
Copy Number Analysis of 9p24.1 in Classic Hodgkin Lymphoma Arising in Immune Deficiency/Dysregulation
 , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Histological Examinations
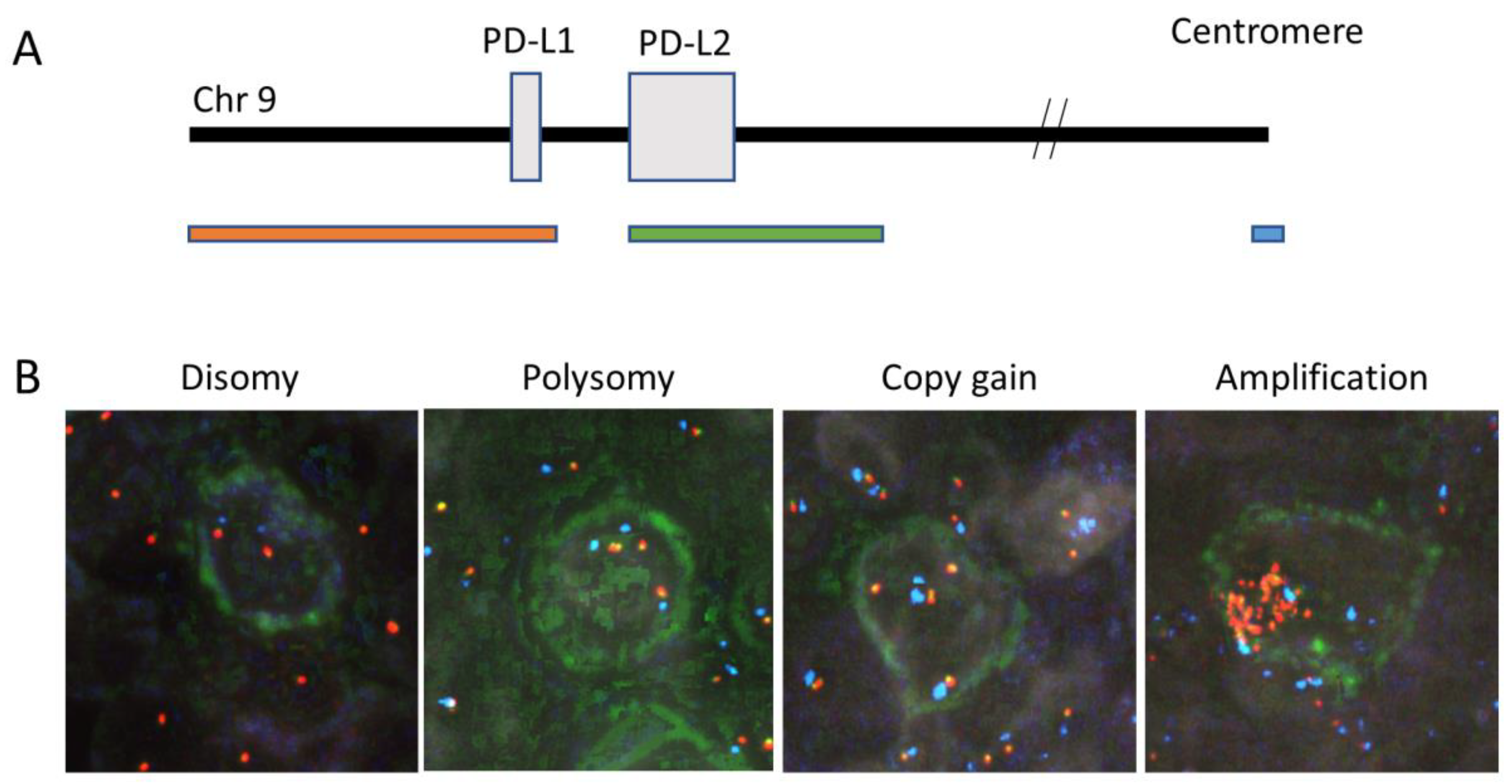
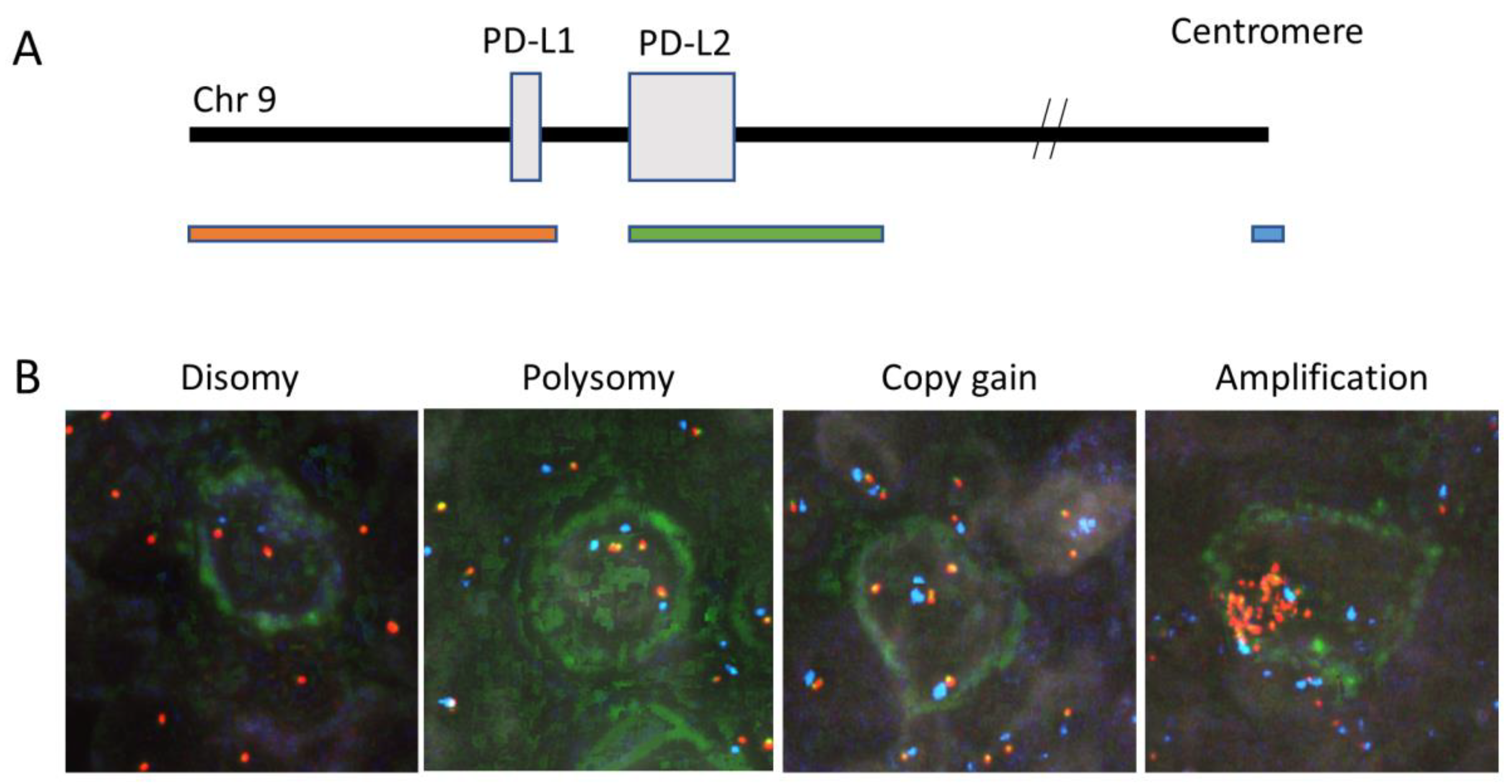
2.3. Immunofluorescence In Situ Hybridization
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
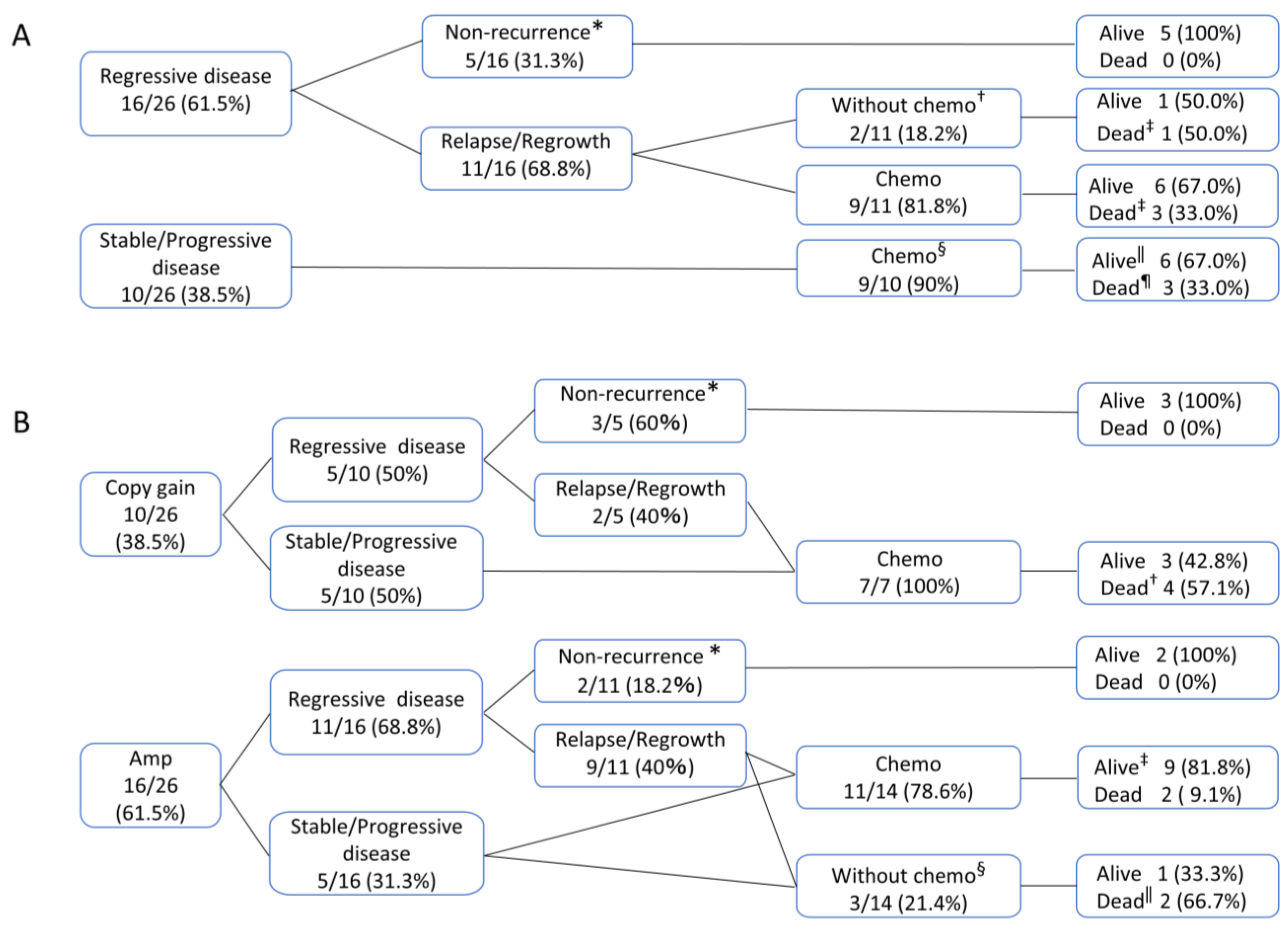
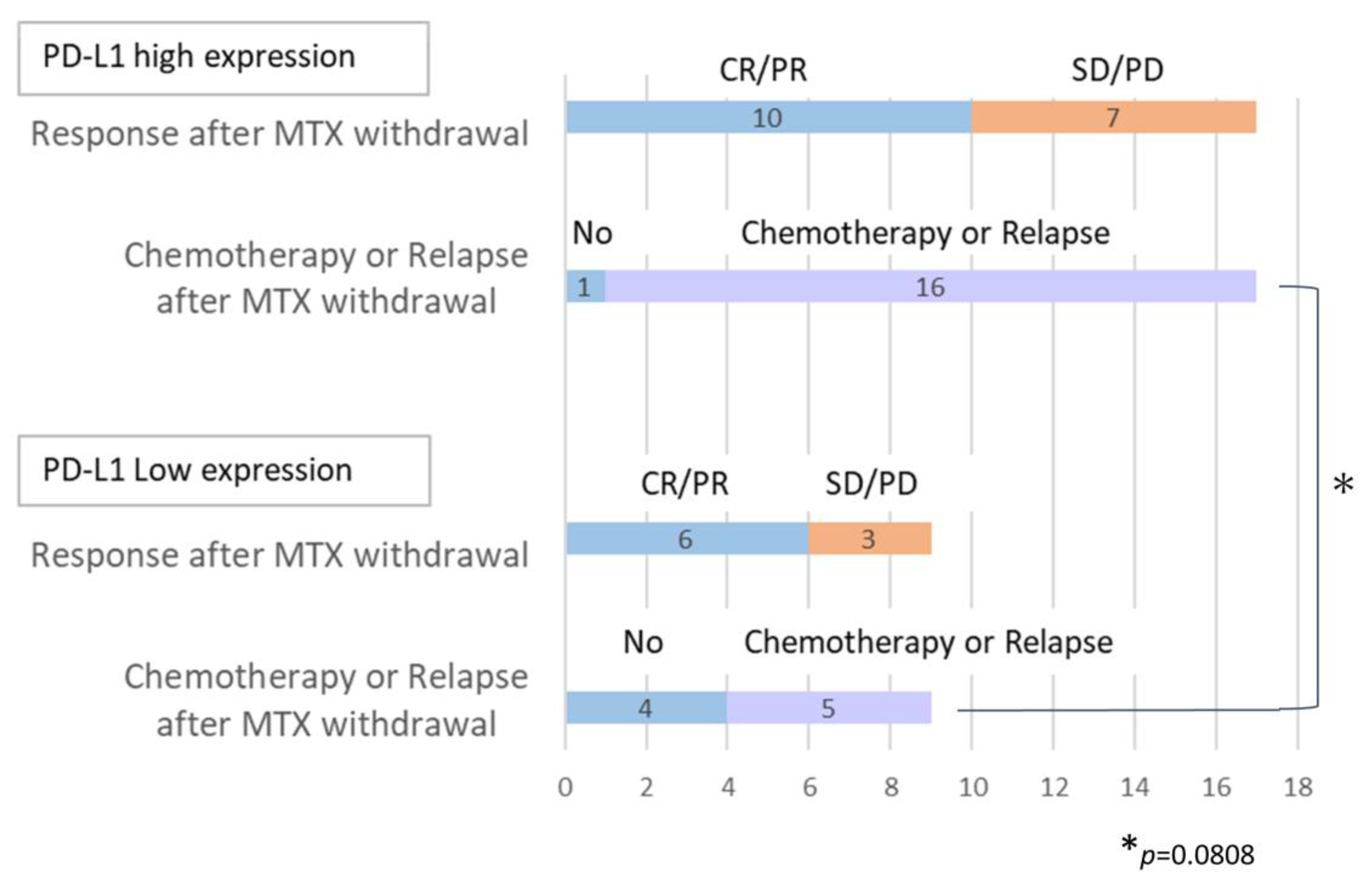
3.2. Clinical Courses after Methotrexate Withdrawal
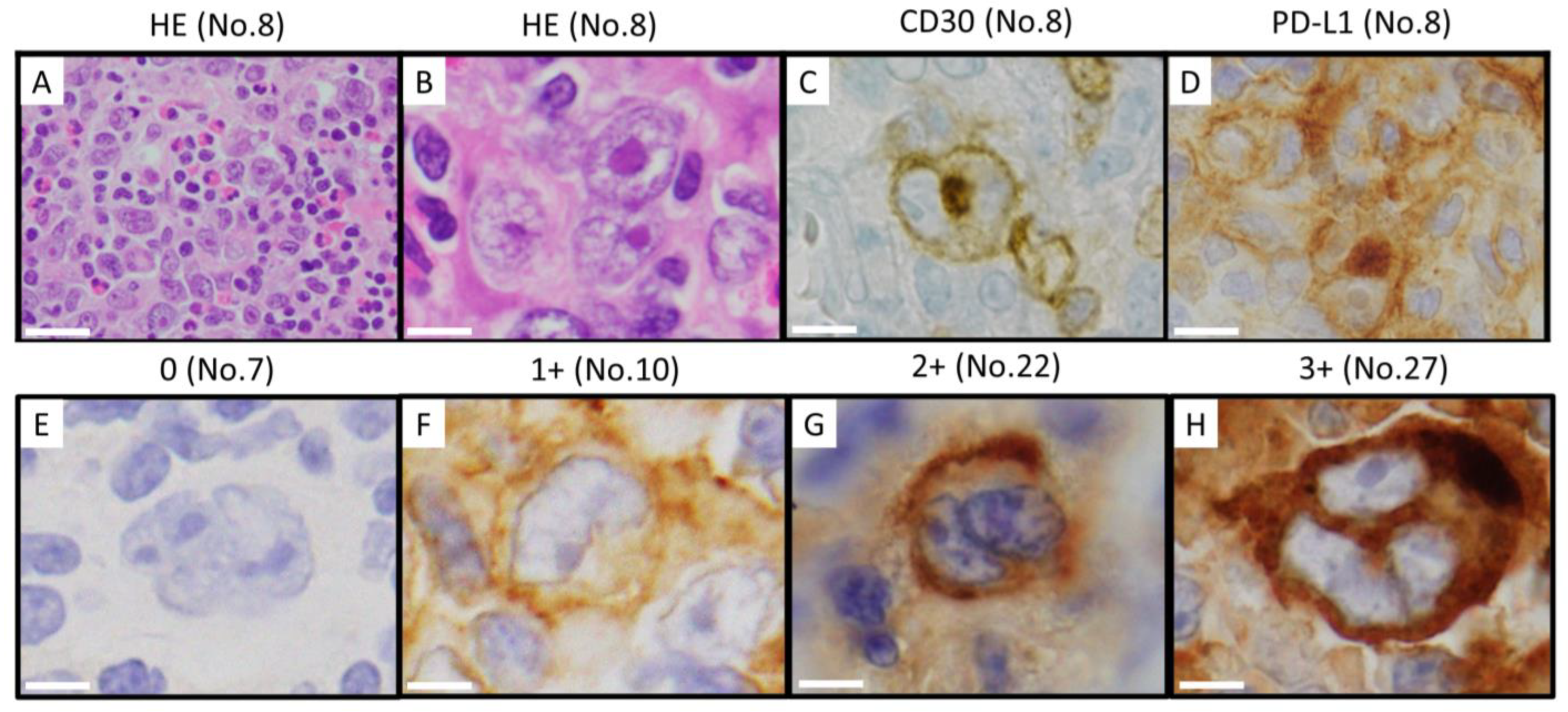
3.3. Immunohistochemical Phenotype and Epstein–Barr Virus Latency
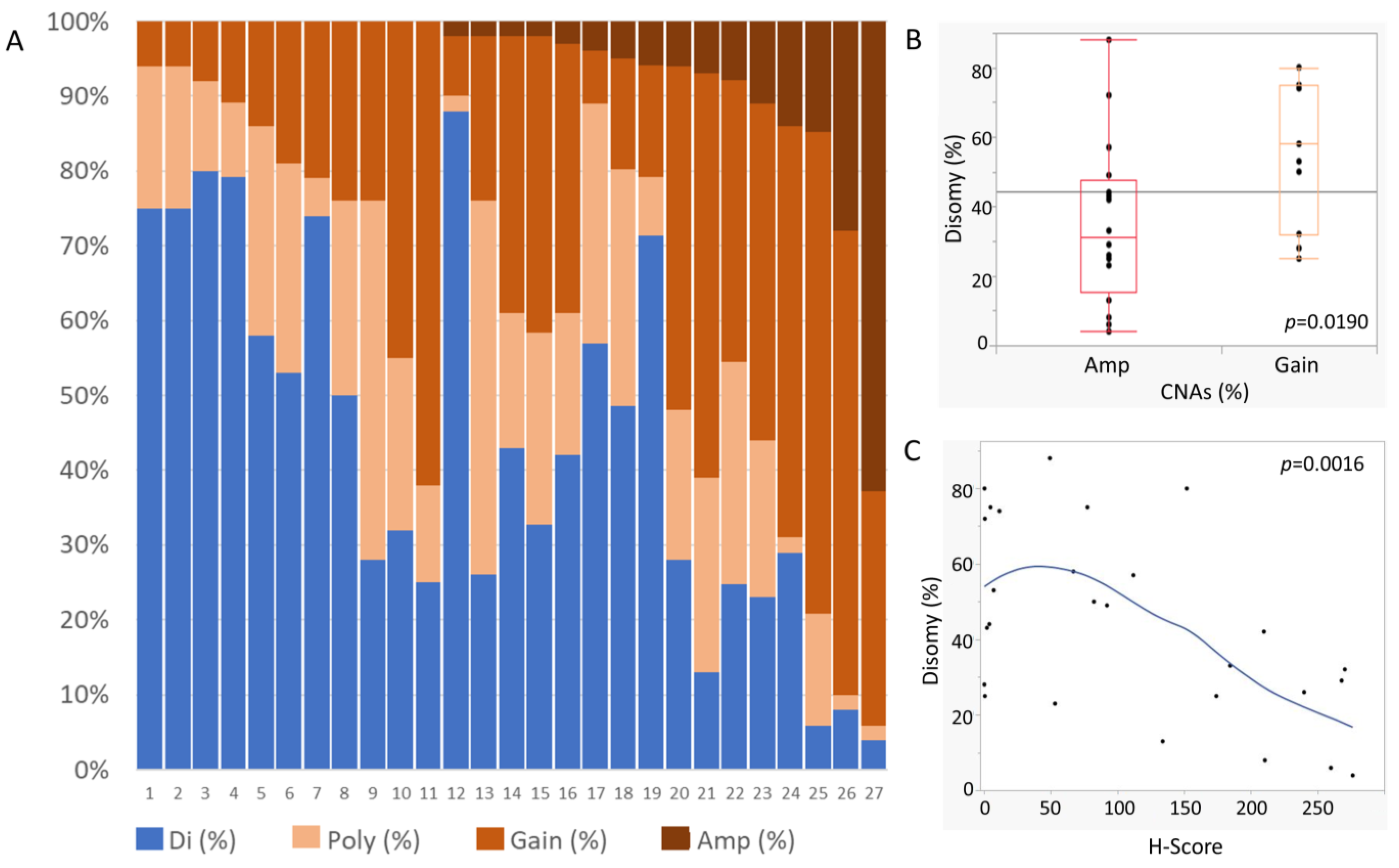
3.4. Genetic Alterations to 9p24.1
3.5. Relationship between 9p24.1 Genetic Alterations and Clinicopathological Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaulard, P.; Swerdlow, S.H.; Harris, N.L.; Jaffe, E.S.; Sundstrom, C.; International Agency for Research on Cancer. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Vardiman, J.W., Eds.; IARC Press: Lyon, France, 2008; pp. 350–351. [Google Scholar]
- Isomäki, H.A.; Hakulinen, T.; Joutsenlahti, U. Excess risk of lymphomas, leukemia and myeloma in patients with rheumatoid arthritis. J. Chronic Dis. 1978, 31, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Baecklund, E.; Askling, J.; Rosenquist, R.; Ekbom, A.; Klareskog, L. Rheumatoid arthritis and malignant lymphomas. Curr. Opin. Rheumatol. 2004, 16, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Zintzaras, E.; Voulgarelis, M.; Moutsopoulos, H.M. The risk of lymphoma development in autoimmune diseases: A meta-analysis. Arch. Intern. Med. 2005, 165, 2337–2344. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, A.; Arakawa, F.; Kiyasu, J.; Sato, K.; Miyoshi, H.; Niino, D.; Kimura, Y.; Takeuchi, M.; Yoshida, M.; Ishibashi, Y.; et al. Methotrexate/iatrogenic lymphoproliferative disorders in rheumatoid arthritis: Histology, Epstein-Barr virus, and clonality are important predictors of disease progression and regression. Eur. J. Haematol. 2013, 91, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Ichikawa, A.; Umezawa, N.; Yamamoto, K.; Yoshifuji, K.; Okada, K.; Nogami, A.; Umezawa, Y.; Nagao, T.; Sakashita, C.; et al. Lymphoproliferative disorder risk after methotrexate treatment for rheumatoid arthritis. Cancer Sci. 2023, 114, 3719–3727. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.S.; Chia, F.; Dans, L.; Harrison, A.; Hsieh, T.Y.; Jain, R.; Jung, S.M.; Kishimoto, M.; Kumar, A.; Leong, K.P.; et al. 2018 update of the APLAR recommendations for treatment of rheumatoid arthritis. Int. J. Rheum. Dis. 2019, 22, 357–375. