
The Impact of Genetic Variations on Radiotherapy Toxicity in Breast Cancer Patients: A Meta-Analysis of Acute and Late Skin Adverse Effects

 ,
,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
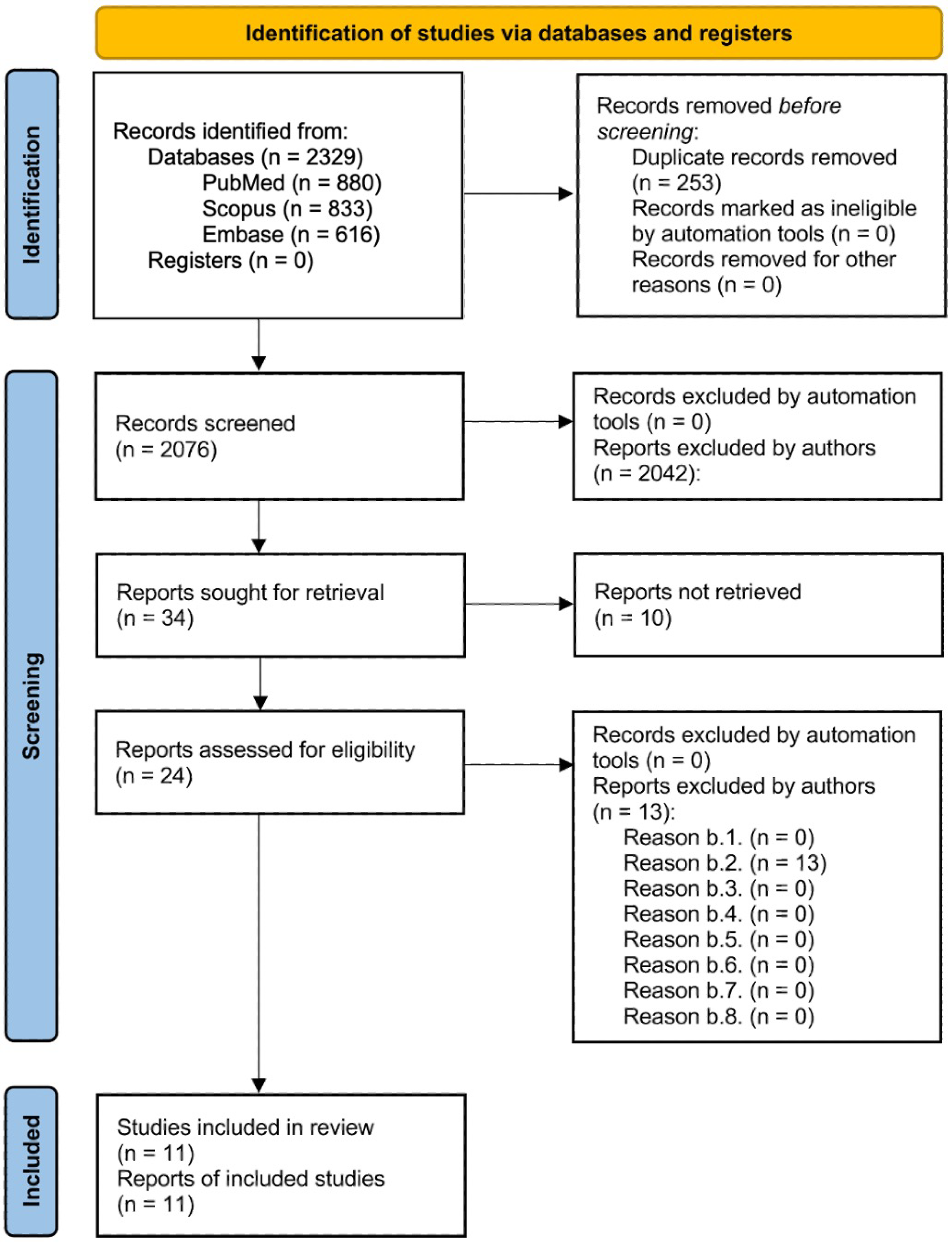
2.1. Protocol and Guideline Compliance
2.2. Literature Search Strategy and Database Selection
2.3. Selection Criteria Overview
- Inclusion criteria:
- a.1.
- Studied population: articles involving breast cancer patients who have undergone radiotherapy;
- a.2.
- Genetic focus: research examining genetic markers or genetic variations associated with skin radiotoxicity;
- a.3.
- Study design: case-control studies, observational studies, or randomized controlled trials;
- a.4.
- Outcomes studied: studies investigating the correlation between genetic markers and skin radiotherapy-induced side effects, including both acute and late-onset toxicity;
- a.5.
- Language: articles published in English;
- a.6.
- Human studies: studies conducted exclusively on human participants;
- a.7.
- Publication date range: articles published between 1 January 2014, and 31 December 2024;
- Exclusion criteria:
- b.1.
- Non-breast cancer populations: studies focused on cancers other than breast cancer;
- b.2.
- Lack of genetic data: articles lacking information on genetic markers or genetic variations relevant to skin radiotoxicity;
- b.3.
- Preclinical studies: research involving animal models or in vitro studies;
- b.4.
- Radiotherapy without genetic focus: studies discussing skin radiotoxicity in breast cancer patients without examining genetic predispositions;
- b.5.
- Language restrictions: articles published in languages other than English;
- b.6.
- Ineligible works: meta-analyses, systematic reviews, reviews, case reports, conference abstracts, encyclopedia articles, book chapters, posters, or oral presentations addressing genetic factors influencing radiotoxicity in breast cancer patients;
- b.7.
- Chemotherapy toxicity: studies investigating toxicity associated with chemotherapy or other systemic therapies (e.g., hormonal or immunotherapy);
- b.8.
- Out-of-date publications: articles published before 1 January 2014, or after 31 December 2024.
2.4. Article Selection Process
2.5. Data Collection Process
2.6. Outcomes Sought
2.7. Selected Articles
2.8. Excluded Studies and Reasons for Ineligibility
2.9. Statistical Methods Applied
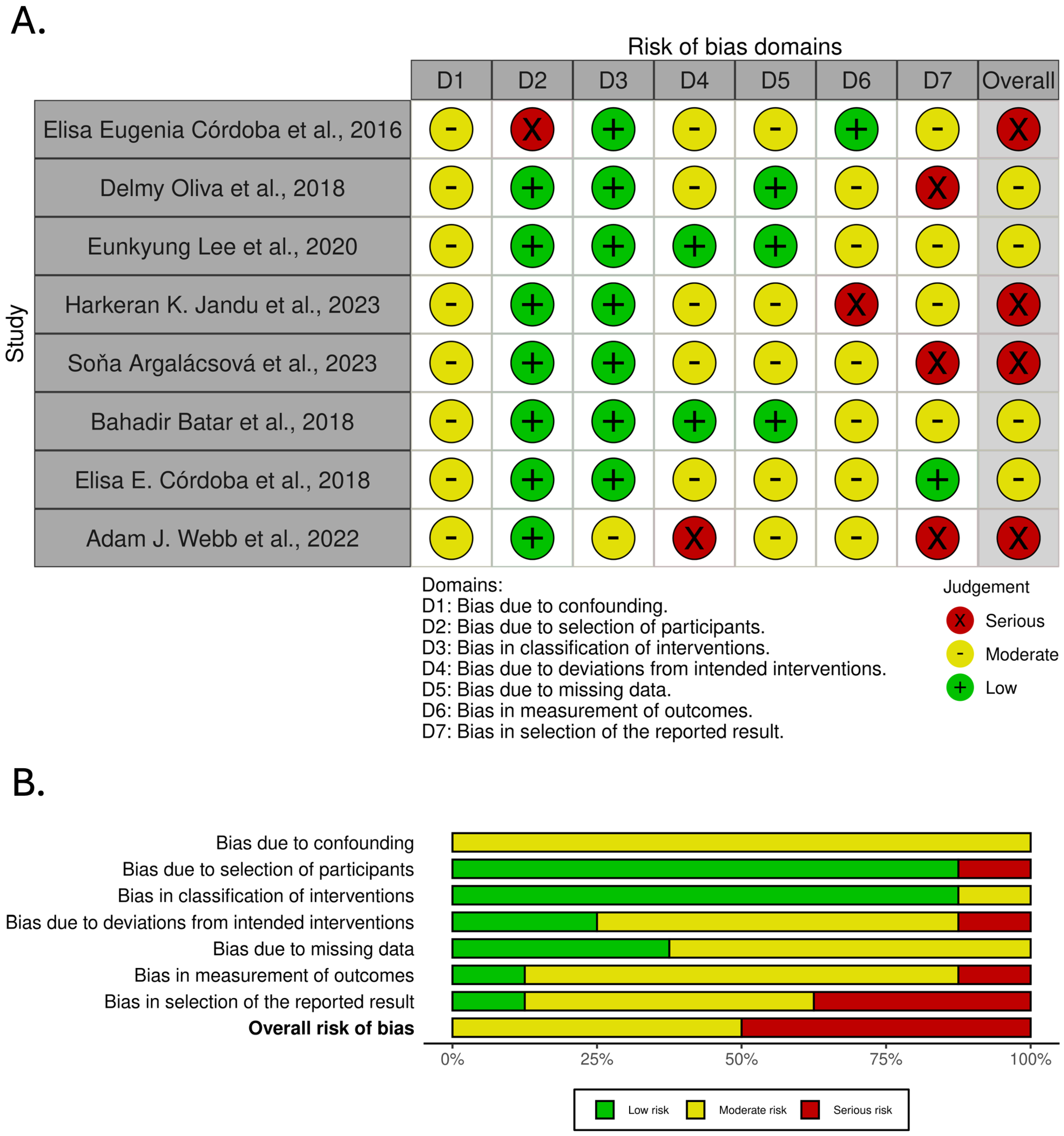
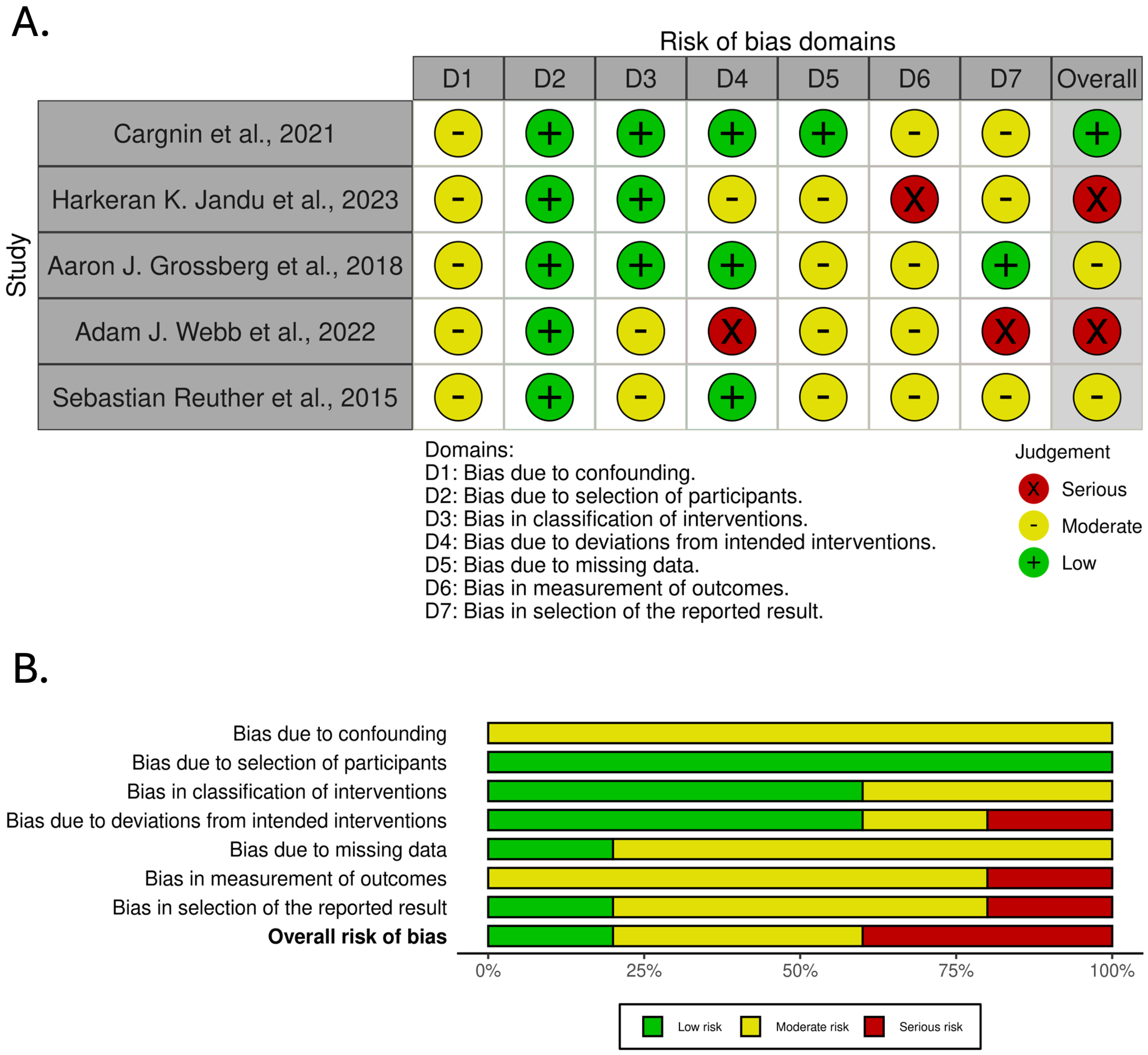
2.10. Bias Assessment
3. Results
3.1. Results of the Assessment of Bias
3.2. Impact of Excluding High-Risk Studies on Meta-Analysis Results
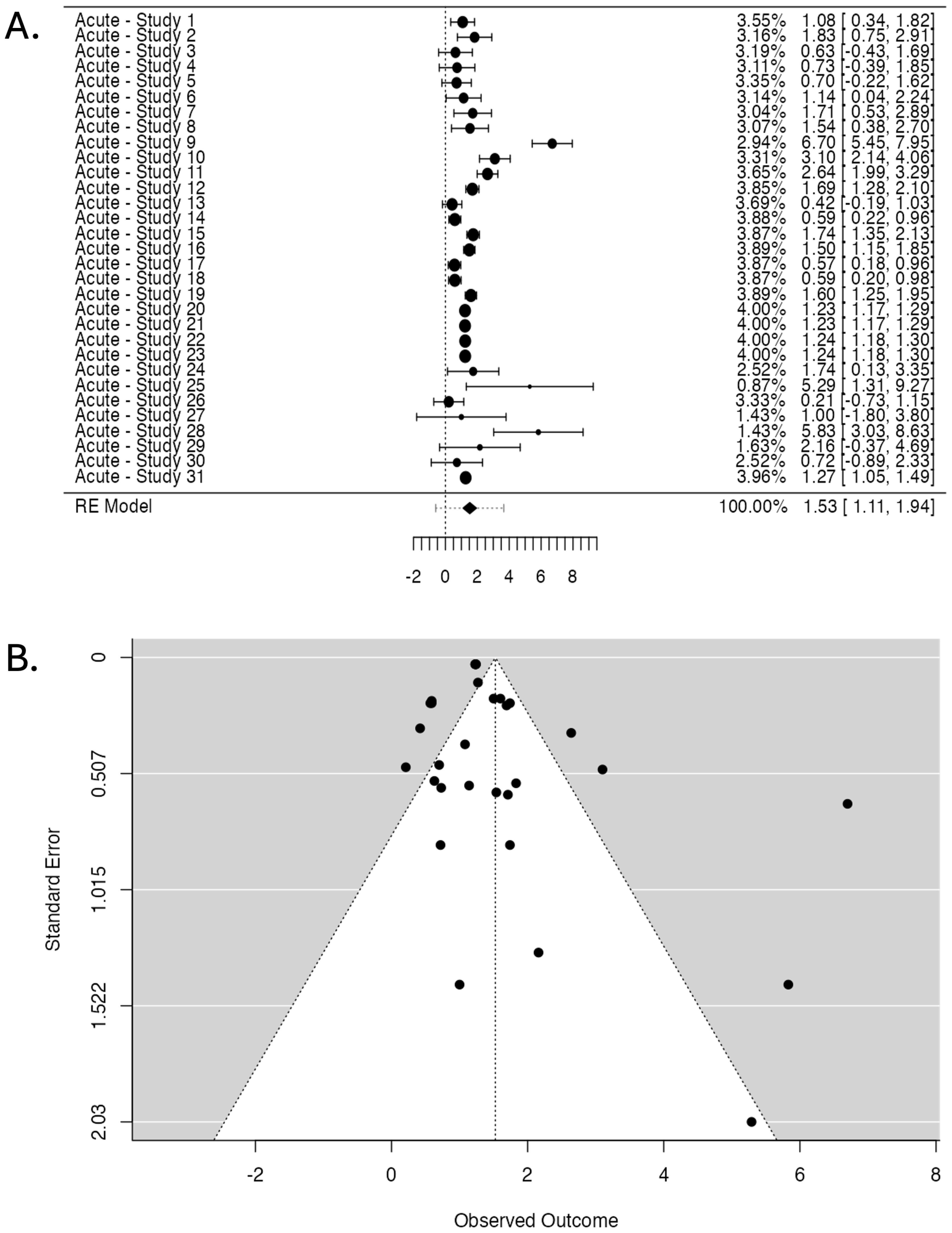
3.3. Pooled Analysis of Genetic Markers Associated with Radiotherapy-Induced Skin Acute Effects
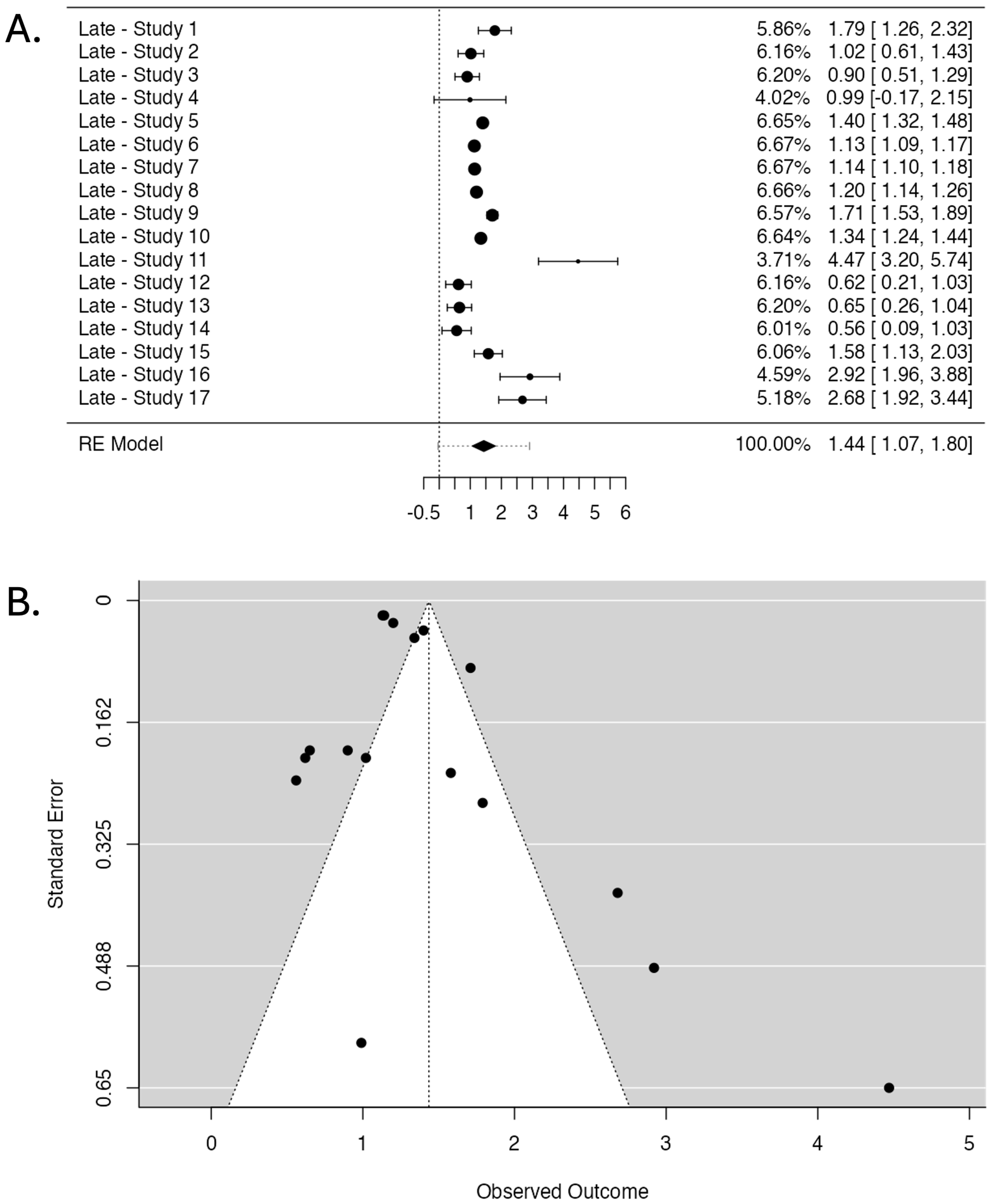
3.4. Pooled Analysis of Genetic Markers Associated with Radiotherapy-Induced Skin Late Effects
