
Clinical and Diagnostic Utility of Genomic Profiling for Digestive Cancers: Real-World Evidence from Japan
 ,
,  , ,
, ,  , , , , , ,
, , , , , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
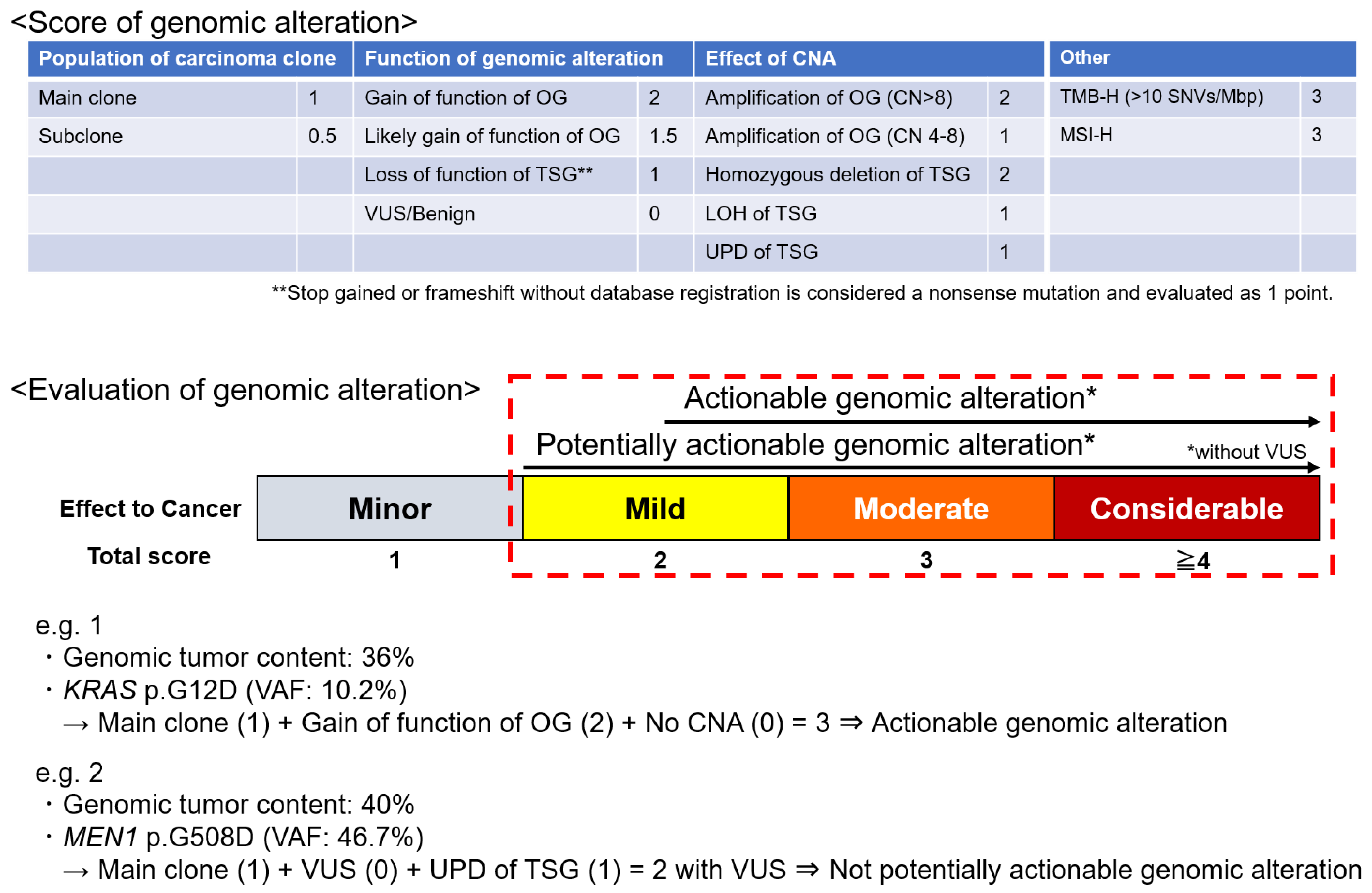
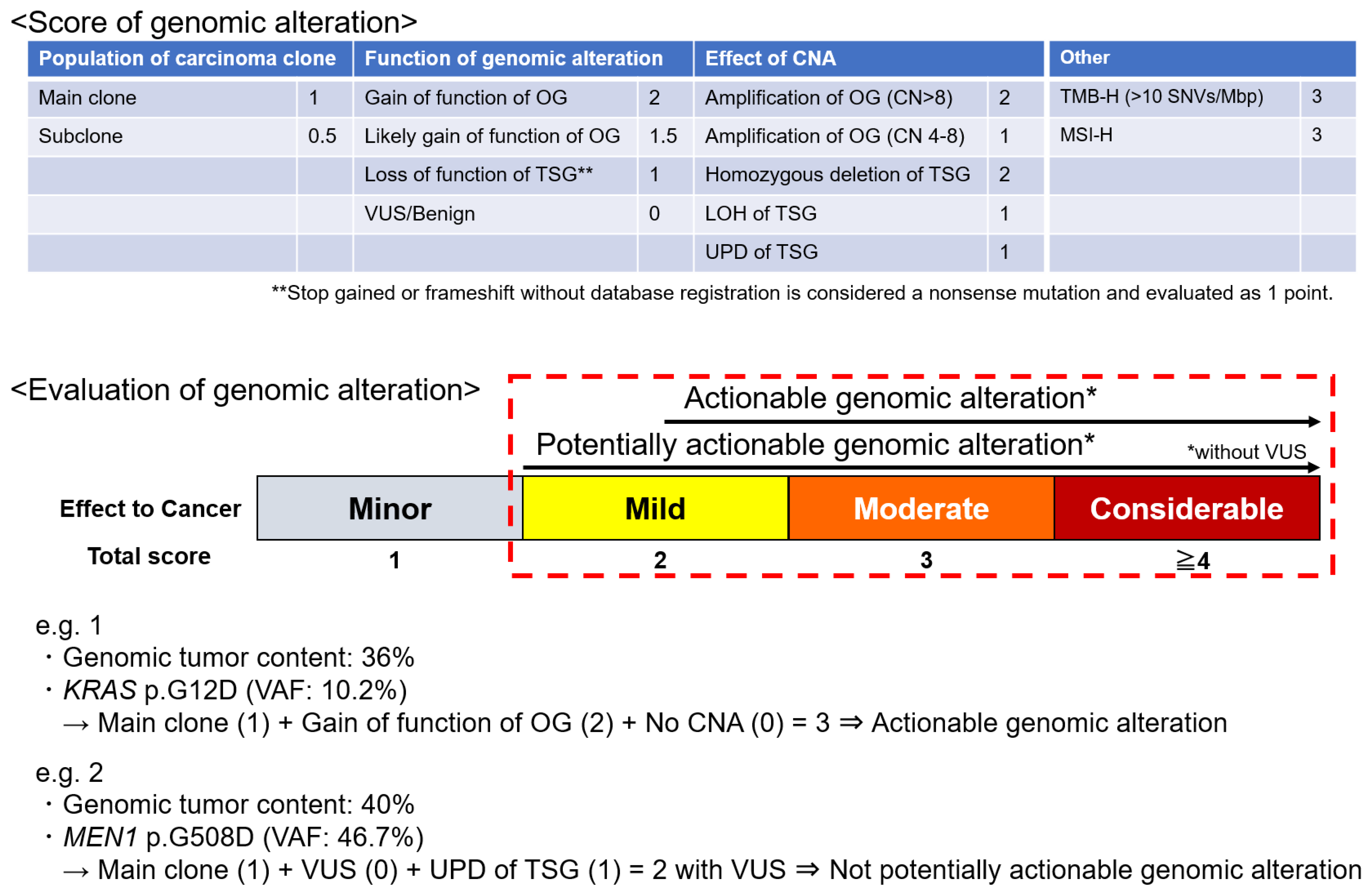
2.1. Sequencing and Identification of Genomic Alterations
2.2. Statistical Analysis
3. Results
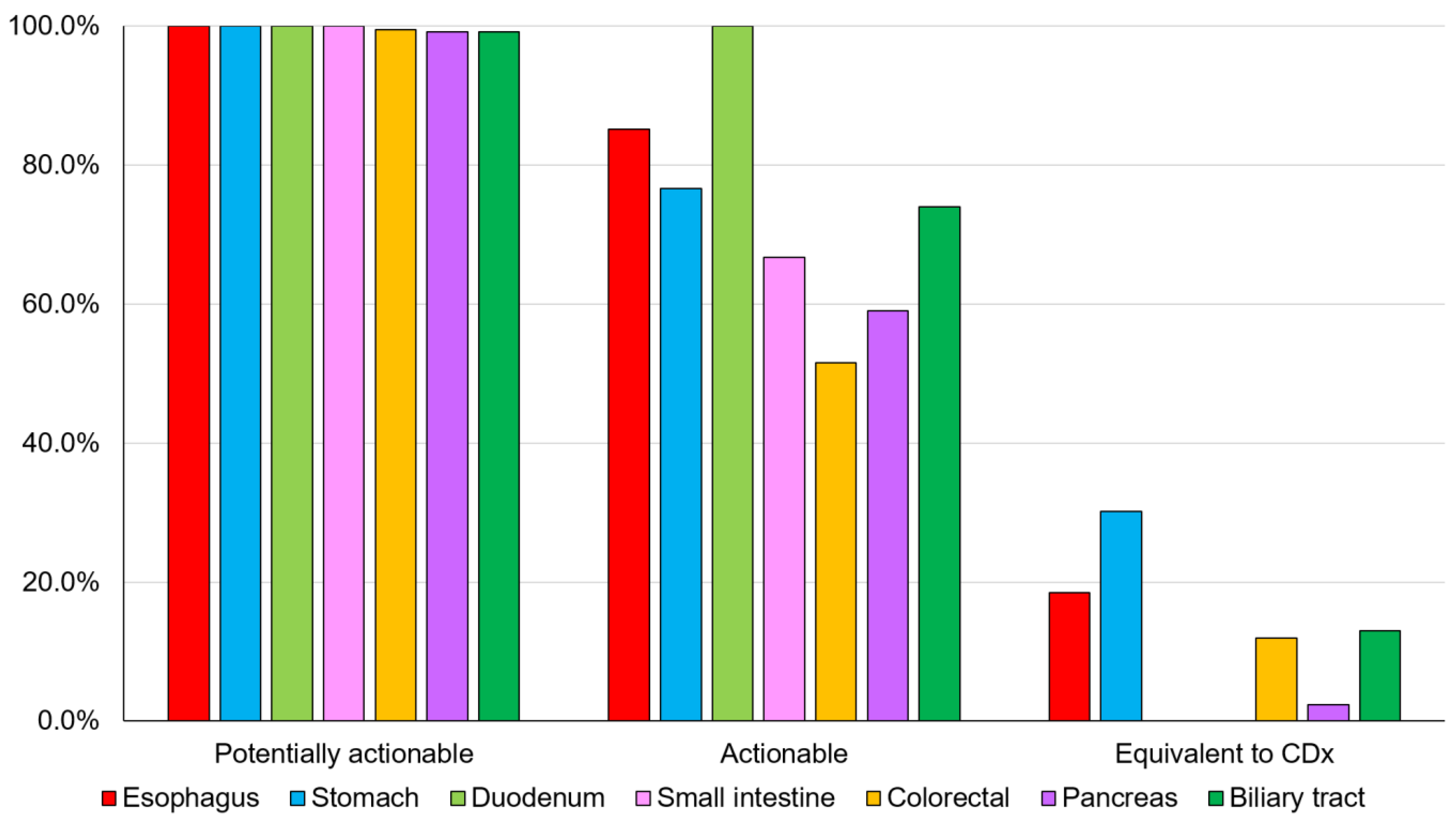
3.1. Detection Rate of Genomic Alterations in Digestive Cancers
