
A Biopsy-Controlled Prospective Study of Contrast-Enhancing Diffuse Glioma Infiltration Based on FET-PET and FLAIR
 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Ethical Approval and Consent
2.2. Patients and Inclusion and Exclusion Criteria
2.3. FET-PET Acquisition and Evaluation
2.4. Classification Tree for Differential Diagnoses
2.5. Statistical Analysis
3. Results
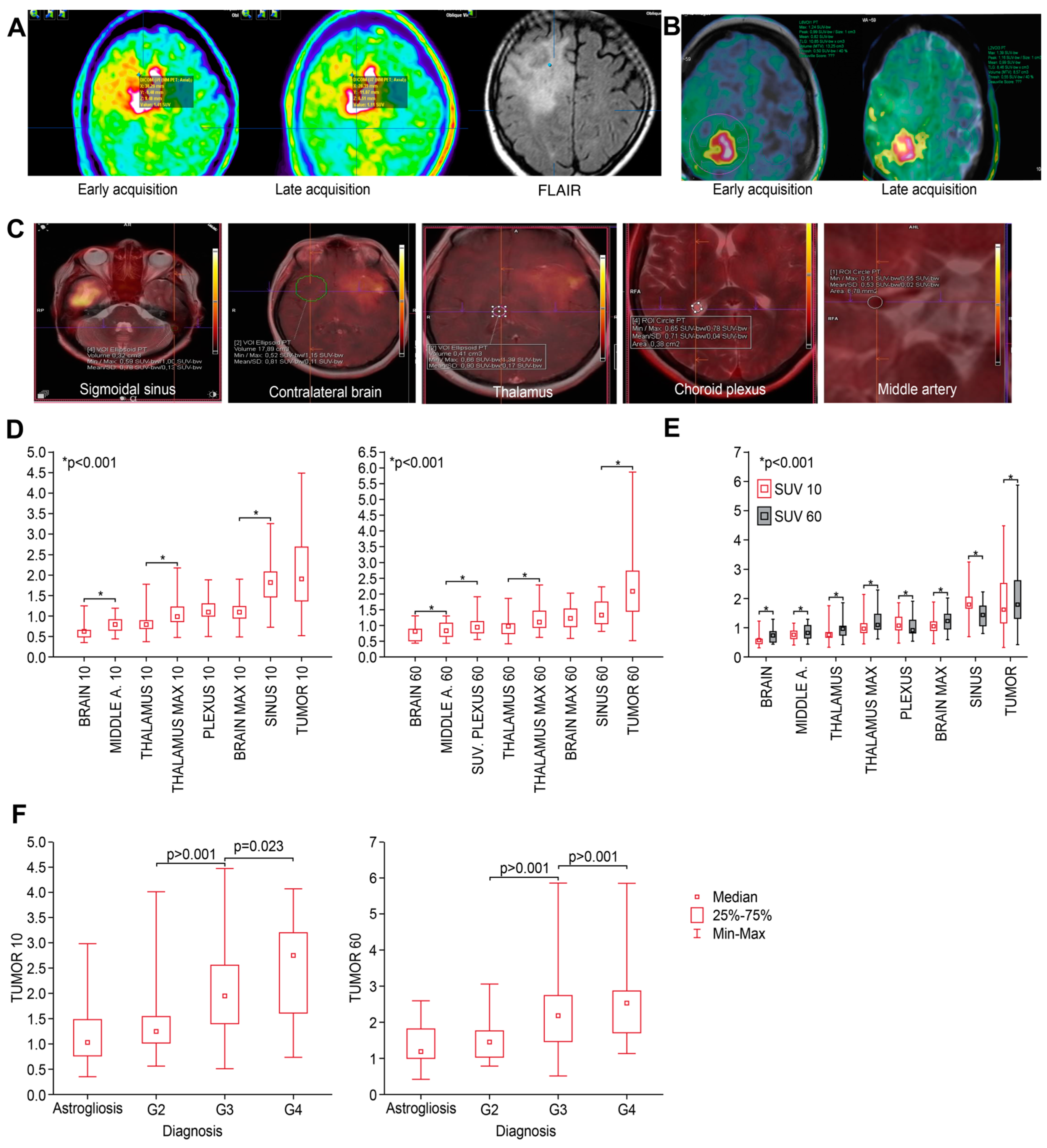
3.1. SUVs and TBR Values 10 and 60 min a.r.i. According to Biopsy Site
3.2. Differences in SUVs between Different Anatomical Structures at 10 and 60 min
3.3. Differences in SUV Related to Tumor Grade
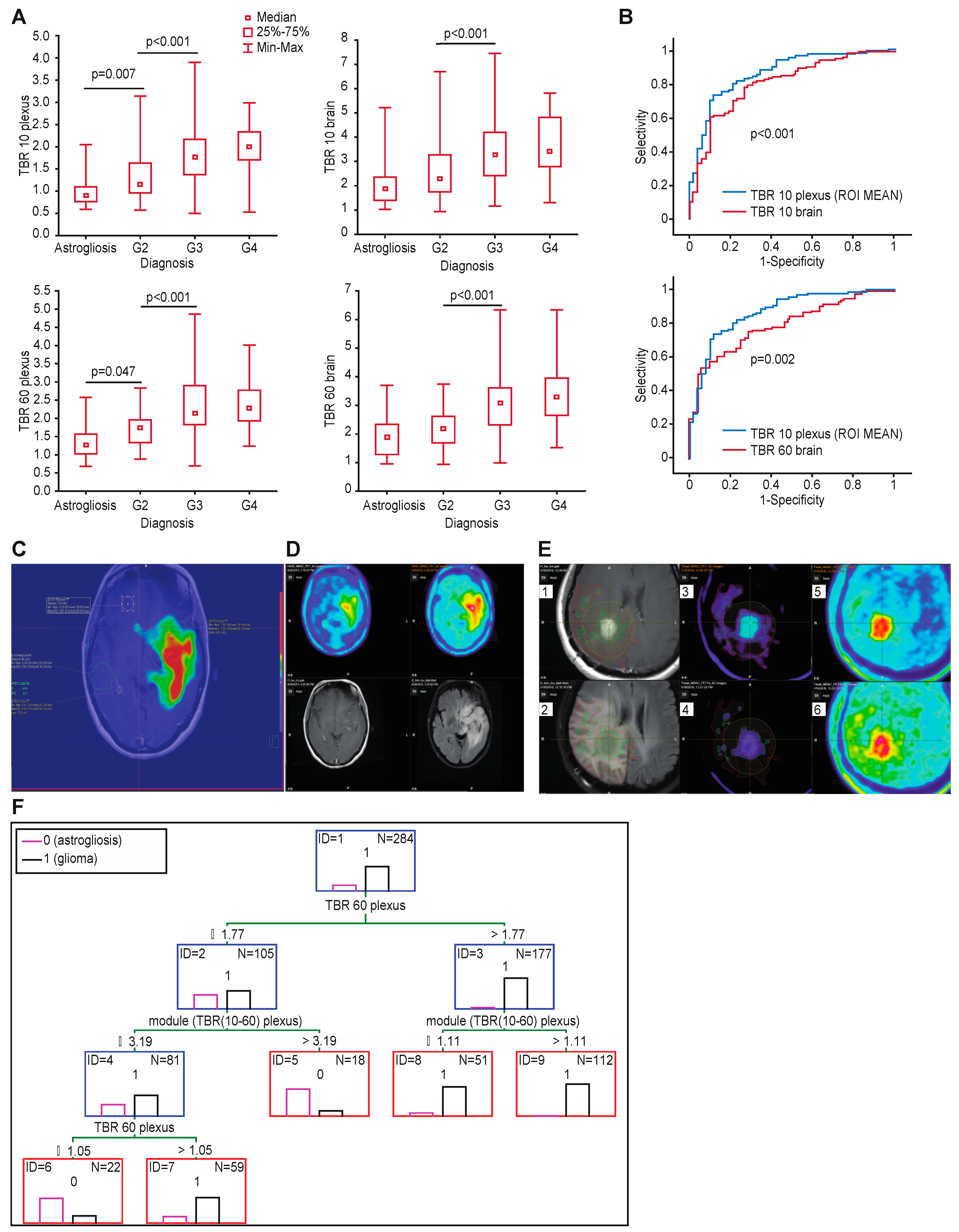
3.4. Target-to-Background Ratios
3.5. Accuracy of Differentiating Tumor from Astrogliosis
