
Long-Term Clinical Outcomes for Adolescent and Young-Adult Uveal Melanoma Patients Treated with Dedicated Particle-Beam Radiation †

 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Radiation Technique
2.3. Statistical Analysis
3. Results
3.1. AYA UM Proton Patient and Tumor Characteristics
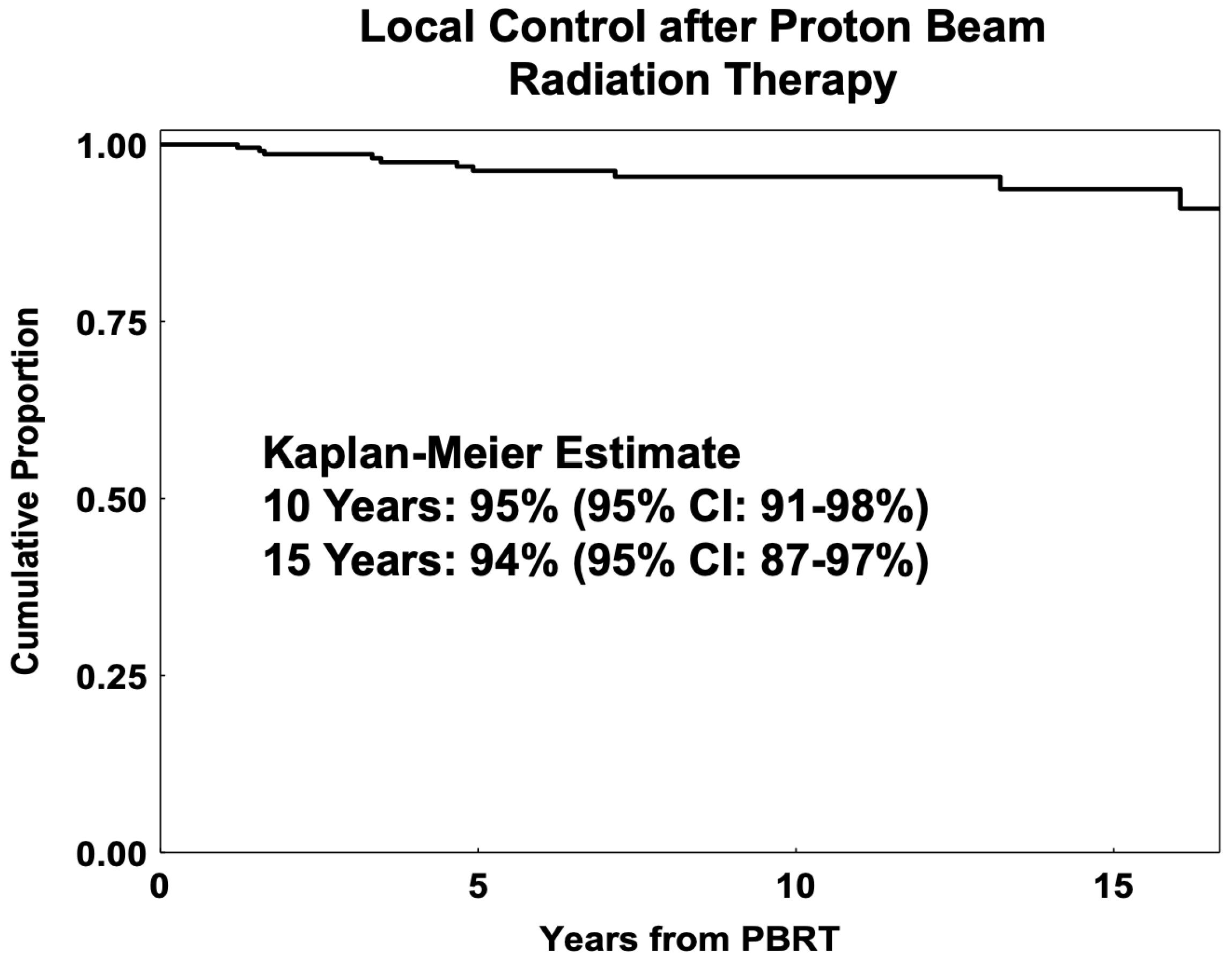
3.2. Local Control PBRT