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Takeuchi, T. Immune response in LPD during methotrexate administration (MTX-LPD) in rheumatoid arthritis patients. J. Clin. Exp. Hematop. 2019, 59, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Ellman, M.H.; Hurwitz, H.; Thomas, C.; Kozloff, M. Lymphoma developing in a patient with rheumatoid arthritis taking low dose weekly methotrexate. J. Rheumatol. 1991, 18, 1741–1743. [Google Scholar]
- Koens, L.; Senff, N.J.; Vermeer, M.H.; Willemze, R.; Jansen, P.M. Methotrexate-associated B-cell lymphoproliferative disorders presenting in the skin: A clinicopathologic and immunophenotypical study of 10 cases. Am. J. Surg. Pathol. 2014, 38, 999–1006. [Google Scholar] [CrossRef]
- Hashimoto, A.; Chiba, N.; Tsuno, H.; Komiya, A.; Furukawa, H.; Matsui, T.; Nishino, J.; Tohma, S. Incidence of malignancy and the risk of lymphoma in Japanese patients with rheumatoid arthritis compared to the general population. J. Rheumatol. 2015, 42, 564–571. [Google Scholar] [CrossRef]
- Gaulard, P.; Swerdlow, S.H.; Harris, N.L.; Jaffe, E.S.; Christer, S.; International Agency for Research on Cancer. WHO classification of tumours of haematopoietic and lymphoid tissues. In WHO Classification of Tumours, 4th ed.; Swerdlow, S.H., Harris, N.L., Jaffe, E.S., Pileri, S.A., Harald, S., Jurgen, T., Eds.; International Agency for Research on Cancer: Lyon, France, 2017; pp. 462–464. [Google Scholar]
- Momose, S.; Tamaru, J.I. Iatrogenic immunodeficiency-associated lymphoproliferative disorders of B-cell type that develop in patients receiving immunosuppressive drugs other than in the post-transplant setting. J. Clin. Exp. Hematop. 2019, 59, 48–55. [Google Scholar] [CrossRef]
- Tokuhira, M.; Saito, S.; Suzuki, K.; Higashi, M.; Momose, S.; Shimizu, T.; Mori, T.; Kimura, Y.; Amano, K.; Okamoto, S.; et al. Clinicopathological features of clinical methotrexate-related lymphoproliferative disorders. Leuk. Lymphoma 2019, 60, 2508–2515. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Amado, C.; Anagnostopoulo, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, A.M.; Boyer, D.; Calaminici, M.; Chadurn, A.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef] [PubMed]