3.5. Statistically Significant Genetic Markers Identified
4. Discussion
4.1. Discussion of Radiotherapy-Induced Skin Acute Effects and Associated Genetic Markers
4.2. Discussion of Radiotherapy-Induced Skin Late Effects and Associated Genetic Markers
4.3. Pathway-Based Analysis of Radiogenomic Markers in Skin Toxicity
4.3.1. DNA Repair Genes and Radiotherapy Toxicity
4.3.2. Circadian Rhythm and Radiotherapy Toxicity
4.3.3. Oxidative Stress Pathway in Radiation Skin Toxicity
4.3.4. Inflammatory Gene Polymorphisms in Radiation Skin Toxicity
4.4. Relevance and Future Potential of Genetic Markers Identified
4.5. Impact of Methodological Differences Among Included Studies
4.6. Feasibility, Validity, and Generalizability of the Meta-Analysis Findings
5. Limitations
- High inter-study heterogeneity: the included studies varied significantly in their design, patient characteristics, radiotherapy techniques, toxicity scoring systems, and SNP genotyping methods. This heterogeneity likely contributed to the wide range of reported effect sizes and may reduce the overall comparability and reproducibility of the findings;
- Risk of bias across studies: the ROBINS-I tool rated many of the studies included in the meta-analysis as having moderate-to-serious risk of bias. Common concerns involved confounding factors, missing outcome data, and inconsistencies in reporting, all of which may have influenced the strength and direction of observed associations;
- Potential publication bias: Funnel Plot asymmetry and Egger’s regression tests suggested the presence of publication bias, particularly for studies on acute toxicity. This indicates that studies with non-significant or null results may be underrepresented in the literature, potentially leading to overestimating true associations;
- Limited number of studies and replication: the number of eligible studies—especially those examining late toxicity—remains small. Many gene–toxicity associations were reported in isolated studies and have yet to be replicated, limiting the findings’ generalizability and clinical validity;
- Lack of standardized protocols: there was no uniform approach to SNP selection, outcome classification, or statistical modeling across studies. This lack of standardization impedes cross-study comparison and hinders the development of robust, reproducible predictive models;
- Insufficient adjustment for confounders: several studies did not adequately control for important confounding variables such as age, BMI, comorbidities, or specific treatment variables (e.g., radiation dose or technique), which could have influenced toxicity outcomes independently of genetic factors;
- Variability in toxicity assessment tools: different grading scales (e.g., CTCAE, RTOG, and LENT-SOMA) across studies may have led to inconsistent classification of toxicity severity, complicating pooled analyses and interpretation of effect estimates.
