
High-Risk Early-Stage Endometrial Cancer: Role of Adjuvant Therapy and Prognostic Factors Affecting Survival



Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
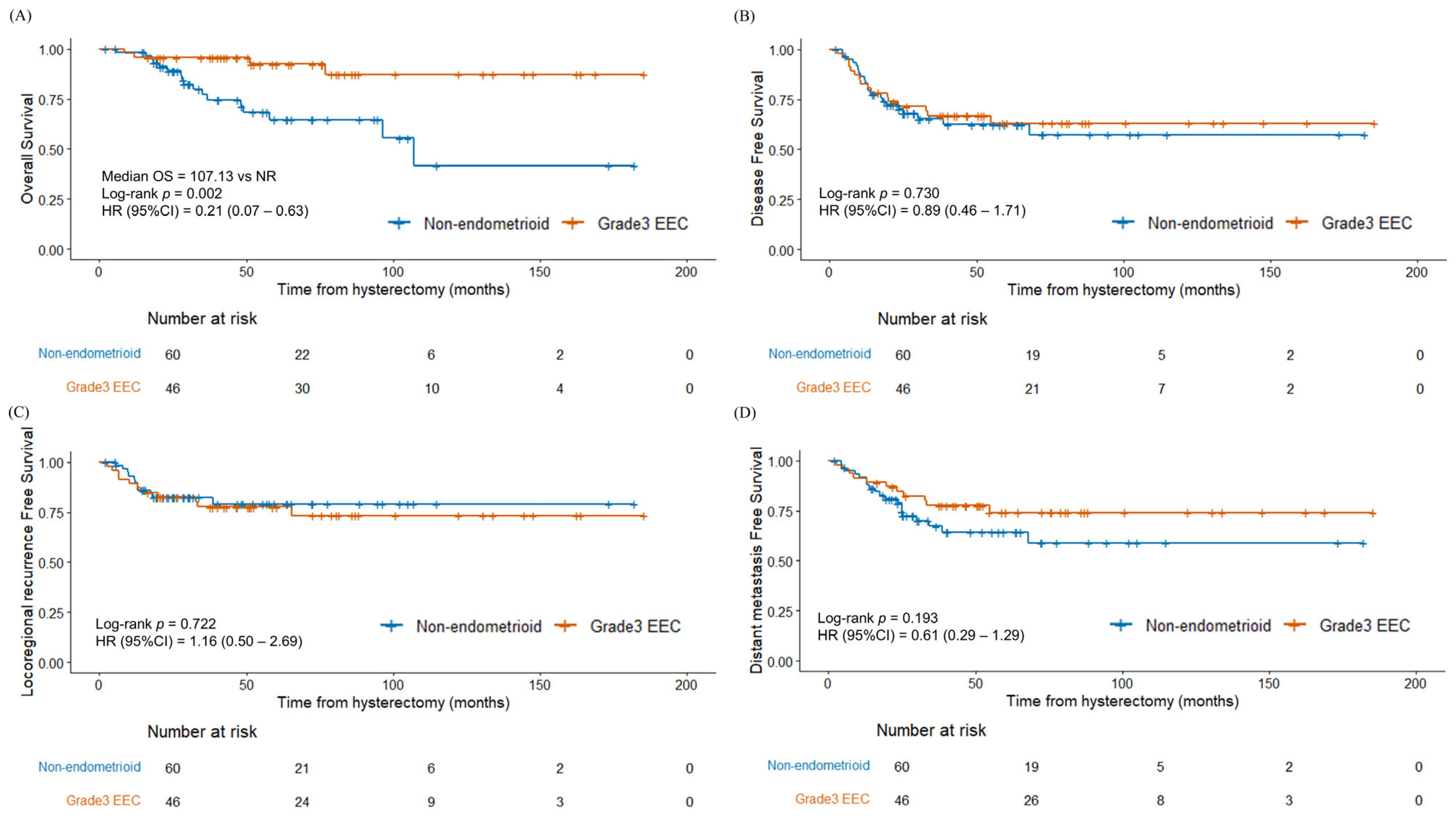
4.1. Survival Outcomes and Histological Subtypes
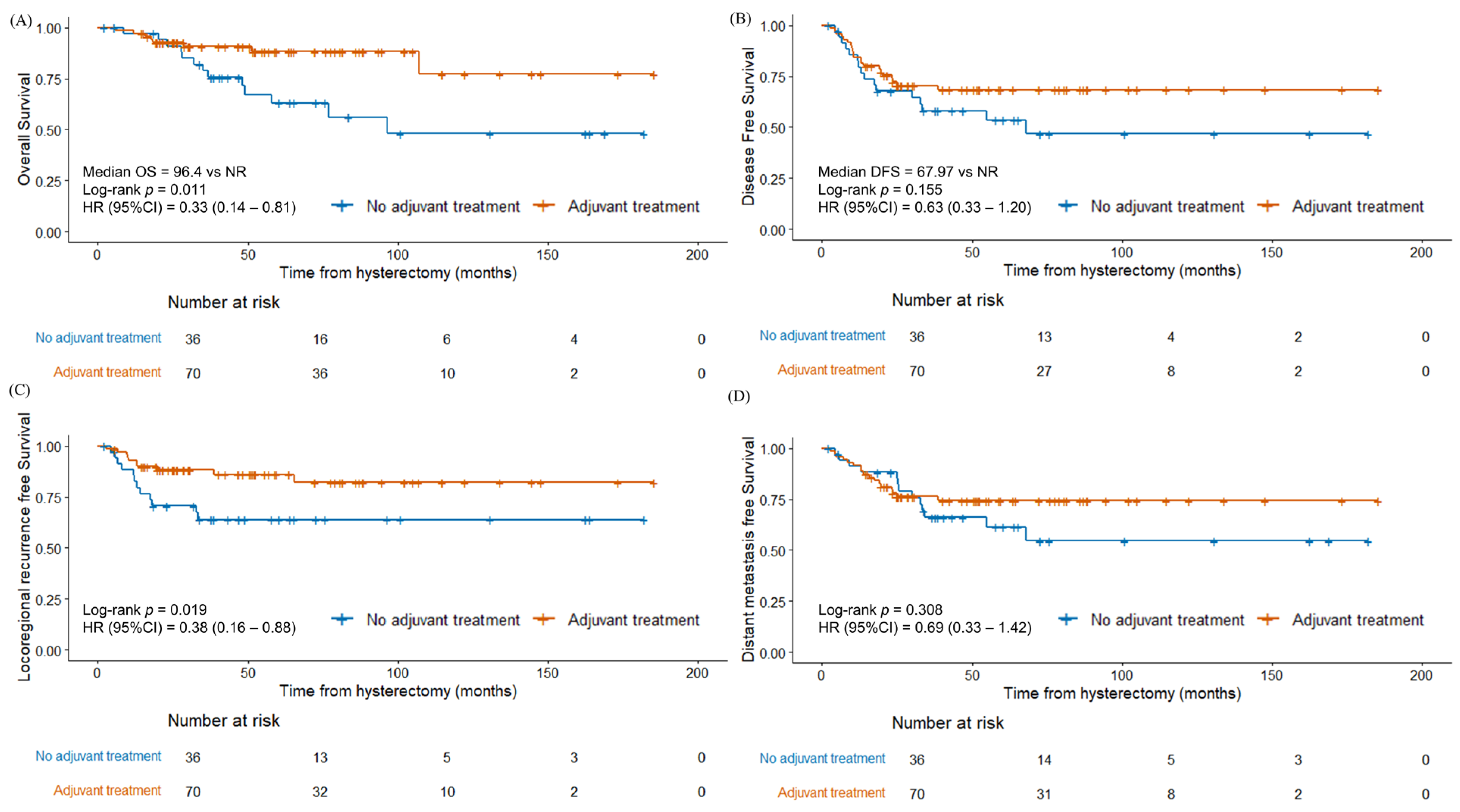
4.2. Role of Adjuvant Therapy and Prognostic Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OS | Overall Survival |
| FIGO | International Federation of Gynecology and Obstetrics |
| RT | Radiotherapy |
| EBRT | External beam radiation therapy |
| ICR | Intracavitary radiation |
| DFS | Disease-free survival |
| LRRFS | Locoregional recurrence-free survival |
| DMFS | Distant metastasis-free survival |
| PLND | Pelvic lymph node dissection |
| DOI | Depth of invasion |
| BMI | Body mass index |
| SLN | Sentinel lymph node |
References
- Singh, S.; Raidoo, S.; Pettigrew, G.; Debernardo, R. Management of early stage, high-risk endometrial carcinoma: Preoperative and surgical considerations. Obstet. Gynecol. Int. 2013, 2013, 757249. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Devesa, S.S.; Harvey, S.V.; Wentzensen, N. Hysterectomy-Corrected Uterine Corpus Cancer Incidence Trends and Differences in Relative Survival Reveal Racial Disparities and Rising Rates of Nonendometrioid Cancers. J. Clin. Oncol. 2019, 37, 1895–1908. [Google Scholar] [CrossRef]
- Berek, J.S.; Matias-Guiu, X.; Creutzberg, C.; Fotopoulou, C.; Gaffney, D.; Kehoe, S.; Lindemann, K.; Mutch, D.; Concin, N. FIGO staging of endometrial cancer: 2023. Int. J. Gynaecol. Obstet. 2023, 162, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Restaino, S.; Paglietti, C.; Arcieri, M.; Biasioli, A.; Della Martina, M.; Mariuzzi, L.; Andreetta, C.; Titone, F.; Bogani, G.; Raimondo, D.; et al. Management of Patients Diagnosed with Endometrial Cancer: Comparison of Guidelines. Cancers 2023, 15, 1091. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef]
- Lee, S.J.; Kang, H.J.; Kwak, Y.K.; Kim, M.; Kim, J. Non-endometrioid endometrial cancer: Analysis of recurrence pattern and identification of prognostic and treatment factors affecting recurrence and survival. Strahlenther. Onkol. 2023, 199, 828–837. [Google Scholar] [CrossRef]
- Klopp, A.; Smith, B.D.; Alektiar, K.; Cabrera, A.; Damato, A.L.; Erickson, B.; Fleming, G.; Gaffney, D.; Greven, K.; Lu, K.; et al. The role of postoperative radiation therapy for endometrial cancer: Executive summary of an American Society for Radiation Oncology evidence-based guideline. Pract. Radiat. Oncol. 2014, 4, 137–144. [Google Scholar] [CrossRef]