- Kaji, D.; Kusakabe, M.; Sakata-Yanagimoto, M.; Makishima, K.; Suehara, Y.; Hattori, K.; Ota, Y.; Mitsuki, T.; Yuasa, M.; Kageyama, K.; et al. Retrospective analyses of other iatrogenic immunodeficiency-associated lymphoproliferative disorders in patients with rheumatic diseases. Br. J. Haematol. 2021, 195, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Salloum, E.; Cooper, D.L.; Howe, G.; Lacy, J.; Tallini, G.; Crouch, J.; Schultz, M.; Murren, J. Spontaneous regression of lymphoproliferative disorders in patients treated with methotrexate for rheumatoid arthritis and other rheumatic diseases. J. Clin. Oncol. 1996, 14, 1943–1949. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, K.; Hatanaka, K.C.; Hatanaka, Y.; Kasahara, I.; Yamamoto, S.; Tsuji, T.; Nakata, M.; Takakuwa, Y.; Haseyama, Y.; Oyamada, Y.; et al. Association of Epstein-Barr virus with regression after withdrawal of immunosuppressive drugs and subsequent progression of iatrogenic immunodeficiency-associated lymphoproliferative disorders in patients with autoimmune diseases. Hematol. Oncol. 2020, 38, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Satou, A.; Banno, S.; Kohno, K.; Takahara, T.; Takahashi, E.; Nobata, H.; Iwagaitsu, S.; Watanabe, D.; Hanamura, I.; Takami, A.; et al. Primary cutaneous methotrexate-associated B-cell lymphoproliferative disorders other than EBV-positive mucocutaneous ulcer: Clinical, pathological, and immunophenotypic features. Pathology 2021, 53, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Saito, K.; Nawata, A.; Hanami, K.; Kubo, S.; Miyagawa, I.; Fujino, Y.; Nakayamada, S.; Tanaka, Y. Clinical aspects in patients with rheumatoid arthritis complicated with lymphoproliferative disorders without regression after methotrexate withdrawal and treatment for arthritis after regression of lymphoproliferative disorders. Mod. Rheumatol. 2021, 31, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, N.; Sugiyama, K.; Nagasawa, Y.; Hamaguchi, M.; Kobayashi, H.; Takei, M. Involvement of Epstein-Barr virus in the development and spontaneous regression of methotrexate-associated lymphoproliferative disorder in patients with rheumatoid arthritis. Clin. Exp. Rheumatol. 2022, 40, 1330–1335. [Google Scholar] [CrossRef] [PubMed]
- Kuramoto, N.; Saito, S.; Fujii, T.; Kaneko, Y.; Saito, R.; Tanaka, M.; Takada, H.; Nakano, K.; Saito, K.; Sugimoto, N.; et al. Characteristics of rheumatoid arthritis with immunodeficiency-associated lymphoproliferative disorders to regress spontaneously by the withdrawal of methotrexate and their clinical course: A retrospective, multicenter, case-control study. Mod. Rheumatol. 2022, 32, 24–31. [Google Scholar] [CrossRef]
