Simple Summary
Primary central nervous system lymphoma is a rare but aggressive cancer that mostly affects older adults who often present with reduced performance status at first diagnosis. In this study, we reviewed the treatment courses and outcomes of 64 patients who received radiotherapy as part of their treatment. We aimed to understand which clinical factors influence patients’ survival and how radiotherapy can benefit patients who are not eligible for chemotherapy. Our analysis highlights that age ≥ 70 years, reduced performance status, seizures at diagnosis, and incomplete radiotherapy were linked to dismal outcomes. Interestingly, 80% of tumor relapses occurred within the initial tumor region, raising questions about the benefit of treating the entire brain. Our results provide insight into how radiotherapy could be better tailored to individual patients and highlight the need for further research to improve treatment strategies while minimizing side effects.
Abstract
Background/Objectives: Primary central nervous system lymphoma (PCNSL) is a rare but aggressive tumor, primarily affecting elderly patients. Radiotherapy (RT) remains an important treatment option, particularly for patients who are ineligible for systemic chemotherapy. This study aims to identify prognostic factors and evaluate recurrence patterns in a real-world cohort of PCNSL patients treated with RT. Methods: We retrospectively analyzed 64 PCNSL patients treated with radiotherapy at our institution between 2000 and 2022. Clinical characteristics, treatment details, and outcomes were collected by chart review. Overall survival (OS) was analyzed using Kaplan–Meier and Cox regression methods. Recurrence patterns were assessed based on available post-treatment imaging. Results: Median patient age was 71 years (range: 31–83); 53.1% had an Eastern Cooperative Oncology Group (ECOG) performance status ≥2. Radiotherapy was used as first-line treatment in 62.5% of cases, primarily due to contraindications to chemotherapy. Median OS was 10 months from diagnosis. Age, poor performance status, seizures at presentation, absence of systemic therapy, incomplete radiotherapy, and <80% applied dose of planned radiotherapy were associated with inferior OS in our univariable analysis. Multivariable analysis confirmed age, systemic therapy, seizures, and radiotherapy dose <80% as independent predictors. Among twenty-nine patients with imaging follow-up, eight recurrences after RT were documented: six of those within, and two outside of the initially affected areas. All recurrences occurred within previously irradiated areas. Conclusions: This study confirms known negative prognostic factors in PCNSL and underscores the importance of systemic chemotherapy for curatively intended treatments aiming for prolonged survival. The recurrence patterns observed question the added benefit of whole-brain irradiation in preventing distant relapses. These findings support the need for prospective trials to optimize radiotherapy strategies while balancing efficacy and neurotoxicity.
1. Introduction
Diffuse large B-cell lymphoma presenting as primary central nervous system (CNS) lymphoma (PCNSL) represents a rare form of Non-Hodgkin lymphoma, wherein brain, spinal cord, leptomeninges, and/or eyes are the only involved sites of disease. PCNSL accounts for approximately 4% of all primary malignant CNS tumors [1]. While the disease is confined to the CNS, it shares histopathological features with systemic diffuse large B-cell lymphoma, yet exhibits unique biological behavior and treatment responses due to the sanctuary nature of the CNS.
Radiotherapy, particularly whole-brain radiotherapy (WBRT), has historically played a pivotal role in the management of PCNSL, either as a primary modality for patients ineligible for chemotherapy or as consolidation following induction with high-dose systemic regimens [2,3,4]. However, its role has been re-evaluated over time due to concerns regarding late neurotoxicity and the emergence of more effective systemic treatment strategies [5,6,7].
PCNSL typically presents in older adults and is associated with aggressive clinical behavior, including rapidly progressive focal neurological deficits, neurocognitive impairment, and increased intracranial pressure. Without treatment, prognosis is dismal. The standard of care for fit patients consists of high-dose methotrexate (HD-MTX)-based chemotherapy, often in combination with rituximab and other agents such as cytarabine or thiotepa [2,6,8]. This approach has substantially improved outcomes, with reported median overall survival (OS) of up to 121 months in highly selected clinical trial cohorts [8]. However, a substantial proportion of patients—especially the elderly or frail—are ineligible for such regimens due to age-related vulnerability, comorbidities, or poor performance status. In addition, relapse and refractory disease remain critical therapeutic challenges, with limited evidence to guide second-line decision-making [9,10].
In this context, radiotherapy continues to have an important, albeit evolving, role. For chemotherapy-ineligible patients, WBRT remains a cornerstone of palliative and sometimes definitive treatment, offering rapid symptom relief and transient disease control [11]. For patients responding to systemic induction therapy, consolidative radiotherapy may help reduce CNS relapse rates, although its contribution to long-term neurotoxicity remains a matter of debate [8,12]. Particularly in older individuals, delayed cognitive deterioration after WBRT has prompted the evaluation of reduced-dose protocols and more focal radiotherapeutic strategies in prospective studies [12,13,14].