- Small, W., Jr.; Beriwal, S.; Demanes, D.J.; Dusenbery, K.E.; Eifel, P.; Erickson, B.; Jones, E.; Rownd, J.J.; De Los Santos, J.F.; Viswanathan, A.N.; et al. American Brachytherapy Society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy. Brachytherapy 2012, 11, 58–67. [Google Scholar] [CrossRef]
- Hamilton, C.A.; Cheung, M.K.; Osann, K.; Chen, L.; Teng, N.N.; Longacre, T.A.; Powell, M.A.; Hendrickson, M.R.; Kapp, D.S.; Chan, J.K. Uterine papillary serous and clear cell carcinomas predict for poorer survival compared to grade 3 endometrioid corpus cancers. Br. J. Cancer 2006, 94, 642–646. [Google Scholar] [CrossRef]
- Desai, N.B.; Kollmeier, M.A.; Makker, V.; Levine, D.A.; Abu-Rustum, N.R.; Alektiar, K.M. Comparison of outcomes in early stage uterine carcinosarcoma and uterine serous carcinoma. Gynecol. Oncol. 2014, 135, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Callister, M.; Ramondetta, L.M.; Jhingran, A.; Burke, T.W.; Eifel, P.J. Malignant mixed Müllerian tumors of the uterus: Analysis of patterns of failure, prognostic factors, and treatment outcome. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Gunther, J.R.; Christensen, E.N.; Allen, P.K.; Ramondetta, L.M.; Jhingran, A.; Fleming, N.D.; Euscher, E.D.; Lu, K.H.; Eifel, P.J.; Klopp, A.H. Role of Radiation Therapy in the Multidisciplinary Management of Uterine Carcinosarcoma. Int. J. Gynecol. Cancer 2018, 28, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Cao, D.; Zhou, H.; Wang, T.; Wang, J.; Zhang, Y.; Yu, M.; Cheng, N.; Peng, P.; Yang, J.; et al. Survival outcomes and the prognostic significance of clinicopathological features in patients with endometrial clear cell carcinoma: A 35-year single-center retrospective study. World J. Surg. Oncol. 2023, 21, 106. [Google Scholar] [CrossRef]
- Bosse, T.; Nout, R.A.; McAlpine, J.N.; McConechy, M.K.; Britton, H.; Hussein, Y.R.; Gonzalez, C.; Ganesan, R.; Steele, J.C.; Harrison, B.T.; et al. Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups. Am. J. Surg. Pathol. 2018, 42, 561–568. [Google Scholar] [CrossRef]
- León-Castillo, A.; de Boer, S.M.; Powell, M.E.; Mileshkin, L.R.; Mackay, H.J.; Leary, A.; Nijman, H.W.; Singh, N.; Pollock, P.M.; Bessette, P.; et al. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer: Impact on Prognosis and Benefit from Adjuvant Therapy. J. Clin. Oncol. 2020, 38, 3388–3397. [Google Scholar] [CrossRef]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Occhiali, T.; Poli, A.; Arcieri, M.; Driul, L.; Ditto, A.; Bogani, G.; Mariani, A.; Scambia, G.; Restaino, S.; Vizzielli, G. The exciting journey of progress: Exploring FIGO 2023 staging for endometrial cancer at a leading ESGO institution. Eur. J. Surg. Oncol. 2025, 51, 109695. [Google Scholar] [CrossRef]