- Hoshida, Y.; Tsujii, A.; Ohshima, S.; Saeki, Y.; Yagita, M.; Miyamura, T.; Katayama, M.; Kawasaki, T.; Hiramatsu, Y.; Oshima, H.; et al. The effect of recent antirheumatic drug on features of rheumatoid arthritis-associated lymphoproliferative disorders. Arthritis Rheumatol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Gion, Y.; Iwaki, N.; Takata, K.; Takeuchi, M.; Nishida, K.; Orita, Y.; Tachibana, T.; Yoshino, T.; Sato, Y. Clinicopathological analysis of methotrexate-associated lymphoproliferative disorders: Comparison of diffuse large B-cell lymphoma and classical Hodgkin lymphoma types. Cancer Sci. 2017, 108, 1271–1280. [Google Scholar] [CrossRef]
- Gion, Y.; Doi, M.; Nishimura, Y.; Ikeda, T.; Filiz Nishimura, M.; Sakamoto, M.; Egusa, Y.; Nishikori, A.; Fujita, A.; Iwaki, N.; et al. PD-L1 expression is associated with the spontaneous regression of patients with methotrexate-associated lymphoproliferative disorders. Cancer Med. 2022, 11, 417–432. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.; Patel, S.P.; Kurzrock, R. PD-1-PD-L1 immune-checkpoint blockade in B-cell lymphomas. Nat. Rev. Clin. Oncol. 2017, 14, 203–220. [Google Scholar] [CrossRef] [PubMed]
- Roemer, M.G.; Advani, R.H.; Ligon, A.H.; Natkunam, Y.; Redd, R.A.; Homer, H.; Connelly, C.F.; Sun, H.H.; Daadi, S.E.; Freeman, G.J.; et al. PD-L1 and PD-L2 Genetic Alterations Define Classical Hodgkin Lymphoma and Predict Outcome. J. Clin. Oncol. 2016, 34, 2690–2697. [Google Scholar] [CrossRef] [PubMed]
- Shiraiwa, S.; Kikuti, Y.Y.; Carreras, J.; Kondo, Y.; Ohmachi, K.; Ogawa, Y.; Kawada, H.; Sato, S.; Gion, Y.; Sato, Y.; et al. 9p24.1 Genetic Alteration and PD-L1 Expression Are Characteristic of De Novo and Methotrexate-associated Epstein-Barr Virus-positive Hodgkin Lymphoma, But Not Methotrexate-associated Hodgkin-like Lesions. Am. J. Surg. Pathol. 2022, 46, 1017–1024. [Google Scholar] [CrossRef]
- Kurita, D.; Miyoshi, H.; Ichikawa, A.; Kato, K.; Imaizumi, Y.; Seki, R.; Sato, K.; Sasaki, Y.; Kawamoto, K.; Shimono, J.; et al. Methotrexate-associated Lymphoproliferative Disorders in Patients With Rheumatoid Arthritis: Clinicopathologic Features and Prognostic Factors. Am. J. Surg. Pathol. 2019, 43, 869–884. [Google Scholar] [CrossRef]
