

Real-World Evidence of Treatment-Free Remission Strategies and Outcomes in Chronic Myeloid Leukemia

 , , , ,
, , , ,
Simple Summary
Abstract
1. Introduction
2. Methods
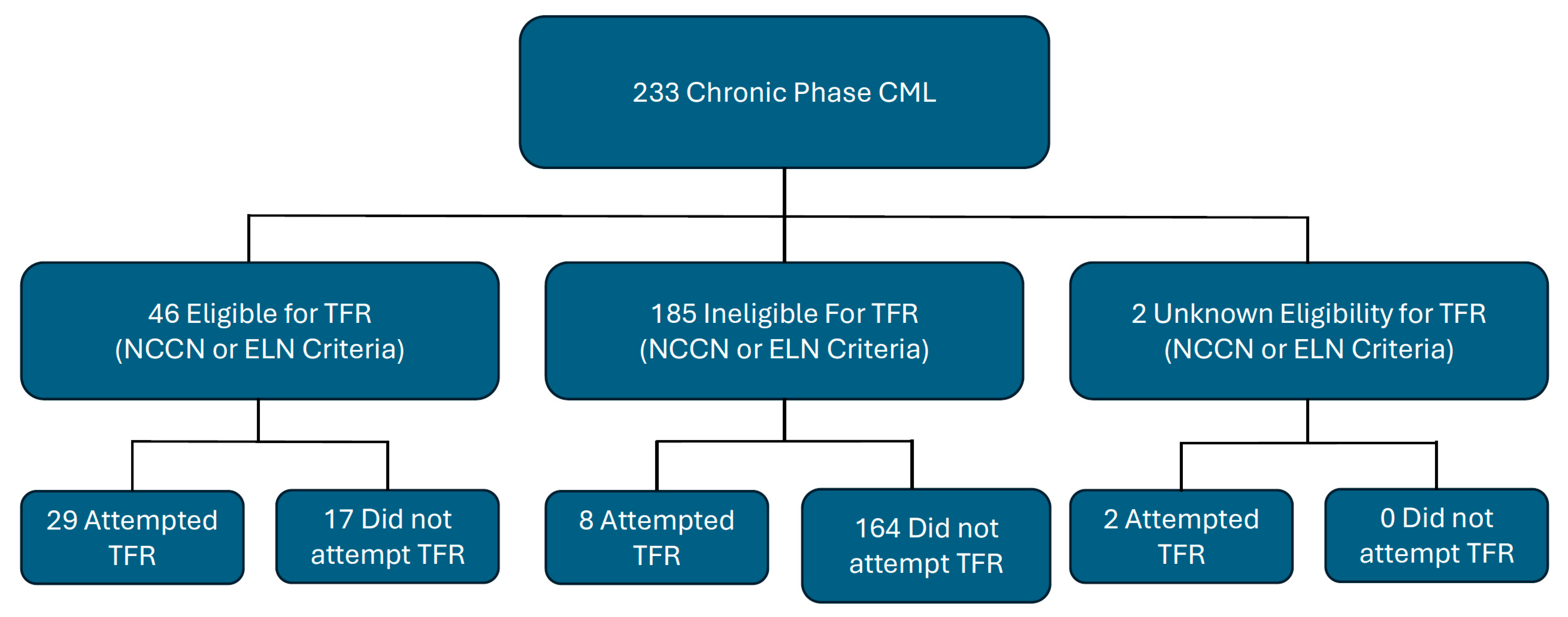
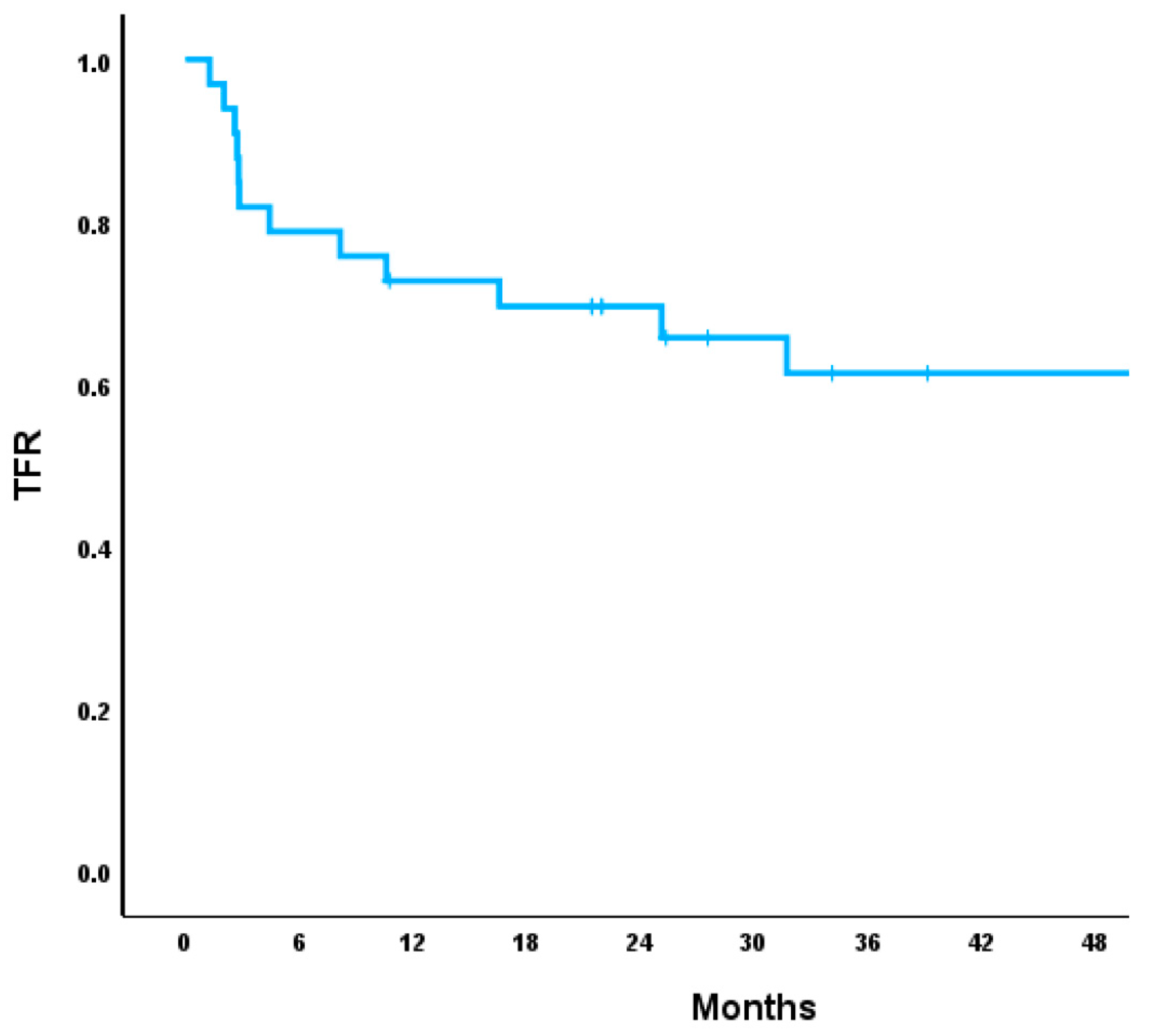
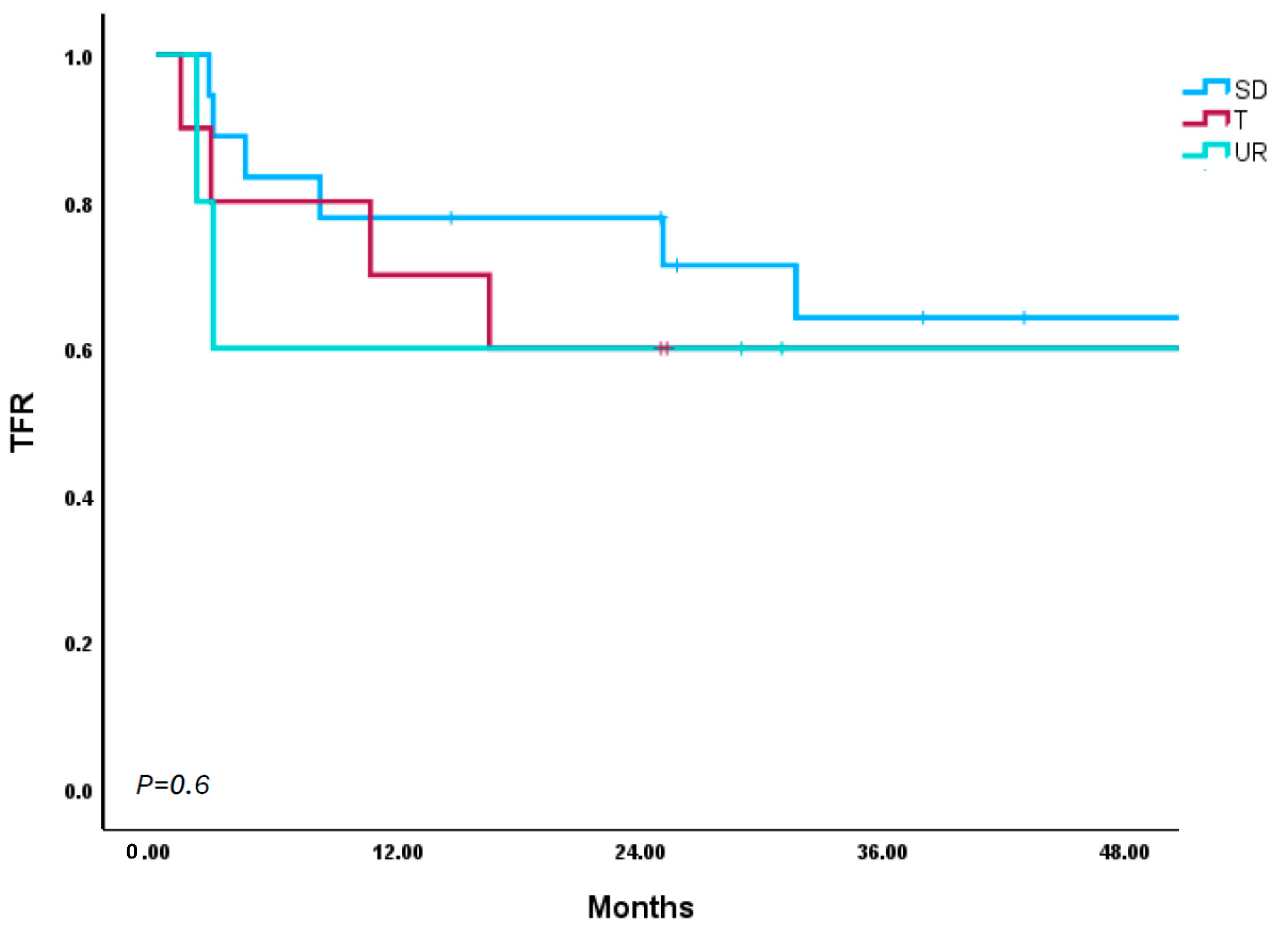
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourne, G.; Bhatia, R.; Jamy, O. Treatment-Free Remission in Chronic Myeloid Leukemia. J. Clin. Med. 2024, 13, 2567. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.; O’Brien, S.; Jabbour, E.; Garcia-Manero, G.; Quintas-Cardama, A.; Shan, J.; Rios, M.B.; Ravandi, F.; Faderl, S.; Kadia, T.; et al. Improved survival in chronic myeloid leukemia since the introduction of imatinib therapy: A single-institution historical experience. Blood 2012, 119, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Oehler, V.G.; Koller, P.B.; Jamy, O.; Lomaia, E.; Hunter, A.M.; Uspenskaya, O.; Samarina, S.; Mukherjee, S.; Cortes, J.E.; et al. Olverembatinib After Failure of Tyrosine Kinase Inhibitors, Including Ponatinib or Asciminib: A Phase 1b Randomized Clinical Trial. JAMA Oncol. 2025, 11, 28–35. [Google Scholar] [CrossRef]
- Kantarjian, H.; Zhai, Y.; Oehler, V.G.; Jamy, O.; Koller, P.B.; Haddad, F.G.; Sasaki, K.; Jabbour, E.J. Olverembatinib in chronic myeloid leukemia-Review of historical development, current status, and future research. Cancer 2025, 131, e35832. [Google Scholar] [CrossRef]
- Cohen, M.H.; Johnson, J.R.; Pazdur, R.U.S. Food and Drug Administration Drug Approval Summary: Conversion of imatinib mesylate (STI571; Gleevec) tablets from accelerated approval to full approval. Clin. Cancer Res. 2005, 11, 12–19. [Google Scholar] [CrossRef]
- Jamy, O.; Godby, R.; Sarmad, R.; Costa, L.J. Survival of chronic myeloid leukemia patients in comparison to the general population in the tyrosine kinase inhibitors era: A US population-based study. Am. J. Hematol. 2021, 96, E265–E268. [Google Scholar] [CrossRef]