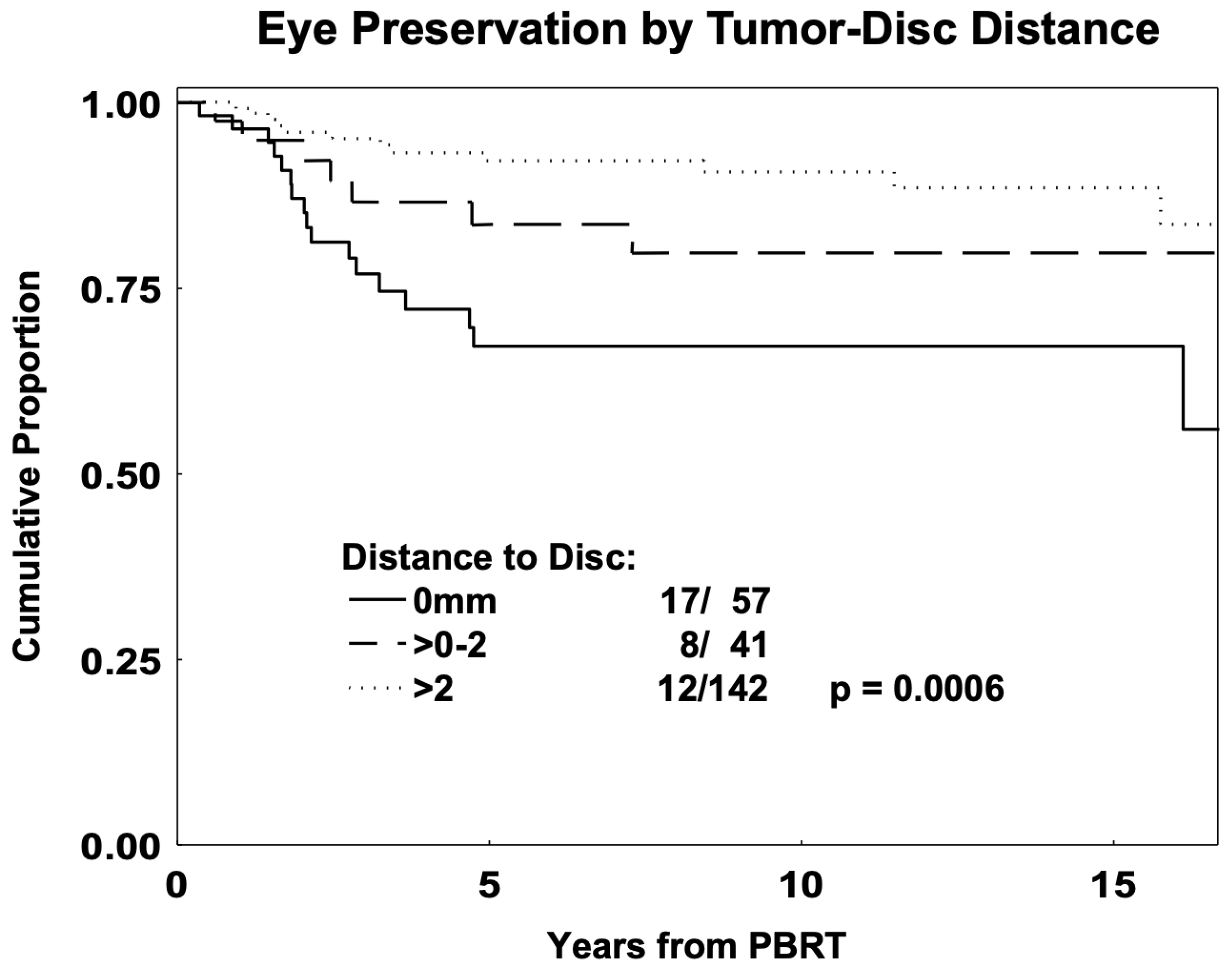
3.3. Eye Preservation in PBRT
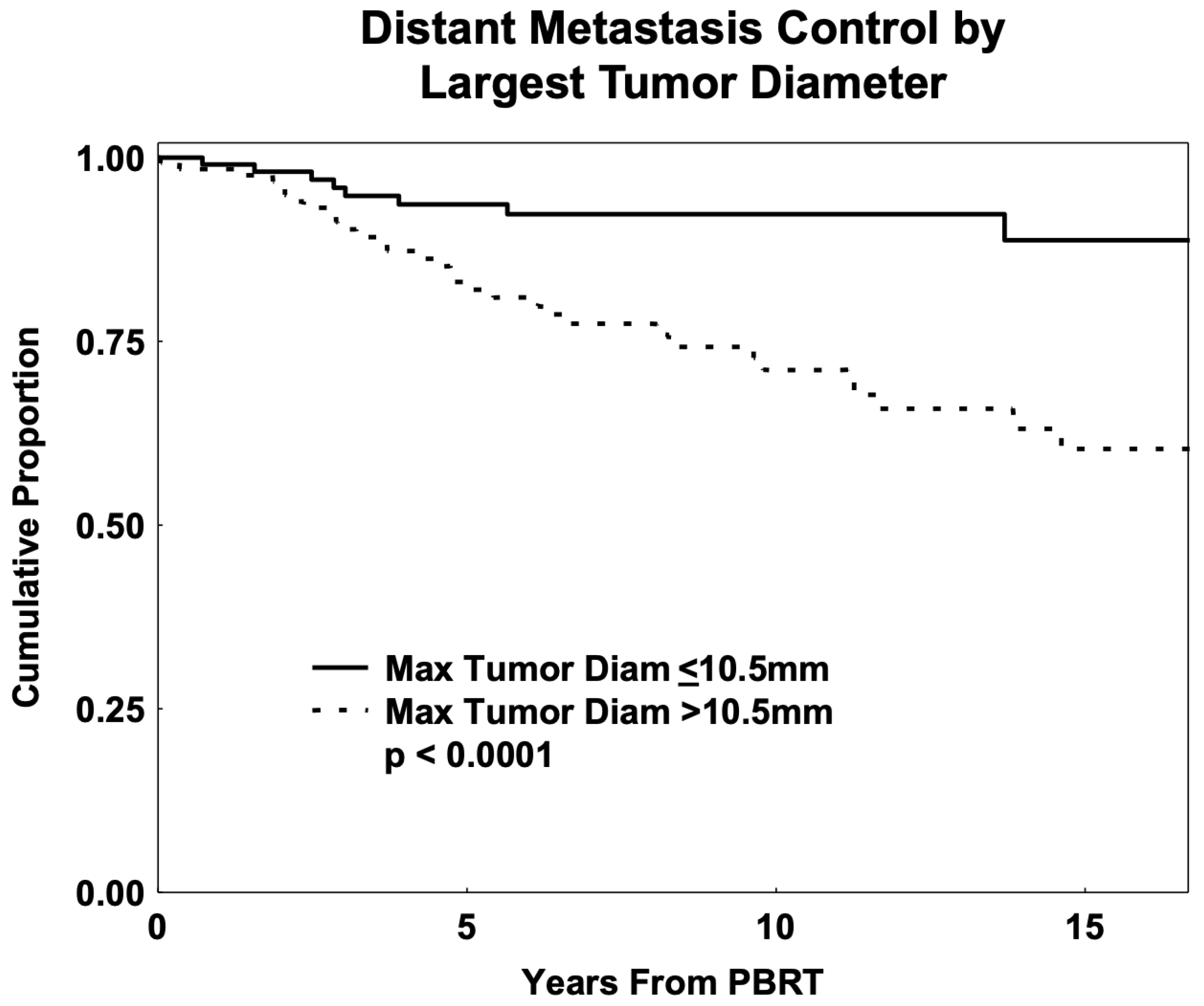
3.4. Distant Metastasis and Overall Survival
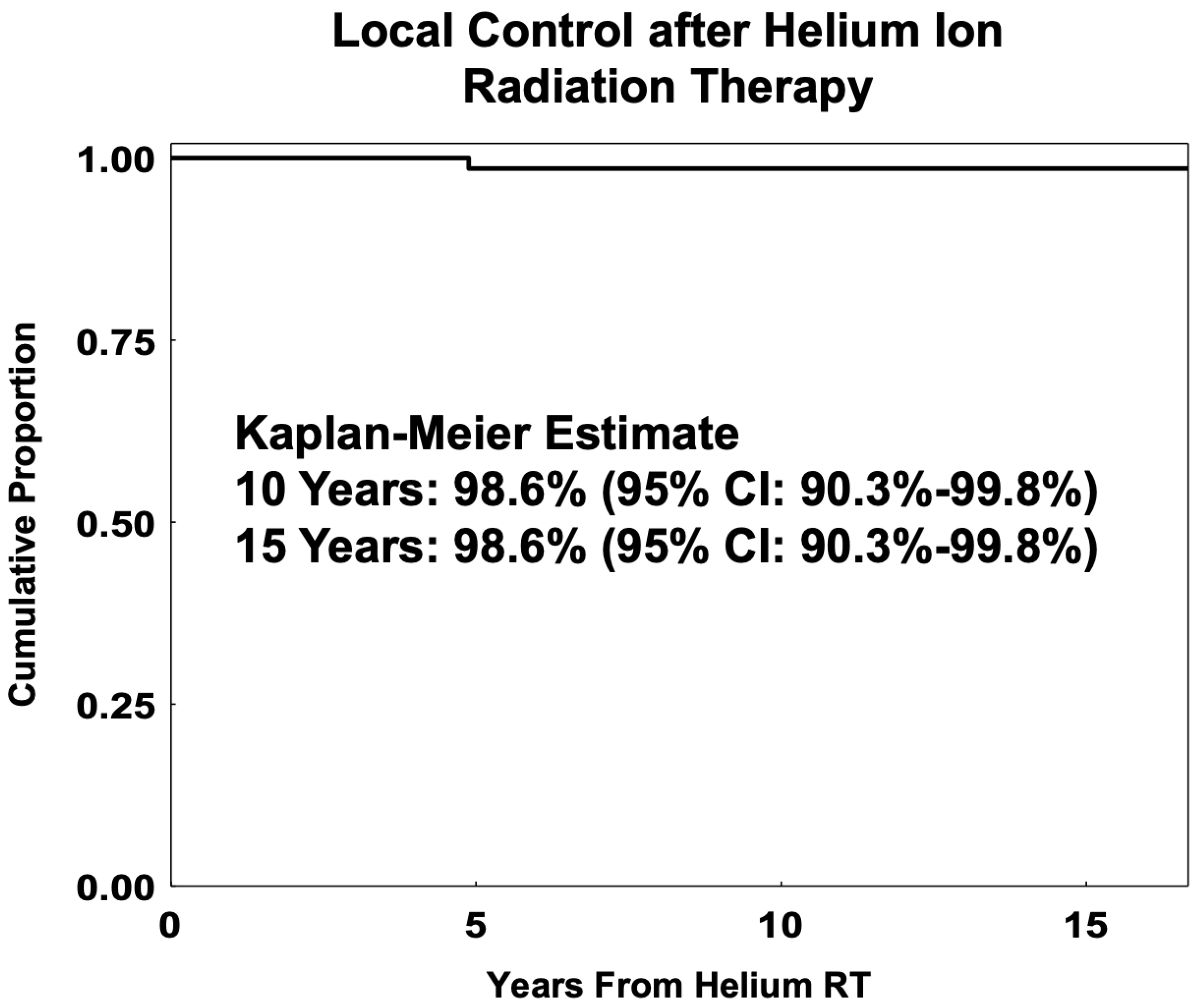
3.5. Helium-Ion RT Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| AYA | Adolescent and young-adult |
| CB | Ciliary body |
| CI | Confidence interval |
| DM | Distant metastasis |
| DVH | Dose–volume histogram |
| GEP | Gene expression profiling |
| GyE | Gray equivalent |
| HR | Hazard ratio |
| LC | Local control |
| LLR | Likelihood ratio |
| LR | Local recurrence |
| LTD | Largest tumor diameter |
| OS | Overall survival |
| PBRT | Proton-beam radiation therapy |
| RBE | Relative biological effectiveness |
| RT | Radiation therapy |
| UM | Uveal melanoma |
References
- Mishra, K.K.; Afshar, A.R.; Jessica, S.; Kacperek, A.; Damato, B.E. Ocular Malignancies. In Principles and Practice of Particle Therapy; Wiley Online Library: Hoboken, NJ, USA, 2022; Available online: https://onlinelibrary.wiley.com/doi/10.1002/9781119707530.ch14 (accessed on 7 March 2025).