- Gerhard-Hartmann, E.; Goergen, H.; Bröckelmann, P.J.; Mottok, A.; Steinmüller, T.; Grund, J.; Zamò, A.; Ben-Neriah, S.; Sasse, S.; Borchmann, S.; et al. 9p24.1 alterations and programmed cell death 1 ligand 1 expression in early stage unfavourable classical Hodgkin lymphoma: An analysis from the German Hodgkin Study Group NIVAHL trial. Br. J. Haematol. 2022, 196, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Paydas, S.; Bağır, E.; Seydaoglu, G.; Ercolak, V.; Ergin, M. Programmed death-1 (PD-1), programmed death-ligand 1 (PD-L1), and EBV-encoded RNA (EBER) expression in Hodgkin lymphoma. Ann. Hematol. 2015, 94, 1545–1552. [Google Scholar] [CrossRef]
- Green, M.R.; Rodig, S.; Juszczynski, P.; Ouyang, J.; Sinha, P.; O’Donnell, E.; Neuberg, D.; Shipp, M.A. Constitutive AP-1 activity and EBV infection induce PD-L1 in Hodgkin lymphomas and posttransplant lymphoproliferative disorders: Implications for targeted therapy. Clin. Cancer Res. 2012, 18, 1611–1618. [Google Scholar] [CrossRef]
- Kume, A.; Shinozaki-Ushiku, A.; Kunita, A.; Kondo, A.; Ushiku, T. Enhanced PD-L1 Expression in LMP1-positive Cells of Epstein-Barr Virus-associated Malignant Lymphomas and Lymphoproliferative Disorders: A Single-cell Resolution Analysis With Multiplex Fluorescence Immunohistochemistry and In Situ Hybridization. Am. J. Surg. Pathol. 2022, 46, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Gamaleldin, M.A.; Ghallab, O.M.; Nadwan, E.A.; Abo Elwafa, R.A. PD-1 and PD-L1 gene expressions and their association with Epstein-Barr virus infection in chronic lymphocytic leukemia. Clin. Transl. Oncol. 2021, 23, 2309–2322. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Nishikawa, J.; Sakai, K.; Iizasa, H.; Yoshiyama, H.; Yanagihara, M.; Shuto, T.; Shimokuri, K.; Kanda, T.; Suehiro, Y.; et al. EBV-associated gastric cancer evades T-cell immunity by PD-1/PD-L1 interactions. Gastric Cancer 2019, 22, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, W. Expression of PD-L1 in EBV-associated malignancies. Int. Immunopharmacol. 2021, 95, 23. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H.; Saito, M.; Nakajima, S.; Saito, K.; Nakayama, Y.; Kase, K.; Yamada, L.; Kanke, Y.; Hanayama, H.; Onozawa, H.; et al. PD-L1 overexpression in EBV-positive gastric cancer is caused by unique genomic or epigenomic mechanisms. Sci. Rep. 2021, 11, 1982. [Google Scholar] [CrossRef]
