
Real-World Data on Immune-Checkpoint Inhibitors in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Study

 , , and
, , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Objetcives
2.3. Statistical Analysis
2.4. Review
3. Results
3.1. Patient Characteristics
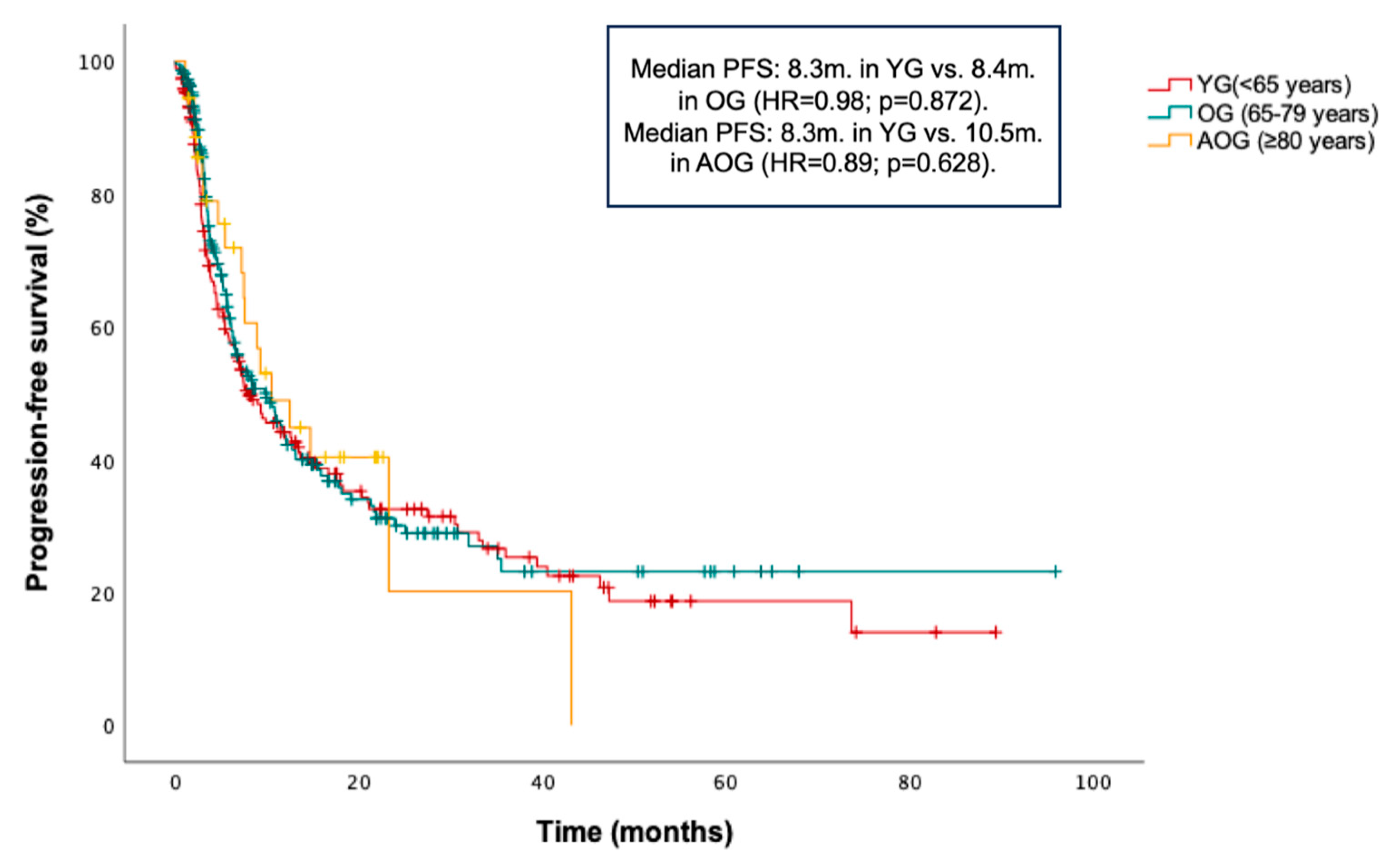
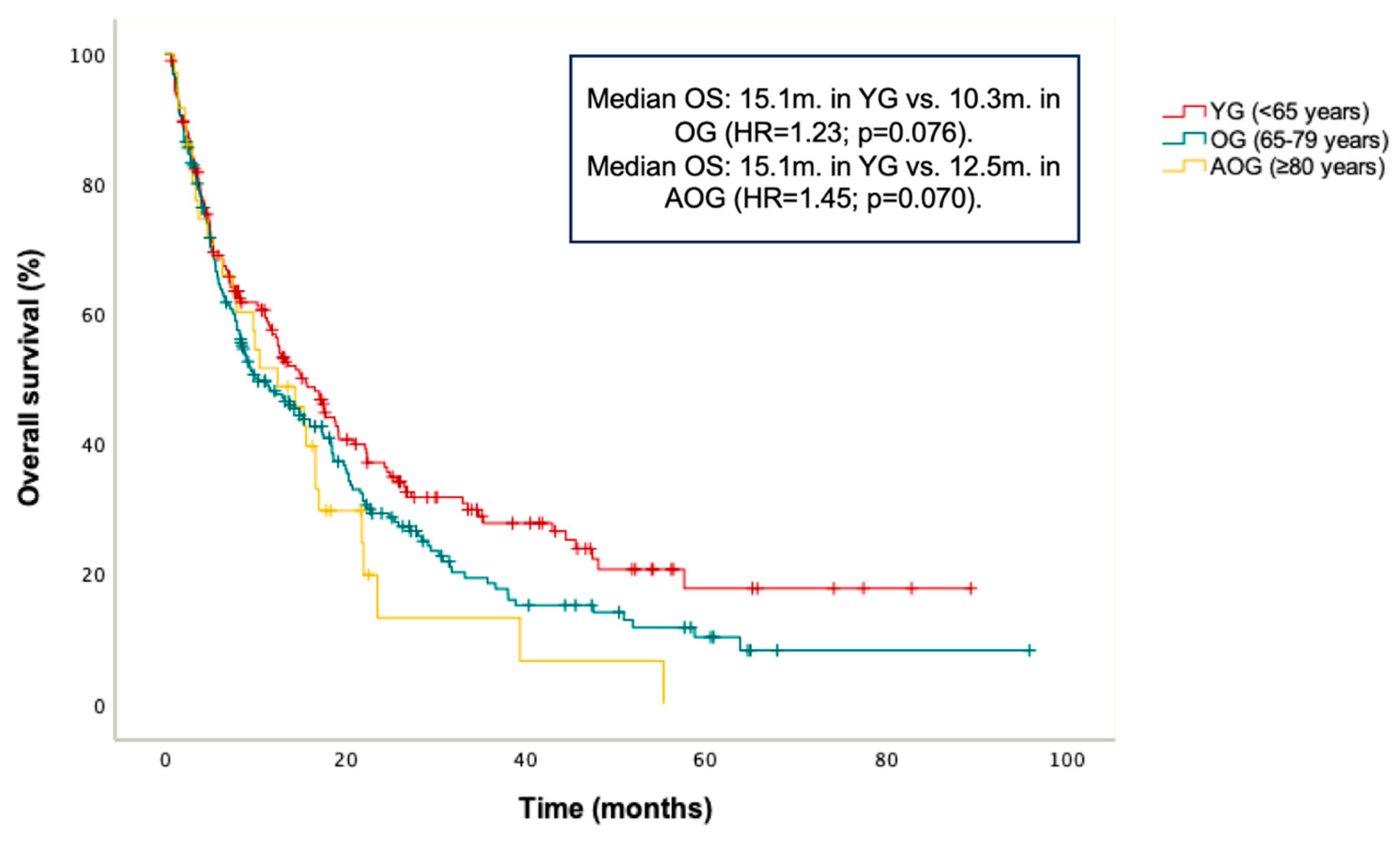
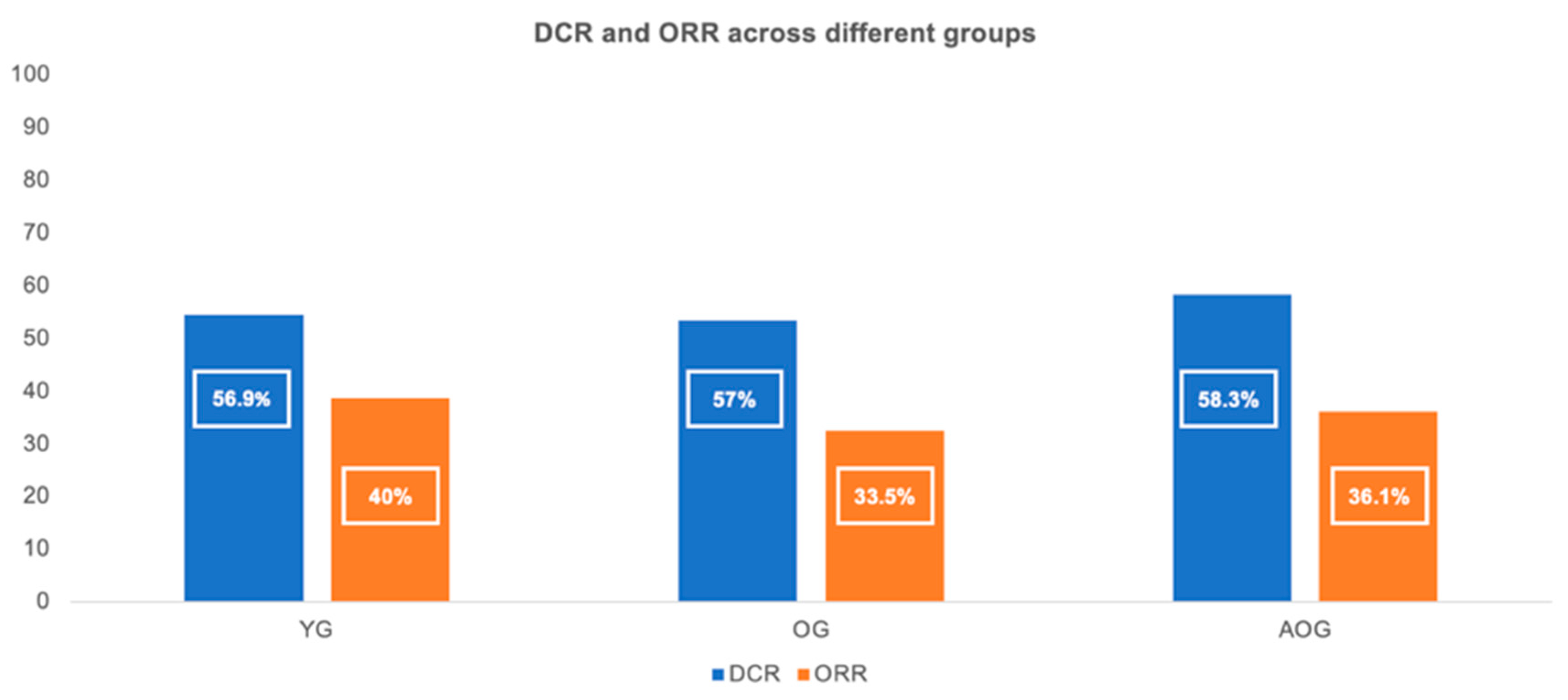
3.2. Outcomes
3.3. Safety
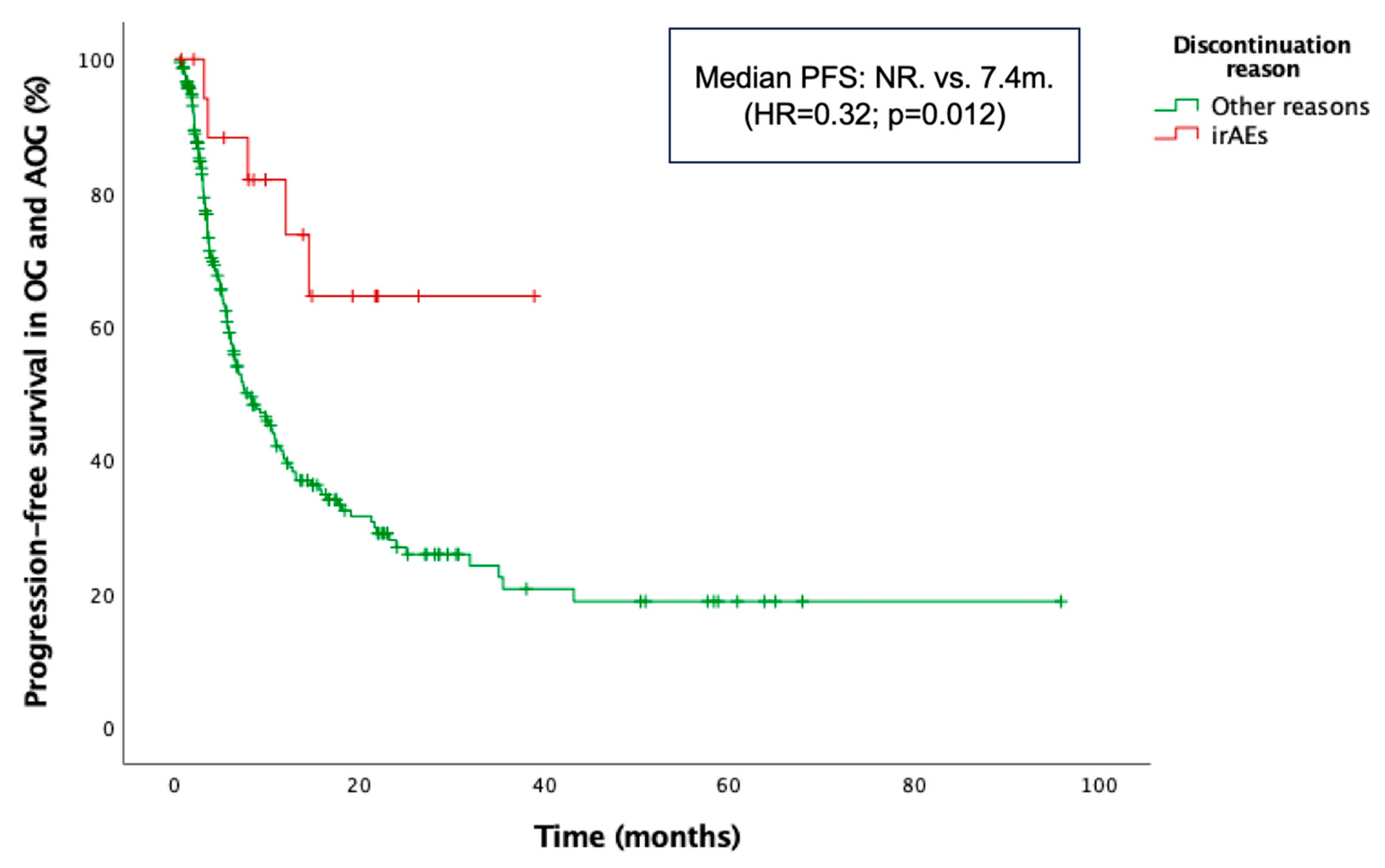
3.4. Prognostic Factors in the OG and AOG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| NSCLC | Non-small cell lung cancer |
| ICIs | Immune-checkpoint inhibitors |
| YG | Younger group |
| OG | Older group |
| AOG | Advanced older group |
| PFS | Progression-free survival |
| OS | Overall survival |
| irAEs | Immune-related adverse events |
| PD-1 | Programmed cell death protein 1 |
| ECOG | Eastern Cooperative Oncology Group |
| ORR | Overall response rate |
| DCR | Disease control rate |
| CR | Complete response |
| PR | Partial response |
| SD | Stable disease |
| PD | Progression disease |
| CTCAE | Common Terminology Criteria for Adverse Events |
| MTD | Median treatment duration |
| NR | Not reached |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Giroux Leprieur, E.; Dumenil, C.; Julie, C.; Giraud, V.; Dumoulin, J.; Labrune, S.; Chinet, T. Immunotherapy revolutionises non-small-cell lung cancer therapy: Results, perspectives and new challenges. Eur. J. Cancer 2017, 78, 16–23. [Google Scholar] [CrossRef]
- National Cancer Institute. Lung and bronchus cancer—Cancer stat facts. Bethesda (MD): National Cancer Institute. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 26 May 2025).