- Restaino, S.; Poli, A.; Arcieri, M.; Mariuzzi, L.; Orsaria, M.; Tulisso, A.; Pellecchia, G.; Paparcura, F.; Petrillo, M.; Bogani, G.; et al. Molecular classification of endometrial carcinoma on endometrial biopsy: An early prognostic value to guide personalized treatment. Int. J. Gynecol. Cancer 2024, 34, 1211–1216. [Google Scholar] [CrossRef]
- Arcieri, M.; Vizzielli, G.; Occhiali, T.; Giorgiutti, C.; Tius, V.; Pregnolato, S.; Mariuzzi, L.; Orsaria, M.; Tulisso, A.; Damante, G.; et al. Application of novel algorithm on a retrospective series to implement the molecular classification for endometrial cancer. Eur. J. Surg. Oncol. 2024, 50, 108436. [Google Scholar] [CrossRef]
- Altman, A.D.; Ferguson, S.E.; Atenafu, E.G.; Köbel, M.; McAlpine, J.N.; Panzarella, T.; Lau, S.; Gien, L.T.; Gilks, B.; Clarke, B.; et al. Canadian high risk endometrial cancer (CHREC) consortium: Analyzing the clinical behavior of high risk endometrial cancers. Gynecol. Oncol. 2015, 139, 268–274. [Google Scholar] [CrossRef]
- Voss, M.A.; Ganesan, R.; Ludeman, L.; McCarthy, K.; Gornall, R.; Schaller, G.; Wei, W.; Sundar, S. Should grade 3 endometrioid endometrial carcinoma be considered a type 2 cancer-a clinical and pathological evaluation. Gynecol. Oncol. 2012, 124, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Nieto, K.; Adams, W.; Pham, N.; Block, A.M.; Grover, S.; Small, W., Jr.; Harkenrider, M.M. Adjuvant therapy in patients with clear cell endometrial carcinoma: An analysis of the National Cancer Database. Gynecol. Oncol. 2018, 148, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.C.; Foote, J.; Broadwater, G.; Gaillard, S.; Havrilesky, L.J.; Chino, J.P. Impact of Chemotherapy and Radiotherapy on Management of Early Stage Clear Cell and Papillary Serous Carcinoma of the Uterus. Int. J. Gynecol. Cancer 2017, 27, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; English, D.P.; Kidd, E.A. National patterns of care and cancer-specific outcomes of adjuvant treatment in patients with serous and clear cell endometrial carcinoma. Gynecol. Oncol. 2019, 152, 599–604. [Google Scholar] [CrossRef]
- Chang-Halpenny, C.N.; Natarajan, S.; Hwang-Graziano, J.M. Early-Stage Uterine Pure and Mixed Clear Cell Carcinoma: Outcomes and Recurrence with and Without Adjuvant Therapy. Am. J. Clin. Oncol. 2018, 41, 371–378. [Google Scholar] [CrossRef]