- Conway, R.M.; Poothullil, A.M.; Daftari, I.K.; Weinberg, V.; Chung, J.E.; O’Brien, J.M. Estimates of Ocular and Visual Retention Following Treatment of Extra-Large Uveal Melanomas by Proton Beam Radiotherapy. Arch. Ophthalmol. 2006, 124, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, A.; Bergin, C.; Schalenbourg, A.; Goitein, G.; Zografos, L. Proton Therapy for Uveal Melanoma in 43 Juvenile Patients: Long-Term Results. Ophthalmology 2014, 121, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Rana’a, T.; Cassoux, N.; Desjardins, L.; Damato, B.; Konstantinidis, L.; Coupland, S.E.; Heimann, H.; Petrovic, A.; Zografos, L.; Schalenbourg, A.; et al. The Pediatric Choroidal and Ciliary Body Melanoma Study. Ophthalmology 2016, 123, 898–907. [Google Scholar]
- Pogrzebielski, A.; Orłowska-Heitzman, J.; Romanowska-Dixon, B. Uveal melanoma in young patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2006, 244, 1646–1649. [Google Scholar] [CrossRef]
- Fry, M.V.; Augsburger, J.J.; Hall, J.; Corrêa, Z.M. Posterior uveal melanoma in adolescents and children: Current perspectives. Clin. Ophthalmol. 2018, 12, 2205–2212. [Google Scholar] [CrossRef] [PubMed]
- Nisanova, A.; Park, S.S.; Amin, A.; Zako, C.; Wilson, M.D.; Scholey, J.; Afshar, A.R.; Tsai, T.; Char, D.H.; Mishra, K.K. Novel risk factors for uveal melanoma in adolescent and young adult patients: A comprehensive case-control analysis. Ophthalmol. Sci. 2024, 5, 100687. [Google Scholar] [CrossRef]
- Kornblau, I.; King, B.A.; CERNICHIARO-ESPINOSA, L.A.A.; Wilson, M.W. Clinical characteristics and outcomes in young patients with uveal melanoma from the mid-south United States. Invest. Ophthalmol. Vis. Sci. 2023, 64, 898. [Google Scholar]
- Mishra, K.K.; Quivey, J.M.; Daftari, I.K.; Char, D.H. 64. Uveal Melanoma. In Leibel and Phillips Textbook of Radiation Oncology, 3rd ed.; Hoppe, R.T., Phillips, T.L., Roach, M., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2010; pp. 1400–1421. [Google Scholar] [CrossRef]
- Shields, C.L.; Kaliki, S.; Furuta, M.; Mashayekhi, A.; Shields, J.A. CLINICAL SPECTRUM AND PROGNOSIS OF UVEAL MELANOMA BASED ON AGE AT PRESENTATION IN 8,033 CASES. RETINA 2012, 32, 1363. [Google Scholar] [CrossRef]
- Pica, A.; Weber, D.C.; Schweizer, C.; Chaouch, A.; Zografos, L.; Schalenbourg, A. Clinical Outcomes in AYAs (Adolescents and Young Adults) Treated with Proton Therapy for Uveal Melanoma: A Comparative Matching Study with Elder Adults. Cancers 2023, 15, 4652. [Google Scholar] [CrossRef]
- Fry, M.V.; Augsburger, J.J.; Corrêa, Z.M. Clinical Features, Metastasis, and Survival in Patients Younger Than 21 Years With Posterior Uveal Melanoma. JAMA Ophthalmol. 2019, 137, 75–81. [Google Scholar] [CrossRef]
- Vavvas, D.; Kim, I.; Lane, A.M.; Chaglassian, A.; Mukai, S.; Gragoudas, E. Posterior Uveal Melanoma in Young Patients Treated with Proton Beam Therapy. RETINA 2010, 30, 1267. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Topham, A. Incidence of uveal melanoma in the United States: 1973–1997. Ophthalmology 2003, 110, 956–961. [Google Scholar] [CrossRef]
- Aubin, S.; Barr, R.; Rogers, P.; Schacter, B.; Bielack, S.S.; Ferrari, A.; Manchester, R.A.; McMaster, K.; Morgan, S.; Patterson, M. What Should the Age Range Be for AYA Oncology? J. Adolesc. Young Adult Oncol. 2011, 1, 3–10. [Google Scholar] [CrossRef]
- Bhatia, S.; Pappo, A.S.; Acquazzino, M.; Allen-Rhoades, W.A.; Barnett, M.; Borinstein, S.C.; Casey, R.; Choo, S.; Chugh, R.; Dinner, S.; et al. Adolescent and Young Adult (AYA) Oncology, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2023, 21, 851–880. [Google Scholar] [CrossRef]
- Smith, A.W.; Seibel, N.L.; Lewis, D.R.; Albritton, K.H.; Blair, D.G.; Blanke, C.D.; Bleyer, A.W.; Freyer, D.R.; Geiger, A.M.; Hayes-Lattin, B.; et al. Next Steps for Adolescent and Young Adult Oncology Workshop: An Update on Progress and Recommendations for the Future. Cancer 2016, 122, 988–999. [Google Scholar] [CrossRef]
- Adolescent and Young Adult Oncology Progress Review Group. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancer; NIH Publication No. 06-6067; NIH Publication: Bethesda, MD, USA, 2006. [Google Scholar]