- Zhang, W.T.; Zhu, G.L.; Xu, W.Q.; Zhang, W.; Wang, H.Z.; Wang, Y.B.; Li, Y.X. Association of PD-1/PD-L1 expression and Epstein--Barr virus infection in patients with invasive breast cancer. Diagn. Pathol. 2022, 17, 61. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt. No | Age/ Sex | Primary Basal Disease | Anti-RA Drugs at the Time of LPD Development | Clinical Stage | Extranodal Involvement Site | EBER/ Latency Pattern | Response after MTX Withdrawal | Relapse after MTX Withdrawal | Time to Chemotherapy (Month) | Chemotherapy | Duration after Dx (Year) | Alive/ Dead | Cause of Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 67/F | RA | MTX | II | - | I | SD | + | 2.8 | ABVD | 1.92 | Dead | DIC, PBC |
| 2 | 70/M | RA | MTX | IV | lung, bone | II | PR | - | - | - | 2.69 | Alive | |
| 3 | 67/M | RA | MTX, PSL, Sodium Aurothiomalate | NR | - | II | CR | - | - | - | 2.34 | Alive | |
| 4 | 45/F | RA | MTX | IV | bone marrow | II | PD | - | 0.1 | Rituximab, ADR, CP | 0.24 | Dead | PD |
| 5 | 68/F | RA | MTX, PSL | IV | adrenal gland | II | PR | NR | - | - | 0.18 | Alive | |
| 6 | 77/F | RA | MTX, PSL, BUC | IV | lung, liver, adrenal gland | EBER- | SD | + | 44.0 | A-AVD | 4.00 | Alive | |
| 7 | 43/M | RA | MTX | IV | lung | I | SD | + | 1.0 | ABVD | 4.83 | Alive | |
| 8 | 79/F | RA | MTX, SSZ, PSL | III | II | NR | NR | NR | A-AVD | 0.25 | Dead | Unk | |
| 9 | 71/F | RA | MTX, PSL, SSZ, TAC | IV | lung, pleural effusion | II | SD | + | 8.0 | C-MOPP | 0.25 | Dead | PD |
| 10 | 69/F | RA | SASP, PSL, MTX, BUC | III | - | EBER- | CR | + | 9.0 | ABVD | 0.58 | Dead | PD |
| 11 | 59/F | RA | MTX, TAC, ETN, Abatacept, TCZ, SASP, PSL, peficitinib | IV | paravertebral | EBER- | PR | + | 34.0 | ABVD | 9.75 | Alive | |
| 12 | 41/M | SAPHO synd. | MTX, PSL, INF | I | - | II | CR | + | 17.0 | ABVD | 5.96 | Alive | |
| 13 | 70/F | RA | MTX, TAC, ETN, ADA, TCZ | III | - | II | SD | + | 16.0 | ABVD | 4.50 | Alive | |
| 14 | 57/F | RA | MTX, CyA, TAC, INF, ADA, TCZ | I | - | EBER- | CR | + | 9.0 | ABVD | 6.42 | Alive | |
| 15 | 63/F | RA | MTX, PSL | III | - | II | CR | + | 1.4 | ABVD | 2.07 | Alive | |
| 16 | 67/M | RA | MTX, MZB, SSZ | III | - | II | PR | + | 23.0 | A-AVD | 3.17 | Alive | |
| 17 | 64/M | RA | MTX, PSL, BUC | III | - | II | CR | + | 8.0 | ABVD | 5.17 | Dead | PD |
| 18 | 48/F | RA | MTX, PSL, TAC | III | - | EBER- | SD | NR | 1.2 | ABVD | 9.03 | Alive | |
| 19 | 65/M | RA | MTX | I | - | II | PR | - | - | - | 14.08 | Alive | |
| 20 | 68/F | RA | MTX, PSL, TAC | II | - | II | PD | - | 27.8 | ABVD | 9.50 | Alive | |
| 21 | 82/F | RA | MTX | III | - | II | CR | - | - | - | 1.07 | Alive | |
| 22 | 79/F | RA | MTX | III | - | II | PR | + | 7.6 | ABVD | 1.84 | Alive | |
| 23 | 61/F | RA | MTX, | I | - | II | PR | + | 25.0 | CP | 2.16 | Dead | PD |