- Kim, M.; Kwon, B.S.; Chang, H.K.; Lee, S.; Chang, S.J.; Choi, J.Y.; Park, S.Y.; Lee, M.; Ryu, H.S.; Kim, Y.B. Survival outcomes of adjuvant radiotherapy and chemotherapy in women with stage I serous papillary and clear cell carcinoma of the endometrium: A Korean multicenter study. J. Gynecol. Oncol. 2019, 30, e44. [Google Scholar] [CrossRef]
- Åkesson, Å.; Adok, C.; Dahm-Kähler, P. Increased survival in non-endometrioid endometrial cancer after introducing lymphadenectomy and tailoring radiotherapy—A population-based cohort study. Eur. J. Cancer 2022, 169, 54–63. [Google Scholar] [CrossRef]
- Cuccu, I.; Raspagliesi, F.; Malzoni, M.; Vizza, E.; Papadia, A.; Di Donato, V.; Giannini, A.; De Iaco, P.; Perrone, A.M.; Plotti, F.; et al. Sentinel node mapping in high-intermediate and high-risk endometrial cancer: Analysis of 5-year oncologic outcomes. Eur. J. Surg. Oncol. 2024, 50, 108018. [Google Scholar] [CrossRef]
- Restaino, S.; Buda, A.; Puppo, A.; Capozzi, V.A.; Sozzi, G.; Casarin, J.; Gallitelli, V.; Murgia, F.; Vizzielli, G.; Baroni, A.; et al. Anatomical distribution of sentinel lymph nodes in patients with endometrial cancer: A multicenter study. Int. J. Gynecol. Cancer 2022, 32, 517–524. [Google Scholar] [CrossRef]
- Pinelli, C.; Artuso, V.; Bogani, G.; Laganà, A.S.; Ghezzi, F.; Casarin, J. Lymph node evaluation in endometrial cancer: How did it change over the last two decades? Transl. Cancer Res. 2020, 9, 7778–7784. [Google Scholar] [CrossRef] [PubMed]
- Soliman, P.T.; Westin, S.N.; Dioun, S.; Sun, C.C.; Euscher, E.; Munsell, M.F.; Fleming, N.D.; Levenback, C.; Frumovitz, M.; Ramirez, P.T.; et al. A prospective validation study of sentinel lymph node mapping for high-risk endometrial cancer. Gynecol. Oncol. 2017, 146, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Todo, Y.; Kato, H.; Kaneuchi, M.; Watari, H.; Takeda, M.; Sakuragi, N. Survival effect of para-aortic lymphadenectomy in endometrial cancer (SEPAL study): A retrospective cohort analysis. Lancet 2010, 375, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Dane, C.; Bakir, S. The effect of myometrial invasion on prognostic factors and survival analysis in endometrial carcinoma. Afr. Health Sci. 2019, 19, 3235–3241. [Google Scholar] [CrossRef]
- Wolfson, A.H.; Sightler, S.E.; Markoe, A.M.; Schwade, J.G.; Averette, H.E.; Ganjei, P.; Hilsenbeck, S.G. The prognostic significance of surgical staging for carcinoma of the endometrium. Gynecol. Oncol. 1992, 45, 142–146. [Google Scholar] [CrossRef]