- Kaliki, S.; Shields, C.L.; Mashayekhi, A.; Ganesh, A.; Furuta, M.; Shields, J.A. Influence of Age on Prognosis of Young Patients with Uveal Melanoma: A Matched Retrospective Cohort Study. Eur. J. Ophthalmol. 2013, 23, 208–216. [Google Scholar] [CrossRef]
- Mishra, K.K.; Daftari, I.K.; Weinberg, V.; Cole, T.; Quivey, J.M.; Castro, J.R.; Phillips, T.L.; Char, D.H. Risk Factors for Neovascular Glaucoma After Proton Beam Therapy of Uveal Melanoma: A Detailed Analysis of Tumor and Dose–Volume Parameters. Int. J. Radiat. Oncol. 2013, 87, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Polishchuk, A.L.; Mishra, K.K.; Weinberg, V.; Daftari, I.K.; Nguyen, J.M.; Cole, T.B.; Phillips, T.L.; Char, D.H.; Quivey, J.M. Temporal Evolution and Dose-Volume Histogram Predictors of Visual Acuity After Proton Beam Radiation Therapy of Uveal Melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 91–97. [Google Scholar] [CrossRef]
- Mishra, K.K.; Quivey, J.M.; Daftari, I.K.; Weinberg, V.; Cole, T.B.; Patel, K.; Castro, J.R.; Phillips, T.L.; Char, D.H. Long-term Results of the UCSF-LBNL Randomized Trial: Charged Particle With Helium Ion Versus Iodine-125 Plaque Therapy for Choroidal and Ciliary Body Melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 376–383. [Google Scholar] [CrossRef]
- Daftari, I.K.; Mishra, K.K.; Singh, R.P.; Shadoan, D.J.; Phillips, T.L. An Overview of the Control System for Dose Delivery at the UCSF Dedicated Ocular Proton Beam. Int. J. Med. Phys. Clin. Eng. Radiat. Oncol. 2016, 5, 242–262. [Google Scholar] [CrossRef]
- Egger, E.; Schalenbourg, A.; Zografos, L.; Bercher, L.; Boehringer, T.; Chamot, L.; Goitein, G. Maximizing local tumor control and survival after proton beam radiotherapy of uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef]
- Egger, E.; Zografos, L.; Schalenbourg, A.; Beati, D.; Bhringer, T.; Chamot, L.; Goitein, G. Eye retention after proton beam radiotherapy for uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 867–880. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; de Koning, L.; Coupland, S.E.; Jochemsen, A.G.; Marais, R.; Stern, M.-H.; Valente, A.; Barnhill, R.; Cassoux, N.; Evans, A.; et al. So Close, yet so Far: Discrepancies between Uveal and Other Melanomas. A Position Paper from UM Cure 2020. Cancers 2019, 11, 1032. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef]
- Zako, C.; Scholey, J.; Daftari, I.K.; Weinberg, V.K.; Swason, C.; Quivey, J.M.; Char, D.H.; Mishra, K.K. Long Term Clinical Outcomes with Dedicated Proton Ocular Beam and Helium Ion Radiation for Uveal Melanoma Patients Aged 45 and Younger. In Proceedings of the 2021 American Society for Radiation Oncology Meeting, Chicago, IL, USA, 24–27 October 2021. [Google Scholar]
- Nayman, T.; Bostan, C.; Logan, P.; Burnier, M.N., Jr. Uveal Melanoma Risk Factors: A Systematic Review of Meta-Analyses. Curr. Eye Res. 2017, 42, 1085–1093. [Google Scholar] [CrossRef]
- Gragoudas, E.S.; Lane, A.M.; Regan, S.; Li, W.; Judge, H.E.; Munzenrider, J.E.; Seddon, J.M.; Egan, K.M. A Randomized Controlled Trial of Varying Radiation Doses in the Treatment of Choroidal Melanoma. Arch. Ophthalmol. 2000, 118, 773–778. [Google Scholar] [CrossRef]
- Castro, J.R.; Char, D.H.; Petti, P.L.; Daftari, I.K.; Quivey, J.M.; Singh, R.P.; Blakely, E.A.; Phillips, T.L. 15 years experience with helium ion radiotherapy for uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 989–996. [Google Scholar] [CrossRef]
- Hartsell, W.F.; Kapur, R.; Hartsell, S.O.C.; Sweeney, P.; Lopes, C.; Duggal, A.; Cohen, J.; Chang, J.; Polasani, R.S.; Dunn, M.; et al. Feasibility of Proton Beam Therapy for Ocular Melanoma Using a Novel 3D Treatment Planning Technique. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 353–359. [Google Scholar] [CrossRef]
- Gragoudas, E.S. Proton Beam Irradiation of Uveal Melanomas: The First 30 Years The Weisenfeld Lecture. Investig. Opthalmology Vis. Sci. 2006, 47, 4666–4673. [Google Scholar] [CrossRef] [PubMed]
- Gragoudas, E.; Li, W.; Goitein, M.; Lane, A.M.; Munzenrider, J.E.; Egan, K.M. Evidence-Based Estimates of Outcome in Patients Irradiated for Intraocular Melanoma. Arch. Ophthalmol. 2002, 120, 1665–1671. [Google Scholar] [CrossRef]
- Pica, A.; (San Francisco, CA, USA). Personal communication, 2024.
