
Is [177Lu]Lu-PSMA-617 Redefining Value in mCRPC Care? A Meta-Analysis of Clinical and Economic Endpoints

 ,
, 
 ,
,  , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Selection, Qualitative Analysis and Economic Evaluation
- -
- The article was available in English and accessible in full-text format (including peer-reviewed papers, congress abstracts with full data, or oral/poster presentations).
- -
- The study population consisted of patients with mCRPC treated with [177Lu]Lu-PSMA compared to SOC, ARTA, or Cabazitaxel;
- -
- The study reported Kaplan–Meier curves for rPFS and/or OS.
2.2. Data Extraction
2.3. Statistical Method
2.3.1. Reconstruction of Survival Data
2.3.2. Methodology for Break-Even Cost Analysis
3. Results
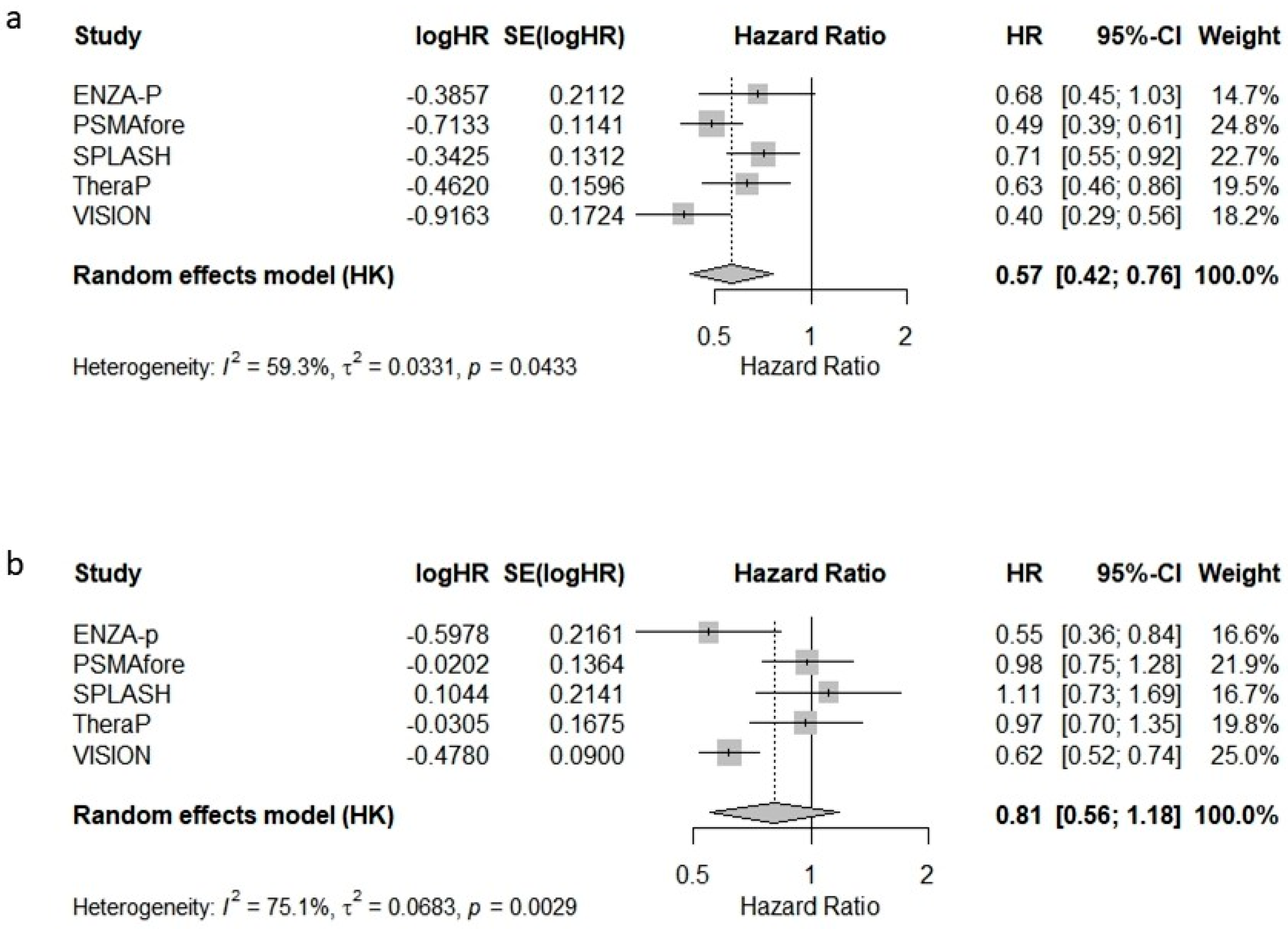
3.1. Meta-Analysis of Hazard Ratios for rPFS and OS
3.2. Radiological Progression-Free Survival (rPFS)
3.3. Overall Survival (OS)
3.4. Overall Survival Subgroup Analysis
3.4.1. Control Group
3.4.2. Lu-PSMA vs. ARTA
3.4.3. Lu-PSMA + SOC vs. SOC Alone
3.4.4. Lu-PSMA as a Monotherapy and [177Lu]Lu-PSMA Combined with Standard of Care (SOC)
3.4.5. Publication Bias
4. Cost-Effectiveness Analysis
5. Discussion
6. Limitations and Future Directions
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yu, E.-M.; Patel, I.; Hwang, M.W.; Polani, F.; Aragon-Ching, J.B. The Rapidly Evolving Treatment Landscape of Metastatic Hormone-Sensitive Prostate Cancer. Clin. Med. Insights Oncol. 2024, 18, 11795549241277180. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 15. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Fizazi, K.; Matsubara, N.; Alekseev, B.Y.; Feyerabend, S.; Kheoh, T.; Chi, K.N. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.-H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-Deprivation Therapy Alone or with Docetaxel in Non-Castrate Metastatic Prostate Cancer (GETUG-AFU 15): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Napoli, G.; Arcangeli, S.; Fionda, B.; Munoz, F.; Tebano, U.; Durante, E.; Tucci, M.; Bortolus, R.; Muraro, M.; Rinaldi, G.; et al. A Systematic Review and a Meta-Analysis of Randomized Controlled Trials’ Control Groups in Metastatic Hormone-Sensitive Prostate Cancer (MHSPC). Curr. Oncol. Rep. 2022, 24, 1633–1644. [Google Scholar] [CrossRef]