- Frei, K.A.; Kinkel, K.; Bonél, H.M.; Lu, Y.; Zaloudek, C.; Hricak, H. Prediction of deep myometrial invasion in patients with endometrial cancer: Clinical utility of contrast-enhanced MR imaging-a meta-analysis and Bayesian analysis. Radiology 2000, 216, 444–449. [Google Scholar] [CrossRef]
- Lee, K.B.; Ki, K.D.; Lee, J.M.; Lee, J.K.; Kim, J.W.; Cho, C.H.; Kim, S.M.; Park, S.Y.; Jeong, D.H.; Kim, K.T. The risk of lymph node metastasis based on myometrial invasion and tumor grade in endometrioid uterine cancers: A multicenter, retrospective Korean study. Ann. Surg. Oncol. 2009, 16, 2882–2887. [Google Scholar] [CrossRef]
- Jeans, E.B.; Breen, W.G.; Mullikin, T.C.; Looker, B.A.; Mariani, A.; Keeney, G.L.; Haddock, M.G.; Petersen, I.A. Adjuvant brachytherapy for FIGO stage I serous or clear cell endometrial cancer. Int. J. Gynecol. Cancer 2021, 31, 859–867. [Google Scholar] [CrossRef]
- Dallaire Nantel, L.; Renaud, M.C.; Gregoire, J.; Sebastianelli, A.; Plante, M. High-grade endometrial carcinoma limited to the endometrium or a polyp: Is adjuvant treatment necessary? Int. J. Gynecol. Cancer 2021, 31, 1335–1340. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Total (n = 106) | NEEC (n = 60) | G3 EEC (n = 46) | p-Value | ||
|---|---|---|---|---|---|---|
| BMI (median, range) | 23.3 (17.0–37.7) | 23.7 (19.2–31.5) | 22.4 (17–37.7) | 0.126 | ||
| Age | ||||||
| <60 years | 46 (43.4%) | 17 (28.3%) | 29 (63.0%) | <0.001 | ||
| ≥60 years | 60 (56.6%) | 43 (71.7%) | 17 (37.0%) | |||
| Hypertension | 31 (29.2%) | 22 (36.7%) | 9 (19.6%) | 0.084 | ||
| Diabetes | 10 (9.4%) | 7 (11.7%) | 3 (6.5%) | 0.508 | ||
| History of breast cancer | 13 (12.3%) | 10 (16.7%) | 3 (6.5%) | 0.143 | ||
| Histologic type | ||||||
| Serous carcinoma | 23 (21.7%) | 23 (38.4%) | ||||
| Clear cell carcinoma | 9 (8.5%) | 9 (15%) | ||||
| Carcinosarcoma | 16 (15.1%) | 16 (26.7%) | ||||
| Undifferentiated | 3 (2.8%) | 3 (5%) | ||||
| Mixed | 9 (8.5%) | 9 (15%) | ||||
| Endometrioid carcinoma | 46 (43.4%) | 46 (100%) | ||||
| FIGO stage (2018) | 0.004 | |||||
| IA | 66 (62.3%) | 43 (71.7%) | 23 (50.0%) | |||
| IB | 26 (24.5%) | 7 (11.7%) | 19 (39.1%) | |||
| II | 15 (14.2%) | 10 (17.7%) | 5 (10.9%) | |||
| Minimally invasive surgery | 73 (68.9%) | 42 (70.0%) | 31 (67.4%) | 0.834 | ||
| Peritoneal washing | 62 (58.5%) | 38 (64.4%) | 24 (55.8%) | 0.416 | ||
| Omental evaluation | 0.110 | |||||
| No | 85 (80.2%) | 46 (78.0%) | 39 (90.7%) | |||
| Omentectomy or Bx | 17 (16.7%) | 13 (22.0%) | 4 (9.3%) | |||
