
Narrative Review: Predictive Biomarkers of Tumor Response to Neoadjuvant Radiotherapy or Total Neoadjuvant Therapy of Locally Advanced Rectal Cancer Patients

 , , , , and
, , , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
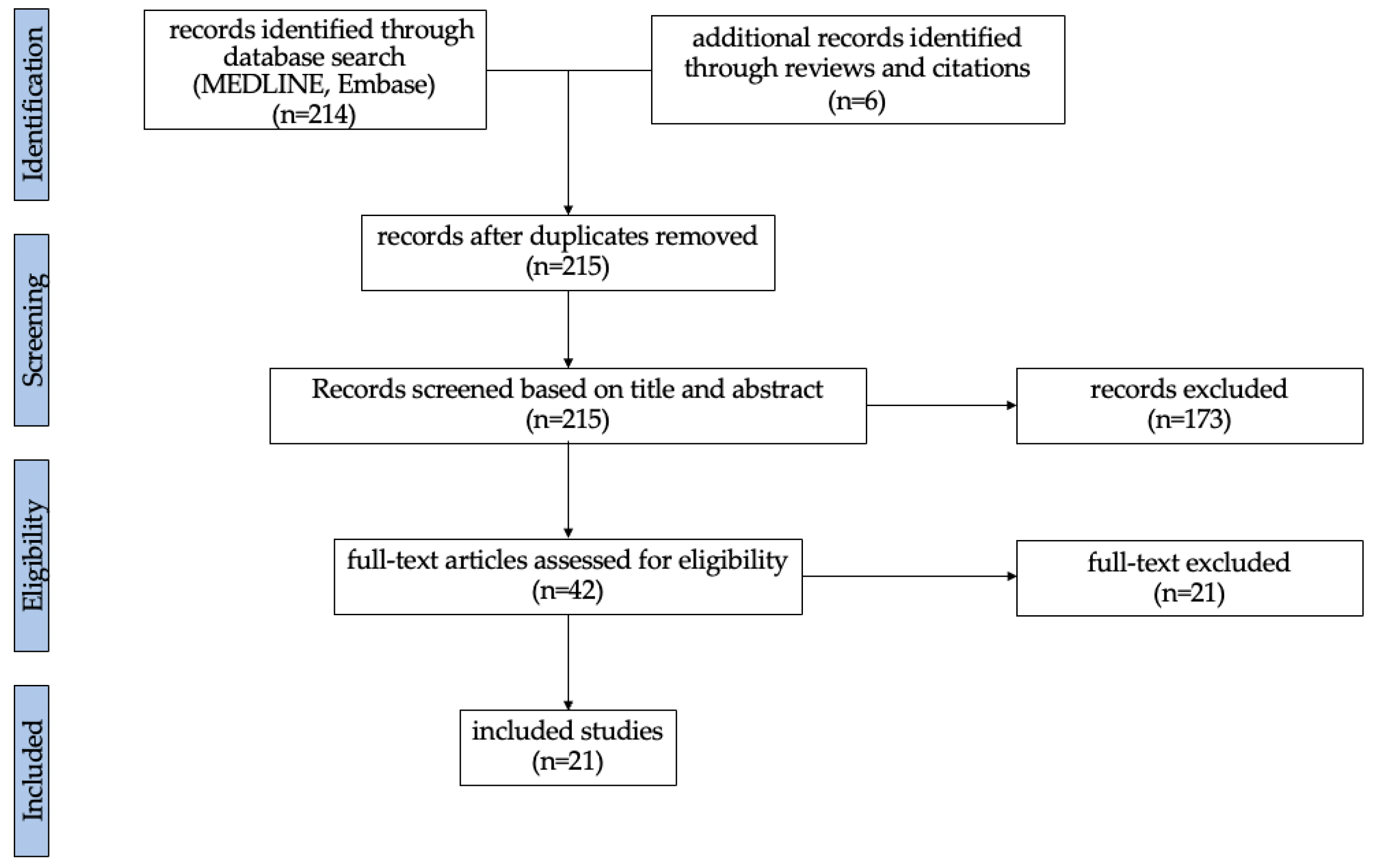
3.1. Literature Searches
3.2. Circulating Markers
3.2.1. CEA
3.2.2. Liquid Biopsy
3.2.3. Flow Cytometry
3.3. Tissue Markers
3.3.1. Immunohistochemistry
3.3.2. Genomic Markers
3.4. Radiomic Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 5-FU | 5-Fluorouracil |
| APAF-1 | Apoptotic protease activating factor-1 |
| BrdUrdLI | Bromodeoxyuridine labeling index |
| CAPOX | Capecitabin and oxaliplatin |
| CBFM | Conventional biexponential fitting |
| cCR | Clinical complete response |
| CD | Cluster of differentiation |
| CEA | Carcinoembryonic antigen |
| cfDNA | Circulating free DNA |
| CRT | Chemoradiotherapy |
| CTC | Circulating tumor cells |
| ctDNA | Circulating tumor DNA |
| DCC | Deleted in colon cancer |
| Dp | Pseudo diffusion |
| dUMP | Deoxyuridine monophosphate |
| DFS | Disease-free survival |
| dTMP | Deoxythymidine monophosphate |
| EGFR | Epidermal growth factor receptor |
| ESMO | European Society for Medical Oncology |
| FC | Flow cytometry |
| FFPE | Fixed paraffin embedded |
| FOLFOX | Folinic acid, fluorouracil and oxaliplatin |
| Glut-1 | Glucose transporter 1 |
| G-MDSC | Granulocytic-myeloid derived suppressor cells |
| HER-2 | Human epidermal growth factor receptor-2 |
| hPEBP4 | Human phosphatidylethanolamine-binding protein 4 |
| IHC | Immunohistochemistry |
| LARC | Locally advanced rectal cancer |
| LN | Lymph node |
| LRP1B | Low-density lipoprotein receptor-related protein 1b |
| mFOLFOX | Modified FOLFOX |
| MIB-1 LI | MIB-1 labeling index |
| M-MDSC | Monocytic-myeloid derived suppressor cells |
| MMR | Microsatellite mismatch repair system |
| MRN | MRE11/RAD50/NBS1 |
| MSI | Microsatellite instability |
| MSS | Microsatellite stable |
| N | Lymph node stage according to the TNM classification |
| NAT | Neoadjuvant treatment |
| NGS | Next-generation sequencing |
| NPV | Negative predictive value |
| OS | Overall survival |
| PCR | Polymerase chain reaction |
| pCR | Pathological complete response |
| PPV | Positive predictive value |
| RC | Rectal cancer |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| RT | Radiotherapy |
| SCRT | Short-course radiotherapy |
| SD | Standard deviation |
| SIS | Standardized index of shape |
| Sn | Sensitivity |
| Sp | Specificity |
| SPF | S-phase fraction |
| T | Tumor size according to the TNM classification |
| TILs | Tumor-infiltrating lymphocytes |
| TME | Tumor microenvironment |
| TNT | Total neoadjuvant treatment |
| Treg | Regulatory T cells |
| TRG | Tumor regression grade |
| TS | Thymidilate synthase |
| TTT | Treatment |
| VARPRO | Variable projection |
| VEGF | Vascular growth factor |
References
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rodel, C.; Cervantes, A.; Arnold, D.; Committee, E.G. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Minicozzi, P.; Innos, K.; Sanchez, M.J.; Trama, A.; Walsh, P.M.; Marcos-Gragera, R.; Dimitrova, N.; Botta, L.; Visser, O.; Rossi, S.; et al. Quality analysis of population-based information on cancer stage at diagnosis across Europe, with presentation of stage-specific cancer survival estimates: A EUROCARE-5 study. Eur. J. Cancer 2017, 84, 335–353. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef]