Despite advances in systemic therapy—including the implementation of high-dose chemotherapy with autologous stem cell transplantation, as well as novel agents such as ibrutinib, lenalidomide, and immune checkpoint inhibitors—radiotherapy remains a clinically relevant treatment option in selected patients [15,16,17]. Nonetheless, robust comparative data on the optimal timing, indication, and impact of radiotherapy in the real-world setting are scarce, especially outside of clinical trials.
In this retrospective study, we analyze the clinical course, treatment approaches, and outcomes of patients with PCNSL who received radiotherapy as part of their treatment course. By comparing patient characteristics and therapeutic responses across both first-line (primary treatment, n = 38; consolidation, n = 2) and second-line settings (progression during chemotherapy, n = 10; progression after chemotherapy, n = 14), we aim to provide real-world insights into the efficacy and tolerability of radiotherapy in this heterogeneous patient population. Our findings may help to refine treatment algorithms and identify subgroups of patients who derive particular benefit from the integration of radiotherapy into multimodal PCNSL therapy.
2. Materials and Methods
2.1. Patients and Study Design
This single-center study retrospectively analyzed patients receiving RT for PCNSL at our institution between 01/2000 and 12/2022. Patients and their respective diagnoses were identified by systematic keyword screening for “lymphoma” in tumor board protocols and manually pruned in the following step: Inclusion criteria required that patients had received at least one fraction of radiotherapy for cerebral lymphoma, either confirmed by histopathological diagnosis (n = 62; 97%) or, in the absence of histopathological verification, based on an interdisciplinary tumor board decision deeming the diagnosis highly probable and recommending treatment accordingly (n = 2; 3%). Data were extracted from physical patient records and RT treatment planning systems (Varian Eclipse, version 15.6, Varian Medical Systems, Palo Alto, CA, USA). Patient follow-up was evaluated through screening of hospital intern data processing systems (ixserv.4, version R20.3, ix.mid software technology, Köln, Germany) and ONKOSTAR (version 2.9.8, IT-Choice Software AG, Karlsruhe, Germany). The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University Medical Center Goettingen (protocol code 17/11/21, date of approval: 25 November 2021).
2.2. Treatment Planning and Administration of Radiotherapy
Treatment consisted of whole-brain irradiation (whole brain radiotherapy, WBRT) with (n = 7, 10.9%) or without (n = 57, 89.1%) tumor boost. WBRT was delivered via a standard helmet field technique (HF), including cervical vertebrae 1 and 2, employing bilateral opposed lateral fields in 95.3% of cases (n = 61); 3 patients received intensity-modulated radiotherapy (IMRT) or volumetric modulated arc therapy (VMAT) (4.7%, Table 1). Target delineation was applied according to hospital internal standard treatment protocols varying over time: Margins from clinical target volume (CTV) to planning target volume (PTV) differed between 5–10 mm; in the case of tumor boost, gross tumor volume (GTV) to CTV-Margin was 10 mm and CTV to PTV was 5 mm. Median prescribed dose including tumor boost was 45 Gy in 1.8 Gy/fraction (n = 45, 70.3%) and ranged from 30 Gy (n = 6, 3 Gy per fraction, due to poor general condition) up to 59,4 Gy (n = 2, according to the RTOG 88-06 trial, [3]).

Table 1.
Patient, disease and treatment characteristics. ECOG = Eastern Cooperative Oncology Group; RT = Radiotherapy; CTx = Chemotherapy (any); 3D-cRT = 3dimensional conformal Radiotherapy; IMRT/VMAT = Intensity-modulated Radiotherapy/Volumetric modulated Arc Therapy; * Applicable for n = 39 Pat.
2.3. Statistical Analysis
Statistical analyses were performed using SPSS (v26) and R (v4.0.2) with the “KMWin” (Kaplan–Meier for Windows) plugin [18]. Survival data were displayed by Kaplan–Meier plots; survival time comparisons were performed by log-rank tests. Univariable Cox regression was applied to assess the impact of variables on survival. We considered p-values < 0.05 as statistically significant. Univariably significant variables were consecutively tested in a multivariable fashion.
3. Results
3.1. Patient, Disease and Radiotherapy Treatment Characteristics
A total of 64 patients were included in this analysis. The median age was 71 years, ranging from 31 to 83 years, and female patients comprised the majority of the cohort (42 patients, 65.6%). At the start of radiotherapy, 30 patients (46.9%) had an ECOG performance status of 0 or 1, whereas 34 patients (53.1%) had a status of 2 or higher. Two out of sixty-four patients (3%) did not have histopathological confirmation (Section 2.1). Radiotherapy was administered as first-line treatment in 40 patients (62.5%) and as second-line treatment in 24 patients (37.5%). Treatment was discontinued prematurely in 27 patients (42.2%). The median prescribed radiotherapy dose was 45.0 Gy, with a range of 31.8 to 59.4 Gy. A total of 11 patients (17.2%) required concomitant anticonvulsant medication during radiotherapy. Please refer to Table 1 for details concerning patient, disease, and RT treatment characteristics.