- Shah, N.P.; Bhatia, R.; Altman, J.K.; Amaya, M.; Begna, K.H.; Berman, E.; Chan, O.; Clements, J.; Collins, R.H.; Curtin, P.T.; et al. Chronic Myeloid Leukemia, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2024, 22, 43–69. [Google Scholar] [CrossRef]
- Jamy, O.; Sarmad, R.; Costa, L. Risk and outcomes of second malignant neoplasms in chronic myeloid leukemia survivors. Leuk. Res. 2019, 82, 1–6. [Google Scholar] [CrossRef]
- Mahon, F.X.; Réa, D.; Guilhot, J.; Guilhot, F.; Huguet, F.; Nicolini, F.; Legros, L.; Charbonnier, A.; Guerci, A.; Varet, B.; et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: The prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010, 11, 1029–1035. [Google Scholar] [CrossRef]
- Clark, R.E.; Polydoros, F.; Apperley, J.F.; Milojkovic, D.; Pocock, C.; Smith, G.; Byrne, J.L.; de Lavallade, H.; O’Brien, S.G.; Coffey, T.; et al. De-escalation of tyrosine kinase inhibitor dose in patients with chronic myeloid leukaemia with stable major molecular response (DESTINY): An interim analysis of a non-randomised, phase 2 trial. Lancet Haematol. 2017, 4, e310–e316. [Google Scholar] [CrossRef]
- Lee, S.E.; Choi, S.Y.; Song, H.Y.; Kim, S.H.; Choi, M.Y.; Park, J.S.; Kim, H.J.; Kim, S.H.; Zang, D.Y.; Oh, S.; et al. Imatinib withdrawal syndrome and longer duration of imatinib have a close association with a lower molecular relapse after treatment discontinuation: The KID study. Haematologica 2016, 101, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Mahon, F.X.; Boquimpani, C.; Kim, D.W.; Benyamini, N.; Clementino, N.C.D.; Shuvaev, V.; Ailawadhi, S.; Lipton, J.H.; Turkina, A.G.; De Paz, R.; et al. Treatment-Free Remission After Second-Line Nilotinib Treatment in Patients with Chronic Myeloid Leukemia in Chronic Phase: Results from a Single-Group, Phase 2, Open-Label Study. Ann. Intern. Med. 2018, 168, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.M.; Branford, S.; Seymour, J.F.; Schwarer, A.P.; Arthur, C.; Yeung, D.T.; Dang, P.; Goyne, J.M.; Slader, C.; Filshie, R.J.; et al. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal residual disease: Results from the TWISTER study. Blood 2013, 122, 515–522. [Google Scholar] [CrossRef]
- Rousselot, P.; Charbonnier, A.; Cony-Makhoul, P.; Agape, P.; Nicolini, F.E.; Varet, B.; Gardembas, M.; Etienne, G.; Réa, D.; Roy, L.; et al. Loss of major molecular response as a trigger for restarting tyrosine kinase inhibitor therapy in patients with chronic-phase chronic myelogenous leukemia who have stopped imatinib after durable undetectable disease. J. Clin. Oncol. 2014, 32, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Saussele, S.; Richter, J.; Guilhot, J.; Gruber, F.X.; Hjorth-Hansen, H.; Almeida, A.; Janssen, J.; Mayer, J.; Koskenvesa, P.; Panayiotidis, P.; et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): A prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018, 19, 747–757. [Google Scholar] [CrossRef]
- Fujisawa, S.; Ueda, Y.; Usuki, K.; Kobayashi, H.; Kondo, E.; Doki, N.; Nakao, T.; Kanda, Y.; Kosugi, N.; Kosugi, H.; et al. Feasibility of the imatinib stop study in the Japanese clinical setting: Delightedly overcome CML expert stop TKI trial (DOMEST Trial). Int. J. Clin. Oncol. 2019, 24, 445–453. [Google Scholar] [CrossRef]
- Kimura, S.; Imagawa, J.; Murai, K.; Hino, M.; Kitawaki, T.; Okada, M.; Tanaka, H.; Shindo, M.; Kumagai, T.; Ikezoe, T.; et al. Treatment-free remission after first-line dasatinib discontinuation in patients with chronic myeloid leukaemia (first-line DADI trial): A single-arm, multicentre, phase 2 trial. Lancet Haematol. 2020, 7, e218–e225. [Google Scholar] [CrossRef]
- Mori, S.; Vagge, E.; le Coutre, P.; Abruzzese, E.; Martino, B.; Pungolino, E.; Elena, C.; Pierri, I.; Assouline, S.; D’Emilio, A.; et al. Age and dPCR can predict relapse in CML patients who discontinued imatinib: The ISAV study. Am. J. Hematol. 2015, 90, 910–914. [Google Scholar] [CrossRef]