- Conroy, T.; Bosset, J.F.; Etienne, P.L.; Rio, E.; Francois, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouche, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Li, L.; Lee, K.C.; Lam, K.O.; Wong, K.H.; Ho, W.M.; Ma, B. Total Neoadjuvant Therapy for High Risk Rectal Cancer in Western and Asian Populations—Current Evidence and Clinical Applications. Clin. Color. Cancer 2022, 21, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Y.; Kardosh, A.; Nabavizadeh, N.; Lopez, C.D. Evolving Treatment Options and Future Directions for Locally Advanced Rectal Cancer. Clin. Color. Cancer 2019, 18, 231–237. [Google Scholar] [CrossRef]
- He, W.; Li, Q.; Li, X. Changing patterns of neoadjuvant therapy for locally advanced rectal cancer: A narrative review. Crit. Rev. Oncol. Hematol. 2023, 181, 103885. [Google Scholar] [CrossRef]
- Timmerman, C.; Taveras, L.R.; Huerta, S. Clinical and molecular diagnosis of pathologic complete response in rectal cancer: An update. Expert Rev. Mol. Diagn. 2018, 18, 887–896. [Google Scholar] [CrossRef]
- Gollins, S.; Sebag-Montefiore, D. Neoadjuvant Treatment Strategies for Locally Advanced Rectal Cancer. Clin. Oncol. (R Coll. Radiol.) 2016, 28, 146–151. [Google Scholar] [CrossRef]
- Bach, S.P. STAR-TREC: An International Three-arm Multicentre, Partially Randomised Controlled Trial Incorporating an External Pilot. Clin. Oncol. (R Coll. Radiol.) 2023, 35, e107–e109. [Google Scholar] [CrossRef]
- Smolskas, E.; Mikulskyte, G.; Sileika, E.; Suziedelis, K.; Dulskas, A. Tissue-Based Markers as a Tool to Assess Response to Neoadjuvant Radiotherapy in Rectal Cancer-Systematic Review. Int. J. Mol. Sci. 2022, 23, 6040. [Google Scholar] [CrossRef] [PubMed]
- Amintas, S.; Giraud, N.; Fernandez, B.; Dupin, C.; Denost, Q.; Garant, A.; Frulio, N.; Smith, D.; Rullier, A.; Rullier, E.; et al. The Crying Need for a Better Response Assessment in Rectal Cancer. Curr. Treat. Options Oncol. 2023, 24, 1507–1523. [Google Scholar] [CrossRef] [PubMed]
- Machado Carvalho, J.V.; Dutoit, V.; Corro, C.; Koessler, T. Promises and Challenges of Predictive Blood Biomarkers for Locally Advanced Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy. Cells 2023, 12, 413. [Google Scholar] [CrossRef]
- Slipsager, A.; Henrichsen, S.N.; Falkmer, U.G.; Dybkaer, K.; Belting, M.; Poulsen, L.O. Predictive biomarkers in radioresistant rectal cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2023, 186, 103991. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Sansone, M.; Granata, V.; Grimm, R.; Pace, U.; Delrio, P.; Tatangelo, F.; Botti, G.; Avallone, A.; Pecori, B.; et al. Diffusion and perfusion MR parameters to assess preoperative short-course radiotherapy response in locally advanced rectal cancer: A comparative explorative study among Standardized Index of Shape by DCE-MRI, intravoxel incoherent motion- and diffusion kurtosis imaging-derived parameters. Abdom. Radiol. 2019, 44, 3683–3700. [Google Scholar] [CrossRef]
- Gasinska, A.; Richter, P.; Darasz, Z.; Niemiec, J.; Bucki, K.; Malecki, K.; Sokolowski, A. Gender-related differences in repopulation and early tumor response to preoperative radiotherapy in rectal cancer patients. J. Gastrointest. Surg. 2011, 15, 1568–1576. [Google Scholar] [CrossRef]
- Gasinska, A.; Adamczyk, A.; Niemiec, J.; Biesaga, B.; Darasz, Z.; Skolyszewski, J. Gender-related differences in pathological and clinical tumor response based on immunohistochemical proteins expression in rectal cancer patients treated with short course of preoperative radiotherapy. J. Gastrointest. Surg. 2014, 18, 1306–1318. [Google Scholar] [CrossRef]