- Fiorica, F.; Buttigliero, C.; Grigolato, D.; Muraro, M.; Turco, F.; Munoz, F.; Tucci, M. Addition of New Androgen Receptor Pathway Inhibitors to Docetaxel and Androgen Deprivation Therapy in Metastatic Hormone-Sensitive Prostate Cancer: A Systematic Review and Metanalysis. Curr. Oncol. 2022, 29, 9511–9524. [Google Scholar] [CrossRef]
- Das, T.; Guleria, M.; Parab, A.; Kale, C.; Shah, H.; Sarma, H.D.; Lele, V.R.; Banerjee, S. Clinical Translation of 177Lu-Labeled PSMA-617: Initial Experience in Prostate Cancer Patients. Nucl. Med. Biol. 2016, 43, 296–302. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus Cabazitaxel in Patients with Metastatic Castration-Resistant Prostate Cancer (TheraP): A Randomised, Open-Label, Phase 2 Trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Emmett, L.; Subramaniam, S.; Crumbaker, M.; Nguyen, A.; Joshua, A.M.; Weickhardt, A.; Lee, S.-T.; Ng, S.; Francis, R.J.; Goh, J.C.; et al. [177Lu]Lu-PSMA-617 plus Enzalutamide in Patients with Metastatic Castration-Resistant Prostate Cancer (ENZA-p): An Open-Label, Multicentre, Randomised, Phase 2 Trial. Lancet Oncol. 2024, 25, 563–571. [Google Scholar] [CrossRef]
- Morris, M.J.; Castellano, D.; Herrmann, K.; de Bono, J.S.; Shore, N.D.; Chi, K.N.; Crosby, M.; Piulats, J.M.; Fléchon, A.; Wei, X.X.; et al. 177Lu-PSMA-617 versus a Change of Androgen Receptor Pathway Inhibitor Therapy for Taxane-Naïve Patients with Progressive Metastatic Castration-Resistant Prostate Cancer (PSMAfore): A Phase 3, Randomised, Controlled Trial. Lancet 2024, 404, 1227–1239. [Google Scholar] [CrossRef]
- Sartor, O.; Jiang, D.M.; Smoragiewicz, M.; Zibelman, M.; Flechon, A.; El-Haddad, G.; Abikhzer, G.; Saad, F.; Tutrone, R.; Tagawa, S.T.; et al. LBA65 Efficacy of 177Lu-PNT2002 in PSMA-Positive MCRPC Following Progression on an Androgen-Receptor Pathway Inhibitor (ARPI) (SPLASH). Ann. Oncol. 2024, 35, S1254–S1255. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) Statement: Updated Reporting Guidance for Health Economic Evaluations. Value Health 2022, 25, 3–9. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Earle, C.C.; Pham, B.; Wells, G.A. An Assessment of Methods to Combine Published Survival Curves. Med. Decis. Mak. 2000, 20, 104–111. