | ER-dominant (ER: 7, PRa: 4) | ER-dominant | Tamoxifen | Belotecan |
| Case 29 | 56 | 3C | HGSC | 4th | 5th | Primary surgery | Rectum | ER-dominant (ER: 7, PRa: 3) | ER-dominant | Tamoxifen | Pegylated liposomal doxorubicin |
| Case 30 | 63 | 4B | HGSC | 4th | 5th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 5) | ER-dominant | Tamoxifen | Pegylated liposomal doxorubicin/carboplatin |
| Case 31 | 59 | 3C | HGSC | 3rd | 4th | Primary surgery | Ovary | ER-dominant (ER: 6, PRa: 4) | ER-dominant | Tamoxifen | Paclitaxel/cisplatin |
| Case 32 | 70 | 3C | HGSC | 4th | 5th | Primary surgery | Ovary | ER-dominant (ER: 7, PRa: 6) | ER-dominant | Tamoxifen | Topotecan |
| Case 33 | 55 | 1C | HGSC | 4th | 5th | Primary surgery | Ovary | ER-dominant (ER: 6, PRa: 5) | ER-dominant | Tamoxifen | Topotecan |
| Case 34 | 65 | 3B | Clear cell | 3rd | 4th | Surgery at the 2nd recurrence | Liver | PRa-dominant (ER: 0, PRa: 6) | PRa-dominant | Megestrol acetate | Topotecan |
| Case 35 | 49 | 4B | Clear cell | 6th | 7th | Primary surgery | Ovary | PRa-dominant (ER: 2, PRa: 3) | PRa-dominant | Megestrol acetate | Vinorelbine |
| Case 36 | 60 | 3C | HGSC | 2nd | 3rd | Primary surgery | Ovary | PRa-dominant (ER: 4, PRa: 5) | PRa-dominant | Megestrol acetate | Docetaxcel/carboplatin |
| Response for 6 Months | Response After 6 Months | ||||
|---|---|---|---|---|---|
| CR | PRb | SD | PD | ||
| Case 1 | 2, 4, and 6 months | SD at 9 months and PD at 11 months a | |||
| Case 2 | 2, 4, and 6 months | PR at 10 months and PD at 14 months a | |||
| Case 3 | 2 months | 4 months | |||
| Case 4 | 2 and 4 months | 6 months | |||
| Case 5 | 2 and 4 months | 6 months | |||
| Case 6 | 2 months | 4 months | |||
| Case 7 | 2 months | ||||
| Case 8 | 2 months | 4 months | |||
| Case 9 | 2 and 4 months | 6 months | |||
| Case 10 | 2, 4, and 6 months | Dropout after SD at 9 and 11 months a | |||
| Case 11 | 2 months | ||||
| Case 12 | 2 months | 4 months | 6 months | ||
| Case 13 | 2 months | 4 months | |||
| Case 14 | 2 months | ||||
| Case 15 | 2 months | 4 months | |||
| Case 16 | 2, 4, and 6 months | Drop out c | |||
| Case 17 | 2 months | 4 and 6 months | SD at 9 months and PD at 12 months a | ||
| Case 18 | 2 and 4 months | 6 months | |||
| Case 19 | 2 months | ||||
| Case 20 | 2, 4, and 6 months | CR at 9 months and PD at 12 months a | |||
| Case 21 | 4 and 6 months | 2 months | Drop out c | ||
| Case 22 | 1 month | ||||
| Case 23 d | 2 and 4 months | ||||
| Case 24 | 2 months | 5 months | |||
| Case 25 | 2 and 4 months | 6 months | |||
| Case 26 | 2, 4, and 6 months | PD at 10 months a | |||
| Case 27 | 4 and 6 months | 2 months | Drop out c | ||
| Case 28 e | 2 and 6 months | 4 months | PR at 8 months and PD at 11 months a | ||
| Case 29 | 2 and 4 months | 6 months | |||
| Case 30 | 2 and 6 months | Dropout after SD at 10 and 13 months a | |||
| Case 31 | 4 months | 2 months | 6 months | PD at 9 months a | |
| Case 32 | 4 months | 6 months | |||
| Case 33 | 1 month | ||||
| Best ORR for 6 months | (9/33) 27.3% (95% CI, 12.1–42.5) | ||||
| ORR at 6 months | (6/32) 18.8% (95% CI, 5.2–32.3) | ||||
| CBR at 6 months | (12/32) 37.5% (95% CI, 20.7–54.3) | ||||
| PD until 6 months | (20/32) 62.5% (95% CI, 45.7–79.3) | ||||
| Chemotherapy Line | |||||||