| SLNB | 28 (26.4%) | 17 (28.3%) | 11 (23.9%) | 0.662 | ||
| PLND | 88 (83.0%) | 45 (75.0%) | 43 (93.5%) | 0.021 | ||
| PaLND | 44 (41.5%) | 23 (38.3%) | 21 (45.7%) | 0.688 | ||
| Dissected LN ≥ 10 | 74 (69.8%) | 36 (60.0%) | 38 (82.6%) | 0.040 | ||
| Tumor size (cm, median, range) | 3.5 (0.0–8.8) | 3.5 (0–8.8) | 3.5 (0–8.4) | 0.673 | ||
| Myometrial invasion | 0.100 | |||||
| None | 14 (13.2%) | 9 (15.0%) | 5 (10.9%) | |||
| <50% | 52 (49.1%) | 32 (53.3%) | 20 (43.5%) | |||
| ≥50% | 31 (29.2%) | 13 (21.7%) | 18 (39.1%) | |||
| DOI/thick (%, median, range) | 22.8 (0.0–93.8) | 21.4 (0–92.3) | 28.6 (0–93.8) | 0.266 | ||
| LVSI | 30 (28.3%) | 13 (21.7%) | 17 (37.0%) | 0.193 | ||
| Adjuvant treatment | <0.001 | |||||
| None | 36 (34.0%) | 20 (33.3%) | 16 (34.8%) | |||
| CTx alone | 14 (13.2%) | 12 (20.0%) | 2 (4.3%) | |||
| RTx alone | 37 (34.9%) | 9 (15.0%) | 28 (60.9%) | |||
| CTx-RTx | 19 (17.9%) | 19 (31.7%) | 0 (0.0%) | |||
| CTx | <0.001 | |||||
| No | 73 (68.9%) | 29 (48.3%) | 44 (95.7%) | |||
| Yes | 33 (31.1%) | 31 (51.7%) | 2 (4.3%) | |||
| RTx | 0.199 | |||||
| No | 50 (47.2%) | 32 (53.3%) | 18 (39.1%) | |||
| Yes | 56 (52.8%) | 28 (46.7%) | 28 (60.9%) | |||
| RTx modality | 0.225 | |||||
| EBRT | 45 (43.4%) | 24 (40.0%) | 21 (45.7%) | |||
| ICR | 8 (7.6%) | 2 (3.3%) | 6 (13.0%) | |||
| EBRT + ICR | 3 (2.8%) | 2 (3.3%) | 1 (2.2%) | |||
| OS | DFS | LRRFS | DMFS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | ||
| BMI | 1.09 (0.98~1.22) | 0.104 | 1.09 (0.99~1.20) | 0.092 | 1.19 (1.06~1.34) | 0.003 | 1.06 (0.96~1.17) | 0.217 | |||||
| Age | <60 * vs. ≥60 | 2.07 (0.83~5.15) | 0.119 | 1.35 (0.70~2.61) | 0.369 | 2.39 (0.93~6.14) | 0.070 | 1.03 (0.50~2.11) | 0.939 | ||||
| Diabetes | No * vs. Yes | 2.65 (0.89~7.87) | 0.080 | 1.36 (0.48~3.85) | 0.560 | 1.85 (0.55~6.26) | 0.323 | 1.22 (0.37~4.02) | 0.747 | ||||
| Hx of breast cancer | No * vs. Yes | 1.11 (0.33~3.78) | 0.863 | 1.74 (0.76~3.97) | 0.187 | 2.12 (0.78~5.75) | 0.140 | 1.77 (0.72~4.32) | 0.213 | ||||
| FIGO (2018) | IA * vs. IB | 1.00 (0.35~2.86) | 0.993 | 1.19 (0.54~2.62) | 0.663 | 1.58 (0.62~4.02) | 0.334 | 1.13 (0.47~2.76) | 0.783 | ||||
| IA * vs. II | 1.43 (0.46~4.43) | 0.537 | 1.99 (0.88~4.52) | 0.100 | 1.04 (0.29~3.70) | 0.949 | 2.05 (0.84~4.98) | 0.114 | |||||
| Histology | NEEC * vs. G3 EEC | 0.21 (0.07~0.63) | 0.005 | 0.89 (0.46~1.71) | 0.730 | 1.17 (0.50~2.69) | 0.722 | 0.61 (0.29~1.29) | 0.198 | ||||
| Minimally invasive surgery | No * vs. Yes | 0.78 (0.32~0.33) | 0.564 | 1.27 (0.63~2.58) | 0.504 | 0.89 (0.37~2.13) | 0.794 | 1.49 (0.66~3.35) | 0.334 | ||||