3.1.1. Esophagus/Stomach Cancer
3.1.2. Bowel Cancer
3.1.3. Pancreatic Cancer
3.1.4. Biliary Tract Cancer
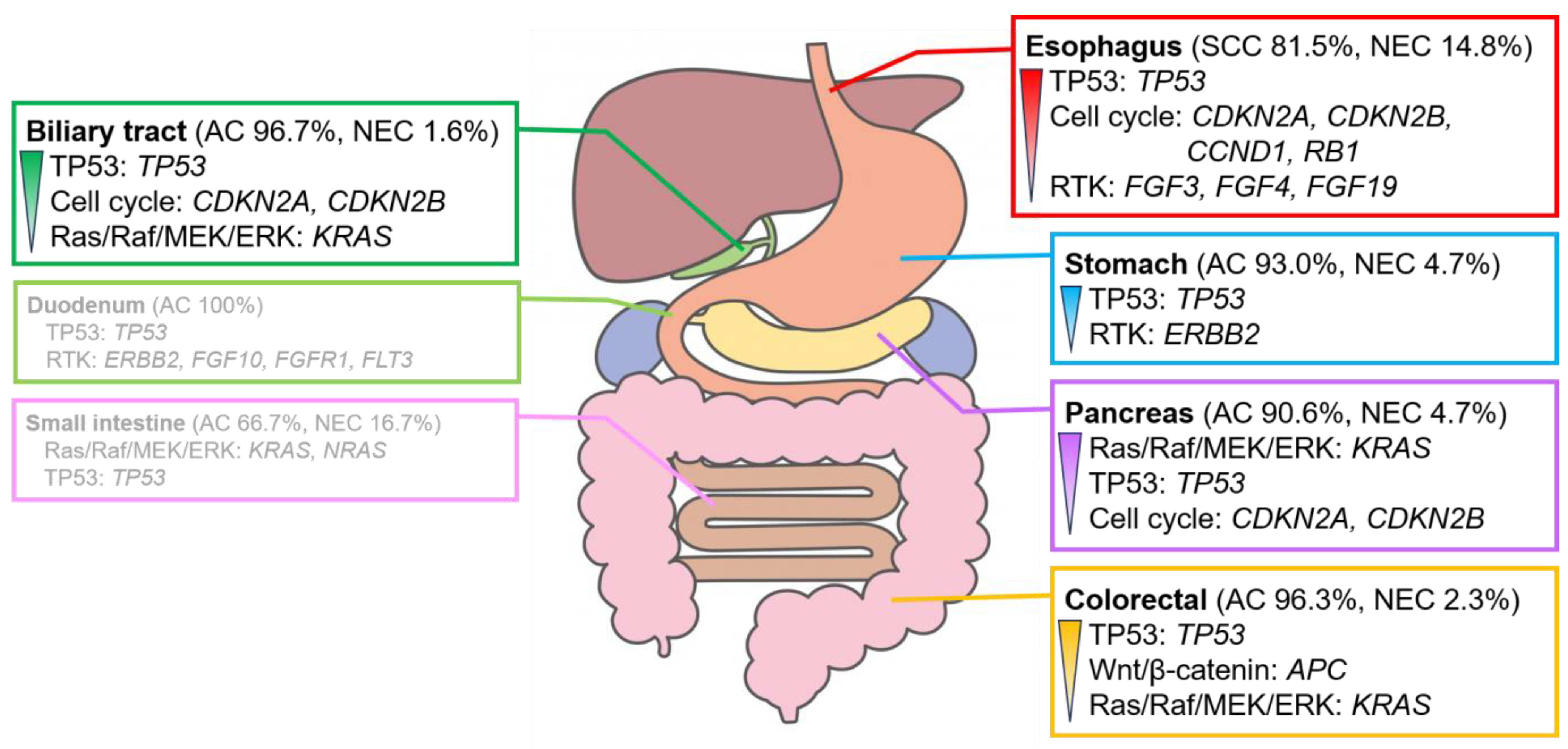
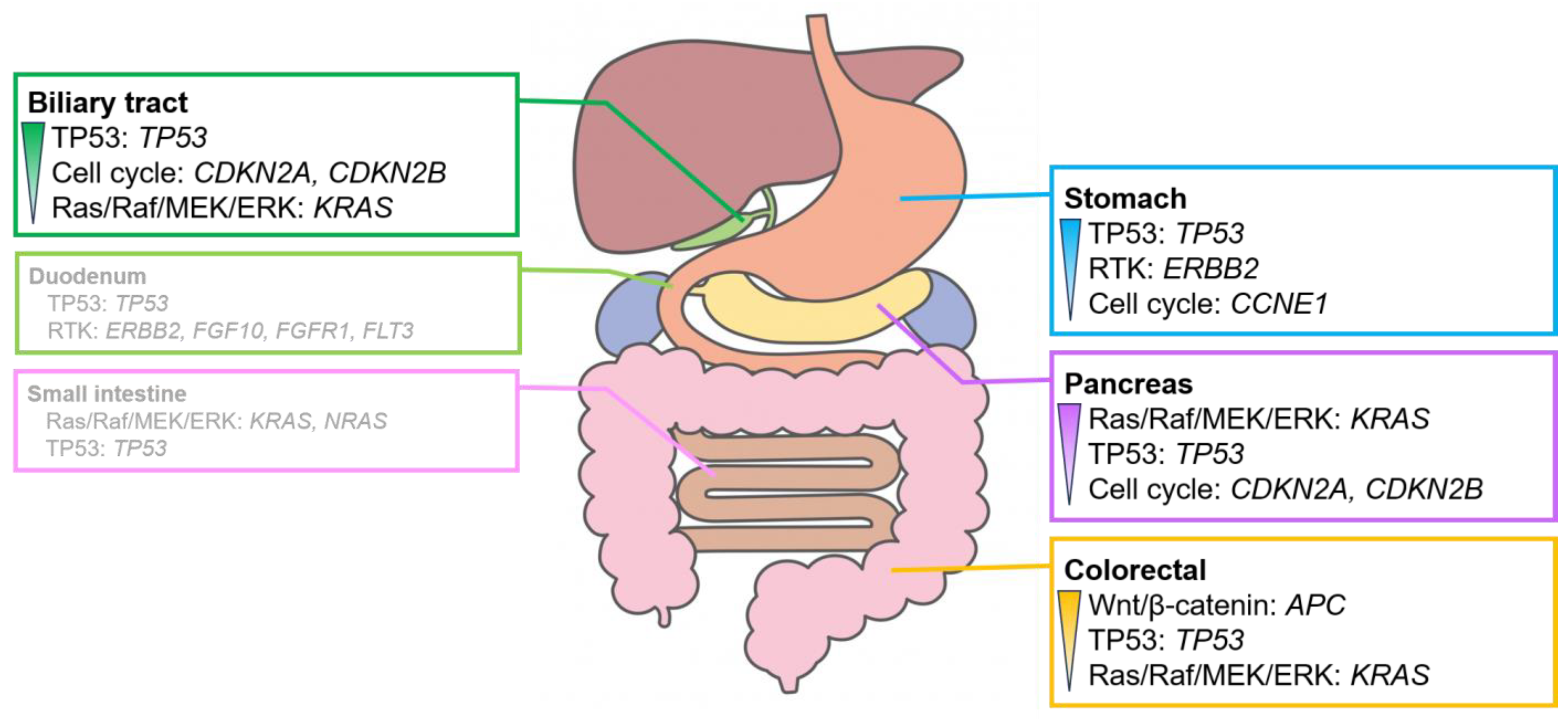
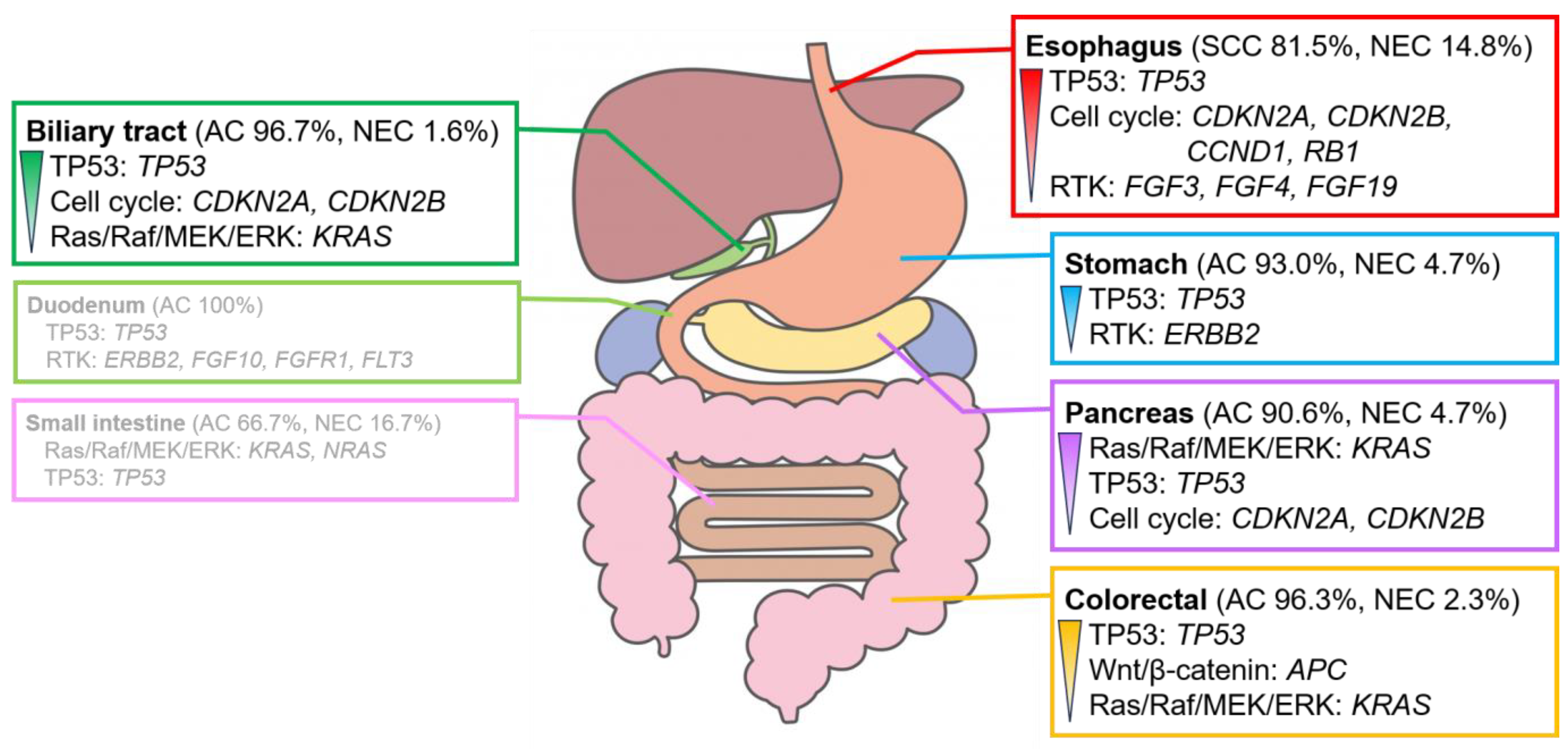
3.2. Genomic Alteration of Digestive Adenocarcinomas
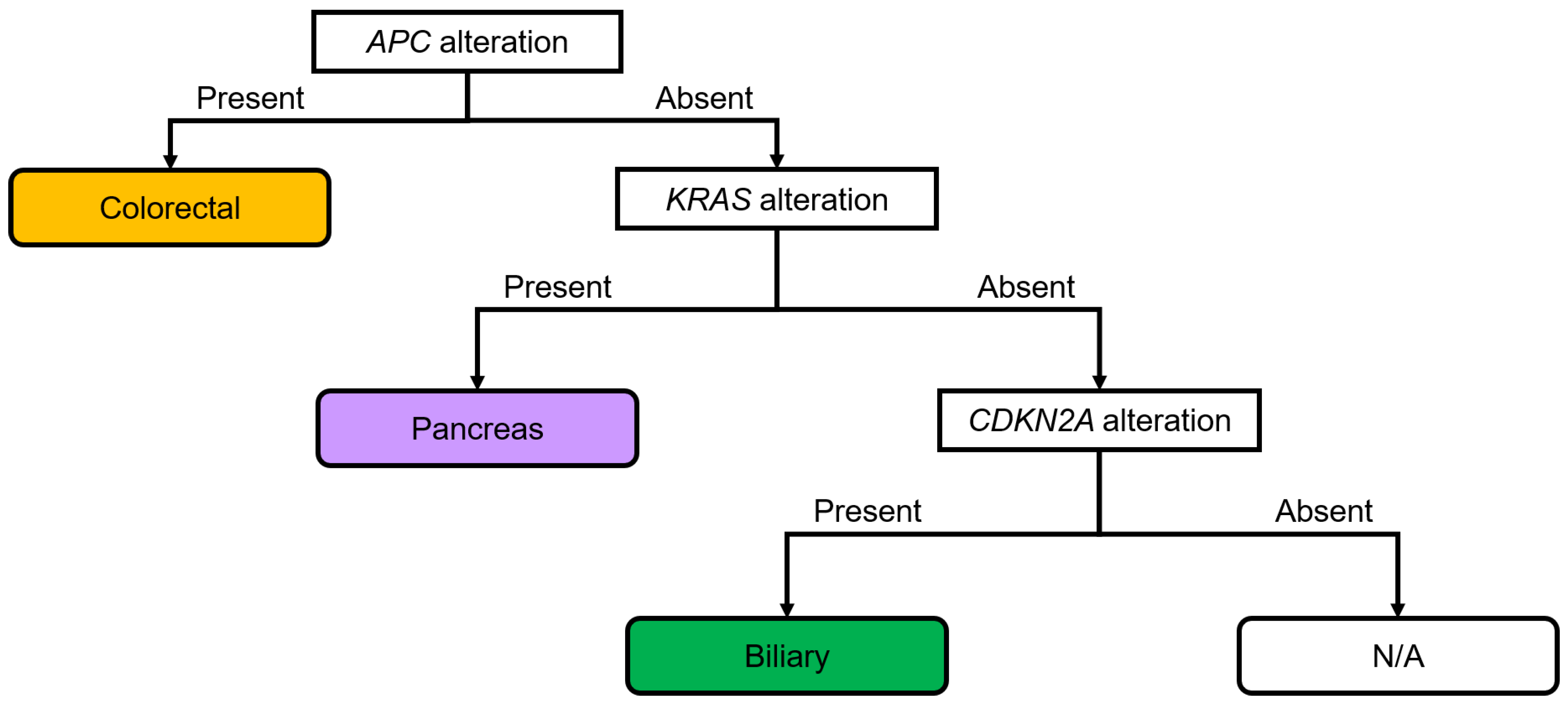
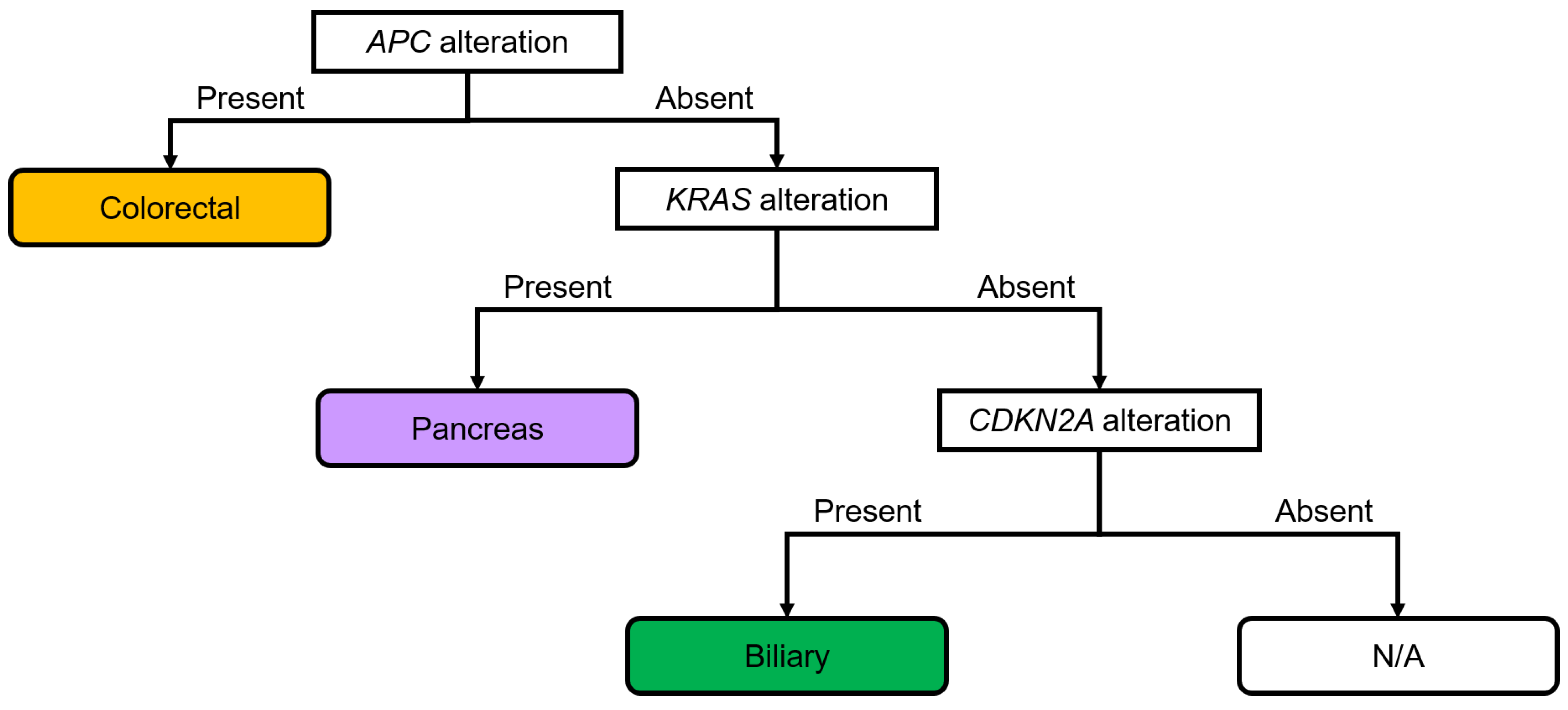
3.3. Diagnostic Flowchart of Digestive Adenocarcinomas