- Okada, M.; Imagawa, J.; Tanaka, H.; Nakamae, H.; Hino, M.; Murai, K.; Ishida, Y.; Kumagai, T.; Sato, S.; Ohashi, K.; et al. Final 3-year Results of the Dasatinib Discontinuation Trial in Patients With Chronic Myeloid Leukemia Who Received Dasatinib as a Second-line Treatment. Clin. Lymphoma Myeloma Leuk. 2018, 18, 353–360.e351. [Google Scholar] [CrossRef]
- Hochhaus, A.; Masszi, T.; Giles, F.J.; Radich, J.P.; Ross, D.M.; Gómez Casares, M.T.; Hellmann, A.; Stentoft, J.; Conneally, E.; García-Gutiérrez, V.; et al. Treatment-free remission following frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: Results from the ENESTfreedom study. Leukemia 2017, 31, 1525–1531. [Google Scholar] [CrossRef]
- Imagawa, J.; Tanaka, H.; Okada, M.; Nakamae, H.; Hino, M.; Murai, K.; Ishida, Y.; Kumagai, T.; Sato, S.; Ohashi, K.; et al. Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicentre phase 2 trial. Lancet Haematol. 2015, 2, e528–e535. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, T.; Nakaseko, C.; Nishiwaki, K.; Yoshida, C.; Ohashi, K.; Takezako, N.; Takano, H.; Kouzai, Y.; Murase, T.; Matsue, K.; et al. Dasatinib cessation after deep molecular response exceeding 2 years and natural killer cell transition during dasatinib consolidation. Cancer Sci. 2018, 109, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Rea, D.; Nicolini, F.E.; Tulliez, M.; Guilhot, F.; Guilhot, J.; Guerci-Bresler, A.; Gardembas, M.; Coiteux, V.; Guillerm, G.; Legros, L.; et al. Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood 2017, 129, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.M.; Masszi, T.; Gómez Casares, M.T.; Hellmann, A.; Stentoft, J.; Conneally, E.; Garcia-Gutierrez, V.; Gattermann, N.; le Coutre, P.D.; Martino, B.; et al. Durable treatment-free remission in patients with chronic myeloid leukemia in chronic phase following frontline nilotinib: 96-week update of the ENESTfreedom study. J. Cancer Res. Clin. Oncol. 2018, 144, 945–954. [Google Scholar] [CrossRef]