- Maione, P.; Perrone, F.; Gallo, C.; Manzione, L.; Piantedosi, F.; Barbera, S.; Cigolari, S.; Rosetti, F.; Piazza, E.; Robbiati, S.F.; et al. Pre-treatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: A prognostic analysis of the multicenter Italian lung cancer in the elderly study. J. Clin. Oncol. 2005, 23, 6865–6872. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, I.; Nokihara, H.; Nomura, S.; Niho, S.; Sugawara, S.; Horinouchi, H.; Azuma, K.; Yoneshima, Y.; Murakami, H.; Hosomi, Y.; et al. Comparison of carboplatin plus pemetrexed followed by maintenance pemetrexed with docetaxel monotherapy in elderly patients with advanced nonsquamous non-small cell lung cancer: A phase 3 randomized clinical trial. JAMA Oncol. 2020, 6, e196828. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Gogishvili, M.; Melkadze, T.; Makharadze, T.; Giorgadze, D.; Dvorkin, M.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: A randomized, controlled, double-blind phase 3 trial. Nat. Med. 2022, 28, 2374–2380. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.L.; Cho, B.C.; Luft, A.; Alatorre-Alexander, J.; Geater, S.L.; Laktionov, K.; Kim, S.W.; Ursol, G.; Hussein, M.; Lim, F.L.; et al. Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: The phase III POSEIDON study. J. Clin. Oncol. 2023, 41, 1213–1227. [Google Scholar] [CrossRef]
- Morinaga, D.; Asahina, H.; Ito, S.; Honjo, O.; Tanaka, H.; Honda, R.; Yokouchi, H.; Nakamura, K.; Takamura, K.; Hommura, F.; et al. Real-world data on the efficacy and safety of immune-checkpoint inhibitors in elderly patients with non-small cell lung cancer. Cancer Med. 2023, 12, 11525–11541. [Google Scholar] [CrossRef] [PubMed]
- Nosaki, K.; Saka, H.; Hosomi, Y.; Baas, P.; de Castro, G., Jr.; Reck, M.; Wu, Y.L.; Brahmer, J.R.; Felip, E.; Sawada, T.; et al. Safety and efficacy of pembrolizumab monotherapy in elderly patients with PD-L1-positive advanced non-small-cell lung cancer: Pooled analysis from the KEYNOTE-010, KEYNOTE-024, and KEYNOTE-042 studies. Lung Cancer 2019, 135, 188–195. [Google Scholar] [CrossRef]
- Lichtenstein, M.R.L.; Nipp, R.D.; Muzikansky, A.; Goodwin, K.; Anderson, D.; Newcomb, R.A.; Gainor, J.F. Impact of age on outcomes with immunotherapy in patients with non-small cell lung cancer. J. Thorac. Oncol. 2019, 14, 547–552. [Google Scholar] [CrossRef]