- Ho, V.; Chung, L.; Singh, A.; Lea, V.; Abubakar, A.; Lim, S.H.; Ng, W.; Lee, M.; de Souza, P.; Shin, J.S.; et al. Overexpression of the MRE11-RAD50-NBS1 (MRN) complex in rectal cancer correlates with poor response to neoadjuvant radiotherapy and prognosis. BMC Cancer 2018, 18, 869. [Google Scholar] [CrossRef]
- Truelsen, C.G.; Kronborg, C.S.; Sorensen, B.S.; Callesen, L.B.; Spindler, K.G. Circulating cell-free DNA as predictor of pathological complete response in locally advanced rectal cancer patients undergoing preoperative chemoradiotherapy. Clin. Transl. Radiat. Oncol. 2022, 36, 9–15. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, X.M.; Li, Z.; Liu, X.J.; Chai, J.; Zhang, G.Y.; Cheng, Y.F. Overexpression of nuclear beta-catenin in rectal adenocarcinoma is associated with radioresistance. World J. Gastroenterol. 2013, 19, 6876–6882. [Google Scholar] [CrossRef]
- Napolitano, M.; D’Alterio, C.; Cardone, E.; Trotta, A.M.; Pecori, B.; Rega, D.; Pace, U.; Scala, D.; Scognamiglio, G.; Tatangelo, F.; et al. Peripheral myeloid-derived suppressor and T regulatory PD-1 positive cells predict response to neoadjuvant short-course radiotherapy in rectal cancer patients. Oncotarget 2015, 6, 8261–8270. [Google Scholar] [CrossRef]
- Kandioler, D.; Zwrtek, R.; Ludwig, C.; Janschek, E.; Ploner, M.; Hofbauer, F.; Kuhrer, I.; Kappel, S.; Wrba, F.; Horvath, M.; et al. TP53 genotype but not p53 immunohistochemical result predicts response to preoperative short-term radiotherapy in rectal cancer. Ann. Surg. 2002, 235, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Negri, F.V.; Campanini, N.; Camisa, R.; Pucci, F.; Bui, S.; Ceccon, G.; Martinelli, R.; Fumagalli, M.; Losardo, P.L.; Crafa, P.; et al. Biological predictive factors in rectal cancer treated with preoperative radiotherapy or radiochemotherapy. Br. J. Cancer 2008, 98, 143–147. [Google Scholar] [CrossRef]
- Qiu, J.; Yang, G.; Shen, Z.; Xie, Y.; Wang, L. hPEBP4 as a predictive marker for the pathological response of rectal cancer to preoperative radiotherapy. Int. J. Color. Dis. 2013, 28, 241–246. [Google Scholar] [CrossRef]
- Rebischung, C.; Gerard, J.P.; Gayet, J.; Thomas, G.; Hamelin, R.; Laurent-Puig, P. Prognostic value of P53 mutations in rectal carcinoma. Int. J. Cancer 2002, 100, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Saw, R.P.; Morgan, M.; Koorey, D.; Painter, D.; Findlay, M.; Stevens, G.; Clarke, S.; Chapuis, P.; Solomon, M.J. p53, deleted in colorectal cancer gene, and thymidylate synthase as predictors of histopathologic response and survival in low, locally advanced rectal cancer treated with preoperative adjuvant therapy. Dis. Colon Rectum 2003, 46, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhong, X.G.; Peng, Y.F.; Li, Z.W.; Gu, J. Prognostic value of pretreatment level of carcinoembryonic antigen on tumour downstaging and early occurring metastasis in locally advanced rectal cancer following neoadjuvant radiotherapy (30 Gy in 10 fractions). Color. Dis. 2014, 16, 33–39. [Google Scholar] [CrossRef]
- Yao, Y.F.; Du, C.Z.; Chen, N.; Chen, P.; Gu, J. Expression of HER-2 in rectal cancers treated with preoperative radiotherapy: A potential biomarker predictive of metastasis. Dis. Colon Rectum 2014, 57, 602–607. [Google Scholar] [CrossRef]
- Zlobec, I.; Vuong, T.; Compton, C.C.; Lugli, A.; Michel, R.P.; Hayashi, S.; Jass, J.R. Combined analysis of VEGF and EGFR predicts complete tumour response in rectal cancer treated with preoperative radiotherapy. Br. J. Cancer 2008, 98, 450–456. [Google Scholar] [CrossRef]