- Shields, C.L.; Kaliki, S.; Arepalli, S.; Atalay, H.T.; Manjandavida, F.P.; Pieretti, G.; Shields, J.A. Uveal melanoma in children and teenagers. Saudi J. Ophthalmol. 2013, 27, 197–201. [Google Scholar] [CrossRef]
- Field, M.G.; Decatur, C.L.; Kurtenbach, S.; Gezgin, G.; van der Velden, P.A.; Jager, M.J.; Kozak, K.N.; Harbour, J.W. PRAME as an independent biomarker for metastasis in uveal melanoma. Clin. Cancer Res. 2016, 22, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Afshar, A.R.; Damato, B.E.; Stewart, J.M.; Zablotska, L.B.; Roy, R.; Olshen, A.B.; Bastian, B.C.; Joseph, N.M. Next-Generation Sequencing of Uveal Melanoma for Detection of Genetic Alterations Predicting Metastasis. Transl. Vis. Sci. Technol. 2019, 8, 18. [Google Scholar] [CrossRef]
- Scholes, A.G.M.; Damato, B.E.; Nunn, J.; Hiscott, P.; Grierson, I.; Field, J.K. Monosomy 3 in Uveal Melanoma: Correlation with Clinical and Histologic Predictors of Survival. Investig. Opthalmology Vis. Sci. 2003, 44, 1008–1011. [Google Scholar] [CrossRef]
- Damato, B.; Duke, C.; Coupland, S.E.; Hiscott, P.; Smith, P.A.; Campbell, I.; Howard, P.; Douglas, A. Cytogenetics of Uveal Melanoma: A 7-Year Clinical Experience. Ophthalmology 2007, 114, 1925–1931.e1. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L.; Shields, J.A. Uveal melanoma: Estimating prognosis. Indian J. Ophthalmol. 2015, 63, 93–102. [Google Scholar] [CrossRef]
- Harbour, J.W. A Prognostic Test to Predict the Risk of Metastasis in Uveal Melanoma Based on a 15-Gene Expression Profile. In Molecular Diagnostics for Melanoma; Humana: Totowa, NJ, USA, 2013; Available online: https://link.springer.com/protocol/10.1007/978-1-62703-727-3_22 (accessed on 7 March 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median | Range | |
|---|---|---|
| Follow-Up (months) | 85.7 | 3–301 |
| Age at RT (years) | 38.3 | 13.3–45.9 |
| Tumor Height (mm) | 4.5 | 0.8–15.8 |
| Largest Tumor Diameter (mm) | 10.5 | 2.3–25.1 |
| Tumor Distance to Disc (mm) | 3.2 | 0–24.0 |
| Tumor Distance to Fovea (mm) | 2.0 | 0–24.0 |
| %Tumor 0–2 mm of Disc | 41% | |
| %Tumor 0–2 mm of Fovea | 52% | |
| %Ciliary Body Tumors | 11% |
| PBRT | ≤30 n = 46 | >30–35 n = 43 | >35–40 n = 59 | >40–45 n = 92 | ANOVA Probability Value |
|---|---|---|---|---|---|
| Height | 5.5 (3.2) | 5.3 (2.5) | 4.6 (2.4) | 5.5 (3.1) | p = 0.24 |
| Max Diameter | 11.4 (4.6) | 10.3 (2.9) | 10.4 (3.7) | 11.0 (3.9) | p = 0.41 |
| Helium-Ion RT | ≤30 n = 14 | >30–35 n = 19 | >35–40 n = 18 | >40–45 n = 27 | Kruskal–Wallis Probability Value |
| Height | 5.5 (3.2) | 5.3 (2.5) | 4.6 (2.4) | 5.5 (3.1) | p = 0.30 |