3.2. Survival Parameters and Potential Influencers
The median OS from initial diagnosis for the entire cohort was 10 months (95% CI: 2.9–17). Among patients who received RT as part of first-line treatment—excluding those two treated with consolidative intent—the median OS was 6 months (95% CI: 2.8–9.1). In contrast, patients who underwent RT in the second-line setting had a median OS of 34 months (95% CI: 21.3–46.6; p = 0.003 vs. first-line treatment, log-rank test). Of the 2 patients who received consolidative treatment, 1 was still alive at the 127-month follow-up, while the other was lost to follow-up due to relocation to another country.
When OS was calculated from the initiation of RT, the median OS was 4 months (95% CI: 0.5–7.5) for first-line RT patients and 10 months (95% CI: 3.4–16.6) for those receiving RT in the second-line setting (p = 0.42, log-rank test). Kaplan–Meier survival curves illustrating the survival outcomes are shown in Figure 1 and Figure 2.
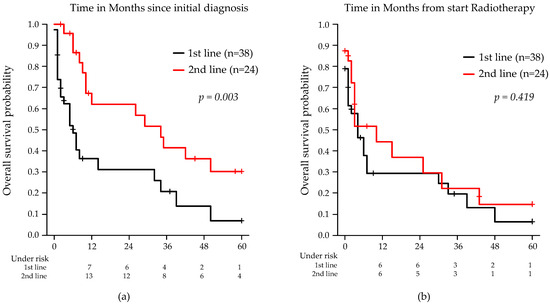
Figure 1.
Kaplan–Meier estimates of OS stratified by RT in first- or second-line treatment of PCNSL: (a) from initial diagnosis; (b) from the start of RT. Note: Two patients who received consolidative RT were excluded from the analysis.
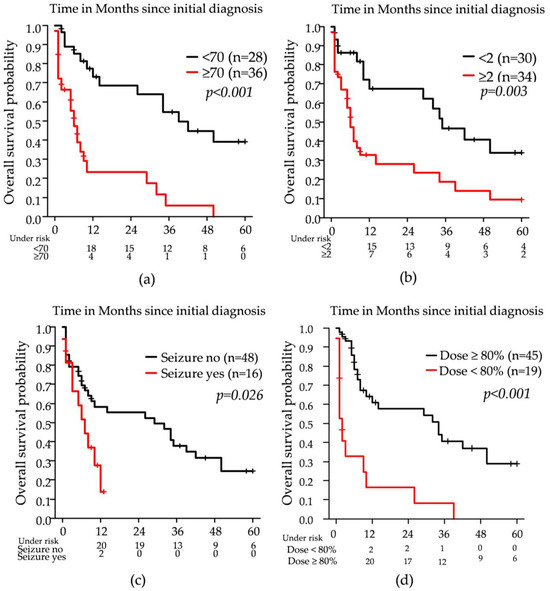
Figure 2.
Kaplan–Meier estimates of overall survival (OS) stratified by clinical prognostic factors: (a) age ≥ 70 vs. <70 years; (b) baseline ECOG performance status <2 vs. ≥2; (c) presence vs. absence of seizures at diagnosis; (d) radiotherapy dose application (<80% vs. ≥80%).
Older age (≥70 years), baseline ECOG ≥ 2, systemic therapy, seizures as a presenting symptom, RT completion as intended, receipt of ≥80% of the prescribed RT dose, and RT line (first vs. second) were all associated with OS in univariable Cox regression analysis. In the multivariable model, age, systemic therapy, seizures, and administration of ≥80% of the RT dose remained statistically significant. Detailed results are provided in Table 2.
Table 2.
Influence of potential prognostic factors on patients’ OS from initial diagnosis. Calculations were done by Cox regression analyses. p values < 0.05 were considered statistically significant and are depicted in bold. Variables with p < 0.1 in univariable analysis were consecutively tested in a multivariable Cox regression model. CI = confidence interval; CCI = Charlson Comorbidity Index, dichotomized by median (=5), Gy = Gray, n.s. = not significant; ECOG = Eastern Cooperative Oncology Group; RT = Radiotherapy * only applicable for n = 17 patients due to missing data.
Radiotherapy dose completion was assessed relative to the initially prescribed total dose. Patients receiving <80% of the intended dose (n = 19) had experienced early discontinuation of treatment, predominantly due to clinical deterioration. In this subgroup, the applied doses ranged from 5.4 Gy to 34.2 Gy, corresponding to 12% to 76% of the planned regimen. Most patients in this group received between 20% and 60% of the intended dose.
The median delivered dose was 21.6 Gy (interquartile range (IQR) 13.2–27.9 Gy). The 80% threshold was pragmatically chosen to differentiate between patients with marked treatment deviations and those who completed radiotherapy as planned, thus enabling stratified survival analysis based on treatment adherence.