- McLean, A.J.; Le Couteur, D.G. Aging biology and geriatric clinical pharmacology. Pharmacol. Rev. 2004, 56, 163–184. [Google Scholar] [CrossRef]
- Lian, J.; Yue, Y.; Yu, W.; Zhang, Y. Immunosenescence: A key player in cancer development. J. Hematol. Oncol. 2020, 13, 151. [Google Scholar] [CrossRef]
- Pawelec, G. Age and immunity: What is “immunosenescence”? Exp. Gerontol. 2018, 105, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Marosi, C.; Köller, M. Challenge of cancer in the elderly. ESMO Open 2016, 1, e000020. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Wildes, T.; Blair, S.L.; Browner, I.S.; Cohen, H.J.; Deshazo, M.; Dotan, E.; Edil, B.H.; Extermann, M.; Ganti, A.K.P.; et al. Senior adult oncology, version 2.2014: Clinical practice guidelines in oncology. J. Natl. Compr. Canc Netw. 2014, 12, 82–125. [Google Scholar] [CrossRef] [PubMed]
- Stauder, R.; Eichhorst, B.; Hamaker, M.E.; Kaplanov, K.; Morrison, V.A.; Österborg, A.; Poddubnaya, I.; Woyach, J.A.; Shanafelt, T.; Smolej, L.; et al. Management of Chronic Lymphocytic Leukemia (CLL) in the Elderly: A Position Paper from an International Society of Geriatric Oncology (SIOG) Task Force. Ann. Oncol. 2016, 27, 761–769. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Moschos, S.J. Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2016, 45, 30–37. [Google Scholar] [CrossRef]
- Lee, S.M.; Schulz, C.; Prabhash, K.; Kowalski, D.; Szczesna, A.; Han, B.; Rittmeyer, A.; Talbot, T.; Vicente, D.; Califano, R.; et al. First-line atezolizumab monotherapy versus single-agent chemotherapy in patients with non-small-cell lung cancer ineligible for treatment with a platinum-containing regimen (IPSOS): A phase 3, global, multicentre, open-label, randomised controlled study. Lancet 2023, 402, 451–463. [Google Scholar] [CrossRef]
