
The Influence of Radioligand Therapy on Immunogenicity Against SARS-CoV-2—A Retrospective Single-Arm Cohort Study of Metastatic Prostate Cancer Patients Receiving PSMA Radioligand Therapy †

 , ,
, ,
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
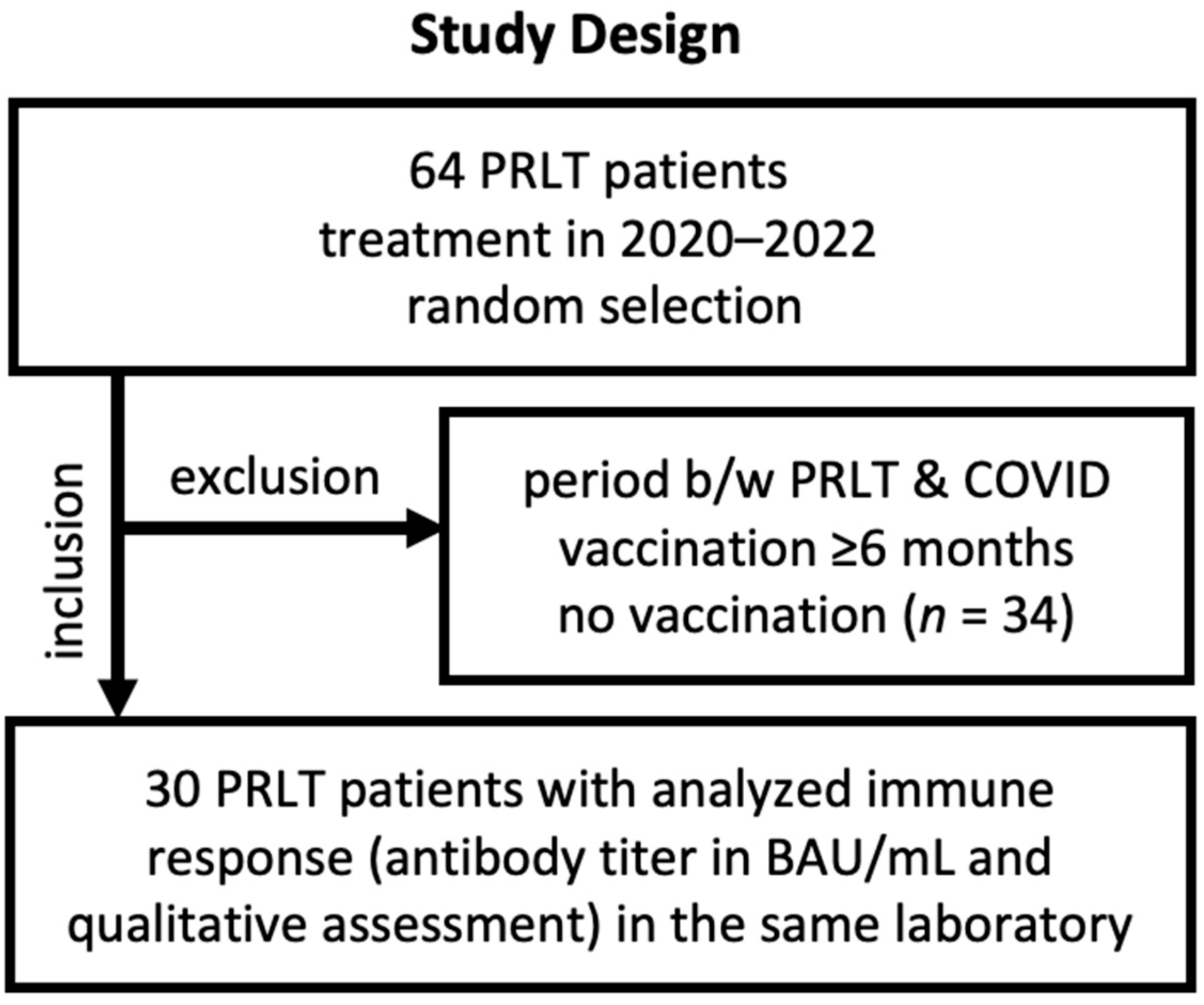
2.1. Patient Selection and Characteristics
2.2. Evaluation of Serological Response
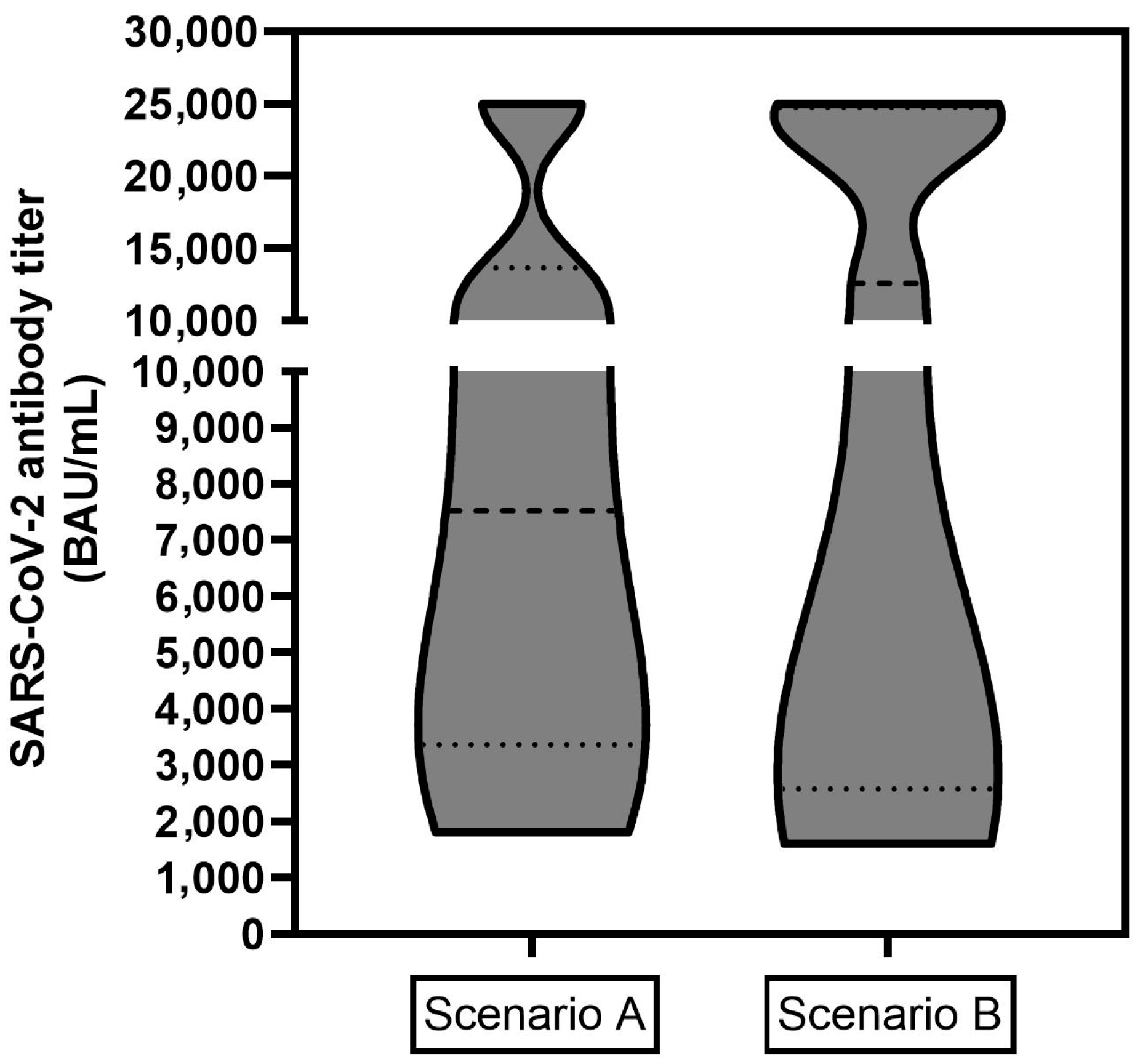
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCO | American Society of Clinical Oncology |
| CAR | chimeric antigen receptor |
| CLL | chronic lymphocytic leukemia |
| COVID-19 | coronavirus disease 2019 |
| CDC | Centers of Disease Control and Prevention |
| ESMO | European Society for Medical Oncology |
| mCRPC | metastatic castration resistant prostate cancer |
| mRNA | messenger ribonucleic acid |
| PRLT | PSMA-directed radioligand therapy |
| PSMA | prostate-specific membrane antigen |
| RLT | radioligand therapy |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
References
- Garassino, M.C.; Vyas, M.; de Vries, E.G.E.; Kanesvaran, R.; Giuliani, R.; Peters, S.; European Society for Medical Oncology. The ESMO Call to Action on COVID-19 vaccinations and patients with cancer: Vaccinate. Monitor. Educate. Ann. Oncol. 2021, 32, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, M.; Bohlke, K.; Baptiste, D.M.; Dunleavy, K.; Fueger, A.; Jones, L.; Kelkar, A.H.; Law, L.Y.; LeFebvre, K.B.; Ljungman, P.; et al. Vaccination of Adults With Cancer: ASCO Guideline. J. Clin. Oncol. 2024, 42, 1699–1721. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, F.; Daher, M.; Spallone, A.; Chemaly, R.F. COVID-19 Vaccination in Patients With Cancer and Recipients of Cellular Therapy. Oncology 2023, 37, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Charla, Y.; Kalra, M.; Chopra, N.; Choudhury, S. COVID-19 vaccination in pediatric cancer patients: A high priority. Pediatr. Blood Cancer 2021, 68, e29397. [Google Scholar] [CrossRef]