3.3. Local Recurrences
Of the total cohort, 45.3% (29/64 patients) underwent post-radiotherapy cerebral imaging, including six patients with contrast-enhanced cerebral CT and twenty-three with contrast-enhanced MRI. Intracerebral recurrence was identified in eight patients—seven by MRI and one by CT. Six out of these eight patients showed local recurrence within or overlapping the original lymphoma manifestation; four of those had initial HF treatment to 45 Gy, two had HF and sequential local boost (37.5 Gy WBRT + 7.5 Gy Boost; 23.4 Gy WBRT + 21.6 Gy Boost). Two out of eight intracerebral recurrences were distant to the initial manifestation; both patients had previously received WBRT in HF technique (45 Gy, 54 Gy), therefore including the area of the following recurrence. Reirradiation was applied in two patients: one with HF technique up to 19.8 Gy (initially: 45 Gy), and one with local reirradiation up to 36 Gy (initial RT 23.4/21.6 Gy). Please refer to Figure 3 for an example of a local recurrence treated with focal re-irradiation.
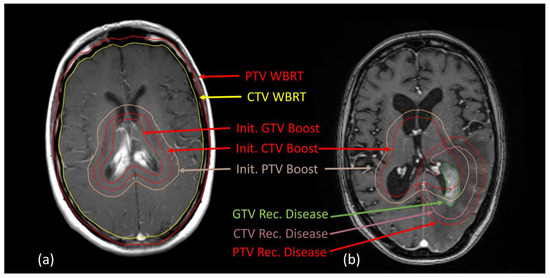
Figure 3.
Representative MRI slices matched with RT planning CT. (a) Initial lymphoma manifestation in the area of mid/posterior corpus callosum and corresponding target volumes, (b) local recurrence at the posterior horn of the left lateral ventricle partly overlapping the initial boost volume, 36 months after initial RT treatment. Abbreviations: GTV = gross tumor volume, CTV = clinical target volume, PTV = planning target volume. Treatment was applied via volumetric modulated arc therapy, initial dosing: PTV whole-brain RT in HF volume: 23.4 Gy/1.8 Gy/fraction; PTV Boost: 21.6 Gy/1.8 Gy; PTV recurrent disease: 36 Gy/1.8 Gy/fraction.
4. Discussion
In this retrospective analysis of 64 patients diagnosed with PCNSL who received RT as part of their treatment regimen, several clinically relevant observations were made. The median age of 71 years indicated that the cohort is a representative PCNSL cohort aligning with the known epidemiology of PCNSL, which predominantly affects elderly individuals. More than half of the patients (53.1%) presented with an ECOG performance status ≥2 at the start of RT, indicating a clinically highly vulnerable population. Seizures were the initial symptom in 25% of patients—an indicator of potentially advanced disease. Furthermore, in 27 cases, comprising 43% of the whole cohort, RT was aborted prematurely, mainly due to a further deterioration in general condition.
RT was administered as first-line therapy in the majority of patients (62.5%), mainly due to insufficient general condition, contraindication for chemotherapy regimens, or toxicity-induced therapy discontinuation (37/40 patients, 92.5%). This reflects both institutional standards—reserving high-dose chemotherapy and autologous stem cell transplantation for fit patients—and the prognostically adverse composition of our cohort. A limitation of our study is the absence of histological confirmation in two patients (3%). While this reflects real-world challenges in frail patients with typical imaging and clinical presentation, it may slightly affect diagnostic accuracy and the interpretation of outcomes.
Median OS from diagnosis was 10 months and was significantly longer in the second-line group. However, when using RT initiation as the starting point, no statistically significant OS difference remained between first- and second-line RT, underlining the central role of systemic chemotherapy. In univariable analysis, age ≥ 70, ECOG ≥ 2, seizure presentation, absence of systemic therapy, incomplete RT, and dose < 80% were all associated with inferior OS. Multivariable analysis confirmed age, systemic therapy, seizures, and RT dose ≥80% as independent predictors. These results corroborate existing data showing that advanced age and poor performance status are among the strongest negative predictors for survival in PCNSL—primarily by representing a contraindication for systemic therapy [10,15,16,19]. If RT is applied as the only therapeutic option, the completion and dose intensity of RT might appear to be critical determinants of treatment effectiveness. However, in our cohort, these results most likely reflect (further) deterioration of general condition during treatment due to PCNSL and, subsequently, very limited short-term survival. Thus, in very frail patients, the decision to initiate RT must weigh potential benefit against limited prognosis. However, it should be noted that WBRT has shown superiority to best supportive care in terms of survival [11].
Interestingly, seizure presentation emerged as an independent predictor of poor outcome. Although seizures are not commonly discussed as a prognostic marker in PCNSL, they may reflect underlying extensive cortical involvement or elevated intracranial pressure, which could contribute to worse clinical status and reduced treatment tolerance [17].
Consolidative RT was remarkably low (n = 2, 3.1%), indicating relevant restraints due to concerns of negative neurocognitive outcomes after combined treatment [20].