3.6. Infiltration Defined by Standard (Single) Acquisition of FET-PET
3.7. Infiltration Defined Using Different Background Reference Structures
3.8. Comparison of Different Tumor-to-Background Ratios
3.9. Infiltration Defined by Dual Acquisition
3.10. Classification Trees to Differentiate Tumor and Astrogliosis at the Tumor Border
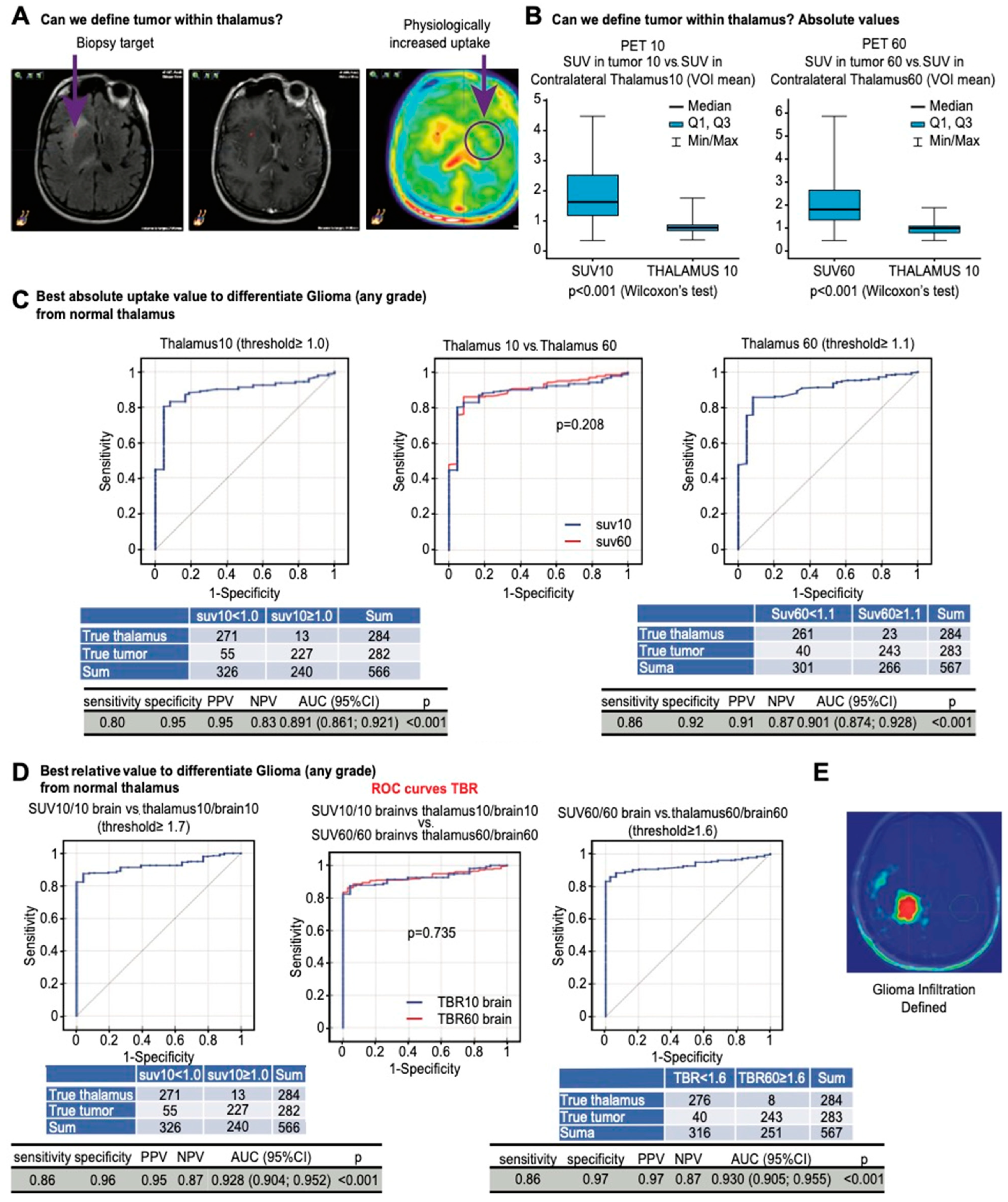
3.11. Differentiating Tumor Infiltration within Thalamus
3.12. Software Impact on Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro-Oncology 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Harat, M.; Malkowski, B.; Wiatrowska, I.; Makarewicz, R.; Roszkowski, K. Relationship between Glioblastoma Dose Volume Parameters Measured by Dual Time Point Fluoroethylthyrosine-PET and Clinical Outcomes. Front. Neurol. 2017, 8, 756. [Google Scholar] [CrossRef] [PubMed]
- Pope, W.B.; Brandal, G. Conventional and advanced magnetic resonance imaging in patients with high-grade glioma. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.R.; Jayamanne, D.; Hsiao, E.; Schembri, G.P.; Bailey, D.L.; Roach, P.J.; Khasraw, M.; Newey, A.; Wheeler, H.R.; Back, M. Utilizing 18F-fluoroethyltyrosine (FET) positron emission tomography (PET) to define suspected nonenhancing tumor for radiation therapy planning of glioblastoma. Pract. Radiat. Oncol. 2018, 8, 230–238. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Central Nervous System Cancers (Version 1.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/cns.pdf (accessed on 26 August 2022).