- Rajan, S.; Akhtar, N.; Sharma, S.; Chakrabarti, D.; Kumar, V. COVID-19 vaccination for cancer patients: Evidence, priority, and practice. Vaccine 2021, 39, 5075–5077. [Google Scholar] [CrossRef]
- Ribas, A.; Sengupta, R.; Locke, T.; Zaidi, S.K.; Campbell, K.M.; Carethers, J.M.; Jaffee, E.M.; Wherry, E.J.; Soria, J.C.; D’Souza, G.; et al. Priority COVID-19 Vaccination for Patients with Cancer while Vaccine Supply Is Limited. Cancer Discov. 2021, 11, 233–236. [Google Scholar] [CrossRef]
- Mandal, A.; Singh, P.; Samaddar, A.; Singh, D.; Verma, M.; Rakesh, A.; Ranjan, R. Vaccination of cancer patients against COVID-19: Towards the end of a dilemma. Med. Oncol. 2021, 38, 92. [Google Scholar] [CrossRef] [PubMed]
- Tran, S.; Truong, T.H.; Narendran, A. Evaluation of COVID-19 vaccine response in patients with cancer: An interim analysis. Eur. J. Cancer 2021, 159, 259–274. [Google Scholar] [CrossRef]
- Yin, J.; Chen, Y.; Li, Y.; Zhang, X.; Wang, C. Seroconversion rate after COVID-19 vaccination in patients with solid cancer: A systematic review and meta-analysis. Hum. Vaccin. Immunother. 2022, 18, 2119763. [Google Scholar] [CrossRef]
- Seneviratne, S.L.; Yasawardene, P.; Wijerathne, W.; Somawardana, B. COVID-19 vaccination in cancer patients: A narrative review. J. Int. Med. Res. 2022, 50, 3000605221086155. [Google Scholar] [CrossRef]
- Hall, V.G.; Teh, B.W. COVID-19 Vaccination in Patients With Cancer and Patients Receiving HSCT or CAR-T Therapy: Immune Response, Real-World Effectiveness, and Implications for the Future. J. Infect. Dis. 2023, 228, S55–S69. [Google Scholar] [CrossRef]
- Davis-Porada, J.; George, A.B.; Lam, N.; Caron, D.P.; Gray, J.I.; Huang, J.; Hwu, J.; Wells, S.B.; Matsumoto, R.; Kubota, M.; et al. Maintenance and functional regulation of immune memory to COVID-19 vaccines in tissues. Immunity 2024, 57, 2895–2913.e8. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Iacono, D.; Cerbone, L.; Palombi, L.; Cavalieri, E.; Sperduti, I.; Cocchiara, R.A.; Mariani, B.; Parisi, G.; Garufi, C. Serological response to COVID-19 vaccination in patients with cancer older than 80 years. J. Geriatr. Oncol. 2021, 12, 1253–1255. [Google Scholar] [CrossRef]