It is known that a multitude of factors can influence neurocognitive outcome: higher age, previous systemic therapy, as well as high RT dose seem to be of highest relevance [21]. In recent years, encouraging prospective data indicating suitability of low-dose (ld-) WBRT (23.4 Gy/1.8 Gy/fr) following systemic therapy without an increase in neurotoxicity and improved PFS have been reported [22]. The use of ld-WBRT, supported by large-scale retrospective data, have since been widely implemented in various guidelines and are now part of routine treatment at our institution [23,24,25].
An ongoing debate among radiation oncology experts concerns the use of WBRT versus partial-brain radiotherapy (PBRT) [14,26,27]. We assessed recurrence patterns in 29 patients with follow-up imaging (45% of the cohort, 78% of those completing therapy). Consistent with literature indicating that only 20% of recurrences are detected via routine imaging, eight intracerebral recurrences were identified [28,29]. Notably, both patients with distant recurrences had previously received WBRT with total doses of 45 Gy and 54 Gy, respectively. This finding aligns with the pattern observed in the six patients who relapsed locally, all of whom had also received radiotherapy to a dose of 45 Gy, with or without an additional boost. Notably, all recurrences—whether local or distant—occurred within areas that had received doses of 45 Gy or higher. Similar findings have been reported in retrospective data from Japan, where both in-field and out-of-field recurrences were documented [30]. Data from Italy indicated that up to 60% of relapses occurred outside the initially irradiated volumes [12]. These discrepancies underline the heterogeneity of recurrence patterns and the challenges in defining optimal target volumes. Recent radiotherapy approaches such as hippocampal-sparing whole-brain irradiation aim to preserve cognitive function without compromising oncological outcomes, particularly in the context of primary or consolidative treatment. However, the feasibility of such techniques in PCNSL remains uncertain due to the frequent periventricular location of lesions and the currently limited clinical evidence supporting their use in this specific setting [12,31].
Currently, recommendations concerning target volume delineation and the use of (simultaneously integrated) boost concepts differ between guidelines [24,32,33]. Our findings—while based on a retrospective design and a limited patient cohort—may question the assumption that WBRT offers superior protection against distant intracranial recurrence. Despite extended target volumes and relatively high total doses, WBRT did not prevent relapses outside the initially involved sites. However, as only a small number of patients (n = 7) received a focal radiotherapy boost, the observed recurrence pattern must be interpreted with caution. No definitive conclusions can be drawn regarding the comparative benefit of whole-brain versus focal irradiation. Additionally, the occurrence of relapses within previously irradiated areas may suggest radioresistance rather than insufficient spatial coverage. Still, a potential benefit of WBRT in preventing future, currently subclinical relapses cannot be excluded, particularly given the retrospective nature of our analysis. For example, data from a French survey of 79 patients reported of significantly shorter OS when PBRT was applied as opposed to WBRT [34]. Reducing total WBRT dose appears to be a viable option not only in the case of consolidation [26]. Contrarily, there are also emerging data on stereotactic ablative RT specifically targeting CNS lesions or combinations of ld-WBRT with SBRT-boost [13,35,36].
In conclusion, both the RT field size (WBRT versus focal) and dose strategies, including ld-WBRT with or without boost, can significantly impact neurocognitive outcomes but remain insufficiently defined by current evidence. Our real-world data contribute to the existing literature by reaffirming established prognostic factors and questioning the assumed oncological superiority of whole-brain radiotherapy. These findings highlight the urgent need for prospective clinical trials to refine radiotherapy approaches and improve personalized treatment for patients with PCNSL.
5. Conclusions
This retrospective analysis of PCNSL patients receiving RT highlights the clinical relevance of known prognostic factors such as age and the ability to receive systemic chemotherapy. Importantly, seizure presentation and incomplete RT—both indicative of aggressive disease and limited treatment tolerance—were also associated with significantly inferior outcomes.
All observed relapses, including distant ones, occurred within previously irradiated regions, suggesting dose resistance rather than insufficient coverage. Given the growing emphasis on minimizing neurotoxicity, approaches such as low-dose WBRT and focal boost concepts warrant further investigation. Overall, our real-world data underscore the urgent need for prospective trials to refine radiotherapy strategies in PCNSL and guide individualized treatment decisions based on clinical and biological risk profiles.
Author Contributions
Conceptualization, M.G., S.R., S.B., J.C.B., and B.C.; methodology, S.B., J.C.B., M.G., S.R., M.L.; software, M.L., J.C.B., M.G.; validation, M.G., M.L., J.C.B., S.B.; formal analysis, M.G., M.L., S.B., J.C.B., investigation, J.C.B., E.A., G.G.W., B.C., M.Z.A., C.M.Z., L.H.D., M.A.S., N.B., H.T., L.-A.v.D., R.A.E.S., S.R., S.D.; resources, M.G., S.R.; data curation, M.G., M.L., J.C.B., S.B.; writing—original draft preparation, M.G.; writing—review and editing, J.C.B., S.B., H.T., E.A., N.B., G.G.W., C.M.Z., M.Z.A., S.D., R.A.E.S., L.-A.v.D., J.T.O., M.A.S., L.H.D., M.L., B.C., S.R., M.G.; visualization, M.L., M.G.; supervision, M.G., S.R.; project administration, M.G., S.R., B.C.; funding acquisition, S.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University Medical Center Goettingen (protocol code 17/11/21, date of approval: 25 November 2021).