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication [Ref.] | Country/ Period | Study Size— Population | Study Design | Association Gene/Pathway with Radiotoxicity, OR (p) | Genetic Testing Methodology | Type of Radiotherapy | Dose and Fractionation | Radiotherapy-Induced Toxicity | Assessment Methods | Statistical Analysis | Authors’ Conclusions | Study No. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Elisa Eugenia Córdoba et al., 2016 [9] | Argentina n/a | 80— Breast Cancer Female— Mean age (59 years) | Observational Study | GSTP1 (rs1695) 1.08 (p = 0.88) | PCR-based restriction fragment length polymorphism | Conventional RT (50–50.4 Gy, 1.8–2 Gy/fraction) followed by a 12–18 Gy electron boost | 50–50.4 Gy, 1.8–2 Gy/fraction; 12–18 Gy electron boost | Acute skin toxicity (Grade ≥ 2) | Radiation Therapy Oncology Group (RTOG) criteria | Univariate logistic regression, Principal Component Analysis (PCA), Odds Ratios (ORs), Confidence Intervals (CIs) | No solid evidence was found for an association between any SNP and acute toxicity. | Acute—Study 1 |
| GSTP1 (rs1695) 1.83 (p = 0.27) | Acute—Study 2 | |||||||||||
| SOD2 (rs4880) 0.63 (p = 0.39) | Acute—Study 3 | |||||||||||
| SOD2 (rs4880) 0.73 (p = 0.57) | Acute—Study 4 | |||||||||||
| NOS3 (rs1799983) 0.70 (p = 0.45) | Acute—Study 5 | |||||||||||
| NOS3 (rs1799983) 1.14 (p = 0.82) | Acute—Study 6 | |||||||||||
| GSTA1 (rs3957356) 1.71 (p = 0.36) | Acute—Study 7 | |||||||||||
| GSTA1 (rs3957356) 1.54 (p = 0.46) | Acute—Study 8 | |||||||||||
| Delmy Oliva et al., 2018 [10] | Sweden February 2011–May 2013 | 119— Breast Cancer Female— Age > 18 | Observational Study | XRCC2 (rs2040639) 6.70 (p = 0.007) | Illumina Golden Gate Genotyping assay | Adjuvant RT with two parallel opposing tangential fields using Varian Linacc 2100 CD (3D treatment planning) | 50 Gy in 25 fractions; 42.56 Gy in 16 fractions (hypofractionated schedule) | Acute radiation skin reactions (ARSR): itching, burning, irritation | Radiation Therapy Oncology Group (RTOG) scoring system, Visual Analog Scale (VAS) | Odds Ratios (ORs), Confidence Intervals (CIs), Fisher’s exact test, Hochberg method for multiple testing correction | XRCC2 rs2040639 SNP associated with burning as ARSR. | Acute—Study 9 |
| IFNG (rs2069705) 3.10 (p = 0.01) | IFNG rs2069705 SNP associated with itching as ARSR. | Acute—Study 10 | ||||||||||
| Eunkyung Lee et al. 2020 [11] | US December 2008–January 2014 | 416— Breast Cancer Female— Age > 18 | Observational Study | ATM (rs61915066) 2.64 (p = 0.004) | Illumina Human Omni2.5–8 v1 genome-wide BeadChip array | Postmastectomy RT, 3D-conformal technique | 42.4 to 66 Gy, 3 to 7 weeks | Early adverse skin reactions (EASRs), moist desquamation | Oncology Nursing Society (ONS) scale (0–6) | Multivariable logistic regression, Odds Ratios (ORs), Confidence Intervals (CIs) | ATM rs61915066 is associated with RT-induced EASR. | Acute—Study 11 |
| CHEK1 (rs11220184) 1.69 (p = 0.013) | No evidence of association for CHEK2 with RT-induced EASR. | Acute—Study 12 | ||||||||||
| ERCC2 (rs60152947) 0.42 (p = 0.007) | ERCC2 variants associated with reduced risk of RT-induced EASR. | Acute—Study 13 | ||||||||||
| ERCC2 (rs10404465) 0.59 (p = 0.007) | Acute—Study 14 | |||||||||||
| ERCC2 (rs1799786) 1.74 (p = 0.007) | Acute—Study 15 | |||||||||||
| TGFB1 (rs4803455) 1.50 (p = 0.025) | TGFB1 rs4803455 associated with RT-induced EASR. | Acute—Study 16 | ||||||||||
| TGFB1 (rs2241714) 0.57 (p = 0.04) | Acute—Study 17 | |||||||||||
| RAD51C (rs302877) 0.59 (p = 0.006) | RAD51C variants associated with reduced risk of RT-induced EASR. | Acute—Study 18 | ||||||||||
| RAD51C (rs405684) 1.60 (p = 0.07) | Acute—Study 19 | |||||||||||
| Harkeran K. Jandu et al., 2023 [12] | France, Italy, Belgium, Spain, UK, US 2014–2016 | 1640— Breast Cancer Female— Mean age (58.5 years) | Case-Control Study | GPC5 (rs145328458) 1.23 (p = 1.06 × 10−9) | Illumina OncoArrays, genotyping and imputation with SHAPEIT and IMPUTEv2 | Whole-breast radiotherapy (adjuvant external beam radiotherapy, 47.9% received IMRT) | 50 Gy in a median of 25 fractions (range: 28.5–56.0) | Oedema Grade ≥ 2 (2-year follow-up) | Standard Terminology Criteria for Adverse Events (CTCAE v4.0) | Multivariable generalized linear models, Logistic regression, Odds Ratios (ORs), and Confidence Intervals (CIs). | Significant association identified for GPC5 rs145328458 with oedema Grade ≥ 2. | Acute—Study 20 |
| GPC5 (rs61966612) 1.23 (p = 1.23 × 10−9) | Significant association was identified for GPC5 rs61966612 with oedema Grade ≥ 2. | Acute—Study 21 | ||||||||||
| AC093240.1 (rs12657177) 1.24 (p = 1.12 × 10−10) | A significant association was identified for AC093240.1 rs12657177 with oedema Grade ≥ 2. | Acute—Study 22 | ||||||||||
| AC093240.1 (rs75912034) 1.24 (p = 1.21 × 10−10) | Significant association identified for AC093240.1 rs73151332 with oedema Grade ≥ 2. | Acute—Study 23 | ||||||||||
| Soňa Argalácsová et al., 2023 [13] | Czech Republic March 2015–May 2021 | 213— Breast Cancer Female— Age >18 | Observational Study | BRCA1, BRCA2 1.74 (p = 0.50) | Germline next-generation sequencing (CZECANCA multigene panel targeting 226 genes) | Adjuvant radiotherapy (whole-breast irradiation, postmastectomy thorax wall radiation with locoregional lymph nodes) | Various doses, not specified precisely | Acute dermatitis, lymphedema | Common Terminology Criteria for Adverse Events (CTCAE) | Cox proportional hazards model, Gehan–Breslow–Wilcoxon test | No evidence of increased radiation-induced toxicity for BRCA1/BRCA2 PV carriers. | Acute—Study 24 |
| CHEK2, ATM, PALB2, RAD51C, RAD51D, BARD1, TP53, FANCM 5.29 (p = 0.41) | No evidence of increased radiation-induced toxicity for OTHER-PV carriers. | Acute—Study 25 | ||||||||||
| Bahadir Batar et al., 2018 [14] | Turkey n/a | 100— Breast Cancer Female— Mean Age (48.7 years) | Observational Study | ERCC1 (rs3212986) 0.21 (p < 0.001) | Genotyping by real-time PCR technique | 3D conformal radiotherapy | 50–66 Gy (2 Gy dose fraction | Acute skin reactions, DNA damage levels, apoptosis | Common Toxicity Criteria (C.T.C.), Micronucleus assay, 8-OHdG assay, TUNEL staining | Pearson’s Chi-square test, Fisher’s exact test, Odds Ratios (ORs), Confidence Intervals (CIs) | ERCC1 rs3212986 CC genotype may provide protection against radiotherapy-induced acute reactions. | Acute—Study 26 |
| XPC (rs3731055) 1.00 (p = 1.00) | There is no evidence of an association between XPC rs3731055 and radiotherapy-induced acute reactions. | Acute—Study 27 | ||||||||||
| Elisa E. Córdoba et al., 2018 [15] | Argentina 2012–2016 | 125— Breast Cancer Female— Age > 18 | Observational Study | TNF-α (rs1800629) 5.83 (p = 0.22) | Pyrosequencing | Conventional 3D external beam therapy | Total dose: 50–50.4 Gy, daily fractions of 1.8–2 Gy over 5 weeks | Severe radiodermatitis (grades 3 and 4) | RTOG (Radiation Therapy Oncology Group) scoring system | Chi-square test, Fisher’s exact test, Odds Ratios (ORs), Confidence Intervals (CIs) | There is no evidence of an association between TNF-α G-308A polymorphism and severe radiodermatitis. | Acute—Study 28 |
| IL-6 (rs1800795) 2.16 (p = 0.54) | There is no evidence of an association between IL-6 G-174C polymorphism and severe radiodermatitis. | Acute—Study 29 | ||||||||||
| ATM (rs1801516) 0.72 (p = 0.68) | There is no evidence of an association between ATM G1853A polymorphism and severe radiodermatitis. | Acute—Study 30 | ||||||||||
| Adam J. Webb et al., 2022 [16] | France, Italy, Belgium, Spain, UK, Germany (2014)–2017 | 1690— Breast Cancer Female— Mean age (58 years) | Case-Control Study | PER3 (rs2087947) 1.27 (p = 0.02) | Genotyping using Illumina Infinium OncoArrays | Conventional radiotherapy | Varied across centers, standard fractionation schedules applied | Acute erythema | CTCAE v4.00 scoring system | Logistic Regression, Odds Ratios (ORs), Confidence Intervals (CIs) | PER3 rs2087947 genotype influences the occurrence of acute erythema. | Acute—Study 31 |
| Author, Year of Publication [Ref.] | Country/ Period | Study Size — Population | Study Design | Association Gene/Pathway with Radiotoxicity, OR (p) | Genetic Testing Methodology | Type of Radiotherapy | Dose and Fractionation | Radiotherapy-Induced Toxicity | Assessment Methods | Statistical Analysis | Authors’ Conclusions | Study No. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cargnin et al., 2021 [17] | Italy 1989–2010 | 285— Breast Cancer Female— Mean age (60.8 years) | Case-Control Study | TP53 (rs1042522), 1.79 (p = 0.028) | Targeted NGS and real-time PCR | 3D Conformal Radiotherapy | 50 Gy in daily fractions of 2 Gy, followed by 9–10 Gy boost for invasive lesions | Subcutaneous fibrosis and/or telangiectasia (grade 2–3) | LENT-SOMA scale (graded annually) | Logistic regression (adjusted for age and BMI), Fisher’s test | No definitive association was established; further studies are required with larger cohorts. | Late—Study 1 |
| ERCC2 (rs1052555), 1.02 (p = 0.922) | Late—Study 2 | |||||||||||
| ERCC2 (rs13181), 0.90 (p = 0.595) | Late—Study 3 | |||||||||||
| LIG1 (rs7246696), 0.99 (p = 0.971) | Late—Study 4 | |||||||||||