- Cordova, J.S.; Shu, H.K.; Liang, Z.; Gurbani, S.S.; Cooper, L.A.; Holder, C.A.; Olson, J.J.; Kairdolf, B.; Schreibmann, E.; Neill, S.G.; et al. Whole-brain spectroscopic MRI biomarkers identify infiltrating margins in glioblastoma patients. Neuro-Oncology 2016, 18, 1180–1189. [Google Scholar] [CrossRef]
- Watanabe, M.; Tanaka, R.; Takeda, N. Magnetic resonance imaging and histopathology of cerebral gliomas. Neuroradiology 1992, 34, 463–469. [Google Scholar] [CrossRef]
- Laino, M.E.; Young, R.; Beal, K.; Haque, S.; Mazaheri, Y.; Corrias, G.; Bitencourt, A.G.; Karimi, S.; Thakur, S.B. Magnetic resonance spectroscopic imaging in gliomas: Clinical diagnosis and radiotherapy planning. BJR Open 2020, 2, 20190026. [Google Scholar] [CrossRef]
- Rose, S.; Fay, M.; Thomas, P.; Bourgeat, P.; Dowson, N.; Salvado, O.; Gal, Y.; Coulthard, A.; Crozier, S. Correlation of MRI-derived apparent diffusion coefficients in newly diagnosed gliomas with [18F]-fluoro-L-dopa PET: What are we really measuring with minimum ADC? AJNR Am. J. Neuroradiol. 2013, 34, 758–764. [Google Scholar] [CrossRef]
- de Leeuw, C.N.; Vogelbaum, M.A. Supratotal resection in glioma: A systematic review. Neuro-Oncology 2019, 21, 179–188. [Google Scholar] [CrossRef]
- Galldiks, N.; Langen, K.-J.; Pope, W.B. From the clinician’s point of view-What is the status quo of positron emission tomography in patients with brain tumors? Neuro-Oncology 2015, 17, 1434–1444. [Google Scholar] [CrossRef]
- Langen, K.J.; Galldiks, N.; Lohmann, P. Combined FET PET/ADC mapping: Improved imaging of glioma infiltration? Neuro-Oncology 2020, 22, 313–314. [Google Scholar] [CrossRef]
- Ort, J.; Hamou, H.A.; Kernbach, J.M.; Hakvoort, K.; Blume, C.; Lohmann, P.; Galldiks, N.; Heiland, D.H.; Mottaghy, F.M.; Clusmann, H. 18F-FET-PET-guided gross total resection improves overall survival in patients with WHO grade III/IV glioma: Moving towards a multimodal imaging-guided resection. J. Neuro-Oncol. 2021, 155, 71–80. [Google Scholar] [CrossRef]
- Pirotte, B.J.; Levivier, M.; Goldman, S.; Massager, N.; Wikler, D.; Dewitte, O.; Bruneau, M.; Rorive, S.; David, P.; Brotchi, J. Positron emission tomography-guided volumetric resection of supratentorial high-grade gliomas: A survival analysis in 66 consecutive patients. Neurosurgery 2009, 64, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Harat, M.; Rakowska, J.; Harat, M.; Szylberg, T.; Furtak, J.; Miechowicz, I.; Malkowski, B. Combining amino acid PET and MRI imaging increases accuracy to define malignant areas in adult glioma. Nat. Commun. 2023, 14, 4572. [Google Scholar] [CrossRef] [PubMed]