Informed Consent Statement
Due to the retrospective study design, additional informed consent was not required.
Data Availability Statement
The datasets generated and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CCI | Charlson Comorbidity Index |
| CI | confidence interval |
| CTV | clinical target volume |
| CTx | Chemotherapy |
| ECOG | Eastern Cooperative Oncology Group |
| GTV | gross tumor volume |
| Gy | Gray |
| HF | helmet field technique |
| IMRT | intensity-modulated radiotherapy |
| ld | Low-dose |
| n.s. | not significant |
| OS | Overall survival |
| PCNSL | Primary central nervous system lymphoma |
| PTV | planning target volume |
| RT | Radiotherapy |
| VMAT | volumetric modulated arc therapy |
| WBRT | whole-brain radiotherapy |
| 3D-cRT | 3dimensional conformal Radiotherapy |
References
- Villano, J.L.; Koshy, M.; Shaikh, H.; Dolecek, T.A.; McCarthy, B.J. Age, gender, and racial differences in incidence and survival in primary CNS lymphoma. Br. J. Cancer 2011, 105, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.G.; Correa, D.D.; Yahalom, J.; Raizer, J.J.; Schiff, D.; Grant, B.; Grimm, S.; Lai, R.K.; Reiner, A.S.; Panageas, K.; et al. Rituximab, methotrexate, procarbazine, and vincristine followed by consolidation reduced-dose whole-brain radiotherapy and cytarabine in newly diagnosed primary CNS lymphoma: Final results and long-term outcome. J. Clin. Oncol. 2013, 31, 3971–3979. [Google Scholar] [CrossRef]
- Schultz, C.; Scott, C.; Sherman, W.; Donahue, B.; Fields, J.; Murray, K.; Fisher, B.; Abrams, R.; Meis-Kindblom, J. Preirradiation chemotherapy with cyclophosphamide, doxorubicin, vincristine, and dexamethasone for primary CNS lymphomas: Initial report of radiation therapy oncology group protocol 88-06. J. Clin. Oncol. 1996, 14, 556–564. [Google Scholar] [CrossRef]
- Abrey, L.E.; Ben-Porat, L.; Panageas, K.S.; Yahalom, J.; Berkey, B.; Curran, W.; Schultz, C.; Leibel, S.; Nelson, D.; Mehta, M.; et al. Primary central nervous system lymphoma: The Memorial Sloan-Kettering Cancer Center prognostic model. J. Clin. Oncol. 2006, 24, 5711–5715. [Google Scholar] [CrossRef] [PubMed]
- Calimeri, T.; Steffanoni, S.; Gagliardi, F.; Chiara, A.; Ferreri, A.J.M. How we treat primary central nervous system lymphoma. ESMO Open 2021, 6, 100213. [Google Scholar] [CrossRef] [PubMed]
- Houillier, C.; Taillandier, L.; Dureau, S.; Lamy, T.; Laadhari, M.; Chinot, O.; Moluçon-Chabrot, C.; Soubeyran, P.; Gressin, R.; Choquet, S.; et al. Radiotherapy or Autologous Stem-Cell Transplantation for Primary CNS Lymphoma in Patients 60 Years of Age and Younger: Results of the Intergroup ANOCEF-GOELAMS Randomized Phase II PRECIS Study. J. Clin. Oncol. 2019, 37, 823–833. [Google Scholar] [CrossRef]
- Correa, D.D.; Braun, E.; Kryza-Lacombe, M.; Ho, K.-W.; Reiner, A.S.; Panageas, K.S.; Yahalom, J.; Sauter, C.S.; Abrey, L.E.; DeAngelis, L.M.; et al. Longitudinal cognitive assessment in patients with primary CNS lymphoma treated with induction chemotherapy followed by reduced-dose whole-brain radiotherapy or autologous stem cell transplantation. J. Neurooncol. 2019, 144, 553–562. [Google Scholar] [CrossRef]
- Houillier, C.; Soussain, C.; Ghesquières, H.; Soubeyran, P.; Chinot, O.; Taillandier, L.; Lamy, T.; Choquet, S.; Ahle, G.; Damaj, G.; et al. Management and outcome of primary CNS lymphoma in the modern era: An LOC network study. Neurology 2020, 94, e1027–e1039. [Google Scholar] [CrossRef]
- Kaulen, L.D.; Baehring, J.M. Treatment Options for Recurrent Primary CNS Lymphoma. Curr. Treat. Options Oncol. 2022, 23, 1548–1565. [Google Scholar] [CrossRef]
- Mendez, J.S.; Ostrom, Q.T.; Gittleman, H.; Kruchko, C.; DeAngelis, L.M.; Barnholtz-Sloan, J.S.; Grommes, C. The elderly left behind-changes in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro Oncol. 2018, 20, 687–694. [Google Scholar] [CrossRef]