- Chapman, B.C.; Lai, S.H.; Friedrich, T.; Lieu, C.H.; Moskalenko, M.; Olsen, J.R.; Herter, W.; Birnbaum, E.H.; McCarter, M.D.; Vogel, J.D. Rectal Cancer: Clinical and Molecular Predictors of a Complete Response to Total Neoadjuvant Therapy. Dis. Colon Rectum 2023, 66, 521–530. [Google Scholar] [CrossRef]
- Iseas, S.; Sendoya, J.M.; Robbio, J.; Coraglio, M.; Kujaruk, M.; Mikolaitis, V.; Rizzolo, M.; Cabanne, A.; Ruiz, G.; Salanova, R.; et al. Prognostic Impact of An Integrative Landscape of Clinical, Immune, and Molecular Features in Non-Metastatic Rectal Cancer. Front. Oncol. 2021, 11, 801880. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, F.; Chau, I.; Cunningham, D.; Peckitt, C.; Lampis, A.; Hahne, J.C.; Braconi, C.; Tabernero, J.; Glimelius, B.; Cervantes, A.; et al. Prognostic role of the LCS6 KRAS variant in locally advanced rectal cancer: Results of the EXPERT-C trial. Ann. Oncol. 2015, 26, 1936–1941. [Google Scholar] [CrossRef]
- Vidal, J.; Casadevall, D.; Bellosillo, B.; Pericay, C.; Garcia-Carbonero, R.; Losa, F.; Layos, L.; Alonso, V.; Capdevila, J.; Gallego, J.; et al. Clinical Impact of Presurgery Circulating Tumor DNA after Total Neoadjuvant Treatment in Locally Advanced Rectal Cancer: A Biomarker Study from the GEMCAD 1402 Trial. Clin. Cancer Res. 2021, 27, 2890–2898. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Tang, B.; Yu, M.; He, L.; Zheng, P.; Yan, C.; Li, J.; Peng, Q. Development and Validation of a Radiomics Model Based on Lymph-Node Regression Grading After Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, 821–833. [Google Scholar] [CrossRef]
- Li, Y.; Pan, C.; Gao, Y.; Zhang, L.; Ji, D.; Cui, X.; Zhang, X.; Cai, Y.; Zhang, Y.; Yao, Y.; et al. Total Neoadjuvant Therapy With PD-1 Blockade for High-Risk Proficient Mismatch Repair Rectal Cancer. JAMA Surg. 2024, 159, 529–537. [Google Scholar] [CrossRef]
- Hammarstrom, S. The carcinoembryonic antigen (CEA) family: Structures, suggested functions and expression in normal and malignant tissues. Semin. Cancer Biol. 1999, 9, 67–81. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabieres, C. Circulating tumour cells in cancer patients: Challenges and perspectives. Trends Mol. Med. 2010, 16, 398–406. [Google Scholar] [CrossRef]
- Reimers, N.; Pantel, K. Liquid biopsy: Novel technologies and clinical applications. Clin. Chem. Lab. Med. 2019, 57, 312–316. [Google Scholar] [CrossRef]
- Bronkhorst, A.J.; Wentzel, J.F.; Aucamp, J.; van Dyk, E.; du Plessis, L.; Pretorius, P.J. Characterization of the cell-free DNA released by cultured cancer cells. Biochim. Biophys. Acta 2016, 1863, 157–165. [Google Scholar] [CrossRef]
- Fleischhacker, M.; Schmidt, B. Circulating nucleic acids (CNAs) and cancer--a survey. Biochim. Biophys. Acta 2007, 1775, 181–232. [Google Scholar] [CrossRef]
- Volik, S.; Alcaide, M.; Morin, R.D.; Collins, C. Cell-free DNA (cfDNA): Clinical Significance and Utility in Cancer Shaped By Emerging Technologies. Mol. Cancer Res. 2016, 14, 898–908. [Google Scholar] [CrossRef]
- McKinnon, K.M. Flow Cytometry: An Overview. Curr. Protoc. Immunol. 2018, 120, 5.1.1–5.1.11. [Google Scholar] [CrossRef]
- Shi, S.R.; Key, M.E.; Kalra, K.L. Antigen retrieval in formalin-fixed, paraffin-embedded tissues: An enhancement method for immunohistochemical staining based on microwave oven heating of tissue sections. J. Histochem. Cytochem. 1991, 39, 741–748. [Google Scholar] [CrossRef]