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Serizawa, M.; Mizuguchi, M.; Urakami, K.; Nagashima, T.; Ohshima, K.; Hatakeyama, K.; Ohnami, S.; Ohnami, S.; Maruyama, K.; Ashizawa, T.; et al. JCGA: The: Japanese version of the Cancer Genome Atlas and its contribution to the interpretation of gene alterations detected in clinical cancer genome sequencing. Hum. Genome Var. 2021, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.H.; Hsu, G.; Siden, E.G.; Thorlund, K.; Mills, E.J. An overview of precision oncology basket and umbrella trials for clinicians. CA Cancer J. Clin. 2020, 70, 12–137. [Google Scholar] [CrossRef] [PubMed]
- Kohno, T. Implementation of “clinical sequencing” in cancer genome medicine in Japan. Cancer Sci. 2018, 109, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Kou, T.; Kanai, M.; Yamamoto, Y.; Kamada, M.; Nakatsui, M.; Sakuma, T.; Mochizuki, H.; Hiroshima, A.; Sugiyama, A.; Nakamura, E.; et al. Clinical sequencing using a next-generation sequencing-based multiplex gene assay in patients with advanced solid tumors. Cancer Sci. 2017, 108, 1440–1446. [Google Scholar] [CrossRef]
- Frampton, G.M.; Fichtenholtz, A.; Otto, G.A.; Wang, K.; Downing, S.R.; He, J.; Schnall-Levin, M.; White, J.; Sanford, E.M.; An, P.; et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat. Biotechnol. 2013, 31, 1023–1031. [Google Scholar] [CrossRef]
- Ebi, H.; Bando, H. Precision oncology and the universal health coverage system in Japan. JCO Precis. Oncol. 2019, 3, PO.19.00291. [Google Scholar] [CrossRef] [PubMed]
- As Our Understanding of Cancer Evolves, So Do Our Tests: FoundationOne®, CDx Gene List. FoundationOne®, CDx. Available online: https://www.foundationmedicine.in/content/dam/rfm/in_v2-en_in/CDx/FoundationOne%20CDx%20Gene%20list.pdf (accessed on 10 March 2024).