- Agha, M.; Blake, M.; Chilleo, C.; Wells, A.; Haidar, G. Suboptimal response to COVID-19 mRNA vaccines in hematologic malignancies patients. medRxiv 2021. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfo, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef]
- Perry, C.; Luttwak, E.; Balaban, R.; Shefer, G.; Morales, M.M.; Aharon, A.; Tabib, Y.; Cohen, Y.C.; Benyamini, N.; Beyar-Katz, O.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with B-cell non-Hodgkin lymphoma. Blood Adv. 2021, 5, 3053–3061. [Google Scholar] [CrossRef]
- Stampfer, S.D.; Goldwater, M.S.; Jew, S.; Bujarski, S.; Regidor, B.; Daniely, D.; Chen, H.; Xu, N.; Li, M.; Green, T.; et al. Response to mRNA vaccination for COVID-19 among patients with multiple myeloma. Leukemia 2021, 35, 3534–3541. [Google Scholar] [CrossRef]
- Grinshpun, A.; Rottenberg, Y.; Ben-Dov, I.Z.; Djian, E.; Wolf, D.G.; Kadouri, L. Serologic response to COVID-19 infection and/or vaccine in cancer patients on active treatment. ESMO Open 2021, 6, 100283. [Google Scholar] [CrossRef]
- Shmueli, E.S.; Lawrence, Y.R.; Rahav, G.; Itay, A.; Lustig, Y.; Halpern, N.; Boursi, B.; Margalit, O. Serological response to a third booster dose of BNT162b2 COVID-19 vaccine among seronegative cancer patients. Cancer Rep. 2022, 5, e1645. [Google Scholar] [CrossRef]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.W.; Le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: A longitudinal study. Lancet Microbe 2021, 2, e240–e249. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Ruckert, M.; Flohr, A.S.; Hecht, M.; Gaipl, U.S. Radiotherapy and the immune system: More than just immune suppression. Stem Cells 2021, 39, 1155–1165. [Google Scholar] [CrossRef]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- ECDC/EMA. ECDC and EMA Update Recommendations on Additional Booster Doses of mRNA COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/news/ecdc-ema-update-recommendations-additional-booster-doses-mrna-covid-19-vaccines (accessed on 26 September 2021).