- Felip, E.; Ardizzoni, A.; Ciuleanu, T.; Cobo, M.; Laktionov, K.; Szilasi, M.; Califano, R.; Carcereny, E.; Griffiths, R.; Paz-Ares, L.; et al. CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations. Eur. J. Cancer 2020, 127, 160–172. [Google Scholar] [CrossRef]
- Spigel, D.R.; McCleod, M.; Jotte, R.M.; Einhorn, L.; Horn, L.; Waterhouse, D.M.; Creelan, B.; Babu, S.; Leighl, N.B.; Chandler, J.C.; et al. Safety, efficacy, and patient-reported health-related quality of life and symptom burden with nivolumab in patients with advanced non-small cell lung cancer, including patients aged 70 years or older or with poor performance status (CheckMate 153). J. Thorac. Oncol. 2019, 14, 1628–1639. [Google Scholar] [CrossRef]
- Grossi, F.; Crinò, L.; Logroscino, A.; Canova, S.; Delmonte, A.; Melotti, B.; Proto, C.; Gelibter, A.; Cappuzzo, F.; Turci, D.; et al. Use of nivolumab in elderly patients with advanced squamous non-small-cell lung cancer: Results from the Italian cohort of an expanded access programme. Eur. J. Cancer 2018, 100, 126–134. [Google Scholar] [CrossRef]
- Galli, G.; De Toma, A.; Pagani, F.; Randon, G.; Trevisan, B.; Prelaj, A.; Ferrara, R.; Proto, C.; Signorelli, D.; Ganzinelli, M.; et al. Efficacy and safety of immunotherapy in elderly patients with non-small cell lung cancer. Lung Cancer 2019, 137, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Imai, H.; Mouri, A.; Tsukamoto, K.; Masaki, K.; Hashimoto, K.; Miura, Y.; Shiono, A.; Yamaguchi, O.; Nakagawa, J.; et al. Efficacy and safety of first-line nivolumab plus ipilimumab treatment in elderly patients (aged ≥ 75 years) with non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2025, 151, 43. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Maggio, I.; Massucci, M.; Mollica, V.; Fragomeno, B.; Ardizzoni, A. ECOG performance status ≥2 as a prognostic factor in patients with advanced non-small cell lung cancer treated with immune checkpoint inhibitors—A systematic review and meta-analysis of real-world