- Hamacher, K.; Coenen, H.H. Efficient routine production of the 18F-labelled amino acid O-2-18F fluoroethyl-L-tyrosine. Appl. Radiat. Isot. 2002, 57, 853–856. [Google Scholar] [CrossRef] [PubMed]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; la Fougere, C.; Langen, K.J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [(18)F]FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Schmalenbach, M.; Jungehülsing, M.; Theissen, P.; Dietlein, M.; Schröder, U.; Eschner, W.; Stennert, E.; Schicha, H. 18F-FDG PET for detecting recurrent head and neck cancer, local lymph node involvement and distant metastases. Nuklearmedizin-NuclearMedicine 2004, 43, 91–101. [Google Scholar]
- Breiman, L. Classification and Regression Trees; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Tufféry, S. Data Mining and Statistics for Decision Making; John Wiley & Sons: West Sussex, UK, 2011. [Google Scholar]
- Unterrainer, M.; Eze, C.; Ilhan, H.; Marschner, S.; Roengvoraphoj, O.; Schmidt-Hegemann, N.S.; Walter, F.; Kunz, W.G.; Rosenschold, P.M.A.; Jeraj, R.; et al. Recent advances of PET imaging in clinical radiation oncology. Radiat. Oncol. 2020, 15, 88. [Google Scholar] [CrossRef] [PubMed]
- Calcagni, M.L.; Galli, G.; Giordano, A.; Taralli, S.; Anile, C.; Niesen, A.; Baum, R.P. Dynamic O-(2-[18F] fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma grading: Assessment of individual probability of malignancy. Clin. Nucl. Med. 2011, 36, 841–847. [Google Scholar] [CrossRef]
- Pöpperl, G.; Kreth, F.W.; Mehrkens, J.H.; Herms, J.; Seelos, K.; Koch, W.; Gildehaus, F.J.; Kretzschmar, H.A.; Tonn, J.C.; Tatsch, K. FET PET for the evaluation of untreated gliomas: Correlation of FET uptake and uptake kinetics with tumour grading. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1933–1942. [Google Scholar] [CrossRef]
- Weckesser, M.; Langen, K.J.; Rickert, C.H.; Kloska, S.; Straeter, R.; Hamacher, K.; Kurlemann, G.; Wassmann, H.; Coenen, H.H.; Schober, O. O-(2-[18F]fluorethyl)-L-tyrosine PET in the clinical evaluation of primary brain tumours. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 422–429. [Google Scholar] [CrossRef]
- Fuenfgeld, B.; Machler, P.; Fischer, D.R.; Esposito, G.; Rushing, E.J.; Kaufmann, P.A.; Stolzmann, P.; Huellner, M.W. Reference values of physiological 18F-FET uptake: Implications for brain tumor discrimination. PLoS ONE 2020, 15, e0230618. [Google Scholar] [CrossRef]
- Pauleit, D.; Floeth, F.; Hamacher, K.; Riemenschneider, M.J.; Reifenberger, G.; Müller, H.-W.; Zilles, K.; Coenen, H.H.; Langen, K.-J. O-(2-[18F] fluoroethyl)-L-tyrosine PET combined with MRI improves the diagnostic assessment of cerebral gliomas. Brain 2005, 128, 678–687. [Google Scholar] [CrossRef]
- Jansen, N.L.; Suchorska, B.; Wenter, V.; Schmid-Tannwald, C.; Todica, A.; Eigenbrod, S.; Niyazi, M.; Tonn, J.-C.; Bartenstein, P.; Kreth, F.-W. Prognostic significance of dynamic 18F-FET PET in newly diagnosed astrocytic high-grade glioma. J. Nucl. Med. 2015, 56, 9–15. [Google Scholar] [CrossRef]