|---|---|---|---|---|---|---|---|
| 3rd | 4th | 5th | 6th | 7th | 8th | 9th | |
| Total patients with the best objective response assessment for 6 months (n = 33) | 7/33 (100%) | 8/33 (100%) | 5/33 (100%) | 5/33 (100%) | 2/33 (100%) | 4/33 (100%) | 2/33 (100%) |
| Patients with the best objective response for 6 months (n) | 3/7 (42.9%) | 4/8 (50%) | 1/5 (20%) | 1/5 (20%) | 0 (0%) | 0 (0%) | 0 (0%) |
| CR | 0 (0%) | 1/8 (12.5%) a | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| PRb | 3/7 (42.9%) | 3/8 (37.5%) | 1/5 (20%) | 1/5 (20%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Total patients with response assessment at 6 months (n = 32) | 7/32 (100%) | 7/32 (100%) | 5/32 (100%) | 5/32 (100%) | 2/32 (100%) | 4/32 (100%) | 2/32 (100%) |
| Patients with objective response at 6 months (n) | 3/7 (42.9%) | 1/7 (14.3%) | 1/5 (20%) | 1/5 (20%) | 0 (0%) | 0 (0%) | 0 (0%) |
| CR | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| PRb | 3/7 (42.9%) | 1/7 (14.3%) | 1/5 (20%) | 1/5 (20%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Patients with SD at 6 months (n) | 1/7 (14.3%) | 3/7 (42.9%) | 0 (0%) | 1/5 (20%) | 1/2 (50%) | 0 (0%) | 0 (0%) |
| Patients with PD until 6 months (n) | 3/7 (42.9%) | 3/7 (42.9%) | 4/5 (80%) | 3/5 (60%) | 1/2 (50%) | 4/4 (100%) | 2/2 (100%) |
| Response for 6 Months | ||||
|---|---|---|---|---|
| CR | PRb | SD | PD | |
| Case 34 | 2 months | |||
| Case 35 | 2 months | |||
| Case 36 | 2 and 4 months | 6 months | ||
| Best ORR for 6 months | 0% | |||
| ORR at 6 months | 0% | |||
| CBR at 6 months | 0% | |||
| PD until 6 months | (3/3) 100% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Choi, C.H.; Park, S.-Y.; Kim, M.K.; Lee, K.H.; Lee, E.-J.; Lim, M.C.; Park, Y.H.; Kyung, M.S.; No, J.H.; et al. Efficacy and Safety of Chemotherapy Combined with Hormonal Therapy in Heavily Pretreated Advanced Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer (ELSA/KGOG3049): A Multicenter Pilot Study. Cancers 2025, 17, 2320. https://doi.org/10.3390/cancers17142320
Kim K, Choi CH, Park S-Y, Kim MK, Lee KH, Lee E-J, Lim MC, Park YH, Kyung MS, No JH, et al. Efficacy and Safety of Chemotherapy Combined with Hormonal Therapy in Heavily Pretreated Advanced Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer (ELSA/KGOG3049): A Multicenter Pilot Study. Cancers. 2025; 17(14):2320. https://doi.org/10.3390/cancers17142320
Chicago/Turabian StyleKim, Kidong, Chel Hun Choi, Sang-Yoon Park, Min Kyu Kim, Keun Ho Lee, Eun-Ju Lee, Myong Cheol Lim, Young Han Park, Min Sun Kyung, Jae Hong No, and et al. 2025. "Efficacy and Safety of Chemotherapy Combined with Hormonal Therapy in Heavily Pretreated Advanced Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer (ELSA/KGOG3049): A Multicenter Pilot Study" Cancers 17, no. 14: 2320. https://doi.org/10.3390/cancers17142320
APA StyleKim, K., Choi, C. H., Park, S.-Y., Kim, M. K., Lee, K. H., Lee, E.-J., Lim, M. C., Park, Y. H., Kyung, M. S., No, J. H., Suh, D. H., Lee, J.-W., Ahn, S., & Lee, B. (2025). Efficacy and Safety of Chemotherapy Combined with Hormonal Therapy in Heavily Pretreated Advanced Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer (ELSA/KGOG3049): A Multicenter Pilot Study. Cancers, 17(14), 2320. https://doi.org/10.3390/cancers17142320