- CDC. COVID-19 Vaccine—Interim COVID-19 Immunization Schedule. Available online: https://www.cdc.gov/vaccines/covid-19/downloads/COVID-19-immunization-schedule-ages-6months-older.pdf (accessed on 26 September 2022).
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwobel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Kramer, C.S.; Eismant, A.; Mishra, A.; Müller, C.; Landvogt, C.; Baum, R.P. The Influence of Radioligand Therapy on Immunogenicity against SARS-CoV-2. In Proceedings of the SNMMI 2023, Chicago, IL, USA, 24–27 July 2023. Poster. [Google Scholar]
- Kramer, C.S.; Eismant, A.; Mishra, A.; Greifenstein, L.; Müller, C.; Landvogt, C.; Baum, R.P. Einfluss der PSMA-Radioligandentherapie (PRLT) auf die Immunogenität einer Impfung gegen SARS-CoV-2—Eine retrospektive einarmige Kohortenstudie bei Patienten mit metastasierten Prostatakarzinomen. In Proceedings of the German Society of Nuclear Medicine (DGN) Congress 2023, Leipzig, Germany, 19–22 April 2023. Poster, Abstract in: Nuklearmedizin 2023, 62, 142–143. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Sex | Male = 30 |
| Age 1 | Mean: 70.6 years, Span: 56–86 |
| Tumor | mCRPC |
| RLT cycles 2 | Modal value: 2, Span: 1–4 |
| Regimen | Patients receiving lutetium-177-PSMA-I&T: 24 Patients receiving lutetium-177-PSMA-I&T and/or TANDEM therapy: 6 Cumulative mean activity of lutetium-177: 16.1 ± 7.2 GBq (435.1 ± 194.6 mCi)/patient Cumulative mean activity of actinium-225: 13.7 ± 6.6 MBq (0.37 ± 0.18 mCi)/patient (TANDEM) Administered lutetium-177-PSMA cycles: 57 (1.9 per patient) Administered TANDEM cycles: 10 (1.7 per TANDEM patient) |
| Vaccinations | Modal value: 3, Span: 1–4 |
| Vaccines (drug developer) | BioNTech-Pfizer:34 Moderna: 11 AstraZeneca-Oxford: 9 Johnson & Johnson (Janssen): 1 Unknown: 27 Confirmed COVID-19 infections: 4 |
| Radioligand Therapy (Cumulative Administered Activity) | COVID-19 Vaccination | ||||||
|---|---|---|---|---|---|---|---|
| Pat. | Age 1 | Cycles | Lutetium-177, GBq (mCi) | Actinium-225, MBq (mCi) | Doses | Vaccines (Drug Developer) or Infection | Seroresponse |
| 1 | 85 | 2 | 15.1 (408.1) | - | 3 | BNT, BNT, BNT | + |
| 2 | 69 | 3 | 22.5 (608.1) | - | 1 | C, BNT | + |
| 3 | 53 | 4 | 20.1 (543.2) | 23.7 (0.64) | 3 | BNT, BNT, BNT | + |
| 4 | 65 | 2 | 16.1 (435.1) | - | 2 | BNT, BNT | + |
| 5 | 69 | 2 | 15.6 (421.6) | 12.0 (0.32) | 3 | U, BNT, BNT | + |
| 6 | 73 | 2 | 18.0 (486.5) | 16.7 (0.45) | 3 | U, U, BNT | + |
| 7 | 85 | 2 | 13.4 (362.2) | - | 3 | U, U, BNT | + |
| 8 | 71 | 2 | 15.5 (418.9) | - | 3 | U, U, BNT | + |
| 9 | 73 | 2 | 18.4 (497.3) | - | 2 | MD, MD | + |