- Lohmann, P.; Stavrinou, P.; Lipke, K.; Bauer, E.K.; Ceccon, G.; Werner, J.-M.; Neumaier, B.; Fink, G.R.; Shah, N.J.; Langen, K.-J. FET PET reveals considerable spatial differences in tumour burden compared to conventional MRI in newly diagnosed glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 591–602. [Google Scholar] [CrossRef]
- Lohmann, P.; Piroth, M.D.; Sellhaus, B.; Weis, J.; Geisler, S.; Oros-Peusquens, A.M.; Mohlberg, H.; Amunts, K.; Shah, N.J.; Galldiks, N.; et al. Correlation of Dynamic O-(2-[(18)F]Fluoroethyl)-L-Tyrosine Positron Emission Tomography, Conventional Magnetic Resonance Imaging, and Whole-Brain Histopathology in a Pretreated Glioblastoma: A Postmortem Study. World Neurosurg. 2018, 119, e653–e660. [Google Scholar] [CrossRef] [PubMed]
- Eidel, O.; Burth, S.; Neumann, J.-O.; Kieslich, P.J.; Sahm, F.; Jungk, C.; Kickingereder, P.; Bickelhaupt, S.; Mundiyanapurath, S.; Bäumer, P. Tumor infiltration in enhancing and non-enhancing parts of glioblastoma: A correlation with histopathology. PLoS ONE 2017, 12, e0169292. [Google Scholar] [CrossRef] [PubMed]
- Verburg, N.; Koopman, T.; Yaqub, M.M.; Hoekstra, O.S.; Lammertsma, A.A.; Barkhof, F.; Pouwels, P.J.W.; Reijneveld, J.C.; Heimans, J.J.; Rozemuller, A.J.M.; et al. Improved detection of diffuse glioma infiltration with imaging combinations: A diagnostic accuracy study. Neuro-Oncology 2020, 22, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Langen, K.-J.; Stoffels, G.; Filss, C.; Heinzel, A.; Stegmayr, C.; Lohmann, P.; Willuweit, A.; Neumaier, B.; Mottaghy, F.M.; Galldiks, N. Imaging of amino acid transport in brain tumours: Positron emission tomography with O-(2-[18F] fluoroethyl)-L-tyrosine (FET). Methods 2017, 130, 124–134. [Google Scholar] [CrossRef]
- Barry, N.; Francis, R.J.; Ebert, M.A.; Koh, E.S.; Rowshanfarzad, P.; Hassan, G.M.; Kendrick, J.; Gan, H.K.; Lee, S.T.; Lau, E.; et al. Delineation and agreement of FET PET biological volumes in glioblastoma: Results of the nuclear medicine credentialing program from the prospective, multi-centre trial evaluating FET PET In Glioblastoma (FIG) study-TROG 18.06. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3970–3981. [Google Scholar] [CrossRef] [PubMed]
- Stegmayr, C.; Stoffels, G.; Kops, E.R.; Lohmann, P.; Galldiks, N.; Shah, N.J.; Neumaier, B.; Langen, K.J. Influence of Dexamethasone on O-(2-[18F]-Fluoroethyl)-L-Tyrosine Uptake in the Human Brain and Quantification of Tumor Uptake. Mol. Imaging Biol. 2019, 21, 168–174. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patient | Number of Samples Analyzed from Each Trajectory | Final Histopathology Result (WHO 2021) | |||
|---|---|---|---|---|---|
| T1-Gad+ | PET+ | PET- | FLAIR+ | ||
| 1 | 7 | 8 | 0 | 8 | Oligodendroglioma, IDH-mutant, G3 |
| 2 | 8 | 8 | 0 | 7 | Astrocytoma, IDH-mutant, G3 |
| 3 | 7 | 8 | 6 | 3 | Oligodendroglioma, IDH-mutant, G3 |
| 4 | 5 | 4 | 0 | 4 | Astrocytoma IDH-mutant, G3 |