- Kaloni, D.; Diepstraten, S.T.; Strasser, A.; Kelly, G.L. BCL-2 protein family: Attractive targets for cancer therapy. Apoptosis 2023, 28, 20–38. [Google Scholar] [CrossRef]
- Uribe, M.L.; Marrocco, I.; Yarden, Y. EGFR in Cancer: Signaling Mechanisms, Drugs, and Acquired Resistance. Cancers 2021, 13, 2748. [Google Scholar] [CrossRef]
- Wang, X.; Li, N.; Li, H.; Liu, B.; Qiu, J.; Chen, T.; Cao, X. Silencing of human phosphatidylethanolamine-binding protein 4 sensitizes breast cancer cells to tumor necrosis factor-alpha-induced apoptosis and cell growth arrest. Clin. Cancer Res. 2005, 11, 7545–7553. [Google Scholar] [CrossRef]
- Qiu, J.; Tao, Y.; Yang, G.; Xu, K.; Lin, A.L.; Li, L. Effect of a chemical inhibitor of human phosphatidylethanolamine-binding protein 4 on radiosensitivity of rectal cancer cells. World J. Surg. Oncol. 2016, 14, 221. [Google Scholar] [CrossRef]
- Menon, S.S.; Guruvayoorappan, C.; Sakthivel, K.M.; Rasmi, R.R. Ki-67 protein as a tumour proliferation marker. Clin. Chim. Acta 2019, 491, 39–45. [Google Scholar] [CrossRef]
- Pandey, A.; Shen, C.; Feng, S.; Enosi Tuipulotu, D.; Ngo, C.; Liu, C.; Kurera, M.; Mathur, A.; Venkataraman, S.; Zhang, J.; et al. Ku70 senses cytosolic DNA and assembles a tumor-suppressive signalosome. Sci. Adv. 2024, 10, eadh3409. [Google Scholar] [CrossRef]
- Sanchez-Canteli, M.; Juesas, L.; Garmendia, I.; Otero-Rosales, M.; Calvo, A.; Alvarez-Fernandez, M.; Astudillo, A.; Montuenga, L.M.; Garcia-Pedrero, J.M.; Rodrigo, J.P. Tumor-Intrinsic Nuclear beta-Catenin Associates with an Immune Ignorance Phenotype and a Poorer Prognosis in Head and Neck Squamous Cell Carcinomas. Int. J. Mol. Sci. 2022, 23, 11559. [Google Scholar] [CrossRef]
- Li, X.; Xiang, Y.; Li, F.; Yin, C.; Li, B.; Ke, X. WNT/beta-Catenin Signaling Pathway Regulating T Cell-Inflammation in the Tumor Microenvironment. Front. Immunol. 2019, 10, 2293. [Google Scholar] [CrossRef]
- Ghalehbandi, S.; Yuzugulen, J.; Pranjol, M.Z.I.; Pourgholami, M.H. The role of VEGF in cancer-induced angiogenesis and research progress of drugs targeting VEGF. Eur. J. Pharmacol. 2023, 949, 175586. [Google Scholar] [CrossRef]
- Zhang, S.; Xiao, X.; Yi, Y.; Wang, X.; Zhu, L.; Shen, Y.; Lin, D.; Wu, C. Tumor initiation and early tumorigenesis: Molecular mechanisms and interventional targets. Signal Transduct. Target. Ther. 2024, 9, 149. [Google Scholar] [CrossRef]
- Behjati, S.; Tarpey, P.S. What is next generation sequencing? Arch. Dis. Child. Educ. Pract. Ed. 2013, 98, 236–238. [Google Scholar] [CrossRef]
- Dienstmann, R.; Jang, I.S.; Bot, B.; Friend, S.; Guinney, J. Database of genomic biomarkers for cancer drugs and clinical targetability in solid tumors. Cancer Discov. 2015, 5, 118–123. [Google Scholar] [CrossRef]
- Hernandez Borrero, L.J.; El-Deiry, W.S. Tumor suppressor p53: Biology, signaling pathways, and therapeutic targeting. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188556. [Google Scholar] [CrossRef]
- Wan, R.; Feng, J.; Tang, L. Consequences of Mutations and Abnormal Expression of SMAD4 in Tumors and T Cells. Onco Targets Ther. 2021, 14, 2531–2540. [Google Scholar] [CrossRef]
- Huang, L.; Guo, Z.; Wang, F.; Fu, L. KRAS mutation: From undruggable to druggable in cancer. Signal Transduct. Target. Ther. 2021, 6, 386. [Google Scholar] [CrossRef]