data. Lung Cancer 2020, 145, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Rocco, D.; Della Gravara, L.; Ragone, A.; Sapio, L.; Naviglio, S.; Gridelli, C. Prognostic factors in advanced non-small cell lung cancer patients treated with immunotherapy. Cancers 2023, 15, 4684. [Google Scholar] [CrossRef]
- Arbour, K.C.; Mezquita, L.; Long, N.; Rizvi, H.; Auclin, E.; Ni, A.; Martínez-Bernal, G.; Ferrara, R.; Lai, W.V.; Hendriks, L.E.L.; et al. Impact of baseline steroids on efficacy of programmed cell death-1 and programmed death-ligand 1 blockade in patients with non-small-cell lung cancer. J. Clin. Oncol. 2018, 36, 2872–2878. [Google Scholar] [CrossRef]
- Petrelli, F.; Signorelli, D.; Ghidini, M.; Ghidini, A.; Pizzutilo, E.G.; Ruggieri, L.; Cabiddu, M.; Borgonovo, K.; Dognini, G.; Brighenti, M.; et al. Association of steroids use with survival in patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Cancers 2020, 12, 546. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall, n (%) (n = 452) | YG n (%) (n = 195) | OG n (%) (n = 221) | AOG n (%) (n = 36) | p Value | |
|---|---|---|---|---|---|
| Sex | p < 0.001 | ||||
| Male | 371 (82.1%) | 145 (74.4%) | 195 (88.2%) | 31 (86.1%) | |
| Female | 81 (17.9%) | 50 (25.6%) | 26 (11.8%) | 5 (13.9%) | |
| Smoking status | p < 0.001 | ||||
| Current smoker | 204 (45.1%) | 111 (56.9%) | 84 (37.4%) | 9 (25%) | |
| Never smoker | 40 (8.8%) | 12 (6.2%) | 24 (10.8%) | 4 (11.1%) | |
| Former smoker | 208 (46.1%) | 72 (36.9%) | 113 (51.8%) | 23 (63.9%) | |
| ECOG PS | p = 0.111 | ||||
| 0–1 | 398 (88.1%) | 173 (88.7%) | 196 (88.7%) | 29 (80.6%) | |
| ≥2 | 54 (11.9%) | 22 (11.3%) | 25 (11.3%) | 7 (19.4%) | |
| Histology | p = 0.009 | ||||
| Adenocarcinoma | 264 (58.4%) | 131 (67.2%) | 118 (53.4%) | 15 (41.7%) | |
| Squamous cell carc. | 152 (33.6%) | 43 (22.1%) | 90 (40.7%) | 19 (52.8%) | |
| NOS | 33 (7.3%) | 19 (9.7%) | 12 (5.4%) | 2 (5.6%) | |
| Other | 3 (0.7%) | 2 (1.2%) | 1 (0.5%) | 0 (0%) | |