| Max Diameter | 11.4 (4.6) | 10.3 (2.9) | 10.4 (3.7) | 11.0 (3.9) | p = 0.74 |
| Significant Univariate Predictors | Hazard Ratio (95% CI) | LLR Test Probability Value |
|---|---|---|
| ↓ Tumor Height | 1.21 (1.10–1.33) | 0.0003 |
| ↑ Tumor–Disc Distance (≤2 vs. >2 mm) | 0.32 (0.16–0.65) | 0.0008 |
| ↓ Dose to: | ||
| ≤50% Nerve | 1.17 (1.07–1.26) | 0.0004 |
| ≤ 50% Lens | 1.02 (1.01–1.03) | 0.004 |
| ≤50% Disc | 1.01 (1.004–1.02) | 0.001 |
| ≤20% Ciliary Body | 1.04 (1.02–1.06) | 0.0002 |
| Multivariate Independent Predictors | ||
| ↓ Tumor Height | 1.12 (1.01–1.25) | 0.036 |
| ↓ ≤20% Dose to Ciliary Body | 1.04 (1.01–1.06) | 0.0002 |
| ↑ Tumor–Disc Distance (≤2 vs. >2 mm) | 0.27 (0.13–0.54) | 0.0003 |
| Median | Range | |
|---|---|---|
| Follow-Up (months) | 256.7 | 24–450 |
| Age at RT (years) | 37.1 | 18.1–45.5 |
| Median Dose (GyE) | 70 | 48–80 |
| Tumor Height (mm) | 6.0 | 2.9–14.0 |
| Largest Tumor Diameter (mm) | 10.5 | 5.0–25.0 |
| Tumor Distance to Disc (mm) | 3.5 | 0–13.0 |
| Tumor Distance to Fovea (mm) | 3.0 | 0–10.5 |
| %Tumor 0–2 mm of Disc | 33% | |
| %Tumor 0–2 mm of Fovea | 44% | |
| %Ciliary Body Tumors | 22% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zako, C.; Nisanova, A.; Weinberg, V.; Scholey, J.; Swason, C.; Afshar, A.R.; Quivey, J.; Daftari, I.K.; Tsai, T.; Park, S.S.; et al. Long-Term Clinical Outcomes for Adolescent and Young-Adult Uveal Melanoma Patients Treated with Dedicated Particle-Beam Radiation. Cancers 2025, 17, 2042. https://doi.org/10.3390/cancers17122042
Zako C, Nisanova A, Weinberg V, Scholey J, Swason C, Afshar AR, Quivey J, Daftari IK, Tsai T, Park SS, et al. Long-Term Clinical Outcomes for Adolescent and Young-Adult Uveal Melanoma Patients Treated with Dedicated Particle-Beam Radiation. Cancers. 2025; 17(12):2042. https://doi.org/10.3390/cancers17122042
Chicago/Turabian StyleZako, Carly, Arina Nisanova, Vivian Weinberg, Jessica Scholey, Carisa Swason, Armin R. Afshar, Jeanne Quivey, Inder K. Daftari, Tony Tsai, Susanna S. Park, and et al. 2025. "Long-Term Clinical Outcomes for Adolescent and Young-Adult Uveal Melanoma Patients Treated with Dedicated Particle-Beam Radiation" Cancers 17, no. 12: 2042. https://doi.org/10.3390/cancers17122042
APA StyleZako, C., Nisanova, A., Weinberg, V., Scholey, J., Swason, C., Afshar, A. R., Quivey, J., Daftari, I. K., Tsai, T., Park, S. S., Seider, M., Johnson, R. N., Char, D. H., & Mishra, K. K. (2025). Long-Term Clinical Outcomes for Adolescent and Young-Adult Uveal Melanoma Patients Treated with Dedicated Particle-Beam Radiation. Cancers, 17(12), 2042. https://doi.org/10.3390/cancers17122042