| 24 | 57/M | RA | MTX, PSL | II | - | ND | PD | - | 2.3 | R-CHOP | 1.02 | Alive | |
| 25 | 81/F | RA | MTX, ETN, PSL | II | - | II | SD | + | - | - | 0.58 | Dead | PD |
| 26 | 71/F | RA | MTX, PSL | III | - | II | PR | + | - | - | 1.67 | Alive | |
| 27 | 79/M | RA | BUC, MTX, SSZ, TAC | III | - | II | PR | + | - | - | 0.08 | Dead | PD |
| ALL | Copy Gain | Amp | p-Value | ||
|---|---|---|---|---|---|
| N | 27 | 11 | 16 | ||
| Clinical features | Age (range) | 67 (41–82) | 68 (43–79) | 66 (41–82) | 0.9516 |
| Sex (M/F) | 9/18 | 3/8 | 6/10 | 0.6828 | |
| LDH > normal upper range | 12/25 (148–442) | 4/10 (196–390) | 8/15 (148–442) | 0.9902 | |
| sIL2R > normal upper range | 21/23 (409–4981) | 8/10 (409–4000) | 13/13 (486–4981) | 0.4833 | |
| PS ≥ 2 | 15.0% (3/20) | 25.0% (2/8) | 8.3% (1/12) | 0.5368 | |
| Clinical stage ≥ 3 | 69.2% (18/26) | 90.0% (9/10) | 56.3% (9/16) | 0.0989 | |
| Clinical stage 3 | 42.3% (11/26) | 20.0% (2/10) | 56.3% (9/16) | 0.0687 | |
| Ratio of extranodal Involvement | 26.9% (7/26) | 70% (7/10) | 0% (0/16) | 0.0002 | |
| B symptom positive | 71.4% (15/21) | 88.9% (8/9) | 58.3% (7/12) | 0.1778 | |
| EBER positive | 80.8% (21/26) | 72.7% (8/11) | 86.7% (13/15) | 0.6196 | |
| MTX | 100% (27/27) | 100% (11/11) | 100% (16/16) | 1 | |
| Anti-RA drugs at the time of LPD development | Prednisolone | 55.6% (15/27) | 63.6% (7/11) | 50.0% (8/16) | 0.696 |
| Tacrolimus | 25.9% (7/27) | 18.2% (2/11) | 31.3% (5/16) | 0.6618 | |
| Other immunosuppressive drugs | 51.9% (14/27) | 54.5% (6/11) | 50.0% (8/16) | 1 | |
| Regression | 61.5% (16/26) | 50.0% (5/10) | 68.8% (11/16) | 0.425 | |
| Clinical response after MTX discontinuation | Ratio | 69.2% (18/26) | 70.0% (7/10) | 68.8% (11/16) | 1 |
| Chemotherapy after MTX-LPD | Response: CR/PR | 81.3% (13/16) | 71.4% (5/7) | 88.9% (8/9) | 0.55 |
| Alive/Dead | 18/9 | 6/5 | 12/4 | 0.4105 |
| ALL | Copy Gain | Amp | p-Value | ||
|---|---|---|---|---|---|
| N | 27 | 11 | 16 | ||
| CD30 | 100% (27/27) | 100% (11/11) | 100% (16/16) | 1 | |
| CD15 | 72.7% (16/22) | 50.0% (4/8) | 85.7% (12/14) | 0.1365 | |
| CD20 | 37.0% (10/27) | 36.4% (4/11) | 37.5% (6/16) | 1 | |
| CD79a | 37.0% (10/27) | 45.5% (5/11) | 31.3% (5/16) | 0.6868 | |
| PD-L1 | 100% (27/27) | 100% (11/11) | 100% (16/16) | 1 | |
| PD-L1 | Score 1 | 29.6% (8/27) | 36.4% (4/11) | 25% (4/16) | 0.5873 |
| Score 2 | 3.7% (1/27) | 9.1% (1/11) | 0% (0/16) | ||
| Score 3 | 14.8% (4/27) | 9.1% (1/11) | 18.8% (3/16) | ||
| Score 4 | 51.9% (14/27) | 45.5% (5/11) | 56.3% (9/16) | ||