| 5 | 4 | 4 | 0 | 6 | Glioblastoma, IDH wildtype, G4 |
| 6 | 3 | 3 | 0 | 2 | Glioblastoma, NOS, G4 |
| 7 | 3 | 3 | 0 | 5 | Astrocytoma, IDH-mutant, G3 |
| 8 | 4 | 4 | 0 | 7 | Glioblastoma, NOS, G4 |
| 9 | 4 | 5 | 0 | 5 | Oligodendroglioma, IDH-mutant, G3 |
| 10 | 3 | 3 | 5 | 5 | Glioblastoma, IDH wildtype, G4 |
| 11 | 3 | 6 | 0 | 8 | Astrocytoma, NOS, G2 |
| 12 | 4 | 4 | 0 | 3 | Oligodendroglioma, IDH-mutant, G3 |
| 13 | 4 | 4 | 0 | 0 | Glioblastoma, IDH wildtype, G4 |
| 14 | 3 | 4 | 0 | 4 | Astrocytoma, IDH-mutant, G3 |
| 15 | 6 | 6 | 0 | 4 | Astrocytoma, IDH-mutant, G4 |
| 16 | 0 | 7 | 0 | 3 | Astrocytoma, IDH wildtype, G2 |
| 17 | 7 | 3 | 0 | 2 | Astrocytoma, IDH-mutant, G4 |
| 18 | 4 | 4 | 0 | 3 | Glioblastoma IDH wildtype G4 |
| 19 | 5 | 4 | 0 | 4 | Glioblastoma IDH wildtype G4 |
| 20 | 6 | 5 | 0 | 5 | Oligodendroglioma, IDH-mutant, G3 |
| 21 | 0 | 5 | 0 | 1 | Oligodendroglioma, IDH-mutant, G3 |
| 22 | 3 | 1 | 0 | 2 | Glioblastoma NOS, G4 |
| 23 | 0 | 7 | 0 | 3 | Astrocytoma, IDH-mutant, G4 |
| HP | Overall | T1-GAD | PET | PET- | FLAIR | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
| Astrogliosis | 54 | 19 | 4 | 4 | 9 | 8 | 3 | 27 | 38 | 53 |
| G2 | 45 | 16 | 5 | 6 | 21 | 19 | 6 | 55 | 13 | 18 |
| G3 | 125 | 44 | 55 | 60 | 51 | 46 | 2 | 18 | 17 | 24 |
| G4 | 60 | 21 | 27 | 30 | 29 | 27 | 0 | 0 | 4 | 5 |
| SUV | N | Mean | Median | Min | Max | Lower Q | Upper Q | SD |
|---|---|---|---|---|---|---|---|---|
| PLEXUS 10 | 23 | 1.12 | 1.07 | 0.48 | 1.86 | 0.91 | 1.28 | 0.31 |
| THALAMUS MAX 10 | 23 | 1.04 | 0.97 | 0.46 | 2.15 | 0.80 | 1.19 | 0.37 |
| THALAMUS | 23 | 0.77 | 0.77 | 0.35 | 1.76 | 0.60 | 0.86 | 0.27 |
| BRAIN 10 | 23 | 0.60 | 0.60 | 0.33 | 1.23 | 0.47 | 0.69 | 0.20 |
| BRAIN 10 MAX | 23 | 1.09 | 1.05 | 0.47 | 1.88 | 0.92 | 1.22 | 0.32 |
| Middle A. 10 | 23 | 0.78 | 0.77 | 0.42 | 1.17 | 0.64 | 0.90 | 0.19 |
| SINUS 10 | 23 | 1.88 | 1.92 | 0.71 | 3.25 | 1.45 | 2.08 | 0.55 |
| SINUS 60 | 23 | 1.46 | 1.45 | 0.82 | 2.23 | 1.07 | 1.83 | 0.41 |
| PLEXUS 60 | 23 | 0.98 | 0.91 | 0.56 | 1.92 | 0.76 | 1.13 | 0.31 |
| THALAMUS Max 60 | 22 | 1.17 | 1.10 | 0.63 | 2.30 | 0.90 | 1.39 | 0.40 |
| THALAMUS 60 | 23 | 0.90 | 0.88 | 0.43 | 1.86 | 0.72 | 1.05 | 0.30 |
| BRAIN 60 | 23 | 0.73 | 0.74 | 0.44 | 1.31 | 0.51 | 0.88 | 0.23 |
| BRAIN 60 MAX | 23 | 1.20 | 1.17 | 0.60 | 2.03 | 0.83 | 1.48 | 0.37 |
| MIDDLE A. 60 | 23 | 0.85 | 0.82 | 0.45 | 1.31 | 0.60 | 1.08 | 0.26 |
| HP | Timepoint | N | Mean | Median | Min | Max | Lower Q | Upper Q | SD |
|---|---|---|---|---|---|---|---|---|---|
| Astrogliosis | SUV10 | 52 | 1.12 | 1.04 | 0.34 | 2.98 | 0.76 | 1.47 | 0.54 |
| SUV60 | 53 | 1.40 | 1.21 | 0.43 | 2.61 | 1.02 | 1.83 | 0.57 | |
| G2 | SUV10 | 45 | 1.35 | 1.23 | 0.55 | 4.02 | 1.01 | 1.54 | 0.60 |
| SUV60 | 45 | 1.60 | 1.47 | 0.79 | 3.07 | 1.05 | 1.77 | 0.62 | |