| Peritoneal washing | No * vs. Yes | 2.82 (0.95~8.38) | 0.062 | 1.00 (0.51~1.97) | 0.995 | 1.01 (0.41~2.47) | 0.986 | 1.07 (0.50~2.28) | 0.865 | ||||
| Washing result | (−) * vs. (+) | 2.79 (0.89~8.77) | 0.078 | 3.50 (1.26~9.76) | 0.017 | 3.16 (0.85~11.80) | 0.087 | 3.58 (1.15~11.13) | 0.028 | ||||
| Omentectal evaluation | No * vs. Yes | 2.55 (0.92~7.12) | 0.073 | 1.70 (0.77~3.75) | 0.189 | 0.59 (0.14~2.54) | 0.476 | 2.72 (1.19~6.21) | 0.018 | ||||
| PaLND | No * vs. Yes | 0.70 (0.28~1.74) | 0.438 | 1.20 (0.62~2.30) | 0.595 | 0.60 (0.24~1.48) | 0.268 | 1.08 (0.52~2.24) | 0.840 | ||||
| Dissected nodes | <10 * vs. ≥10 | 0.16 (0.06~0.41) | <0.001 | 0.70 (0.33~1.49) | 0.353 | 0.57 (0.22~1.49) | 0.252 | 0.47 (0.21~1.04) | 0.061 | ||||
| Tumor size | 1.05 (0.84~1.32) | 0.649 | 1.02 (0.87 ~1.21) | 0.777 | 0.93 (0.74~1.17) | 0.544 | 0.96 (0.80~1.16) | 0.694 | |||||
| DOI/thick | 1.06 (1.03~1.09) | <0.001 | 1.01 (1.00~1.02) | 0.065 | 1.01 (1.00~1.03) | 0.130 | 1.01 (0.99~1.02) | 0.293 | |||||
| LVSI | No * vs. Yes | 0.81 (0.29~2.27) | 0.695 | 0.87 (0.42~1.81) | 0.715 | 1.68 (0.71~4.00) | 0.239 | 0.85 (0.38~1.93) | 0.699 | ||||
| Adjuvant treatment | No * vs. Yes | 0.34 (0.14~0.82) | 0.016 | 0.65 (0.34~1.25) | 0.197 | 0.40 (0.17~0.92) | 0.031 | 0.71 (0.34~1.46) | 0.346 | ||||
| No * vs. CTx alone | 0.52 (0.15~1.83) | 0.306 | 0.44 (0.13~1.53) | 0.198 | 0.20 (0.03~1.55) | 0.124 | 0.60 (0.17~2.10) | 0.420 | |||||
| No * vs. RTx alone | 0.23 (0.07~0.80) | 0.021 | 0.70 (0.33~1.48) | 0.351 | 0.43 (0.16~1.15) | 0.091 | 0.60 (0.25~1.44) | 0.253 | |||||
| No * vs. CTx-RTx | 0.43 (0.10~1.94) | 0.274 | 0.72 (0.28~1.84) | 0.491 | 0.48 (0.14~1.71) | 0.256 | 1.06 (0.40~2.81) | 0.902 | |||||
| CTx | No * vs. Yes | 0.98 (0.38~2.53) | 0.962 | 0.76 (0.37~1.57) | 0.457 | 0.48 (0.16~1.41) | 0.181 | 1.18 (0.55~2.52) | 0.677 | ||||
| RTx | No * vs. Yes | 0.41 (0.16~1.07) | 0.068 | 0.92 (0.48~1.76) | 0.807 | 0.68 (0.30~1.59) | 0.377 | 0.92 (0.45~1.88) | 0.814 | ||||
| OS | DFS | LRRFS | DMFS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | HR | 95% CI | p Value | ||
| BMI | 1.17 (0.95~1.45) | 0.147 | 1.09 (0.96~1.24) | 0.177 | 1.20 (1.03~1.41) | 0.021 | 1.08 (0.95~1.23) | 0.250 | |||||
| Age | <60 * vs. ≥60 | 1.39 (0.31~6.32) | 0.667 | 1.22 (0.46~3.24) | 0.691 | 2.87 (0.76~10.86) | 0.120 | 0.56 (0.17~1.82) | 0.331 | ||||
| Diabetes | No * vs. Yes | 2.57 (0.62~10.61) | 0.192 | 1.67 (0.47~5.97) | 0.429 | 1.40 (0.31~6.42) | 0.663 | 2.25 (0.52~9.66) | 0.277 | ||||