| 10 | 65 | 1 | 8.7 (235.1) | - | 3 | AZ, AZ, BNT | + (b) |
| 11 | 78 | 2 | 17.5 (473.0) | - | 3 | C, U, U, BNT | + |
| 12 | 68 | 2 | 14.5 (391.9) | - | 3 | U, AZ, MD | + |
| 13 | 69 | 3 | 19.4 (524.3) | - | 3 | MD, MD, MD | + |
| 14 | 63 | 1 | 6.3 (170.3) | - | 3 | BNT, BNT, BNT | - |
| 15 | 77 | 1 | 12.8 (346.0) | - | 2 | C, MD, MD | + |
| 16 | 70 | 4 | 30.1 (813.5) | 4.7 (0.13) | 3 | U, BNT, BNT | + |
| 17 | 66 | 2 | 17.4 (470.3) | - | 3 | U, AZ, BNT | + |
| 18 | 68 | 2 | 16.0 (432.4) | - | 3 | AZ, AZ, MD | + |
| 19 | 72 | 4 | 30.3 (818.9) | - | 1 | JNJ, C | + |
| 20 | 86 | 3 | 23.9 (645.9) | - | 3 | BNT, BNT, BNT | + |
| 21 | 62 | 3 | 15.2 (410.8) | - | 3 | U, U, BNT | + |
| 22 | 74 | 2 | 15.5 (418.9) | - | 2 | BNT, BNT | + |
| 23 | 66 | 1 | 8.9 (240.5) | - | 3 | U, U, BNT | + |
| 24 | 75 | 3 | 7.5 (707.7) | - | 3 | U, U, U | + |
| 25 | 74 | 1 | 7.5 (707.7) | - | 4 | U, U, AZ, MD | + |
| 26 | 56 | 3 | 7.0 (189.2) | - | 3 | BNT, MD, MD | + |
| 27 | 71 | 4 | 33.2 (897.3) | - | 4 | U, BNT, U, BNT | + |
| 28 | 73 | 2 | 19.7 (532.4) | - | 3 | U, U, BNT | + |
| 29 | 70 | 2 | 14.5 (391.9) | 9.0 (0.24) | 3 | U, U, BNT | + |
| 30 | 74 | 1 | 2.1 (56.8) | 16.0 (0.43) | 3 | AZ, AZ, BNT | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kramer, C.S.; Eismant, A.; Mishra, A.; Müller, C.; Landvogt, C.; Baum, R.P. The Influence of Radioligand Therapy on Immunogenicity Against SARS-CoV-2—A Retrospective Single-Arm Cohort Study of Metastatic Prostate Cancer Patients Receiving PSMA Radioligand Therapy. Cancers 2025, 17, 1865. https://doi.org/10.3390/cancers17111865
Kramer CS, Eismant A, Mishra A, Müller C, Landvogt C, Baum RP. The Influence of Radioligand Therapy on Immunogenicity Against SARS-CoV-2—A Retrospective Single-Arm Cohort Study of Metastatic Prostate Cancer Patients Receiving PSMA Radioligand Therapy. Cancers. 2025; 17(11):1865. https://doi.org/10.3390/cancers17111865
Chicago/Turabian StyleKramer, Carsten S., Aleksandr Eismant, Aditi Mishra, Corinna Müller, Christian Landvogt, and Richard P. Baum. 2025. "The Influence of Radioligand Therapy on Immunogenicity Against SARS-CoV-2—A Retrospective Single-Arm Cohort Study of Metastatic Prostate Cancer Patients Receiving PSMA Radioligand Therapy" Cancers 17, no. 11: 1865. https://doi.org/10.3390/cancers17111865
APA StyleKramer, C. S., Eismant, A., Mishra, A., Müller, C., Landvogt, C., & Baum, R. P. (2025). The Influence of Radioligand Therapy on Immunogenicity Against SARS-CoV-2—A Retrospective Single-Arm Cohort Study of Metastatic Prostate Cancer Patients Receiving PSMA Radioligand Therapy. Cancers, 17(11), 1865. https://doi.org/10.3390/cancers17111865