- Milbury, C.A.; Creeden, J.; Yip, W.K.; Smith, D.L.; Pattani, V.; Maxwell, K.; Sawchyn, B.; Gjoerup, O.; Meng, W.; Skoletsky, J.; et al. Clinical and analytical validation of FoundationOne®CDx, a comprehensive genomic profiling assay for solid tumors. PLoS ONE 2022, 17, e0264138. [Google Scholar] [CrossRef] [PubMed]
- Ida, H.; Koyama, T.; Mizuno, T.; Sunami, K.; Kubo, T.; Sudo, K.; Tao, K.; Hirata, M.; Yonemori, K.; Kato, K.; et al. Clinical utility of comprehensive genomic profiling tests for advanced or metastatic solid tumor in clinical practice. Cancer Sci. 2022, 113, 4300–4310. [Google Scholar] [CrossRef] [PubMed]
- Koguchi, D.; Tsumura, H.; Tabata, K.; Shimura, S.; Satoh, T.; Ikeda, M.; Watanabe, A.; Yoshida, T.; Sasaki, J.; Matsumoto, K.; et al. Real-world data on the comprehensive genetic profiling test for Japanese patients with metastatic castration-resistant prostate cancer. Jpn. J. Clin. Oncol. 2024, hyae003. [Google Scholar] [CrossRef]
- Higashigawa, S.; Matsubayashi, H.; Kiyozumi, Y.; Kado, N.; Nishimura, S.; Oishi, T.; Sugino, T.; Fushiki, K.; Shirasu, H.; Yasui, H.; et al. Present status of germline findings in precision medicine for Japanese cancer patients: Issues in the current system. Jpn. J. Clin. Oncol. 2022, 52, 599–608. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Kano, Y.; Tohyama, K.; Matsudera, S.; Kumaki, Y.; Takahashi, K.; Mitsumura, T.; Harada, Y.; Sato, A.; Nakamura, H.; et al. Clinical utility of comprehensive genomic profiling in Japan: Result of PROFILE-F study. PLoS ONE 2022, 17, e0266112. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, J.; Ohhara, Y.; Takada, K.; Tanabe, H.; Hatanaka, K.; Amano, T.; C Hatanaka, K.; Hatanaka, Y.; Mitamura, T.; Kato, M.; et al. Clinical significance of comprehensive genomic profiling tests covered by public insurance in patients with advanced solid cancers in Hokkaido, Japan. Jpn. J. Clin. Oncol. 2021, 51, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Sbaraglia, M.; Bellan, E.; Tos, A.P.D. The 2020 WHO Classification of Soft Tissue Tumours: News and perspectives. Pathologica 2021, 113, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Kohno, T.; Kato, M.; Kohsaka, S.; Sudo, T.; Tamai, I.; Shiraishi, Y.; Okuma, Y.; Ogasawara, D.; Suzuki, T.; Yoshida, T.; et al. C-CAT: The National Datacenter for Cancer Genomic Medicine in Japan. Cancer Discov. 2022, 12, 2509–2515. [Google Scholar] [CrossRef] [PubMed]
- Sunami, K.; Naito, Y.; Aimono, E.; Amano, T.; Ennishi, D.; Kage, H.; Kanai, M.; Komine, K.; Koyama, Y.; Maeda, T.; et al. The initial assessment of expert panel performance in core hospitals for cancer genomic medicine in Japan. Int. J. Clin. Oncol. 2021, 26, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Aburatani, H.; Amano, T.; Baba, E.; Furukawa, T.; Hayashida, T.; Hiyama, E.; Ikeda, S.; Kanai, M.; Kato, M.; et al. Clinical Practice Guidance for Next-Generation Sequencing in Cancer Diagnosis and Treatment (edition 2.1). Int. J. Clin. Oncol. 2021, 26, 233–283. [Google Scholar] [CrossRef]
- González-González, M.; Gutiérrez, M.L.; Sayagués, J.M.; Muñoz-Bellvís, L.; Orfao, A. Genomic profiling of sporadic liver metastatic colorectal cancer. Semin. Cancer Biol. 2021, 71, 98–108. [Google Scholar] [CrossRef]
- Yamai, T.; Ikezawa, K.; Sugimoto, N.; Urabe, M.; Kai, Y.; Takada, R.; Nakabori, T.; Uehara, H.; Kawamura, T.; Kunimasa, K.; et al. Utility of comprehensive genomic profiling tests for patients with incurable pancreatic cancer in clinical practice. Cancers 2023, 15, 970. [Google Scholar] [CrossRef]
- Bekaii-Saab, T.S.; Bridgewater, J.; Normanno, N. Practical considerations in screening for genetic alterations in cholangiocarcinoma. Ann. Oncol. 2021, 32, 1111–1126. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, P.; Borrelli, A.; Tuccillo, F.M.; Silvestro, L.; Palaia, R.; Buonaguro, F.M. Precision medicine in gastric cancer. World J. Gastrointest. Oncol. 2019, 11, 804–829. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Integrated genomic characterization of oesophageal carcinoma. Nature 2017, 541, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Guinney, J.; Dienstmann, R.; Wang, X.; Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Integrated Genomic Characterization of Pancreatic Ductal Adenocarcinoma. Cancer Cell 2017, 32, 185–203.e13. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Shirota, H.; Komine, K.; Takahashi, M.; Takahashi, S.; Miyauchi, E.; Niizuma, H.; Tada, H.; Shimada, M.; Niihori, T.; Aoki, Y.; et al. Clinical decisions by the molecular tumor board on comprehensive genomic profiling tests in Japan: A retrospective observational study. Cancer Med. 2023, 12, 6170–6181. [Google Scholar] [CrossRef]