| G3 | SUV10 | 125 | 2.05 | 1.96 | 0.50 | 4.47 | 1.39 | 2.55 | 0.89 |
| SUV60 | 125 | 2.27 | 2.18 | 0.53 | 5.86 | 1.47 | 2.75 | 0.99 | |
| G4 | SUV10 | 60 | 2.50 | 2.75 | 0.72 | 4.08 | 1.60 | 3.20 | 0.87 |
| SUV60 | 60 | 2.60 | 2.56 | 1.15 | 5.86 | 1.72 | 2.87 | 1.17 |
| Timepoint | TBR | Cut-off | Sensitivity | Specificity | PPV | NPV | AUC (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| 10 min | TBR | 1.60 | 0.93 | 0.37 | 0.87 | 0.56 | 0.809 (0.744; 0.874) | <0.001 |
| TBR max | 1.60 | 0.57 | 0.87 | 0.95 | 0.31 | 0.796 (0.730; 0.862) | <0.001 | |
| TBR plexus | 1.00 | 0.87 | 0.65 | 0.92 | 0.53 | 0.868 (0.820; 0.917) | <0.001 | |
| TBR plexus ROI mean | 1.00 | 0.95 | 0.58 | 0.90 | 0.71 | 0.869 (0.814; 0.923) | <0.001 | |
| TBR thalamus | 1.55 | 0.83 | 0.69 | 0.92 | 0.48 | 0.801 (0.735; 0.868) | <0.001 | |
| TBR thalamus max | 1.40 | 0.74 | 0.69 | 0.91 | 0.38 | 0.742 (0.668; 0.817) | <0.001 | |
| TBR MIDDLE A. | 1.90 | 0.71 | 0.85 | 0.95 | 0.40 | 0.831 (0.774; 0.889) | <0.001 | |
| TBR sinus | 0.74 | 0.77 | 0.81 | 0.95 | 0.44 | 0.843 (0.788; 0.899) | <0.001 | |
| 60 min | TBR | 1.60 | 0.91 | 0.36 | 0.86 | 0.48 | 0.797 (0.738; 0.856) | <0.001 |
| TBR max | 1.60 | 0.57 | 0.75 | 0.91 | 0.29 | 0.7621 (0.698; 0.827) | <0.001 | |
| TBR plexus | 1.20 | 0.94 | 0.40 | 0.87 | 0.60 | 0.845 (0.790; 0.900) | <0.001 | |
| TBR plexus ROI mean | 1.20 | 0.91 | 0.38 | 0.86 | 0.51 | 0.828 (0.773; 0.883) | <0.001 | |
| TBR thalamus | 1.80 | 0.77 | 0.70 | 0.92 | 0.41 | 0.789 (0.725; 0.852) | <0.001 | |
| TBR thalamus max | 1.10 | 0.88 | 0.51 | 0.88 | 0.50 | 0.752 (0.680; 0.823) | <0.001 | |
| TBR MIDDLE A. | 2.10 | 0.64 | 0.79 | 0.93 | 0.34 | 0.788 (0.727; 0.849) | <0.001 | |
| TBR sinus | 1.30 | 0.63 | 0.89 | 0.960 | 0.35 | 0.793 (0.735; 0.850) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harat, M.; Miechowicz, I.; Rakowska, J.; Zarębska, I.; Małkowski, B. A Biopsy-Controlled Prospective Study of Contrast-Enhancing Diffuse Glioma Infiltration Based on FET-PET and FLAIR. Cancers 2024, 16, 1265. https://doi.org/10.3390/cancers16071265
Harat M, Miechowicz I, Rakowska J, Zarębska I, Małkowski B. A Biopsy-Controlled Prospective Study of Contrast-Enhancing Diffuse Glioma Infiltration Based on FET-PET and FLAIR. Cancers. 2024; 16(7):1265. https://doi.org/10.3390/cancers16071265
Chicago/Turabian StyleHarat, Maciej, Izabela Miechowicz, Józefina Rakowska, Izabela Zarębska, and Bogdan Małkowski. 2024. "A Biopsy-Controlled Prospective Study of Contrast-Enhancing Diffuse Glioma Infiltration Based on FET-PET and FLAIR" Cancers 16, no. 7: 1265. https://doi.org/10.3390/cancers16071265
APA StyleHarat, M., Miechowicz, I., Rakowska, J., Zarębska, I., & Małkowski, B. (2024). A Biopsy-Controlled Prospective Study of Contrast-Enhancing Diffuse Glioma Infiltration Based on FET-PET and FLAIR. Cancers, 16(7), 1265. https://doi.org/10.3390/cancers16071265