- Shah, N.P.; García-Gutiérrez, V.; Jiménez-Velasco, A.; Larson, S.; Saussele, S.; Rea, D.; Mahon, F.X.; Levy, M.Y.; Gómez-Casares, M.T.; Pane, F.; et al. Dasatinib discontinuation in patients with chronic-phase chronic myeloid leukemia and stable deep molecular response: The DASFREE study. Leuk. Lymphoma 2020, 61, 650–659. [Google Scholar] [CrossRef]
- Campiotti, L.; Suter, M.B.; Guasti, L.; Piazza, R.; Gambacorti-Passerini, C.; Grandi, A.M.; Squizzato, A. Imatinib discontinuation in chronic myeloid leukaemia patients with undetectable BCR-ABL transcript level: A systematic review and a meta-analysis. Eur. J. Cancer 2017, 77, 48–56. [Google Scholar] [CrossRef]
- Chen, K.K.; Du, T.F.; Xiong, P.S.; Fan, G.H.; Yang, W. Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia with Losing Major Molecular Response as a Definition for Molecular Relapse: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 372. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef]
- Breccia, M.; Abruzzese, E.; Stagno, F.; Iurlo, A.; Pene, F.; Attolica, I.; Sportoletti, P.; Pregno, P.; Galimberti, S.; Scappini, B.; et al. First Interim Analysis of the Italian Dante Study: De-Escalation before Treatment-Free Remission in Patients with Chronic Myeloid Leukemia Treated with First-Line Nilotinib. Blood 2021, 138, 1474. [Google Scholar] [CrossRef]
- Clark, R.E.; Polydoros, F.; Apperley, J.F.; Milojkovic, D.; Rothwell, K.; Pocock, C.; Byrne, J.; de Lavallade, H.; Osborne, W.; Robinson, L.; et al. De-escalation of tyrosine kinase inhibitor therapy before complete treatment discontinuation in patients with chronic myeloid leukaemia (DESTINY): A non-randomised, phase 2 trial. Lancet Haematol. 2019, 6, e375–e383. [Google Scholar] [CrossRef]