- Normanno, N.; De Luca, A.; Abate, R.E.; Morabito, A.; Milella, M.; Tabbò, F.; Curigliano, G.; Masini, C.; Marchetti, P.; Pruneri, G.; et al. Current practice of genomic profiling of patients with advanced solid tumours in Italy: The Italian Register of Actionable Mutations (RATIONAL) study. Eur. J. Cancer 2023, 187, 174–184. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Sunami, K.; Ichikawa, H.; Kubo, T.; Kato, M.; Fujiwara, Y.; Shimomura, A.; Koyama, T.; Kakishima, H.; Kitami, M.; Matsushita, H.; et al. Feasibility and utility of a panel testing for 114 cancer-associated genes in a clinical setting: A hospital-based study. Cancer Sci. 2019, 110, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Matsubara, J.; Quy, P.N.; Fukuyama, K.; Nomura, M.; Funakoshi, T.; Doi, K.; Sakamori, Y.; Yoshioka, M.; Yokoyama, A.; et al. Comprehensive genomic profiling for patients with chemotherapy-naïve advanced cancer. Cancer Sci. 2021, 112, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Larson, K.L.; Huang, B.; Weiss, H.L.; Hull, P.; Westgate, P.M.; Miller, R.W.; Arnold, S.M.; Kolesar, J.M. Clinical outcomes of molecular tumor boards: A systematic review. JCO Precis. Oncol. 2021, 5, PO.20.00495. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Takahama, T.; Sakai, K.; Shimizu, S.; Watanabe, S.; Kawakami, H.; Tanaka, K.; Sato, C.; Hayashi, H.; Nonagase, Y.; et al. Clinical application of the FoundationOne CDx assay to therapeutic decision-making for patients with advanced solid tumors. Oncologist 2021, 26, e588–e596. [Google Scholar] [CrossRef]
- Seet, A.O.L.; Tan, A.C.; Tan, T.J.; Ng, M.C.H.; Tai, D.W.M.; Lam, J.Y.C.; Tan, G.S.; Gogna, A.; Too, C.W.; Tan, B.S.; et al. Individualized molecular profiling for allocation to clinical trials Singapore study—An Asian tertiary cancer center experience. JCO Precis. Oncol. 2021, 5, PO.20.00261. [Google Scholar] [CrossRef]
- C-CAT Registration Status. Available online: https://for-patients.c-cat.ncc.go.jp/registration_status/ (accessed on 5 April 2024).
- Mukai, Y.; Ueno, H. Establishment and implementation of cancer genomic medicine in Japan. Cancer Sci. 2021, 112, 970–977. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, M.; Nakamura, K.; Kawano, R.; Hayashi, H.; Ikeda, T.; Saito, M.; Niida, Y.; Sasaki, J.; Okuda, H.; Ishihara, S.; et al. Clinical and Diagnostic Utility of Genomic Profiling for Digestive Cancers: Real-World Evidence from Japan. Cancers 2024, 16, 1504. https://doi.org/10.3390/cancers16081504
Ishikawa M, Nakamura K, Kawano R, Hayashi H, Ikeda T, Saito M, Niida Y, Sasaki J, Okuda H, Ishihara S, et al. Clinical and Diagnostic Utility of Genomic Profiling for Digestive Cancers: Real-World Evidence from Japan. Cancers. 2024; 16(8):1504. https://doi.org/10.3390/cancers16081504
Chicago/Turabian StyleIshikawa, Marin, Kohei Nakamura, Ryutaro Kawano, Hideyuki Hayashi, Tatsuru Ikeda, Makoto Saito, Yo Niida, Jiichiro Sasaki, Hiroyuki Okuda, Satoshi Ishihara, and et al. 2024. "Clinical and Diagnostic Utility of Genomic Profiling for Digestive Cancers: Real-World Evidence from Japan" Cancers 16, no. 8: 1504. https://doi.org/10.3390/cancers16081504
APA StyleIshikawa, M., Nakamura, K., Kawano, R., Hayashi, H., Ikeda, T., Saito, M., Niida, Y., Sasaki, J., Okuda, H., Ishihara, S., Yamaguchi, M., Shimada, H., Isobe, T., Yuza, Y., Yoshimura, A., Kuroda, H., Yukisawa, S., Aoki, T., Takeshita, K., ... Nishihara, H. (2024). Clinical and Diagnostic Utility of Genomic Profiling for Digestive Cancers: Real-World Evidence from Japan. Cancers, 16(8), 1504. https://doi.org/10.3390/cancers16081504