- Song, J.; Samant, R.; Jay, M.; Chaudry, H.; Fan, X.Y.; MacDonald, D.; Bence-Bruckler, I.; Nair, V. Whole brain radiotherapy improves survival outcomes in primary CNS lymphoma patients ineligible for systemic therapy. Support. Care Cancer 2020, 28, 5363–5369. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, C.; Chiesa, S.; Toppi, L.; Hohaus, S.; Gaudino, S.; D’Alo, F.; Dinapoli, N.; Davide, R.; Zinicola, T.; Bracci, S.; et al. May we routinely spare hippocampal region in primary central nervous system lymphoma during whole brain radiotherapy? Radiat. Oncol. 2023, 18, 161. [Google Scholar] [CrossRef]
- Foreman, B.E.; Mullikin, T.C.; Floyd, S.R.; Kelsey, C.R.; Patel, M.P.; Peters, K.B.; Kirkpatrick, J.P.; Reitman, Z.J.; Vaios, E.J. Long-term outcomes with reduced-dose whole-brain radiotherapy and a stereotactic radiosurgery boost for primary central nervous system lymphoma. Neurooncol. Adv. 2023, 5, vdad097. [Google Scholar] [CrossRef]
- Shibamoto, Y.; Hayabuchi, N.; Hiratsuka, J.; Tokumaru, S.; Shirato, H.; Sougawa, M.; Oya, N.; Uematsu, Y.; Hiraoka, M. Is whole-brain irradiation necessary for primary central nervous system lymphoma? Patterns of recurrence after partial-brain irradiation. Cancer 2003, 97, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Ney, D.E.; Reiner, A.S.; Panageas, K.S.; Brown, H.S.; DeAngelis, L.M.; Abrey, L.E. Characteristics and outcomes of elderly patients with primary central nervous system lymphoma: The Memorial Sloan-Kettering Cancer Center experience. Cancer 2010, 116, 4605–4612. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Hamamoto, Y.; Fujii, T.; Ochi, T.; Harada, H.; Ohnishi, T.; Mochizuki, T. Prognosis of primary central nervous system lymphoma treated with radiotherapy alone. Jpn. J. Radiol. 2012, 30, 806–810. [Google Scholar] [CrossRef]
- Aboubakr, O.; Houillier, C.; Alentorn, A.; Choquet, S.; Dupont, S.; Mokhtari, K.; Leclercq, D.; Nichelli, L.; Kas, A.; Rozenblum, L.; et al. Epilepsy in Patients With Primary CNS Lymphoma: Prevalence, Risk Factors, and Prognostic Significance. Neurology 2024, 103, e209748. [Google Scholar] [CrossRef]
- Gross, A.; Ziepert, M.; Scholz, M. KMWin—A convenient tool for graphical presentation of results from Kaplan-Meier survival time analysis. PLoS ONE 2012, 7, e38960. [Google Scholar] [CrossRef]
- Curry, L.D.; Munker, R.; Li, N.; Yan, D.; Pryor, P.; Nozad, S.; Keller, P.; Monohan, G.P.; Iragavarapu, C.; Krem, M.M. Performance status, comorbidities, and cycles of methotrexate exert the greatest influence on outcomes of primary and secondary CNS lymphomas: The Lexington experience. Ann. Hematol. 2023, 102, 141–154. [Google Scholar] [CrossRef]
- Omuro, A.M.P.; Ben-Porat, L.S.; Panageas, K.S.; Kim, A.K.; Correa, D.D.; Yahalom, J.; DeAngelis, L.M.; Abrey, L.E. Delayed neurotoxicity in primary central nervous system lymphoma. Arch. Neurol. 2005, 62, 1595–1600. [Google Scholar] [CrossRef]
- Morales-Martinez, A.; Lozano-Sanchez, F.; Duran-Peña, A.; Hoang-Xuan, K.; Houillier, C. Primary Central Nervous System Lymphoma in Elderly Patients: Management and Perspectives. Cancers 2021, 13, 3479. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.M.P.; DeAngelis, L.M.; Karrison, T.; Bovi, J.A.; Rosenblum, M.; Corn, B.W.; Correa, D.; Wefel, J.S.; Aneja, S.; Grommes, C.; et al. Randomized phase II study of rituximab, methotrexate (MTX), procarbazine, vincristine, and cytarabine (R-MPV-A) with and without low-dose whole-brain radiotherapy (LD-WBRT) for newly diagnosed primary CNS lymphoma (PCNSL). J. Clin. Oncol. 2020, 38, 2501. [Google Scholar] [CrossRef]