| Harkeran K. Jandu et al., 2023 [12] | France, Italy, Belgium, Spain, UK, US 2014–2016 | 1640— Breast Cancer Female— Mean age (58.5 years) | Case-Control Study | PAX7 (rs643644), 1.40 (p = 3.54 × 10−8) | Illumina OncoArrays (~600,000 SNPs), Imputation using SHAPEIT and IMPUTEv2 | Whole-breast radiotherapy, with or without tumor-bed boost | 50 Gy in daily fractions of 2 Gy, with boost for some patients | Arm lymphoedema G1 | CTCAE v4.0, Annual follow-up | Logistic regression, Generalized Linear Models, PLINK v2 | PAX7 is associated with an increased risk of arm lymphoedema; replication is recommended. | Late—Study 5 |
| ATXN7L1 (rs11345494), 1.13 (p = 5.78 × 10−8) | Arm lymphoedema G1 | ATXN7L1 is associated with an increased risk of arm lymphoedema. | Late–Study 6 | |||||||||
| ANOS1 (rs188287402), 1.14 (p = 2.80 × 10−8) | Nipple Retraction G2 | ANOS1 is associated with an increased risk of nipple retraction. | Late—Study 7 | |||||||||
| CRYM/ANKS4B (rs12443861), 1.20 (p = 6.17 × 10−8) | Telangiectasia G1 | CRYM/ANKS4B is associated with an increased risk of telangiectasia. | Late—Study 8 | |||||||||
| SLC10A4 (rs34063419), 1.71 (p = 1.21 × 10−8) | Induration G2 | SLC10A4 is associated with an increased risk of induration. | Late—Study 9 | |||||||||
| LINC01779 (rs77311050), 1.34 (p = 2.54 × 10−8) | Induration G2 | LINC01779 is associated with an increased risk of induration. | Late—Study 10 | |||||||||
| Aaron J. Grossberg et al., 2018 [18] | US 2011–2014 | 287— Breast Cancer Female — Age 40+ | Observational Study | TGFB1 (C−509T), 4.47 (p = 0.02) | Real-time polymerase chain reaction analyses | Hypofractionated WBI vs. conventionally fractionated WBI | 42.56 Gy in 16 fractions or 50 Gy in 25 fractions | Subcutaneous fibrosis (grade 2+) | Physician-assessed fibrosis using LENT/SOMA scale; patient-reported outcomes | Multivariable logistic regression models; Fisher exact test; significance levels reported | The C−509T allele in TGFB1 is associated with an increased risk of grade 2 or higher fibrosis. Genetic profiling of TGFB1 may help guide treatment decisions. | Late—Study 11 |
| Adam J. Webb et al., 2022 [16] | France, Italy, Belgium, Spain, UK, Germany 2014–2017 | 1690— Breast Cancer Female— Mean age (58 years) | Case-Control Study | CLOCK (rs1801260), 0.62 (p < 0.01) | Genotyping using Illumina Infinium OncoArrays (600k SNPs) and imputation using 1000 Genomes Project data | Conventional radiotherapy | Biologically Effective Dose (BED): Acute toxicity = 65 Gy, Late toxicity = 94 Gy | Late atrophy (2 years post-radiotherapy) | CTCAE v4.00, Breast photos | Logistic regression (GLM), mixed effects models, AIC selection | CLOCK (rs1801260), PER3 (rs2087947), and RASD1 (rs11545787) associated with reduced risk of late atrophy (2 years post-radiotherapy). | Late—Study 12 |
| PER3 (rs2087947), 0.65 (p = 0.04) | Late—Study 13 | |||||||||||
| RASD1 (rs11545787), 0.56 (p = 0.02) | Late—Study 14 | |||||||||||
| Sebastian Reuther et al., 2015 [19] | Germany 1988–1995 | 123 Breast Cancer Female—Age mean (60.1 years) | Observational Study | ROS Pathway, 1.58 (p = 0.045) | PCR, TaqMan SNP Genotyping, MassARRAY System | Conventional radiotherapy | Median dose: 55 Gy | Subcutaneous Fibrosis | LENT/SOMA score | Weighted risk model, logistic regression | ROS pathway genes have a minor impact on fibrosis but are significant when using a weighted risk model. | Late—Study 15 |
| DNA Repair, 2.92 (p = 0.023) | DNA repair pathway genes are strongly associated with fibrosis when using a weighted risk model. | Late—Study 16 | ||||||||||
| TGFB1 Signalling, 2,68 (p = 0.005) | Using a weighted risk model, a TGFB1 signaling pathway is strongly associated with fibrosis. | Late—Study 17 |
| No. Crt. | Author, Year of Publication [Ref.] | Reason of Exclusion |
|---|---|---|
| 1. | Kimi Drobin et al., 2020 [55] | Lack of genetic data: articles lacking information on genetic markers or genetic variations relevant to skin radiotoxicity. |
| 2. | Elahe Abdollahi et al., 2023 [56] | |
| 3. | Elahe Abdollahi et al., 2023 [57] | |
| 4. | Narjes Bakhtari et al., 202 [58] | |
| 5. | Joshua Dulong et al., 2020 [59] | |
| 6. | Yi Cui et al., 2018 [60] | |
| 7. | Leslie A Modlin et al., 202 [61] | |
| 8. | Joanna Huszno et al., 2013 [62] | |
| 9. | Jan Drooger et al., 2015 [63] | |
| 10. | Elnaz Naderi et al., 2023 [64] | |
| 11. | Christoph Weigel et al., 2016 [65] | |
| 12. | Otilia Nuta et al., 2016 [66] | |
| 13. | María J Fuentes-Raspall et al., 2015 [67] |
Appendix B
| No. Ctr. | Article, Year, [Ref.] | Bias Due to Confounding | Bias in Selection of Participants | Bias in Classification of Interventions | Bias Due to Deviations from Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Elisa Eugenia Córdoba et al., 2016 [9] | The study controlled for the most important confounding factors, but residual uncontrolled confounding may exist. | Post-intervention variables may have influenced the selection of participants. | Interventions were clearly classified without misclassification or differential misclassification. | Some deviations occurred but were unlikely to affect outcomes significantly. | Some data were missing, but sensitivity analyses suggest minimal impact on results. | Outcome measures were objective and consistently applied across groups. | There was some concern about selective reporting, though most results were transparently reported. | The overall risk of bias is judged as serious due to the serious risk of bias in participant selection and moderate bias in other domains. |
| 2. | Delmy Oliva et al., 2018 [10] | The study does not account for several potential confounders, such as genetic variations unrelated to ARSR. | Participants were consecutively selected from a single hospital. Inclusion and exclusion criteria were clear. | Radiotherapy was uniformly administered based on standard protocols, ensuring consistent classification. | Some participants used corticosteroid cream, while others used moisturizer, leading to differential treatment. | A complete dataset was used for 119 women; minimal missing data were reported. | The Visual Scale is self-reported and may be prone to subjective bias. | Multiple SNPs were tested; only statistically significant results were reported without correction for multiple testing. | The overall risk of bias is assessed as moderate, primarily due to issues related to confounding, outcome measurement, and selection of reported results. |
| 3. | Eunkyung Lee et al., 2019 [11] | Adjusted for significant covariates (race, age, BMI, RT schedule), but potential residual confounding exists. | Patients were part of a well-defined prospective cohort with standardized inclusion criteria. | Radiation therapy was consistently delivered using standardized protocols. | Patients received uniform treatment without deviation from planned interventions. | No missing data were reported for EASRs (Early Adverse Skin Reactions) outcomes, ensuring complete outcome measurement. | Trained physicians performed EASR assessments but could be subjective; the use of a validated scale mitigates this. | The study reports on most outcomes comprehensively but lacks external validation, which may affect reproducibility. | Although the study is well-designed with appropriate adjustments for confounders and comprehensive data collection, the absence of external validation and potential subjectivity in outcome measurement pose a moderate risk of bias. |
| 4. | Harkeran K. Jandu et al., 2023 [12] | The study attempted to control for potential confounders by including clinical and treatment variables in the analysis. However, there may still be unmeasured or residual confounding. | Patients were recruited from multiple centers across Europe and the US. Inclusion and exclusion criteria were clearly defined and applied. | The intervention (radiotherapy) is defined and applied consistently according to protocol at different centers. | Some deviations may have occurred due to different radiotherapy techniques used across centers, but the analysis accounted for these. | Although the study had a relatively large cohort, data points related to certain toxicity endpoints were missing, which could influence the results. | Toxicity assessments were conducted by different clinicians at various sites, potentially introducing measurement variability and bias. | Not all previously reported SNPs associated with toxicity were replicated, and some were excluded from the analysis due to a lack of statistical significance. | The study has a serious risk of bias. The primary weaknesses relate to inconsistencies in outcome measurement and the potential for unmeasured confounding. The findings should be interpreted cautiously, particularly where subjective toxicity measures are involved. |
| 5. | Soňa Argalácsová et al., 2023 [13] | The study attempted to control for important confounders, but residual confounding remains possible. | Interventions were clearly classified according to predefined criteria, with minimal misclassification. | The study had well-defined inclusion criteria and used a clear recruitment process. | Some deviations from the intervention protocol were reported, but they were unlikely to affect the outcome substantially. | Some missing data were reported, but the extent of missingness was insufficient to significantly affect the results. | Measurement of outcomes relied partly on self-reports, which may introduce subjective bias. | Selective reporting was identified, with only statistically significant results being highlighted | The study has a serious risk of bias, due to the presence of serious risk of bias in the selection of reported results, as well as moderate bias in several other domains. |