- Dewdney, A.; Cunningham, D.; Tabernero, J.; Capdevila, J.; Glimelius, B.; Cervantes, A.; Tait, D.; Brown, G.; Wotherspoon, A.; Gonzalez de Castro, D.; et al. Multicenter randomized phase II clinical trial comparing neoadjuvant oxaliplatin, capecitabine, and preoperative radiotherapy with or without cetuximab followed by total mesorectal excision in patients with high-risk rectal cancer (EXPERT-C). J. Clin. Oncol. 2012, 30, 1620–1627. [Google Scholar] [CrossRef]
- Sha, D.; Lee, A.M.; Shi, Q.; Alberts, S.R.; Sargent, D.J.; Sinicrope, F.A.; Diasio, R.B. Association study of the let-7 miRNA-complementary site variant in the 3′ untranslated region of the KRAS gene in stage III colon cancer (NCCTG N0147 Clinical Trial). Clin. Cancer Res. 2014, 20, 3319–3327. [Google Scholar] [CrossRef]
- Principe, C.; Dionisio de Sousa, I.J.; Prazeres, H.; Soares, P.; Lima, R.T. LRP1B: A Giant Lost in Cancer Translation. Pharmaceuticals 2021, 14, 836. [Google Scholar] [CrossRef]
- Wang, J.H.; Wahid, K.A.; van Dijk, L.V.; Farahani, K.; Thompson, R.F.; Fuller, C.D. Radiomic biomarkers of tumor immune biology and immunotherapy response. Clin. Transl. Radiat. Oncol. 2021, 28, 97–115. [Google Scholar] [CrossRef]
- Shur, J.D.; Doran, S.J.; Kumar, S.; Ap Dafydd, D.; Downey, K.; O’Connor, J.P.B.; Papanikolaou, N.; Messiou, C.; Koh, D.M.; Orton, M.R. Radiomics in Oncology: A Practical Guide. Radiographics 2021, 41, 1717–1732. [Google Scholar] [CrossRef]
- Bourbonne, V.; Schick, U.; Pradier, O.; Visvikis, D.; Metges, J.P.; Badic, B. Radiomics Approaches for the Prediction of Pathological Complete Response after Neoadjuvant Treatment in Locally Advanced Rectal Cancer: Ready for Prime Time? Cancers 2023, 15, 432. [Google Scholar] [CrossRef]
- Ohue, Y.; Nishikawa, H. Regulatory T (Treg) cells in cancer: Can Treg cells be a new therapeutic target? Cancer Sci. 2019, 110, 2080–2089. [Google Scholar] [CrossRef]
- Wu, B.; Zhang, B.; Li, B.; Wu, H.; Jiang, M. Cold and hot tumors: From molecular mechanisms to targeted therapy. Signal Transduct. Target. Ther. 2024, 9, 274. [Google Scholar] [CrossRef]
- Tie, Y.; Tang, F.; Wei, Y.Q.; Wei, X.W. Immunosuppressive cells in cancer: Mechanisms and potential therapeutic targets. J. Hematol. Oncol. 2022, 15, 61. [Google Scholar] [CrossRef]
- Su, W.; Ling, Y.; Yang, X.; Wu, Y.; Xing, C. Tumor microenvironment remodeling after neoadjuvant chemoradiotherapy in local advanced rectal cancer revealed by single-cell RNA sequencing. J. Transl. Med. 2024, 22, 1037. [Google Scholar] [CrossRef]
- Dias Costa, A.; Vayrynen, S.A.; Chawla, A.; Zhang, J.; Vayrynen, J.P.; Lau, M.C.; Williams, H.L.; Yuan, C.; Morales-Oyarvide, V.; Elganainy, D.; et al. Neoadjuvant Chemotherapy Is Associated with Altered Immune Cell Infiltration and an Anti-Tumorigenic Microenvironment in Resected Pancreatic Cancer. Clin. Cancer Res. 2022, 28, 5167–5179. [Google Scholar] [CrossRef]
- Feng, X.; Meng, X.; Tang, D.; Guo, S.; Liao, Q.; Chen, J.; Xie, Q.; Liu, F.; Fang, Y.; Sun, C.; et al. Reversal of the immunosuppressive tumor microenvironment via platinum-based neoadjuvant chemotherapy in cervical cancer. Cancer Pathog. Ther. 2024, 2, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Wu, M.L.; Huang, K.C.; Huang, I.P.; Chung, Y.L. The Effects of Neoadjuvant Treatment on the Tumor Microenvironment in Rectal Cancer: Implications for Immune Activation and Therapy Response. Clin. Color. Cancer 2020, 19, e164–e180. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; El Dika, I.H.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N. Engl. J. Med. 2022, 386, 2363–2376. [Google Scholar] [CrossRef]