- Iurlo, A.; Breccia, M.; Stagno, F.; Abruzzese, E.; Pane, F.; Attolico, I.; Sportoletti, P.; Cerrano, M.; Galimberti, S.; Scappini, B.; et al. Full Treatment-Free Remission Outcome in Patients with Chronic Myeloid Leukemia in Chronic Phase Following One Year of Nilotinib De-Escalation: 96-Week Update of Dante Study. Blood 2023, 142, 4534. [Google Scholar] [CrossRef]
- Gener-Ricos, G.; Haddad, F.G.; Sasaki, K.; Issa, G.C.; Skinner, J.; Masarova, L.; Borthakur, G.; Alvarado, Y.; Garcia-Manero, G.; Jabbour, E.; et al. Low-Dose Dasatinib (50 mg Daily) Frontline Therapy in Newly Diagnosed Chronic Phase Chronic Myeloid Leukemia: 5-Year Follow-up Results. Clin. Lymphoma Myeloma Leuk. 2023, 23, 742–748. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | TFR Cohort (N = 39) | Full Cohort (N = 233) | ||
|---|---|---|---|---|
| Age in Years (Median) | 47 | Range: 20 y–65 y | 54 | Range: 20 y–72 y |
| Gender (%) | ||||
| Female | 69 | 63 | ||
| Race (%) | ||||
| Caucasian | 76 | 72 | ||
| African American | 20 | 26 | ||
| Asian | 4 | 2 | ||
| Vital Status (%) | ||||
| Alive | 89 | 81 | ||
| Deceased | 11 | 11 | ||
| Lost to Follow-up | 0 | 8 | ||
| Standard-Dose Abrupt Stop (N = 21) | Standard-Dose Tapering (N = 11) | Upfront Dose Reduction (N = 7) | ||||
|---|---|---|---|---|---|---|
| Age in Years (Median) | 47 | Range: 20–65 y | 58 | Range: 26–61 y | 46 | Range: 28–61 y |
| Gender (%) | ||||||
| Female | 65 | 73 | 71 | |||
| Race (%) | ||||||
| Caucasian | 73 | 71 | ||||
| African | 65 | 9 | 29 | |||
| American | 20 | |||||
| Asian | 10 | |||||
| TKI prior to TFR (%) | ||||||
| Imatinib | 48 | 10 | 29 | |||
| Dasatinib | 33 | 45 | 71 | |||
| Nilotinib | 19 | 45 | ||||
| CML Related Death (%) | ||||||
| No | 95 | 91 | 100 | |||
| Lost to Follow-up | 5 | 9 | ||||
| Total CML-CP Patients Receiving and/or Eligible for TFR (N = 56) | |
|---|---|
| Number Eligible (NCCN and/or ELN) | N = 46 |
| NCCN Criteria (%) | 100 (N = 46) |
| ELN Criteria (%) | 96 (N = 44) |