| FIGO (2018) | IA * vs. IB | 13.80 (0.65~291.57) | 0.092 | 1.12 (0.20~6.37) | 0.901 | 3.28 (0.24~45.16) | 0.375 | 1.63 (0.23~11.59) | 0.625 | ||||
| IA * vs. II | 15.60 (1.09~222.58) | 0.043 | 2.85 (0.60~13.50) | 0.188 | 3.44 (0.25~47.26) | 0.356 | 2.16 (0.36~13.08) | 0.402 | |||||
| Histology | NEEC * vs. G3 EEC | 0.21 (0.04~1.21) | 0.081 | 0.94 (0.31~2.89) | 0.920 | 2.00 (0.45~8.86) | 0.361 | 0.54 (0.13~2.18) | 0.386 | ||||
| Peritoneal washing | No * vs. Yes | 4.91 (0.79~30.58) | 0.088 | 0.90 (0.39~2.06) | 0.804 | 1.36 (0.41~4.54) | 0.614 | 0.81 (0.31~2.13) | 0.665 | ||||
| Omentectal evaluation | No * vs. Yes | 2.08 (0.57~7.59) | 0.269 | 1.86 (0.69~4.99) | 0.217 | 1.00 (0.19~5.42) | 1.000 | 2.06 (0.72~5.95) | 0.181 | ||||
| PLND | No * vs. Yes | 0.34 (0.08~1.46) | 0.146 | 1.01 (0.27~3.77) | 0.995 | 0.76 (0.13~4.48) | 0.759 | 0.44 (0.11~1.77) | 0.245 | ||||
| DOI/thick | 0.99 (0.95~1.02) | 0.484 | 1.01 (0.99~1.03) | 0.377 | 1.00 (0.97~1.04) | 0.951 | 1.00 (0.98~1.03) | 0.766 | |||||
| Adjuvant treatment | No * vs. Yes | 0.41 (0.10~1.61) | 0.202 | 0.65 (0.27~1.56) | 0.338 | 0.40 (0.12~1.29) | 0.124 | 0.70 (0.25~1.92) | 0.482 | ||||
| No * vs. CTx alone | 0.34 (0.05~2.32) | 0.270 | 0.58 (0.13~2.57) | 0.475 | 0.47 (0.05~4.82) | 0.527 | 0.85 (0.18~3.96) | 0.835 | |||||
| No * vs. RTx alone | 0.72 (0.12~4.47) | 0.722 | 0.71 (0.27~1.84) | 0.481 | 0.32 (0.08~1.29) | 0.110 | 0.66 (0.20~2.17) | 0.495 | |||||
| No * vs. CTx-RTx | 0.19 (0.02~1.80) | 0.147 | 0.54 (0.13~2.14) | 0.377 | 0.76 (0.12~4.78) | 0.770 | 0.80 (0.17~3.78) | 0.779 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.H.; Kang, J.; Lee, S.J.; Lee, K.H.; Hur, S.Y.; Kim, Y.-S. High-Risk Early-Stage Endometrial Cancer: Role of Adjuvant Therapy and Prognostic Factors Affecting Survival. Cancers 2025, 17, 2056. https://doi.org/10.3390/cancers17122056
Hong JH, Kang J, Lee SJ, Lee KH, Hur SY, Kim Y-S. High-Risk Early-Stage Endometrial Cancer: Role of Adjuvant Therapy and Prognostic Factors Affecting Survival. Cancers. 2025; 17(12):2056. https://doi.org/10.3390/cancers17122056
Chicago/Turabian StyleHong, Ji Hyun, Jun Kang, Sung Jong Lee, Keun Ho Lee, Soo Young Hur, and Yeon-Sil Kim. 2025. "High-Risk Early-Stage Endometrial Cancer: Role of Adjuvant Therapy and Prognostic Factors Affecting Survival" Cancers 17, no. 12: 2056. https://doi.org/10.3390/cancers17122056
APA StyleHong, J. H., Kang, J., Lee, S. J., Lee, K. H., Hur, S. Y., & Kim, Y.-S. (2025). High-Risk Early-Stage Endometrial Cancer: Role of Adjuvant Therapy and Prognostic Factors Affecting Survival. Cancers, 17(12), 2056. https://doi.org/10.3390/cancers17122056