- Orhan, A.; Khesrawi, F.; Tvilling Madsen, M.; Peuliche Vogelsang, R.; Dohrn, N.; Kanstrup Fiehn, A.M.; Gogenur, I. Tumor-Infiltrating Lymphocytes as Biomarkers of Treatment Response and Long-Term Survival in Patients with Rectal Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 636. [Google Scholar] [CrossRef]
- Piringer, G. ASCO highlights: Neoadjuvant immunotherapy in mismatch repair deficient colorectal cancer. Mag. Eur. Med. Oncol. 2025, 18, 26–29. [Google Scholar] [CrossRef]
- Cercek, A.; Dos Santos Fernandes, G.; Roxburgh, C.S.; Ganesh, K.; Ng, S.; Sanchez-Vega, F.; Yaeger, R.; Segal, N.H.; Reidy-Lagunes, D.L.; Varghese, A.M.; et al. Mismatch Repair-Deficient Rectal Cancer and Resistance to Neoadjuvant Chemotherapy. Clin. Cancer Res. 2020, 26, 3271–3279. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- El Sissy, C.; Kirilovsky, A.; Van den Eynde, M.; Musina, A.M.; Anitei, M.G.; Romero, A.; Marliot, F.; Junca, A.; Doyen, J.; Mlecnik, B.; et al. A Diagnostic Biopsy-Adapted Immunoscore Predicts Response to Neoadjuvant Treatment and Selects Patients with Rectal Cancer Eligible for a Watch-and-Wait Strategy. Clin. Cancer Res. 2020, 26, 5198–5207. [Google Scholar] [CrossRef]
- Mowery, Y.M.; Salama, J.K.; Zafar, S.Y.; Moore, H.G.; Willett, C.G.; Czito, B.G.; Hopkins, M.B.; Palta, M. Neoadjuvant long-course chemoradiation remains strongly favored over short-course radiotherapy by radiation oncologists in the United States. Cancer 2017, 123, 1434–1441. [Google Scholar] [CrossRef]
- Krook, J.E.; Moertel, C.G.; Gunderson, L.L.; Wieand, H.S.; Collins, R.T.; Beart, R.W.; Kubista, T.P.; Poon, M.A.; Meyers, W.C.; Mailliard, J.A.; et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N. Engl. J. Med. 1991, 324, 709–715. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Authors | Study Year | Number of Patients | Treatment Type | Drugs and Radiation Dosage | Time to Surgery | Sampling Time | Technic | Measured Biomarker | Tumor Response Endpoint |
|---|---|---|---|---|---|---|---|---|---|
| Chapman et al. (2023) [31] | 2016–2020 | 102 | TNT (I + CRT) | FOLFOX or CAPOX + CRT (5-FU and 25–28 radiation fractions) | n/a | pre-treatment | Blood sample NGS | CEA MMR status 8 genes panel | cCR pCR |
| Fusco et al. (2019) [16] | 2011–2016 | 34 | SCRT | 25 Gy in 5 fractions | 4–6 weeks | pre-treatment post-treatment | Radiomic MRI | SIS IVIM DKI-derived parameters | TRG (Mandard) |
| Gasinska et al. (2011) [17] | 2003–2006 | 122 | SCRT | 25 Gy in 5 fractions | 1 or 4 weeks | pre-treatment post-treatment | FC | MIB-1 LI BrdUrd LI/SPF | CR (RECIST) |
| Gasinska et al. (2014) [18] | 2003–2006 | 111 | SCRT | 25 Gy in 5 fractions | 3–53 days | Pre-treatment | IHC | CD34/P53/BCL2/ Ku70/Ki-67/GLUT-1 | CTR (RECIST) TRG (Dworak) |
| Ho et al. (2018) [19] | 2000–2011 | 55 | SCRT | 25 Gy in 5 fractions | n/a | post-treatment | IHC | RAD50/MRE11/NBS1 complex MMR status | TRG (AJCC, 7th edition) |
| Iseas et al. (2021) [32] | 2015–2018 | 36 | TNT (I + CRT) | CAPOX + CRT (Capecitabin + 50.4 Gy in 28 fractions) | 12–16 weeks | pre-treatment | IHC targeted DNA sequencing | MMR status TILs (CD3-CD8+)/HER2 PD-L1 72 genes panel | mrTRG TRG (CAP) |
| Kandioler et al. (2002) [23] | 1994–1998 | 64 | RT | 25 Gy in 10 fractions | n/a | pre-treatment post-treatment | IHC targeted PCR | P53 | T stage downstaging |
| Li et al. (2024) [36] | 2020–2021 | 25 | TNT (I + CRT + C) | CAPOX and camrelizmab + CRT +/− CAPOX | n/a | pre-treatment | NGS Liquid biopsy | ctDNA | pCR |