| EBER-ISH | 81.5% (22/27) | 72.7% (8/11) | 87.5% (14/16) | 0.3705 | |
| LMP-1 | 73.1% (19/26) | 54.5% (6/11) | 77.8% (13/15) | 0.0946 | |
| EBNA2 | 0.00% (0/15) | 0.00% (0/7) | 0.00% (0/8) | 1 | |
| Latency | type I | 9.5% (2/21) | 25% (2/8) | 0% (0/13) | 0.1333 |
| type II | 90.5% (19/21) | 75% (6/8) | 100% (13/13) | ||
| type III | - | - | - | ||
| Case No. | H-Score | Ave. Score | % of PD-L1positive HRS Cells |
|---|---|---|---|
| 9 | 0.24 | 0.06 | 4 |
| 3 | 0.36 | 0.06 | 6 |
| 19 | 0.64 | 0.08 | 8 |
| 21 | 0.64 | 0.08 | 8 |
| 14 | 2.20 | 0.22 | 10 |
| 23 | 4.00 | 0.33 | 12 |
| 2 | 4.88 | 0.33 | 15 |
| 6 | 7.28 | 0.28 | 26 |
| 7 | 11.52 | 0.48 | 24 |
| 12 | 49.28 | 0.88 | 56 |
| 22 | 53.04 | 1.02 | 52 |
| 5 | 67.00 | 0.85 | 79 |
| 1 | 77.52 | 1.02 | 76 |
| 8 | 82.36 | 1.42 | 58 |
| 18 | 92.01 | 1.28 | 72 |
| 17 | 112.00 | 1.40 | 80 |
| 20 | 133.92 | 1.86 | 72 |
| 4 | 152.00 | 1.90 | 80 |
| 11 | 174.18 | 2.08 | 84 |
| 15 | 184.52 | 1.91 | 96 |
| 16 | 209.84 | 2.44 | 86 |
| 26 | 210.60 | 2.34 | 90 |
| 13 | 240.00 | 2.40 | 100 |
| 25 | 260.00 | 2.60 | 100 |
| 24 | 268.00 | 2.68 | 100 |
| 10 | 270.48 | 2.76 | 98 |
| 27 | 276.48 | 2.88 | 96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohsawa, K.; Momose, S.; Nishikori, A.; Nishimura, M.F.; Gion, Y.; Sawada, K.; Higashi, M.; Tokuhira, M.; Tamaru, J.-i.; Sato, Y. Copy Number Analysis of 9p24.1 in Classic Hodgkin Lymphoma Arising in Immune Deficiency/Dysregulation. Cancers 2024, 16, 1298. https://doi.org/10.3390/cancers16071298
Ohsawa K, Momose S, Nishikori A, Nishimura MF, Gion Y, Sawada K, Higashi M, Tokuhira M, Tamaru J-i, Sato Y. Copy Number Analysis of 9p24.1 in Classic Hodgkin Lymphoma Arising in Immune Deficiency/Dysregulation. Cancers. 2024; 16(7):1298. https://doi.org/10.3390/cancers16071298
Chicago/Turabian StyleOhsawa, Kumiko, Shuji Momose, Asami Nishikori, Midori Filiz Nishimura, Yuka Gion, Keisuke Sawada, Morihiro Higashi, Michihide Tokuhira, Jun-ichi Tamaru, and Yasuharu Sato. 2024. "Copy Number Analysis of 9p24.1 in Classic Hodgkin Lymphoma Arising in Immune Deficiency/Dysregulation" Cancers 16, no. 7: 1298. https://doi.org/10.3390/cancers16071298
APA StyleOhsawa, K., Momose, S., Nishikori, A., Nishimura, M. F., Gion, Y., Sawada, K., Higashi, M., Tokuhira, M., Tamaru, J.-i., & Sato, Y. (2024). Copy Number Analysis of 9p24.1 in Classic Hodgkin Lymphoma Arising in Immune Deficiency/Dysregulation. Cancers, 16(7), 1298. https://doi.org/10.3390/cancers16071298