| 6. | Bahadir Batar et al., 2018 [14] | The study attempts to match cases and controls but does not fully adjust for all potential confounders, such as genetic, lifestyle, and treatment-related factors. | Patients were selected based on well-defined inclusion criteria (newly diagnosed breast cancer patients). | Interventions (radiotherapy) were clearly described and uniformly applied to all participants. | All patients received the same radiotherapy protocol, minimizing bias from deviations. | Data appear complete, with no mention of missing or incomplete datasets. | Measurement of outcomes (acute side effects) was based on self-reports and clinical grading, which may be subjective. | Only specific genes (ERCC1 and XPC) were investigated for polymorphisms. Potential bias may exist due to the selective reporting of results, which focuses on positive findings. | The study generally follows good research practices, but the moderate risk is due to potential confounding factors and selective reporting of results. |
| 7. | Elisa E. Córdoba et al., 2018 [15] | The study considered several confounding variables like age, breast size, and genetic polymorphisms. However, the interactions between these factors were not thoroughly analyzed. | The participants were recruited from a well-defined RT center, and appropriate consent was obtained according to ethical standards. | The study consistently applied standardized radiotherapy protocols (3D external beam therapy) across all participants. | There were no indications of deviations from intended interventions during the study process. | The study mentions the absence of the homozygous minor alleles of certain genes in the population, but it is unclear if the sample size was sufficient to detect these alleles. | Measurement of outcomes (radiodermatitis) was based on clinical observation using the RTOG score. However, subjective assessment may introduce bias. | The reported results match the stated objectives and methodology of the study. | This rating is due to potential bias from confounding variables, possible sample size limitations, and the subjective nature of outcome measurements. However, the study followed standard protocols and properly addressed ethical considerations. |
| 8. | Adam J. Webb et al., 2022 [16] | Potential confounders (e.g., BMI, radiation dose, and surgery type) were controlled for, but differences in grading across sites could introduce bias. | Participants were selected from multiple European sites with different protocols; inclusion criteria were consistent. | Interventions (treatment times) were classified accurately based on solar time; however, not all sites provided consistent timing. | Patients were not randomly assigned to treatment times; treatment time was determined by availability or patient choice. | Missing data were not imputed; incomplete records were omitted, which could bias results. | Outcome measures (e.g., erythema and atrophy) were assessed according to standard protocols but with potential inter-site variability. | Multiple statistical models were tested, and not all were reported; there is a risk of selective reporting. | Based on the domains assessed, this study’s overall risk of bias is rated as “Serious.” The lack of randomization in treatment time assignment and potential variability in outcome measurement across multiple sites are significant sources of bias. |
| No. Ctr. | Article, Year, [Ref.] | Bias Due to Confounding | Bias in Selection of Participants | Bias in Classification of Interventions | Bias Due to Deviations from Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Cargnin et al., 2021 [17] | The statistical analysis considered and adjusted for confounders such as age, BMI, and clinical factors, but not all potential confounders may have been accounted for. | All participants were selected based on clear eligibility criteria related to breast cancer diagnosis and treatment. No apparent selection bias was identified. | The intervention (radiotherapy) was applied uniformly to all patients, with no apparent differences in classification. | The study design adhered closely to the planned intervention protocol. No deviations were noted that would impact the results. | Data were collected and reported thoroughly, with no indication of substantial missing data impacting the results. | The outcome assessment relied on clinical observation and patient reports. Though standard scales (LENT-SOMA) were used, there may be some risk of subjective bias. | All results pertinent to the study objectives were reported, with no indication of selective reporting. | Overall, the study has a low risk of bias. The primary concerns relate to the possibility of unmeasured confounders and the subjective nature of outcome measurement. |
| 2. | Harkeran K. Jandu et al., 2023 [12] | The study attempted to control for potential confounders by including clinical and treatment variables in the analysis. However, there may still be unmeasured or residual Confounding. | Patients were recruited from multiple centers across Europe and the US. Inclusion and exclusion criteria were clearly defined and applied. | The intervention (radiotherapy) is defined and applied consistently according to protocol at different centers. | Some deviations may have occurred due to different radiotherapy techniques used across centers, but the analysis accounted for these. | Although the study had a relatively large cohort, data points related to certain toxicity endpoints were missing, which could influence the results. | Toxicity assessments were conducted by different clinicians at various sites, potentially introducing measurement variability and bias. | Not all previously reported SNPs associated with toxicity were replicated, and some were excluded from the analysis due to a lack of statistical significance. | The study has a serious risk of bias. The primary weaknesses relate to inconsistencies in outcome measurement and the potential for unmeasured confounding. The findings should be interpreted with caution, particularly where subjective toxicity measures are involved. |
| 3. | Aaron J. Grossberg et al., 2018 [18] | The study controls for some confounders, but potential unmeasured Confounding could affect the results. | Participants were enrolled according to precise criteria, minimizing selection bias. | Interventions (WBI protocols) are welldocumented and classified appropriately. | No significant deviations from the intended interventions were reported or identified. | There are missing data due to participants lost to follow-up, which could introduce bias. | Outcomes are measured by physicians who are aware of the genotype status, which could introduce bias. | Reported results cover all pre-specified outcomes without evidence of selective reporting. | Overall, the study presents a moderate risk of bias due to potential unmeasured confounding and some missing data. |
| 4. | Adam J. Webb et al., 2022 [16] | Potential confounders (e.g., BMI, radiation dose, surgery type) were controlled for, but differences in grading across sites could introduce bias. | Participants were selected from multiple European sites with different protocols; inclusion criteria were consistent. | Interventions (treatment times) were classified accurately based on solar time; however, not all sites provided consistent timing. | Patients were not randomly assigned to treatment times; treatment time was determined by availability or patient choice. | Missing data were not imputed; incomplete records were omitted, which could bias results. | Outcome measures (e.g., erythema and atrophy) were assessed according to standard protocols but with potential inter-site variability. | Multiple statistical models were tested, and not all were reported; there is a risk of selective reporting. | Based on the domains assessed, the overall risk of bias for this study is rated as “Serious.” The lack of randomization in treatment time assignment and potential variability in outcome measurement across multiple sites are significant sources of bias. |
| 5. | Sebastian Reuther et al., 2015 [19] | The study accounted for known confounders, such as the genes involved in the ROS pathway, DNA repair, and TGFB signalling. However, some potential confounders related to clinical endpoints may not have been adequately adjusted for. | The study included well-defined groups of breast cancer patients who underwent radiotherapy. Ethical approval was obtained, and inclusion criteria were clearly reported. | SNPs were classified based on the prior literature and categorized into pathways, but the approach used to weigh the SNPs could introduce bias, particularly if weighting were not validated externally. | No deviations from intended interventions were reported. The study protocol has been followed consistently. | Some SNPs failed quality control and were excluded from the analysis, which may introduce bias if missingness was not random. | Outcome measurements (RTOG and LENT/SOMA scores for erythema and fibrosis) were well documented, but inter-observer variability and the subjective nature of assessments could introduce some bias. | Multiple statistical models were used without correction for multiple tests. The decision to include or exclude SNPs based on single-SNP analysis could have also introduced selection bias. | While the study had some strengths, including clear endpoints and well-documented methodology, potential bias was introduced by issues related to SNP selection, handling of missing data, and lack of adjustment for multiple testing. |