| Napolitano et al. (2015) [22] | n/a | 13 | SCRT | 25 Gy in 5 fractions | 8 weeks | pre-treatment post-treatment | FC IHC | G-MDSC M-MDSC Treg | TRG (Ryan) |
| Negri et al. (2008) [24] | n/a | 38 | RT | 40 Gy in 16 fractions | 6 weeks | pre-treatment | IHC | MMR status P53/p21/TS/VEGF | pCR |
| Qiu et al. (2013) [25] | 2005–2010 | 86 | RT | 20 Gy in 5 fractions | 4–5 weeks | pre-treatment post-treatment | IHC | hPEBP4 | TRG (Dworak) |
| Rebischung et al. (2002) [26] | 1989–1991 | 86 | RT | 39 Gy in 13 fractions | n/a | pre-treatment | Targeted DNA sequencing | p53 | T downstaging |
| Saw et al. (2003) [27] | 1991–1998 | 25 | RT | 50.4 Gy in 28 fractions | 4–6 weeks | pre-treatment | IHC targeted PCR genotyping | p53/DCC/TS | TRG (Mandard) |
| Sclafani et al. (2015) [33] | 2005–2008 | 155 | TNT (Expert-C) (I + CRT) | Arm1 CAPOX + CRT (Capecitabin + 45 Gy in 25 fractions) Arm2 CAPOX +CRT +Cetuximab | 4–6 weeks | pre-treatment | PCR genotyping | LCS6 | pCR |
| Truelsen et al. (2022) [20] | 2017–2020 | 12 | SCRT | 25 Gy in 5 fractions | 6–8 weeks | pre-treatment during-treatment post-treatment | Blood sample Liquid Biopsy | cfDNA | TRG (Mandard) |
| Vidal et al. (2021) [34] | 2015–2017 | 72 | TNT (I + CRT) | Arm1 Aflibercept + mFOLOFX6 + CRT Arm2 mFOLFOX6 + CRT | n/a | pre-treatment post-treatment | Blood sample Liquid Biopsy | ctDNA | pCR |
| Wang et al. (2013) [21] | 2008–2011 | 136 | SCRT | 25 Gy in 5 fractions | 10–14 days | pre-treatment post-treatment | IHC | nuclear β-catenin | TRG (Dworak) |
| Wang et al. (2014) [28] | 2003–2009 | 240 | RT | 30 Gy in 10 fractions | 2–4 weeks | pre-treatment | Blood sample | CEA | T and N downstaging |
| Yao et al. (2014) [29] | 2002–2005 | 142 | RT | 30 Gy in 10 fractions | 14 days | pre-treatment | IHC Blood sample | HER2 | TRG (AJCC, 7th edition) |
| Zhang et al. (2023) [35] | 2019–2021 | 78 | TNT (CRT + C) | CRT + mFOLFOX6 CRT + CapOx | 8–10 weeks | post-treatment | Radiomic (MRI) | LN characteristics | LRG |
| Zlobec et al. (2008) [30] | n/a | 104 | RT | 26 Gy in 4 fractions | 6–8 weeks | pre-treatment | IHC | EGFR/VEGF/p53/ BCL-2/APAF-1 | pCR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado Carvalho, J.V.; Meyer, J.; Ris, F.; Durham, A.; Bornand, A.; Ricoeur, A.; Corrò, C.; Koessler, T. Narrative Review: Predictive Biomarkers of Tumor Response to Neoadjuvant Radiotherapy or Total Neoadjuvant Therapy of Locally Advanced Rectal Cancer Patients. Cancers 2025, 17, 2229. https://doi.org/10.3390/cancers17132229
Machado Carvalho JV, Meyer J, Ris F, Durham A, Bornand A, Ricoeur A, Corrò C, Koessler T. Narrative Review: Predictive Biomarkers of Tumor Response to Neoadjuvant Radiotherapy or Total Neoadjuvant Therapy of Locally Advanced Rectal Cancer Patients. Cancers. 2025; 17(13):2229. https://doi.org/10.3390/cancers17132229
Chicago/Turabian StyleMachado Carvalho, Joao Victor, Jeremy Meyer, Frederic Ris, André Durham, Aurélie Bornand, Alexis Ricoeur, Claudia Corrò, and Thibaud Koessler. 2025. "Narrative Review: Predictive Biomarkers of Tumor Response to Neoadjuvant Radiotherapy or Total Neoadjuvant Therapy of Locally Advanced Rectal Cancer Patients" Cancers 17, no. 13: 2229. https://doi.org/10.3390/cancers17132229
APA StyleMachado Carvalho, J. V., Meyer, J., Ris, F., Durham, A., Bornand, A., Ricoeur, A., Corrò, C., & Koessler, T. (2025). Narrative Review: Predictive Biomarkers of Tumor Response to Neoadjuvant Radiotherapy or Total Neoadjuvant Therapy of Locally Advanced Rectal Cancer Patients. Cancers, 17(13), 2229. https://doi.org/10.3390/cancers17132229