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.; Ouwens, M.J.; Welton, N.J. Enhanced Secondary Analysis of Survival Data: Reconstructing the Data from Published Kaplan-Meier Survival Curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Combescure, C.; Foucher, Y.; Jackson, D. Meta-Analysis of Single-Arm Survival Studies: A Distribution-Free Approach for Estimating Summary Survival Curves with Random Effects. Stat. Med. 2014, 33, 2521–2537. [Google Scholar] [CrossRef]
- Cabibbo, G.; Enea, M.; Attanasio, M.; Bruix, J.; Craxì, A.; Cammà, C. A Meta-Analysis of Survival Rates of Untreated Patients in Randomised Clinical Trials of Hepatocellular Carcinoma. Hepatology 2010, 51, 1274–1283. [Google Scholar] [CrossRef]
- Bang, H.; Zhao, H. Median-Based Incremental Cost-Effectiveness Ratios with Censored Data. J. Biopharm. Stat. 2016, 26, 552–564. [Google Scholar] [CrossRef]
- Latimer, N.R. Survival Analysis for Economic Evaluations alongside Clinical Trials--Extrapolation with Patient-Level Data: Inconsistencies, Limitations, and a Practical Guide. Med. Decis. Mak. 2013, 33, 743–754. [Google Scholar] [CrossRef]
- Guide to the Methods of Technology Appraisal 2013. 2013. Available online: https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781 (accessed on 23 April 2024).
- Neumann, P.J.; Cohen, J.T.; Weinstein, M.C. Updating Cost-Effectiveness—The Curious Resilience of the $50,000-per-QALY Threshold. N. Engl. J. Med. 2014, 371, 796–797. [Google Scholar] [CrossRef]
- Sartor, O.; Castellano Gauna, D.E.; Herrmann, K.; de Bono, J.S.; Shore, N.D.; Chi, K.N.N.; Crosby, M.; Piulats Rodriguez, J.M.; Flechon, A.; Wei, X.X.; et al. LBA13 Phase III Trial of [177Lu]Lu-PSMA-617 in Taxane-Naïve Patients with Metastatic Castration-Resistant Prostate Cancer (PSMAfore). Ann. Oncol. 2023, 34, S1324–S1325. [Google Scholar] [CrossRef]
- PSMA PET and RLT 2024: PSMA Radioligand Therapy: The VISION and TheraP Trials. Available online: https://www.urotoday.com/conference-highlights/psma-pet-rlt-2024/149213-psma-pet-and-rlt-2024-psma-radioligand-therapy-the-vision-and-therap-trials.html (accessed on 19 June 2025).