| PDL1 | p = 0.224 | ||||
| ≥50% | 183 (40.5%) | 77 (39.5%) | 88 (39.8%) | 18 (50%) | |
| 1–49% | 101 (22.3%) | 41 (21%) | 53 (24%) | 7 (19.4%) | |
| <1% | 101 (22.3%) | 54 (27.7%) | 42 (19%) | 5 (13.9%) | |
| Unknown | 67 (14.9%) | 23 (11.8%) | 38 (17.2%) | 6 (16.7%) | |
| Driver mutations | p = 0.083 | ||||
| ALK | 2 (0.4%) | 1 (0,5%) | 1 (0.5%) | 0 (0%) | |
| EGFR | 18 (4%) | 12 (6%) | 6 (3%) | 0 (0%) | |
| KRAS | 52 (10%) | 29 (10%) | 19 (9%) | 3 (8.3%) | |
| BRAF | 8 (2%) | 4 (2%) | 4 (2%) | 0 (0%) | |
| MET ex14 | 2 (0.4%) | 0 (0%) | 1 (0.5%) | 1 (2.8%) | |
| Stage | p = 0.024 | ||||
| Recurrent IIIA | 17 (3.8%) | 8 (4.1%) | 8 (3.6%) | 1 (2.8%) | |
| Recurrent IIIB | 17 (3.8%) | 5 (2.6%) | 10 (4.5%) | 2 (5.6%) | |
| Recurrent IIIC | 2 (0.4%) | 2 (1%) | 0 (0%) | 0 (0%) | |
| M1a | 158 (34.9%) | 54 (27.7%) | 86 (38.9%) | 18 (50%) | |
| M1b | 85 (18.8%) | 31 (15.9%) | 47 (21.3%) | 7 (19.4%) | |
| M1c | 173 (38.3%) | 95 (48.7%) | 70 (31.7%) | 8 (22.2%) | |
| M1 location | |||||
| Brain | 73 (16.2%) | 43 (22.1%) | 28 (12.7%) | 2 (5.6%) | p = 0.007 |
| Liver | 59 (13.1%) | 26 (13.3%) | 27 (12.2%) | 6 (16.7%) | p = 0.752 |
| Bone | 115 (25.4%) | 58 (29.7%) | 51 (23.1%) | 6 (16.7%) | p = 0.133 |
| Adrenal | 73 (16.2%) | 35 (17.9%) | 33 (14.9%) | 5 (13.9%) | p = 0.660 |
| Treatment line | p = 0.891 | ||||
| First line | 264 (58.4%) | 111 (56.9%) | 130 (56.9%) | 23 (63.9%) | |
| Second line | 153 (33.8%) | 66 (34.2%) | 75 (33.9%) | 12 (33.3%) | |
| Third and beyond | 35 (7.8%) | 18 (8.9%) | 16 (7.2%) | 1 (2.8%) | |
| Treatment regimen | p = 0.157 | ||||
| Chemotherapy-ICI | 149 (32.9%) | 70 (35.9%) | 72 (32.5%) | 7 (19.4%) | |
| Pembrolizumab | 135 (29.9%) | 52 (26.7%) | 67 (34.4%) | 16 (44.4%) | |
| Atezolizumab | 116 (25.7%) | 48 (24.6%) | 56 (28.7%) | 12 (33.3%) | |
| Nivolumab | 52 (11.5%) | 25 (12.8%) | 26 (13.3%) | 1 (2.8%) | |
| IrAEs | |||||
| Any grade | 170 (37.6%) | 83 (42.8%) | 72 (32.6%) | 15 (41.7%) | p = 0.106 |
