
Real-World Experiences Using Atezolizumab + Bevacizumab for the Treatment of Unresectable Hepatocellular Carcinoma: A Multicenter Study †


 , , , ,
, , , ,  ,
,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Data Source
2.2. Study Population
2.3. Study Measures and Outcomes
2.4. Subgroups
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Discontinuation
3.3. Receipt of EGD and HCC Treatments Prior to and After A+B
3.4. Real-World Effectiveness Outcomes
3.4.1. Clinician-Assessed Treatment Response
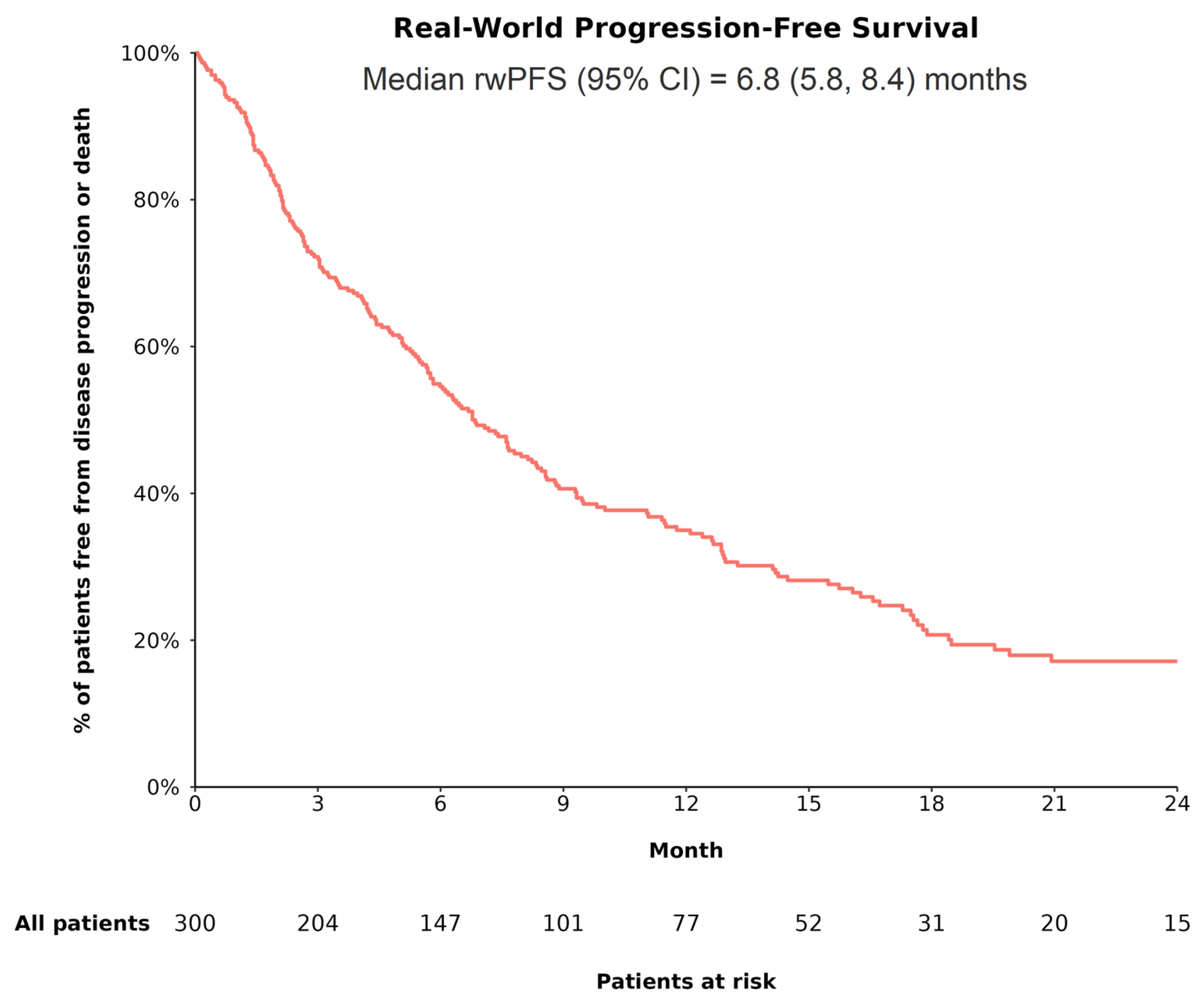
3.4.2. RwPFS
3.4.3. OS
3.5. HCC-Related Hospitalizations and ER Visits
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ntellas, P.; Chau, I. Updates on systemic therapy for hepatocellular carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2024, 44, e430028. [Google Scholar] [CrossRef] [PubMed]
- Casak, S.J.; Donoghue, M.; Fashoyin-Aje, L.; Jiang, X.; Rodriguez, L.; Shen, Y.L.; Xu, Y.; Jiang, X.; Liu, J.; Zhao, H.; et al. FDA approval summary: Atezolizumab plus bevacizumab for the treatment of patients with advanced unresectable or metastatic hepatocellular carcinoma. Clin. Cancer Res. 2021, 27, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Hepatobiliary Cancers V.2.2021; National Comprehensive Cancer Network, Inc.: Plymouth Meeting, PA, USA, 2021. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Hepatobiliary Cancers V.1.2025; National Comprehensive Cancer Network, Inc.: Plymouth Meeting, PA, USA, 2025. [Google Scholar]
- Patel, T.H.; Brewer, J.R.; Fan, J.; Cheng, J.; Shen, Y.L.; Xiang, Y.; Zhao, H.; Lemery, S.J.; Pazdur, R.; Kluetz, P.G.; et al. FDA approval summary: Tremelimumab in combination with durvalumab for the treatment of patients with unresectable hepatocellular carcinoma. Clin. Cancer Res. 2024, 30, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Khunti, K.; Harris, S.B.; Meizinger, C.; Skolnik, N.S. Interpretation and impact of real-world clinical data for the practicing clinician. Adv. Ther. 2018, 35, 1763–1774. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.K.; Van Dao, T.; De Toni, E.N.; et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022, 1, EVIDoa2100070. [Google Scholar] [CrossRef]
- Jan, J.; Osho, A.; Murphy, C.C.; Mazure, C.M.; Singal, A.G.; Rich, N.E. Gender, age, racial and ethnic disparities in clinical trial enrollment for primary liver cancer. Gastroenterology 2022, 163, 14–20.e12. [Google Scholar] [CrossRef]
- Monge, C.; Greten, T.F. Underrepresentation of Hispanics in clinical trials for liver cancer in the United States over the past 20 years. Cancer Med. 2024, 13, e6814. [Google Scholar] [CrossRef]
- Hong, J.C. Strategies to turn real-world data into real-world knowledge. JAMA Netw. Open 2021, 4, e2128045. [Google Scholar] [CrossRef]