| Unknown (%) | 4 (N = 2) |
| TFR Eligible and Not Attempted (%) | 30 (N = 17) |
| TFR Attempted | 70 (N = 39) |
| Eligible and Attempted (%) | 74 (N = 29) |
| Ineligible ant Attempted (%) | 21 (N = 8) |
| Unknown Eligibility and Attempted (%) | 5 (N = 2) |
| Time from Diagnosis to TFR Attempt (Months) | Median = 83 (8–257) |
| Total Duration on TKI Prior to TFR (Months) | Median = 87 (23–220) |
| Duration of Deep Response Prior to TFR (Months) | Median = 58 (0–153) |
| MMR Before TFR (%) | |
| MR4 | 16 |
| MR4.5 | 84 |
| Number of TKIs before TFR (%) | |
| 1 | 82 |
| 2 | 13 |
| 3 | 5 |
| Prior Therapy | Median TFR Duration (m) | Median Time to Lose TFR (m) | TFR Lost 0–6 m | TFR Lost 6–12 m | TFR Lost 1–2 y | TFR Lost >2 y | MMR Reobtained | MR4.5 Reobtained | Median Time to Reobtain MMR (m) | Disease Progression/CML-Related Death |
|---|---|---|---|---|---|---|---|---|---|---|
| Initial TFR for All Participants (n = 39) | 14.6 (2.0–78.0) | 5.9 (2.0–50.7) | 55.00% | 16.00% | 8.00% | 21.00% | 100.00% | 100.00% | 3.1 (0.6–8.4) | 0.00% |
| Standard-Dose Abrupt Cessation (n = 21) | 25.7 (2.9–78.0) | 8.1 (2.6–34.3) | 50.00% | 16.67% | 0.00% | 33.33% | 100.00% | 100.00% | 3.7 (0.8–8.4) | 0.00% |
| Imatinib (n = 10) | 30.3 (3.2–78.0) | 25.1 (2.6–31.7) | 40% | 0.00% | 0.00% | 60% | 100.00% | 100.00% | 5.1 (0.8–6.6) | 0.00% |
| Dasatinib (n = 7) | 9.8 (2.9–45.6) | 7.4 (4.3–13.6) | 100.00% | 0.00% | 0.00% | 0.00% | 100.00% | 100.00% | 3.40 (2.9–5.1) | 0.00% |
| Nilotinib (n = 4) | 9.7 (3.0–39.1) | 5.5 (2.8–8.2) | 50.00% | 50.00% | 0.00% | 0.00% | 100.00% | 100.00% | 3.0 (2.1–4.9) | 0.00% |
| Standard-Dose Taper (n = 11) | 12.9 (2.7–61.6) | 13.6 (2.7–50.7) | 25.00% | 25.00% | 25.00% | 25.00% | 100.00% | 100.00% | 1.2 (0.6–2.8) | 0.00% |
| Imatinib (n = 1) | 11.3 (8.9–25.9) | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | 0.00% |
| Dasatinib (n = 5) | 25.6 (11.2–54.0) | 10.6 (8.5–18.5) | N/A | 40% | 20% | 40% | 100.00% | 100.00% | 1.2 (0.8–4.1) | 0.00% |