References
- De Rose, F.; De Santis, M.C.; Lucidi, S.; Colciago, R.R.; Marino, L.; Cucciarelli, F.; La Rocca, E.; Di Pressa, F.; Lohr, F.; Vanoni, V.; et al. Dose constraints in breast cancer radiotherapy. A critical review. Radiother. Oncol. 2024, 202, 110591. [Google Scholar] [CrossRef] [PubMed]
- Meattini, I.; Coles, C.E.; Tramm, T.; Borghesi, S.; Krug, D.; Montero, A.; Nardone, V.; Salvestrini, V.; Valzano, M.; Valentini, V.; et al. Biomarker-Directed radiotherapy in breast cancer. JAMA Oncol. 2025, 11, 329. [Google Scholar] [CrossRef] [PubMed]
- Meehan, J.; Gray, M.; Martínez-Pérez, C.; Kay, C.; Pang, L.Y.; Fraser, J.A.; Poole, A.V.; Kunkler, I.H.; Langdon, S.P.; Argyle, D.; et al. Precision Medicine and the role of biomarkers of radiotherapy response in breast cancer. Front. Oncol. 2020, 10, 628. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, C.N.; Rosenstein, B.S.; Kerns, S.L.; Ostrer, H.; De Ruysscher, D.; Cesaretti, J.A.; Barnett, G.C.; Dunning, A.M.; Dorling, L.; West, C.M.L.; et al. Individual patient data meta-analysis shows a significant association between the ATM rs1801516 SNP and toxicity after radiotherapy in 5456 breast and prostate cancer patients. Radiother. Oncol. 2016, 121, 431–439. [Google Scholar] [CrossRef]
- Song, Y.-Z.; Han, F.-J.; Liu, M.; Xia, C.-C.; Shi, W.-Y.; Dong, L.-H. Association between Single Nucleotide Polymorphisms in XRCC3 and Radiation-Induced Adverse Effects on Normal Tissue: A Meta-Analysis. PLoS ONE 2015, 10, e0130388. [Google Scholar] [CrossRef]
- Benitez, C.M.; Knox, S.J. Harnessing genome-wide association studies to minimize adverse radiation-induced side effects. Radiat. Oncol. J. 2020, 38, 226–235. [Google Scholar] [CrossRef]
- Green, M.D.; Brenneman, R.; Powell, S.N.; Bergom, C. Harnessing the DNA repair pathway in breast cancer: Germline Mutations/Polymorphisms in breast radiation. Semin. Radiat. Oncol. 2022, 32, 298–302. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 2021, n71. [Google Scholar] [CrossRef]
- Córdoba, E.E.; Abba, M.C.; Lacunza, E.; Fernánde, E.; Güerci, A.M. Polymorphic variants in oxidative stress genes and acute toxicity in breast cancer patients receiving radiotherapy. Cancer Res. Treat. 2016, 48, 948–954. [Google Scholar] [CrossRef]
- Oliva, D.; Nilsson, M.; Strandéus, M.; Andersson, B.-Å.; Sharp, L.; Laytragoon-Lewin, N.; Lewin, F. Individual genetic variation might predict acute skin reactions in women undergoing adjuvant breast cancer radiotherapy. Anticancer Res. 2018, 38, 6763–6770. [Google Scholar] [CrossRef]
- Lee, E.; Eum, S.Y.; Slifer, S.H.; Martin, E.R.; Takita, C.; Wright, J.L.; Hines, R.B.; Hu, J.J. Association between polymorphisms in DNA damage repair genes and Radiation Therapy–Induced Early Adverse Skin Reactions in a Breast Cancer population: A Polygenic Risk Score Approach. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Jandu, H.K.; Veal, C.D.; Fachal, L.; Luccarini, C.; Aguado-Barrera, M.E.; Altabas, M.; Azria, D.; Baten, A.; Bourgier, C.; Bultijnck, R.; et al. Genome-wide association study of treatment-related toxicity two years following radiotherapy for breast cancer. Radiother. Oncol. 2023, 187, 109806. [Google Scholar] [CrossRef] [PubMed]
- Argalácsová, S.; Křížová, Ľ.; Matějů, M.; Svobodová, D.; Vočka, M. Radiation-Induced lymphopoenia and treatment outcome in hereditary breast cancer patients. Folia Biol. 2023, 69, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Batar, B.; Mutlu, T.; Bostanci, M.; Akin, M.; Tuncdemir, M.; Bese, N.; Guven, M. DNA repair and apoptosis: Roles in radiotherapy-related acute reactions in breast cancer patients. Cell. Mol. Biol. 2018, 64, 64–70. [Google Scholar] [CrossRef]
- Córdoba, E.E.; Lacunza, E.; Abba, M.C.; Fernández, E.; Güerci, A.M. Single nucleotide polymorphisms in ATM, TNF-α and IL6 genes and risk of radiotoxicity in breast cancer patients. Mutat. Res./Genet. Toxicol. Environ. Mutagen. 2018, 836, 84–89. [Google Scholar] [CrossRef]
- Webb, A.J.; Harper, E.; Rattay, T.; Aguado-Barrera, M.E.; Azria, D.; Bourgier, C.; Brengues, M.; Briers, E.; Bultijnck, R.; Chang-Claude, J.; et al. Treatment time and circadian genotype interact to influence radiotherapy side-effects. A prospective European validation study using the REQUITE cohort. eBioMedicine 2022, 84, 104269. [Google Scholar] [CrossRef]
- Cargnin, S.; Barizzone, N.; Basagni, C.; Pisani, C.; Ferrara, E.; Masini, L.; D’Alfonso, S.; Krengli, M.; Terrazzino, S. Targeted Next-Generation Sequencing for the identification of genetic predictors of Radiation-Induced late skin toxicity in breast cancer patients: A preliminary study. J. Pers. Med. 2021, 11, 967. [Google Scholar] [CrossRef]
- Grossberg, A.J.; Lei, X.; Xu, T.; Shaitelman, S.F.; Hoffman, K.E.; Bloom, E.S.; Stauder, M.C.; Tereffe, W.; Schlembach, P.J.; Woodward, W.A.; et al. Association of Transforming Growth Factor β Polymorphism C−509T With Radiation-Induced Fibrosis Among Patients With Early-Stage Breast Cancer. JAMA Oncol. 2018, 4, 1751–1757. [Google Scholar] [CrossRef]
- Reuther, S.; Szymczak, S.; Raabe, A.; Borgmann, K.; Ziegler, A.; Petersen, C.; Dikomey, E.; Hoeller, U. Association between SNPs in defined functional pathways and risk of early or late toxicity as well as individual radiosensitivity. Strahlenther. Onkol. 2014, 191, 59–66. [Google Scholar] [CrossRef]
- Jung, K.; Sabri, S.; Hanson, J.; Xu, Y.; Wang, Y.W.; Lai, R.; Abdulkarim, B.S. ElevatedARG1expression in primary monocytes-derived macrophages as a predictor of radiation-induced acute skin toxicities in early breast cancer patients. Cancer Biol. Ther. 2015, 16, 1281–1288. [Google Scholar] [CrossRef]
- Serra, H.; Da Ines, O.; Degroote, F.; Gallego, M.E.; White, C.I. Roles of XRCC2, RAD51B and RAD51D in RAD51-Independent SSA recombination. PLoS Genet. 2013, 9, e1003971. [Google Scholar] [CrossRef] [PubMed]
- Waeldner, K.; Chin, C.; Gilbo, P. Severe Radiation-Induced Brachial Plexopathy: A case report on radiation toxicity in a patient with invasive ductal carcinoma. Cureus 2024, 16, e73043. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Zhou, P.-K. DNA damage repair: Historical perspectives, mechanistic pathways and clinical translation for targeted cancer therapy. Signal Transduct. Target. Ther. 2021, 6, 254. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.R.; Bernstein, K.A. RAD-ical New Insights into RAD51 Regulation. Genes 2018, 9, 629. [Google Scholar] [CrossRef]
- Arranz-Ledo, M.; Infante, M.; Lastra, E.; Olaverri, A.; Orozco, M.; Mateo, L.C.; Martínez, N.; Hernández, L.; Durán, M. Genetic Features of Tumours Arising in the Context of Suspected Hereditary Cancer Syndromes with RAD50, RAD51C/D, and BRIP1 Germline Mutations, Results of NGS-Reanalysis of BRCA/MMR-Negative Families. Genes 2025, 16, 458. [Google Scholar] [CrossRef]
- Lee, J.-H. Targeting the ATM pathway in cancer: Opportunities, challenges and personalized therapeutic strategies. Cancer Treat. Rev. 2024, 129, 102808. [Google Scholar] [CrossRef]
- Tulbah, S.; Alabdulkarim, H.; Alanazi, M.; Parine, N.R.; Shaik, J.; Pathan, A.A.; Al-Amri, A.; Khan, W.; Warsy, A. Polymorphisms in RAD51 and their relation with breast cancer in Saudi females. OncoTargets Ther. 2016, 9, 269–277. [Google Scholar] [CrossRef]
- Tan, J.; Sun, X.; Zhao, H.; Guan, H.; Gao, S.; Zhou, P. Double-strand DNA break repair: Molecular mechanisms and therapeutic targets. MedComm 2023, 4, e388. [Google Scholar] [CrossRef]
- Sy, S.M.H.; Huen, M.S.Y.; Chen, J. PALB2 is an integral component of the BRCA complex required for homologous recombination repair. Proc. Natl. Acad. Sci. USA 2009, 106, 7155–7160. [Google Scholar] [CrossRef]
- Wang, M.; Li, W.; Tomimatsu, N.; Yu, C.H.; Ji, J.-H.; Alejo, S.; Witus, S.R.; Alimbetov, D.; Fitzgerald, O.; Wu, B.; et al. Crucial roles of the BRCA1-BARD1 E3 ubiquitin ligase activity in homology-directed DNA repair. Mol. Cell 2023, 83, 3679–3691.e8. [Google Scholar] [CrossRef]
- Zahid, S.; Dahan, M.S.E.; Iehl, F.; Fernandez-Varela, P.; Du, M.-H.L.; Ropars, V.; Charbonnier, J.B. The multifaceted roles of KU70/80. Int. J. Mol. Sci. 2021, 22, 4134. [Google Scholar] [CrossRef] [PubMed]
- Thakar, T.; Moldovan, G.-L. The emerging determinants of replication fork stability. Nucleic Acids Res. 2021, 49, 7224–7238. [Google Scholar] [CrossRef] [PubMed]
- Vinnikov, V.; Hande, M.P.; Wilkins, R.; Wojcik, A.; Zubizarreta, E.; Belyakov, O. Prediction of the acute or late radiation toxicity effects in radiotherapy patients using ex vivo induced biodosimetric markers: A review. J. Pers. Med. 2020, 10, 285. [Google Scholar] [CrossRef] [PubMed]
- Imamichi, S.; Sharma, M.K.; Kamdar, R.P.; Fukuchi, M.; Matsumoto, Y. Ionizing radiation-induced XRCC4 phosphorylation is mediated through ATM in addition to DNA-PK. Proc. Jpn. Acad. Ser. B 2014, 90, 365–372. [Google Scholar] [CrossRef]
- Bermúdez-Guzmán, L.; Blanco-Saborío, A.; Ramírez-Zamora, J.; Lovo, E. The time for chronotherapy in Radiation Oncology. Front. Oncol. 2021, 11, 687672. [Google Scholar] [CrossRef]