- Himmelsbach, V.; Pinter, M.; Scheiner, B.; Venerito, M.; Sinner, F.; Zimpel, C.; Marquardt, J.U.; Trojan, J.; Waidmann, O.; Finkelmeier, F. Efficacy and safety of atezolizumab and bevacizumab in the real-world treatment of advanced hepatocellular carcinoma: Experience from four tertiary centers. Cancers 2022, 14, 1722. [Google Scholar] [CrossRef] [PubMed]
- Parekh, J.; Abraham, S.; Andanamala, H.; Rehman, A.; Ahearn, P.; Adjepong, Y.; Buller, G.; Stein, S. A single-center, real-world experience of atezolizumab plus bevacizumab as first-line therapy in patients with unresectable hepatocellular carcinoma, including patients with advanced cirrhosis. J. Clin. Oncol. 2024, 42, 445. [Google Scholar] [CrossRef]
- Singal, A.G.; Özgürdal, K.; Fan, X.; Vassilev, Z.; Pan, X.; Multani, J.K.; Chen, C.C.; Zhou, Z.; He, J.; Pisa, F. Real-world systemic treatment patterns after atezolizumab and bevacizumab in patients with hepatocellular carcinoma in the United States. Cancers 2023, 15, 5532. [Google Scholar] [CrossRef]
- D’Alessio, A.; Fulgenzi, C.A.M.; Nishida, N.; Schönlein, M.; von Felden, J.; Schulze, K.; Wege, H.; Gaillard, V.E.; Saeed, A.; Wietharn, B.; et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: A real-world study. Hepatology 2022, 76, 1000–1012. [Google Scholar] [CrossRef]
- Allaire, M.; Hajer, B.K.; Amaddeo, G.; Bouattour, M.; Brusset, B.; Ziol, M.; Merle, P.; Blanc, J.-F.; Uguen, T.; Ganne-Carrié, N.; et al. THU-466 treatment with atezolizumab-bevacizumab for hepatocellular carcinoma in the French population outside clinical trials: Data from the prospective CHIEF cohort. J. Hepatol. 2024, 80, S444. [Google Scholar] [CrossRef]
- Cosgrove, D.; Tan, R.; Osterland, A.J.; Hernandez, S.; Ogale, S.; Mahrus, S.; Murphy, J.; Wilson, T.; Patton, G.; Loaiza-Bonilla, A.; et al. Atezolizumab plus bevacizumab in patients with unresectable hepatocellular carcinoma: Real-world experience from a US Community Oncology Network. J. Hepatocell. Carcinoma 2025, 12, 791–804. [Google Scholar] [CrossRef]
- Fulgenzi, C.A.M.; Cheon, J.; D’Alessio, A.; Nishida, N.; Ang, C.; Marron, T.U.; Wu, L.; Saeed, A.; Wietharn, B.; Cammarota, A.; et al. Reproducible safety and efficacy of atezolizumab plus bevacizumab for HCC in clinical practice: Results of the AB-real study. Eur. J. Cancer 2022, 175, 204–213. [Google Scholar] [CrossRef]
- Kaplan, D.E.; Tan, R.; Xiang, C.; Mu, F.; Hernandez, S.; Ogale, S.; Li, J.; Lin, Y.; Shi, L.; Singal, A.G. Overall survival in real-world patients with unresectable hepatocellular carcinoma receiving atezolizumab plus bevacizumab versus sorafenib or lenvatinib as first-line therapy: Findings from the National Veterans Health Administration Database. Cancers 2024, 16, 3508. [Google Scholar] [CrossRef]