- Tringale, K.R.; Scordo, M.; Yahalom, J.; White, C.; Zhang, Z.; Schefflein, J.; Cederquist, G.; Schaff, L.R.; DeAngelis, L.; Imber, B.S.; et al. Evolving consolidation patterns and outcomes for a large cohort of patients with primary CNS lymphoma. Blood Adv. 2024, 8, 6195–6206. [Google Scholar] [CrossRef] [PubMed]
- Nabors, B.; Portnow, J.; Hattangadi-Gluth, J.; Horbinski, C. NCCN CNS tumor guidelines update for 2023. Neuro Oncol. 2023, 25, 2114–2116. [Google Scholar] [CrossRef]
- Ferreri, A.J.M.; Calimeri, T.; Cwynarski, K.; Dietrich, J.; Grommes, C.; Hoang-Xuan, K.; Hu, L.S.; Illerhaus, G.; Nayak, L.; Ponzoni, M.; et al. Primary central nervous system lymphoma. Nat. Rev. Dis. Primers 2023, 9, 29. [Google Scholar] [CrossRef]
- Ko, M.-K.; Kwak, Y.-K.; Choi, B.-O.; Jeun, S.-S.; Park, J.-S.; Ahn, S.; Song, J.-H. Is reduced-dose whole-brain radiotherapy also feasible in primary CNS lymphoma for curative or salvage purpose? J. Neurooncol. 2023, 165, 321–328. [Google Scholar] [CrossRef]
- Wu, S.Y.; Braunstein, S.E.; Rubenstein, J.L.; Sneed, P.K. Stereotactic Radiosurgery for Primary Central Nervous System Lymphoma. Cureus 2023, 15, e34817. [Google Scholar] [CrossRef]
- Langner-Lemercier, S.; Houillier, C.; Soussain, C.; Ghesquières, H.; Chinot, O.; Taillandier, L.; Soubeyran, P.; Lamy, T.; Morschhauser, F.; Benouaich-Amiel, A.; et al. Primary CNS lymphoma at first relapse/progression: Characteristics, management, and outcome of 256 patients from the French LOC network. Neuro Oncol. 2016, 18, 1297–1303. [Google Scholar] [CrossRef]
- Jahnke, K.; Thiel, E.; Martus, P.; Herrlinger, U.; Weller, M.; Fischer, L.; Korfel, A. Relapse of primary central nervous system lymphoma: Clinical features, outcome and prognostic factors. J. Neurooncol. 2006, 80, 159–165. [Google Scholar] [CrossRef]
- Iwabuchi, M.; Shibamoto, Y.; Sugie, C.; Ayakawa, S.; Ogino, H.; Baba, F. Partial-brain radiotherapy for primary central nervous system lymphoma: Multi-institutional experience. J. Radiat. Res. 2016, 57, 164–168. [Google Scholar] [CrossRef]
- Wagner, H.; Ali, A.; Glantz, M.; Blakeley, A. Role of Hippocampal-Avoidance Whole Brain Radiation Therapy (HA-WBRT) in Patients with Primary CNS Lymphoma (PCNSL). Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, E424. [Google Scholar] [CrossRef][Green Version]
- Manickam Gurusamy, V.; Raveendran Divakar, S.; Halsnad Chandramouli, S.; Kunheri, B.; Hussain Al-Abdulla, H.; Shaikh, G.; Chaudary Apsani, R.; Riyaz Poolakundan, M.; Caparrotti, P.; Wafiq Hammoud, R.; et al. The role of radiotherapy in newly diagnosed primary CNS lymphoma: A descriptive review and a pragmatic approach to clinical practice. Clin. Transl. Radiat. Oncol. 2023, 39, 100559. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.M.; Illerhaus, G.; Doorduijn, J.K.; Auer, D.P.; Bromberg, J.E.C.; Calimeri, T.; Cwynarski, K.; Fox, C.P.; Hoang-Xuan, K.; Malaise, D.; et al. Primary central nervous system lymphomas: EHA-ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2024, 35, 491–507. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Joulié, A.; Houillier, C.; Antoni, D.; Créhange, G.; Jouglar, E.; Colin, P.; Benchalal, M.; Lang, P.; Alfonsi, M.; Hamidou, H.; et al. Brain radiotherapy in patients treated for a newly diagnosed primary central nervous system lymphoma: Professional practice evaluation in 19 French centers. Acta Oncol. 2023, 62, 648–656. [Google Scholar] [CrossRef]
- Palmer, J.D.; Bhamidipati, D.; Shukla, G.; Epperla, N.; Glass, J.; Kim, L.; Shi, W. Outcomes after stereotactic radiosurgery for CNS lymphoma. J. Neurooncol. 2020, 147, 465–476. [Google Scholar] [CrossRef]
- Seidel, C.; Viehweger, C.; Kortmann, R.-D. Is There an Indication for First Line Radiotherapy in Primary CNS Lymphoma? Cancers 2021, 13, 2580. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).