- Dakup, P.P.; Porter, K.I.; Gajula, R.P.; Goel, P.N.; Cheng, Z.; Gaddameedhi, S. The circadian clock protects against ionizing radiation-induced cardiotoxicity. FASEB J. 2020, 34, 3347–3358. [Google Scholar] [CrossRef]
- El-Tanani, M.; Rabbani, S.A.; Ali, A.A.; Alfaouri, I.G.A.; Nsairat, H.A.; Al-Ani, I.H.; Aljabali, A.A.; Rizzo, M.; Patoulias, D.; Khan, M.A.; et al. Circadian rhythms and cancer: Implications for timing in therapy. Discov. Oncol. 2024, 15, 767. [Google Scholar] [CrossRef]
- Nelson, N.; Lombardo, J.; Matlack, L.; Smith, A.; Hines, K.; Shi, W.; Simone, N.L. Chronoradiobiology of Breast cancer: The time is now to link circadian rhythm and radiation biology. Int. J. Mol. Sci. 2022, 23, 1331. [Google Scholar] [CrossRef]
- Alnasser, S.M. The role of glutathione S-transferases in human disease pathogenesis and their current inhibitors. Genes Dis. 2024, 12, 101482. [Google Scholar] [CrossRef]
- Kim, W.; Lee, S.; Seo, D.; Kim, D.; Kim, K.; Kim, E.; Kang, J.; Seong, K.M.; Youn, H.; Youn, B. Cellular stress responses in radiotherapy. Cells 2019, 8, 1105. [Google Scholar] [CrossRef]
- Liu, R.; Bian, Y.; Liu, L.; Liu, L.; Liu, X.; Ma, S. Molecular pathways associated with oxidative stress and their potential applications in radiotherapy (Review). Int. J. Mol. Med. 2022, 49, 65. [Google Scholar] [CrossRef] [PubMed]
- De Aguiar, B.R.L.; Guerra, E.N.S.; Reis, P.E.D.D. Radiogenomics: A Personalized strategy for predicting Radiation-Induced Dermatitis. In IntechOpen eBooks; IntechOpen: London, UK, 2023. [Google Scholar] [CrossRef]
- Lei, G.; Mao, C.; Yan, Y.; Zhuang, L.; Gan, B. Ferroptosis, radiotherapy, and combination therapeutic strategies. Protein Cell 2021, 12, 836–857. [Google Scholar] [CrossRef] [PubMed]
- Lei, G.; Zhang, Y.; Koppula, P.; Liu, X.; Zhang, J.; Lin, S.H.; Ajani, J.A.; Xiao, Q.; Liao, Z.; Wang, H.; et al. The role of ferroptosis in ionizing radiation-induced cell death and tumor suppression. Cell Res. 2020, 30, 146–162. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Peng, Y.; Cao, L.; Chen, Y.; Li, K.; Fu, B. Correlations between serum IL-6 levels and radiation pneumonitis in lung cancer patients: A Meta-Analysis. J. Clin. Lab. Anal. 2014, 30, 145–154. [Google Scholar] [CrossRef]
- Kainthola, A.; Haritwal, T.; Tiwari, M.; Gupta, N.; Parvez, S.; Tiwari, M.; Prakash, H.; Agrawala, P.K. Immunological aspect of Radiation-Induced pneumonitis, current treatment strategies, and future prospects. Front. Immunol. 2017, 8, 506. [Google Scholar] [CrossRef]
- Li, T.; Chen, Z.J. The cGAS–cGAMP–STING pathway connects DNA damage to inflammation, senescence, and cancer. J. Exp. Med. 2018, 215, 1287–1299. [Google Scholar] [CrossRef]
- Bose, D. CGAS/STING Pathway in Cancer: Jekyll and Hyde Story of cancer immune response. Int. J. Mol. Sci. 2017, 18, 2456. [Google Scholar] [CrossRef]
- Zheng, Z.; Su, J.; Bao, X.; Wang, H.; Bian, C.; Zhao, Q.; Jiang, X. Mechanisms and applications of radiation-induced oxidative stress in regulating cancer immunotherapy. Front. Immunol. 2023, 14, 1247268. [Google Scholar] [CrossRef]
- Wang, B.; Wei, J.; Meng, L.; Wang, H.; Qu, C.; Chen, X.; Xin, Y.; Jiang, X. Advances in pathogenic mechanisms and management of radiation-induced fibrosis. Biomed. Pharmacother. 2020, 121, 109560. [Google Scholar] [CrossRef]
- Chumsuwan, N.; Khongkow, P.; Kaewsuwan, S.; Kanokwiroon, K. Interruptin C, a Radioprotective Agent, Derived from Cyclosorus terminans Protect Normal Breast MCF-10A and Human Keratinocyte HaCaT Cells against Radiation-Induced Damage. Molecules 2022, 27, 3298. [Google Scholar] [CrossRef]
- Najafi, M.; Shirazi, A.; Motevaseli, E.; Geraily, G.; Norouzi, F.; Heidari, M.; Rezapoor, S. The melatonin immunomodulatory actions in radiotherapy. Biophys. Rev. 2017, 9, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.L.; Xie, R.L.; Chen, J.C.; Ye, Y.S. Reducing contrast media extravasation during dynamic CT scanning by combined dexamethasone acetate cream and massage. Int. J. Radiat. Res. 2024, 22, 509–513. [Google Scholar] [CrossRef]
- Kerns, S.L.; Hall, W.A.; Marples, B.; West, C.M.L. Normal Tissue toxicity prediction: Clinical translation on the horizon. Semin. Radiat. Oncol. 2023, 33, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Drobin, K.; Marczyk, M.; Halle, M.; Danielsson, D.; Papiez, A.; Sangsuwan, T.; Bendes, A.; Hong, M.-G.; Qundos, U.; Harms-Ringdahl, M.; et al. Molecular Profiling for Predictors of Radiosensitivity in Patients with Breast or Head-and-Neck Cancer. Cancers 2020, 12, 753. [Google Scholar] [CrossRef]
- Abdollahi, E.; Mozdarani, H. Epigenetic regulation of circ-HIPK3, circ-PVT1, miR-25, and miR-149 in radiosensitivity of breast cancer. Exp. Mol. Pathol. 2023, 132–133, 104865. [Google Scholar] [CrossRef]
- Abdollahi, E.; Mozdarani, H.; Alizadeh, B.Z. Role of circ-FOXO3 and miR-23a in radiosensitivity of breast cancer. Breast Cancer 2023, 30, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Bakhtari, N.; Mozdarani, H.; Salimi, M.; Omranipour, R. Association study of miR-22 and miR-335 expression levels and G2 assay related inherent radiosensitivity in peripheral blood of ductal carcinoma breast cancer patients. Neoplasma 2021, 68, 190–199. [Google Scholar] [CrossRef]
- Dulong, J.; Kouakou, C.; Mesloub, Y.; Rorteau, J.; Moratille, S.; Chevalier, F.P.; Vinasco-Sandoval, T.; Martin, M.T.; Lamartine, J. NFATC2 modulates radiation sensitivity in dermal fibroblasts from patients with severe side effects of radiotherapy. Front. Oncol. 2020, 10, 589168. [Google Scholar] [CrossRef]
- Cui, Y.; Li, B.; Pollom, E.L.; Horst, K.C.; Li, R. Integrating radiosensitivity and immune gene signatures for predicting benefit of radiotherapy in breast cancer. Clin. Cancer Res. 2018, 24, 4754–4762. [Google Scholar] [CrossRef]
- Modlin, L.A.; Flynn, J.; Zhang, Z.; Cahlon, O.; Mueller, B.; Khan, A.J.; Gillespie, E.F.; McCormick, B.; Stadler, Z.K.; Robson, M.E.; et al. Tolerability of breast radiotherapy among carriers of ATM germline variants. JCO Precis. Oncol. 2021, 5, 227–234. [Google Scholar] [CrossRef]
- Huszno, J.; Budryk, M.; Kołosza, Z.; Nowara, E. The Influence of BRCA1/BRCA2 Mutations on Toxicity Related to Chemotherapy and Radiotherapy in Early Breast Cancer Patients. Oncology 2013, 85, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Drooger, J.C.; Akdeniz, D.; Pignol, J.-P.; Koppert, L.B.; McCool, D.; Seynaeve, C.M.; Hooning, M.J.; Jager, A. Adjuvant radiotherapy for primary breast cancer in BRCA1 and BRCA2 mutation carriers and risk of contralateral breast cancer with special attention to patients irradiated at younger age. Breast Cancer Res. Treat. 2015, 154, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Naderi, E.; Aguado-Barrera, M.E.; Schack, L.M.H.; Dorling, L.; Rattay, T.; Fachal, L.; Summersgill, H.; Martínez-Calvo, L.; Welsh, C.; Dudding, T.; et al. Large-scale meta–genome-wide association study reveals common genetic factors linked to radiation-induced acute toxicities across cancer types. JNCI Cancer Spectr. 2023, 7, pkad088. [Google Scholar] [CrossRef] [PubMed]
- Weigel, C.; Veldwijk, M.R.; Oakes, C.C.; Seibold, P.; Slynko, A.; Liesenfeld, D.B.; Rabionet, M.; Hanke, S.A.; Wenz, F.; Sperk, E.; et al. Epigenetic regulation of diacylglycerol kinase alpha promotes radiation-induced fibrosis. Nat. Commun. 2016, 7, 10893. [Google Scholar] [CrossRef]
- Nuta, O.; Somaiah, N.; Boyle, S.; Chua, M.L.K.; Gothard, L.; Yarnold, J.; Rothkamm, K.; Herskind, C. Correlation between the radiation responses of fibroblasts cultured from individual patients and the risk of late reaction after breast radiotherapy. Cancer Lett. 2016, 374, 324–330. [Google Scholar] [CrossRef]
- Fuentes-Raspall, M.J.; Caragol, I.; Alonso, C.; Cajal, T.R.Y.; Fisas, D.; Seoane, A.; Carvajal, N.; Bonache, S.; Díez, O.; Gutiérrez-Enríquez, S. Apoptosis for prediction of radiotherapy late toxicity: Lymphocyte subset sensitivity and potential effect of TP53 Arg72Pro polymorphism. Apoptosis 2014, 20, 371–382. [Google Scholar] [CrossRef]
| No. Crt. | Author, Year of Publication [Ref.] | Gene (SNP), OR (p) | Studied Radiotherapy-Induced Toxicity | Authors’ Conclusions | Forest Plot Study No. |
|---|---|---|---|---|---|
| 1. | Elisa Eugenia Córdoba et al., 2016 [9] | GSTP1 (rs1695) 1.08 (p = 0.88) | Acute skin toxicity (Grade 2+) | No solid evidence was found for an association between any SNP and acute toxicity. | Acute—Study 1 |
| GSTP1 (rs1695) 1.83 (p = 0.27) | Acute—Study 2 | ||||
| SOD2 (rs4880) 0.63 (p = 0.39) | Acute—Study 3 | ||||
| SOD2 (rs4880) 0.73 (p = 0.57) | Acute—Study 4 | ||||
| NOS3 (rs1799983) 0.70 (p = 0.45) | Acute—Study 5 | ||||
| NOS3 (rs1799983) 1.14 (p = 0.82) | Acute—Study 6 | ||||
| GSTA1 (rs3957356) 1.71 (p = 0.36) | Acute—Study 7 | ||||
| GSTA1 (rs3957356) 1.54 (p = 0.46) | Acute—Study 8 | ||||
| 2. | Delmy Oliva et al., 2018 [10] | XRCC2 (rs2040639) 6.70 (p = 0.007) | Acute radiation skin reactions (ARSR): itching, burning, irritation | XRCC2 rs2040639 SNP associated with burning as ARSR. | Acute—Study 9 |
| IFNG (rs2069705) 3.10 (p = 0.01) | IFNG rs2069705 SNP associated with itching as ARSR. | Acute—Study 10 | |||
| 3. | Eunkyung Lee et al., 2020 [11] | ATM (rs61915066) 2.64 (p = 0.004) | Early adverse skin reactions (EASR), moist desquamation | ATM (rs61915066) associated with RT-induced EASR. | Acute—Study 11 |