| Nilotinib (n = 5) | 13.8 (2.73–61.6) | 9.7 (2.7–16.7) | 60.00% | 0.00% | 40.00% | 0.00% | 100.00% | 100.00% | 1.7 (0.6–2.8) | 0.00% |
| Upfront Dose Reduction (n = 7) | 7.3 (2.0–51.6) | 3.4 (2.0–5.7) | 100% | 0.00% | 0.00% | 0.00% | 100.00% | 100.00% | 4.3 (2.5–7.5) | 0.00% |
| Imatinib (n = 2) | 4.0 (2.8–5.1) | 2.83 (2.5–3.3) | 100% | N/A | N/A | N/A | 100.00% | 100.00% | 4.7 (4.3–5.1) | 0.00% |
| Dasatinib (n = 5) | 19.0 (2.0–51.6) | 5.11 (4.5–20.2) | 100% | 0.00% | 0.00% | 0.00% | 100.00% | 100.00% | 2.2 (1.5–6.9) | 0.00% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bourne, G.; Diebold, K.; Bascug, G.; Knapp, J.; Espinoza-Gutarra, M.; Vachhani, P.; Bachiashvili, K.; Rangaraju, S.; Mohty, R.; Bhatia, R.; et al. Real-World Evidence of Treatment-Free Remission Strategies and Outcomes in Chronic Myeloid Leukemia. Cancers 2025, 17, 2148. https://doi.org/10.3390/cancers17132148
Bourne G, Diebold K, Bascug G, Knapp J, Espinoza-Gutarra M, Vachhani P, Bachiashvili K, Rangaraju S, Mohty R, Bhatia R, et al. Real-World Evidence of Treatment-Free Remission Strategies and Outcomes in Chronic Myeloid Leukemia. Cancers. 2025; 17(13):2148. https://doi.org/10.3390/cancers17132148
Chicago/Turabian StyleBourne, Garrett, Kendall Diebold, Greg Bascug, Joshua Knapp, Manuel Espinoza-Gutarra, Pankit Vachhani, Kimo Bachiashvili, Sravanti Rangaraju, Razan Mohty, Ravi Bhatia, and et al. 2025. "Real-World Evidence of Treatment-Free Remission Strategies and Outcomes in Chronic Myeloid Leukemia" Cancers 17, no. 13: 2148. https://doi.org/10.3390/cancers17132148
APA StyleBourne, G., Diebold, K., Bascug, G., Knapp, J., Espinoza-Gutarra, M., Vachhani, P., Bachiashvili, K., Rangaraju, S., Mohty, R., Bhatia, R., & Jamy, O. (2025). Real-World Evidence of Treatment-Free Remission Strategies and Outcomes in Chronic Myeloid Leukemia. Cancers, 17(13), 2148. https://doi.org/10.3390/cancers17132148