- Storandt, M.H.; Zemla, T.J.; Patell, K.; Naleid, N.; Gile, J.J.; Tran, N.H.; Chakrabarti, S.; Jin, Z.; Borad, M.; Mahipal, A. Atezolizumab plus bevacizumab as first-line systemic therapy for hepatocellular carcinoma: A multi-institutional cohort study. Oncologist 2024, 29, 986–996. [Google Scholar] [CrossRef]
- de Castro, T.; Jochheim, L.S.; Bathon, M.; Welland, S.; Scheiner, B.; Shmanko, K.; Roessler, D.; Ben Khaled, N.; Jeschke, M.; Ludwig, J.M.; et al. Atezolizumab and bevacizumab in patients with advanced hepatocellular carcinoma with impaired liver function and prior systemic therapy: A real-world experience. Ther. Adv. Med. Oncol. 2022, 14, 17588359221080298. [Google Scholar] [CrossRef]
- Abdelrahim, M.; Esmail, A.; Kim, R.D.; Arora, S.P.; Arshad, J.; Kournoutas, I.; O’Donnell, C.; Totev, T.; Tan, A.; Mu, F.; et al. Real-world (RW) experience with atezolizumab + bevacizumab (A+B) for the treatment of unresectable HCC (uHCC): A multicenter study. J. Clin. Oncol. 2025, 43, 537. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Udoh, U.A.; Sanabria, J.D.; Rajan, P.K.; Banerjee, M.; Schade, M.; Sanabria, J.A.; Smith, G.; Udoh, G.; Sodhi, K.; Pierre, S.; et al. Non-alcoholic fatty liver disease progression to non-alcoholic steatohepatitis-related primary liver cancer. In Liver Cancer; Sergi, C.M., Ed.; Exon Publications: Brisbane, Australia, 2021. [Google Scholar]
- ClinicalTrials.gov. NCT03434379. A Study of Atezolizumab in Combination with Bevacizumab Compared with Sorafenib in Patients with Untreated Locally Advanced or Metastatic Hepatocellular Carcinoma (IMbrave150). Available online: https://clinicaltrials.gov/study/NCT03434379 (accessed on 20 February 2025).
- Kulkarni, A.V.; Tevethia, H.; Kumar, K.; Premkumar, M.; Muttaiah, M.D.; Hiraoka, A.; Hatanaka, T.; Tada, T.; Kumada, T.; Kakizaki, S.; et al. Effectiveness and safety of atezolizumab-bevacizumab in patients with unresectable hepatocellular carcinoma: A systematic review and meta-analysis. eClinicalMedicine 2023, 63, 102179. [Google Scholar] [CrossRef]
- Espinoza, M.; Muquith, M.; Lim, M.; Zhu, H.; Singal, A.G.; Hsiehchen, D. Disease etiology and outcomes after atezolizumab plus bevacizumab in hepatocellular carcinoma: Post-hoc analysis of IMbrave150. Gastroenterology 2023, 165, 286–288.e284. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. NCT06096779. A Study Evaluating Atezolizumab, With or Without Bevacizumab, in Patients with Unresectable Hepatocellular Carcinoma and Child-Pugh B7 and B8 Cirrhosis (Kirros). Available online: https://clinicaltrials.gov/study/NCT06096779 (accessed on 20 February 2025).