| CHEK1 (rs11220184) 1.69 (p = 0.013) | CHEK1 (rs11220184) associated with RT-induced EASR. | Acute—Study 12 | |||
| ERCC2 (rs60152947) 0.42 (p = 0.007) | ERCC2 variants associated with reduced risk of RT-induced EASR. | Acute—Study 13 | |||
| ERCC2 (rs10404465) 0.59 (p = 0.007) | Acute—Study 14 | ||||
| ERCC2 (rs1799786) 1.74 (p = 0.007) | Acute—Study 15 | ||||
| TGFB1 (rs4803455) 1.50 (p = 0.025) | TGFB1 variants associated with RT-induced EASR. | Acute—Study 16 | |||
| TGFB1 (rs2241714) 0.57 (p = 0.04) | Acute—Study 17 | ||||
| RAD51C (rs302877) 0.59 (p = 0.006) | RAD51C variants associated with reduced risk of RT-induced EASR. | Acute—Study 18 | |||
| RAD51C (rs405684) 1.60 (p = 0.07) | Acute—Study 19 | ||||
| 4. | Harkeran K. Jandu et al., 2023 [12] | GPC5 (rs145328458) 1.23 (p = 1.06 × 10−9) | Oedema Grade ≥ 2 (2-year follow-up) | A significant association was identified between GPC5 rs145328458 and oedema Grade ≥ 2. | Acute—Study 20 |
| GPC5 (rs61966612) 1.23 (p = 1.23 × 10−9) | A significant association was identified for GPC5 rs61966612 with oedema Grade ≥ 2. | Acute—Study 21 | |||
| AC093240.1 (rs12657177) 1.24 (p = 1.12 × 10−10) | A significant association was identified for AC093240.1 rs12657177 with oedema Grade ≥ 2. | Acute—Study 22 | |||
| AC093240.1 (rs75912034) 1.24 (p = 1.21 × 10−10) | A significant association was identified for AC093240.1 rs73151332 with oedema Grade ≥ 2. | Acute—Study 23 | |||
| 5 | Soňa Argalácsová et al., 2023 [13] | BRCA1, BRCA2 1.74 (p = 0.50) | Acute dermatitis, lymphedema | There is no evidence of increased radiation-induced toxicity for BRCA1/BRCA2 PV carriers. | Acute—Study 24 |
| CHEK2, ATM, PALB2, RAD51C, RAD51D, BARD1, TP53, FANCM 5.29 (p = 0.41) | There is no evidence of increased radiation-induced toxicity for OTHER-PV carriers. | Acute—Study 25 | |||
| 6. | Bahadir Batar et al., 2018 [14] | ERCC1 (rs3212986) 0.21 (p < 0.001) | Acute skin reactions | ERCC1 rs3212986 CC genotype may protect radiotherapy-induced acute reactions. | Acute—Study 26 |
| XPC (rs3731055) 1.00 (p = 1.00) | There is no evidence of an association between XPC rs3731055 and radiotherapy-induced acute reactions. | Acute—Study 27 | |||
| 7. | Elisa E. Córdoba et al., 2018 [15] | TNF-α (rs1800629) 5.83 (p = 0.22) | Severe radiodermatitis (grades 3 and 4) | There is no evidence of an association between TNF-α (rs1800629) polymorphism and severe radiodermatitis. | Acute—Study 28 |
| IL-6 (rs1800795) 2.16 (p = 0.54) | There is no evidence of an association between IL-6 (rs1800795) polymorphism and severe radiodermatitis. | Acute—Study 29 | |||
| ATM (rs1801516) 0.72 (p = 0.68) | There is no evidence of an association between ATM (rs1801516) polymorphism and severe radiodermatitis. | Acute—Study 30 | |||
| 8. | Adam J. Webb et al., 2022 [16] | PER3 (rs2087947) 1.27 (p = 0.02) | Acute erythema | PER3 rs2087947 genotype influences the occurrence of acute erythema. | Acute—Study 31 |
| No. Crt. | Author, Year of Publication [Ref.] | Gene (SNP), OR (p) | Radiotherapy-Induced Toxicity | Authors’ Conclusions | Forest Plot Study No. |
|---|---|---|---|---|---|
| 1 | Cargnin et al., 2021 [17] | TP53 (rs1042522), 1.79 (p = 0.028) | Subcutaneous fibrosis and/or telangiectasia (grade 2–3) | No definitive association was established; further studies are required with larger cohorts. | Late—Study 1 |
| ERCC2 (rs1052555), 1.02 (p = 0.922) | Late—Study 2 | ||||
| ERCC2 (rs13181), 0.90 (p = 0.595) | Late—Study 3 | ||||
| LIG1 (rs7246696), 0.99 (p = 0.971) | Late—Study 4 | ||||
| 2 | Harkeran K. Jandu et al., 2023 [12] | PAX7 (rs643644), 1.40 (p = 3.54 × 10−8) | Arm lymphoedema G1 | PAX7 is associated with an increased risk of arm lymphoedema; replication is recommended. | Late—Study 5 |
| ATXN7L1 (rs11345494), 1.13 (p = 5.78 × 10−8) | ATXN7L1 is associated with an increased risk of arm lymphoedema. | Late—Study 6 | |||
| ANOS1 (rs188287402), 1.14 (p = 2.80 × 10−8) | Nipple retraction G2 | ANOS1 is associated with an increased risk of nipple retraction. | Late—Study 7 | ||
| CRYM/ANKS4B (rs12443861), 1.20 (p = 6.17 × 10−8) | Telangiectasia G1 | CRYM/ANKS4B is associated with an increased risk of telangiectasia. | Late—Study 8 | ||
| SLC10A4 (rs34063419), 1.71 (p = 1.21 × 10−8) | Induration G2 | SLC10A4 is associated with an increased risk of induration. | Late—Study 9 | ||
| LINC01779 (rs77311050), 1.34 (p = 2.54 × 10−8) | LINC01779 is associated with an increased risk of induration. | Late—Study 10 | |||
| 3 | Aaron J. Grossberg et al., 2018 [18] | TGFB1 (rs1800469), 4.47 (p = 0.02) | Subcutaneous fibrosis (grade 2+) | The C−509T allele in TGFB1 is associated with an increased risk of grade 2 or higher fibrosis. Genetic profiling of TGFB1 may help guide treatment decisions. | Late—Study 11 |
| 4 | Adam J. Webb et al., 2022 [16] | CLOCK (rs1801260), 0.62 (p < 0.01) | Late atrophy (2 years post-radiotherapy) | CLOCK (rs1801260), PER3 (rs2087947), and RASD1 (rs11545787) associated with reduced risk of late atrophy (2 years post-radiotherapy). | Late—Study 12 |
| PER3 (rs2087947), 0.65 (p = 0.04) | Late—Study 13 | ||||
| RASD1 (rs11545787), 0.56 (p = 0.02) | Late—Study 14 | ||||
| 5 | Sebastian Reuther et al., 2015 [19] | ROS Pathway, 1.58 (p = 0.045) | Subcutaneous fibrosis | ROS pathway genes have a minor impact on fibrosis but are significant when using a weighted risk model. | Late—Study 15 |
| DNA Repair, 2.92 (p = 0.023) | DNA repair pathway genes are strongly associated with fibrosis using a weighted risk model. | Late—Study 16 | |||
| TGFB1 Signaling, 2.68 (p = 0.005) | A TGFB1 signaling pathway is strongly associated with fibrosis when using a weighted risk model. | Late—Study 17 |
| No. Crt. | Author, Year of Publication [Ref.] | Gene (SNP)—OR (p) | Studied Radiotherapy-Induced Toxicity |
|---|---|---|---|
| 1. | Delmy Oliva et al., 2018 [10] | XRCC2 (rs2040639)—6.70 (p = 0.007) | Acute radiation skin reactions (ARSRs): itching, burning, irritation. |
| IFNG (rs2069705)—3.10 (p = 0.01) | |||
| 2. | Eunkyung Lee et al., 2020 [11] | ATM (rs61915066)—2.64 (p = 0.004) | Early adverse skin reactions (EASRs), moist desquamation |
| CHEK1 (rs11220184)—1.69 (p = 0.013) | |||
| ERCC2 (rs60152947)—0.42 (p = 0.007) | |||
| ERCC2 (rs10404465)—0.59 (p = 0.007) | |||
| ERCC2 (rs1799786)—1.74 (p = 0.007) | |||
| TGFB1 (rs4803455)—1.50 (p = 0.025) | |||
| TGFB1 (rs2241714)—0.57 (p = 0.04) | |||
| RAD51C (rs302877)—0.59 (p = 0.006) | |||
| RAD51C (rs405684)—1.60 (p = 0.07) | |||
| 3. | Harkeran K. Jandu et al., 2023 [12] | GPC5 (rs145328458)—1.23 (p = 1.06 × 10−9) | Oedema Grade ≥ 2 (2-year follow-up) |
| GPC5 (rs61966612)—1.23 (p = 1.23 × 10−9) | |||
| AC093240.1 (rs12657177)—1.24 (p = 1.12 × 10−10) | |||
| AC093240.1 (rs75912034)—1.24 (p = 1.21 × 10−10) | |||
| 4. | Bahadir Batar et al., 2018 [14] | ERCC1 (rs3212986)—0.21 (p < 0.001) | Acute skin reactions |
| 5. | Adam J. Webb et al., 2022 [16] | PER3 (rs2087947)—1.27 (p = 0.02) | Acute erythema |
| No. Crt. | Author, Year of Publication [Ref.] | Gene (SNP) OR (p) | Studied Radiotherapy-Induced Toxicity |
|---|---|---|---|
| 1. | Cargnin et al., 2021 [17] | TP53 (rs1042522)—1.79 (p = 0.028) | Subcutaneous fibrosis and/or telangiectasia (grade 2–3) |
| 2. | Harkeran K. Jandu et al., 2023 [12] | PAX7 (rs643644)—1.40 (p = 3.54 × 10−8) | Arm lymphoedema G1 |
| ATXN7L1 (rs11345494)—1.13 (p = 5.78 × 10−8) | |||
| ANOS1 (rs188287402)—1.14 (p = 2.80 × 10−8) | Nipple Retraction G2 | ||
| CRYM/ANKS4B (rs12443861)—1.20 (p = 6.17 × 10−8) | Telangiectasia G1 | ||
| SLC10A4 (rs34063419)—1.71 (p = 1.21 × 10−8) | Induration G2 | ||
| LINC01779 (rs77311050)—1.34 (p = 2.54 × 10−8) | |||
| 3. | Aaron J. Grossberg et al., 2018 [18] | TGFB1 (rs1800469)—4.47 (p = 0.02) | Subcutaneous fibrosis (grade 2+) |
| 4. | Adam J. Webb et al., 2022 [16] | CLOCK (rs1801260)—0.62 (p < 0.01) | Late atrophy (2 years post-radiotherapy) |
| PER3 (rs2087947)—0.65 (p = 0.04) | |||
| RASD1 (rs11545787)—0.56 (p = 0.02) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cătană, A.; Pătrășcanu, A.-A.; Martin, D.L.; Militaru, M.S.; Iordănescu, I.I.; Țîpcu, A.; Achimaș-Cadariu, P.; Pîrlog, L.-M. The Impact of Genetic Variations on Radiotherapy Toxicity in Breast Cancer Patients: A Meta-Analysis of Acute and Late Skin Adverse Effects. Cancers 2025, 17, 1880. https://doi.org/10.3390/cancers17111880
Cătană A, Pătrășcanu A-A, Martin DL, Militaru MS, Iordănescu II, Țîpcu A, Achimaș-Cadariu P, Pîrlog L-M. The Impact of Genetic Variations on Radiotherapy Toxicity in Breast Cancer Patients: A Meta-Analysis of Acute and Late Skin Adverse Effects. Cancers. 2025; 17(11):1880. https://doi.org/10.3390/cancers17111880
Chicago/Turabian StyleCătană, Andreea, Andrada-Adelaida Pătrășcanu, Daniela Laura Martin, Mariela Sanda Militaru, Irina Ioana Iordănescu, Alexandru Țîpcu, Patriciu Achimaș-Cadariu, and Lorin-Manuel Pîrlog. 2025. "The Impact of Genetic Variations on Radiotherapy Toxicity in Breast Cancer Patients: A Meta-Analysis of Acute and Late Skin Adverse Effects" Cancers 17, no. 11: 1880. https://doi.org/10.3390/cancers17111880
APA StyleCătană, A., Pătrășcanu, A.-A., Martin, D. L., Militaru, M. S., Iordănescu, I. I., Țîpcu, A., Achimaș-Cadariu, P., & Pîrlog, L.-M. (2025). The Impact of Genetic Variations on Radiotherapy Toxicity in Breast Cancer Patients: A Meta-Analysis of Acute and Late Skin Adverse Effects. Cancers, 17(11), 1880. https://doi.org/10.3390/cancers17111880