| Grade 3–4 | 35 (21%) | 19 (9.7%) | 13 (5.9%) | 3 (8.3%) | p = 0.423 |
| Type of irAE | |||||
| Gastrointestinal | 23 (5.1%) | 15 (7.7%) | 3 (1.4%) | 5 (13.9%) | p < 0.001 |
| Pneumonitis | 21 (4.6%) | 9 (4.6%) | 9 (4.1%) | 3 (8.3%) | p = 0.002 |
| Hepatotoxicity | 18 (4%) | 9 (4.6%) | 9 (4.1%) | 0 (0%) | p = 0.956 |
| Skin toxicity | 46 (10.2%) | 22 (11.3%) | 21 (9.5%) | 3 (8.3%) | p = 0.427 |
| Renal toxicity | 8 (1.8%) | 3 (1.5%) | 5 (2.3%) | 0 (0%) | p = 0.578 |
| Thyroid dysfunction | 25 (5.5%) | 13 (6.7%) | 10 (4.5%) | 2 (5.6%) | p = 0.853 |
| Hypophysitis | 1 (0.2%) | 1 (0.5%) | 0 (0%) | 0 (0%) | p= 0.522 |
| Subsequent line | p = 0.045 | ||||
| 0 | 279 (61.7%) | 108 (55.7%) | 143 (64.7%) | 28 (77.8%) | |
| 1 | 134 (29.6%) | 65 (33.5%) | 61 (27.6%) | 8 (22.2%) | |
| ≥2 | 39 (8.6%) | 22 (11.3%) | 17 (7.7%) | 0 (0%) |
| Overall, n (%) (n = 452) | YG n (%) (n = 195) | OG n (%) (n = 221) | AOG n (%) (n = 36) | p Value | |
|---|---|---|---|---|---|
| Discontinuation reasons | |||||
| DP or death | 309 (68.4%) | 134 (68.7%) | 152 (66.8%) | 23 (63.9%) | 0.769 |
| Toxicity | 30 (6.6%) | 11 (5.6%) | 15 (6.8%) | 4 (11.1%) | 0.446 |
| Maintained response | 23 (5.1%) | 13 (6.7%) | 10 (4.5%) | 0 (0%) | 0.200 |
| Other causes | 29 (6.4%) | 8 (4.1%) | 18 (8.1%) | 3 (8.3%) | 0.240 |
| PFS OG/AOG | OS OG/AOG | |||
|---|---|---|---|---|
| HR | p-Value | HR | p-Value | |
| Sex | ||||
| Male | ||||
| Female | 0.89 (0.48–1.68) | 0.727 | 1.20 (0.72–2.00) | 0.476 |
| Histology | ||||
| Adenocarcinoma | ||||
| Squamous cell carc. | 0.73 (0.47–1.13) | 0.159 | 0.65 (0.45–0.94) | 0.022 |
| ECOG | ||||
| 0–1 | ||||
| ≥2 | 1.81 (0.95–3.45) | 0.070 | 2.56 (1.55–4.25) | <0.001 |
| NLR | ||||
| <3 | ||||
| ≥3 | 0.96 (0.62–1.50) | 0.857 | 1.33 (0.90–1.97) | 0.155 |
| Stage | ||||
| III/IVA | ||||
| IVB | 1.15 (0.71–1.89) | 0.570 | 1.20 (0.78–1.84) | 0.407 |
| Brain metastases | ||||
| No | ||||
| Yes | 1.72 (0.90–3.28) | 0.103 | 1.60 (0.91–2.80) | 0.100 |