{kind=link}
{kind=link}
{kind=link}
| Overall Cohort | |
|---|---|
| n = 300 | |
| Medical center where patients were treated, n (%) | |
| Mayo Clinic | 142 (47.3%) |
| Houston Methodist | 76 (25.3%) |
| Moffitt Cancer Center | 41 (13.7%) |
| Mays Cancer Center | 29 (9.7%) |
| University of Arizona | 12 (4.0%) |
| Patient age at initiation of 1L A+B 1 (mean ± SD; years) | 67.4 ± 9.3 |
| Male, n (%) | 238 (79.3%) |
| Race 2,3, n (%) | |
| White | 236 (78.7%) |
| Black or African American | 35 (11.7%) |
| Asian | 18 (6.0%) |
| Other 4 | 5 (1.7%) |
| Ethnicity 3, n (%) | |
| Hispanic or Latino | 39 (13.0%) |
| Not Hispanic or Latino | 255 (85.0%) |
| Education, n (%) | |
| High school diploma or less | 49 (16.3%) |
| Some college or associate’s degree | 42 (14.0%) |
| College graduate/bachelor’s degree or advanced degree | 55 (18.3%) |
| Unknown | 154 (51.3%) |
| Employment status 2, n (%) | |
| Employed | 51 (17.0%) |
| Unemployed 5 | 22 (7.3%) |
| Retired | 157 (52.3%) |
| On disability 6 | 37 (12.3%) |
| Unknown | 47 (15.7%) |
| Insurance type 2,3, n (%) | |
| Medicare | 204 (68.0%) |
| Commercial/private insurance | 95 (31.7%) |
| Medicaid | 21 (7.0%) |
| Other insurance 7 | 12 (4.0%) |
| Overall Cohort | |
|---|---|
| n = 300 | |
| ECOG PS 1 within 90 days of initiation of 1L A+B treatment, n (%) | |
| Grade 0: Fully active | 110 (36.7%) |
| Grade 1: Restricted | 147 (49.0%) |
| Grade 2: Ambulatory | 34 (11.3%) |
| Grade 3: Confined to bed or chair | 1 (0.3%) |
| Comorbidities, assessed during baseline 2, n (%) | |
| Cirrhosis | 207 (69.0%) |
| Hypertension | 167 (55.7%) |
| Diabetes mellitus | 113 (37.7%) |
| Esophageal varices | 55 (18.3%) |
| Ascites | 54 (18.0%) |
| Mild to moderate ascites | 48 (88.9%) |
| Severe ascites | 6 (11.1%) |
| Encephalopathy | 22 (7.3%) |
| Encephalopathy grade 1 or 2 | 13 (59.1%) |
| Encephalopathy grade unknown | 9 (40.9%) |
| Overall Cohort | |
|---|---|
| n = 300 | |
| Primary HCC etiology, n (%) | |
| Viral etiology 1 | 132 (44.0%) |
| Hepatitis C virus | 114 (86.4%) |
| Hepatitis B virus | 17 (13.0%) |
| Non-viral etiology 1 | 108 (36.0%) |
| Non-alcoholic steatohepatitis | 34 (31.5%) |
| Alcohol-related fatty liver disease | 34 (31.5%) |
| Non-alcoholic fatty liver disease | 9 (8.3%) |
| Diabetes mellitus | 6 (5.6%) |
| Metabolic syndrome | 2 (1.9%) |
| Other etiology 2 | 35 (11.7%) |
| Unknown etiology | 25 (8.3%) |
| CP class within 90 days of initiation of 1L A+B treatment, n (%) | |
| A (CP score = 5–6 points) | 219 (73.0%) |
| B (CP score = 7–9 points) | 79 (26.3%) |
| C (CP score = 10–15 points) | 2 (0.7%) |
| BCLC stage 3,4 within 90 days of initiation of 1L A+B treatment, n (%) | |
| A: Early | 8 (2.7%) |
| B: Intermediate | 41 (13.7%) |
| C: Advanced | 247 (82.3%) |
| D: End-stage | 3 (1.0%) |
| HCC tumor invasion 5 within 90 days of initiation of 1L A+B treatment, n (%) | |
| Extrahepatic spread | 120 (40.0%) |
| Vp4 portal vein invasion | 76 (25.3%) |
| Tumor invasion > 50% of liver | 57 (19.0%) |
| Bile duct invasion | 13 (4.3%) |
| None of the above | 108 (36.0%) |
| ALBI grade 3,6 within 90 days of initiation of 1L A+B treatment, n (%) | |