- Emmett, L.; Subramaniam, S.; Crumbaker, M.; Joshua, A.M.; Sandhu, S.; Nguyen, A.; Weickhardt, A.; Lee, S.-T.; Ng, S.; Francis, R.J.; et al. Overall Survival and Quality of Life with [177Lu]Lu-PSMA-617 plus Enzalutamide versus Enzalutamide Alone in Metastatic Castration-Resistant Prostate Cancer (ENZA-p): Secondary Outcomes from a Multicentre, Open-Label, Randomised, Phase 2 Trial. Lancet Oncol. 2025, 26, 291–299. [Google Scholar] [CrossRef]
- Ciccarese, C.; Bauckneht, M.; Zagaria, L.; Fornarini, G.; Beccia, V.; Lanfranchi, F.; Perotti, G.; Pinterpe, G.; Migliaccio, F.; Tortora, G.; et al. Defining the Position of [177Lu]Lu-PSMA Radioligand Therapy in the Treatment Landscape of Metastatic Castration-Resistant Prostate Cancer: A Meta-Analysis of Clinical Trials. Targ. Oncol. 2025, 20, 103–112. [Google Scholar] [CrossRef]
- Cherny, N.I.; Sullivan, R.; Dafni, U.; Kerst, J.M.; Sobrero, A.; Zielinski, C.; de Vries, E.G.E.; Piccart, M.J. A Standardised, Generic, Validated Approach to Stratify the Magnitude of Clinical Benefit That Can Be Anticipated from Anti-Cancer Therapies: The European Society for Medical Oncology Magnitude of Clinical Benefit Scale (ESMO-MCBS). Ann. Oncol. 2015, 26, 1547–1573. [Google Scholar] [CrossRef]
- Schnipper, L.E.; Davidson, N.E.; Wollins, D.S.; Blayney, D.W.; Dicker, A.P.; Ganz, P.A.; Hoverman, J.R.; Langdon, R.; Lyman, G.H.; Meropol, N.J.; et al. Updating the American Society of Clinical Oncology Value Framework: Revisions and Reflections in Response to Comments Received. J. Clin. Oncol. 2016, 34, 2925–2934. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorica, F.; Candela, M.V.; Sava, T.; Salgarello, M.; Giuliani, J.; Navdeep, S.; Franceschetto, A.; Grigolato, D.; Durante, E.; Palesandro, E.; et al. Is [177Lu]Lu-PSMA-617 Redefining Value in mCRPC Care? A Meta-Analysis of Clinical and Economic Endpoints. Cancers 2025, 17, 2247. https://doi.org/10.3390/cancers17132247
Fiorica F, Candela MV, Sava T, Salgarello M, Giuliani J, Navdeep S, Franceschetto A, Grigolato D, Durante E, Palesandro E, et al. Is [177Lu]Lu-PSMA-617 Redefining Value in mCRPC Care? A Meta-Analysis of Clinical and Economic Endpoints. Cancers. 2025; 17(13):2247. https://doi.org/10.3390/cancers17132247
Chicago/Turabian StyleFiorica, Francesco, Maria Viviana Candela, Teodoro Sava, Matteo Salgarello, Jacopo Giuliani, Singh Navdeep, Antonella Franceschetto, Daniela Grigolato, Emilia Durante, Erica Palesandro, and et al. 2025. "Is [177Lu]Lu-PSMA-617 Redefining Value in mCRPC Care? A Meta-Analysis of Clinical and Economic Endpoints" Cancers 17, no. 13: 2247. https://doi.org/10.3390/cancers17132247
APA StyleFiorica, F., Candela, M. V., Sava, T., Salgarello, M., Giuliani, J., Navdeep, S., Franceschetto, A., Grigolato, D., Durante, E., Palesandro, E., Giusto, E. A., Buttigliero, C., & Tucci, M. (2025). Is [177Lu]Lu-PSMA-617 Redefining Value in mCRPC Care? A Meta-Analysis of Clinical and Economic Endpoints. Cancers, 17(13), 2247. https://doi.org/10.3390/cancers17132247