| PD-L1 (%) | ||||
| <1% | ||||
| 1–49% | 0.76 (0.42–1.36) | 0.352 | 0.88 (0.54–1.42) | 0.598 |
| ≥50% | 0.78 (0.44–1.39) | 0.403 | 0.79 (0.48–1.30) | 0.352 |
| Treatment line | ||||
| First line | ||||
| Second line | 1.31 (0.77–2.24) | 0.320 | 1.14 (0.73–1.80) | 0.563 |
| Third and beyond | 0.64 (0.19–2.09) | 0.456 | 0.65 (0.23–1.81) | 0.405 |
| irAEs | ||||
| No irAEs | ||||
| irAEs | 0.46 (0.29–0.73) | 0.001 | 0.40 (0.26–0.60) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
del Corral-Morales, J.; Ayala-de Miguel, C.; Quintana-Cortés, L.; Sánchez-Vegas, A.; Aranda-Bellido, F.; González-Santiago, S.; Fuentes-Pradera, J.; Ayala-de Miguel, P. Real-World Data on Immune-Checkpoint Inhibitors in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Study. Cancers 2025, 17, 2194. https://doi.org/10.3390/cancers17132194
del Corral-Morales J, Ayala-de Miguel C, Quintana-Cortés L, Sánchez-Vegas A, Aranda-Bellido F, González-Santiago S, Fuentes-Pradera J, Ayala-de Miguel P. Real-World Data on Immune-Checkpoint Inhibitors in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Study. Cancers. 2025; 17(13):2194. https://doi.org/10.3390/cancers17132194
Chicago/Turabian Styledel Corral-Morales, José, Carlos Ayala-de Miguel, Laura Quintana-Cortés, Adrián Sánchez-Vegas, Fuensanta Aranda-Bellido, Santiago González-Santiago, José Fuentes-Pradera, and Pablo Ayala-de Miguel. 2025. "Real-World Data on Immune-Checkpoint Inhibitors in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Study" Cancers 17, no. 13: 2194. https://doi.org/10.3390/cancers17132194
APA Styledel Corral-Morales, J., Ayala-de Miguel, C., Quintana-Cortés, L., Sánchez-Vegas, A., Aranda-Bellido, F., González-Santiago, S., Fuentes-Pradera, J., & Ayala-de Miguel, P. (2025). Real-World Data on Immune-Checkpoint Inhibitors in Elderly Patients with Advanced Non-Small Cell Lung Cancer: A Retrospective Study. Cancers, 17(13), 2194. https://doi.org/10.3390/cancers17132194