| 1 | 98 (32.7%) |
| 2 | 173 (57.7%) |
| 2A | 86 (49.7%) |
| 2B | 87 (50.3%) |
| 3 | 27 (9.0%) |
| Overall Cohort | |
|---|---|
| n = 300 | |
| Locoregional HCC treatment prior to 1L A+B treatment 1, n (%) | |
| No prior locoregional treatment received | 144 (48.0%) |
| Embolization (transarterial embolization or transarterial chemoembolization) | 88 (29.3%) |
| Transarterial radioembolization | 49 (16.3%) |
| Ablation (includes radiofrequency ablation or microwave ablation) | 43 (14.3%) |
| Stereotactic body radiotherapy | 26 (8.7%) |
| Selective internal radiation therapy | 7 (2.3%) |
| External beam radiotherapy | 1 (0.3%) |
| Other locoregional treatment received 2 | 10 (3.3%) |
| Systemic HCC therapy following 1L A+B treatment 1, n (%) | |
| No systemic treatment received | 208 (69.3%) |
| Lenvatinib | 56 (18.7%) |
| Cabozantinib | 15 (5.0%) |
| Sorafenib | 13 (4.3%) |
| Pembrolizumab | 11 (3.7%) |
| Nivolumab | 7 (2.3%) |
| Regorafenib | 4 (1.3%) |
| Ipilimumab | 5 (1.7%) |
| Other systemic therapy received 3 | 26 (8.7%) |
| Overall Cohort | |
|---|---|
| n = 300 | |
| Clinician-assessed best treatment response 1, n (%) | |
| rwCR | 22 (7.3%) |
| rwPR | 70 (23.3%) |
| rwSD | 118 (39.3%) |
| rwPD | 59 (19.7%) |
| Unable to assess | 31 (10.3%) |
| Duration of best treatment response (mean ± SD; months) | 10.3 ± 8.3 |
| Radiological assessment types used to assess best treatment response 2 | |
| Computed tomography | 177 (59.0%) |
| Magnetic resonance imaging | 157 (52.3%) |
| 18F fludeoxyglucose positron emission tomography | 6 (2.0%) |
| Magnetic resonance spectroscopy | 2 (0.7%) |
| Other | 1 (0.3%) |
| Unknown | 29 (9.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrahim, M.; Esmail, A.; Kim, R.D.; Arora, S.P.; Arshad, J.; Kournoutas, I.A.; O’Donnell, C.D.; Totev, T.I.; Tan, A.; Mu, F.; et al. Real-World Experiences Using Atezolizumab + Bevacizumab for the Treatment of Unresectable Hepatocellular Carcinoma: A Multicenter Study. Cancers 2025, 17, 1814. https://doi.org/10.3390/cancers17111814
Abdelrahim M, Esmail A, Kim RD, Arora SP, Arshad J, Kournoutas IA, O’Donnell CD, Totev TI, Tan A, Mu F, et al. Real-World Experiences Using Atezolizumab + Bevacizumab for the Treatment of Unresectable Hepatocellular Carcinoma: A Multicenter Study. Cancers. 2025; 17(11):1814. https://doi.org/10.3390/cancers17111814
Chicago/Turabian StyleAbdelrahim, Maen, Abdullah Esmail, Richard D. Kim, Sukeshi Patel Arora, Junaid Arshad, Ioannis A. Kournoutas, Conor D. O’Donnell, Todor I. Totev, Amie Tan, Fan Mu, and et al. 2025. "Real-World Experiences Using Atezolizumab + Bevacizumab for the Treatment of Unresectable Hepatocellular Carcinoma: A Multicenter Study" Cancers 17, no. 11: 1814. https://doi.org/10.3390/cancers17111814
APA StyleAbdelrahim, M., Esmail, A., Kim, R. D., Arora, S. P., Arshad, J., Kournoutas, I. A., O’Donnell, C. D., Totev, T. I., Tan, A., Mu, F., Seshasayee, S. M., Hernandez, S., & Tran, N. H. (2025). Real-World Experiences Using Atezolizumab + Bevacizumab for the Treatment of Unresectable Hepatocellular Carcinoma: A Multicenter Study. Cancers, 17(11), 1814. https://doi.org/10.3390/cancers17111814