
Diagnosis of Metastatic Non-Small Cell Lung Cancer during Hospitalization: Missed Opportunity for Optimal Supportive Care?


Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barrett, J.; Sharp, D.J.; Stapley, S.; Stabb, C.; Hamilton, W. Pathways to the diagnosis of ovarian cancer in the UK: A cohort study in primary care. BJOG 2010, 117, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.; Hamilton, W. Pathways to the diagnosis of lung cancer in the UK: A cohort study. BMC Fam. Pract. 2008, 9, 31. [Google Scholar] [CrossRef] [PubMed]
- Elliss-Brookes, L.; McPhail, S.; Ives, A.; Greenslade, M.; Shelton, J.; Hiom, S.; Richards, M. Routes to diagnosis for cancer—Determining the patient journey using multiple routine data sets. Br. J. Cancer 2012, 107, 1220–1226. [Google Scholar] [CrossRef]
- Durbin, S.M.; Zubiri, L.; Niemierko, A.; Bardia, A.; Sullivan, R.J.; McEwen, C.; Mulvey, T.M.; Allen, I.M.; Lawrence, D.P.; Cohen, J.V.; et al. Clinical Outcomes of Patients with Metastatic Cancer Receiving Immune Checkpoint Inhibitors in the Inpatient Setting. Oncologist 2021, 26, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Neves, M.B.M.; Neves, Y.C.S.; Bomonetto, J.V.B.; Matos, P.P.C.; Giglio, A.D.; Cubero, D.I.G. Evaluation of factors predicting the benefit from systemic oncological treatment for severely ill hospitalized patients: A retrospective study. BMC Palliat. Care 2023, 22, 131. [Google Scholar] [CrossRef] [PubMed]
- Fiorin de Vasconcellos, V.; Rcc Bonadio, R.; Avanço, G.; Negrão, M.V.; Pimenta Riechelmann, R. Inpatient palliative chemotherapy is associated with high mortality and aggressive end-of-life care in patients with advanced solid tumors and poor performance status. BMC Palliat. Care 2019, 18, 42. [Google Scholar] [CrossRef] [PubMed]
- Firat, S.; Byhardt, R.W.; Gore, E. Comorbidity and Karnofksy performance score are independent prognostic factors in stage III non-small-cell lung cancer: An institutional analysis of patients treated on four RTOG studies. Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 357–364. [Google Scholar] [CrossRef]
- Boeck, S.; Hinke, A.; Wilkowski, R.; Heinemann, V. Importance of performance status for treatment outcome in advanced pancreatic cancer. World J. Gastroenterol. 2007, 13, 224–227. [Google Scholar] [CrossRef]
- Evers, P.D.; Logan, J.E.; Sills, V.; Chin, A.I. Karnofsky performance status predicts overall survival, cancer-specific survival, and progression-free survival following radical cystectomy for urothelial carcinoma. World J. Urol. 2014, 32, 385–391. [Google Scholar] [CrossRef]
- Hwang, S.S.; Scott, C.B.; Chang, V.T.; Cogswell, J.; Srinivas, S.; Kasimis, B. Prediction of survival for advanced cancer patients by recursive partitioning analysis: Role of Karnofsky performance status, quality of life, and symptom distress. Cancer Investig. 2004, 22, 678–687. [Google Scholar] [CrossRef]
- Yates, J.W.; Chalmer, B.; McKegney, F.P. Evaluation of patients with advanced cancer using the Karnofsky performance status. Cancer 1980, 45, 2220–2224. [Google Scholar] [CrossRef]
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non-Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef]
- Igawa, S.; Fukui, T.; Kasajima, M.; Ono, T.; Ozawa, T.; Kakegawa, M.; Kusuhara, S.; Sato, T.; Nakahara, Y.; Hisashi, M.; et al. First-line osimertinib for poor performance status patients with EGFR mutation-positive non-small cell lung cancer: A prospective observational study. Investig. New Drugs 2022, 40, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Stock-Martineau, S.; Magner, K.; Jao, K.; Wheatley-Price, P. Challenges of Immunotherapy in Stage IV Non-Small-Cell Lung Cancer. JCO Oncol. Pract. 2021, 17, 465–471. [Google Scholar] [CrossRef]
- Gao, G.; Zhou, C.; Huang, Y.; Hong, Z.; Yu, P.; Chen, Y.; Gao, J.; Zhang, K.; Xie, Z.; Zhang, J.; et al. Randomized phase III study comparing the first-line chemotherapy regimens in patients with driver mutation-negative advanced non-small cell lung cancer and poor performance status complicated with chronic obstructive pulmonary disease. Transl. Lung Cancer Res. 2021, 10, 2573–2587. [Google Scholar] [CrossRef] [PubMed]
- Alessi, J.V.; Ricciuti, B.; Jiménez-Aguilar, E.; Hong, F.; Wei, Z.; Nishino, M.; Plodkowski, A.J.; Sawan, P.; Luo, J.; Rizvi, H.; et al. Outcomes to first-line pembrolizumab in patients with PD-L1-high (≥50%) non-small cell lung cancer and a poor performance status. J. Immunother. Cancer 2020, 8, e001007. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Ruiz-Patiño, A.; Arrieta, O.; Cardona, A.F.; Martín, C.; Raez, L.E.; Zatarain-Barrón, Z.L.; Barrón, F.; Ricaurte, L.; Bravo-Garzón, M.A.; Mas, L.; et al. Immunotherapy at any line of treatment improves survival in patients with advanced metastatic non-small cell lung cancer (NSCLC) compared with chemotherapy (Quijote-CLICaP). Thorac. Cancer 2020, 11, 353–361. [Google Scholar] [CrossRef]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52 Pt 1, 103–109. [Google Scholar] [CrossRef]
- Gotfrit, J.; Zhang, T.; Zanon-Heacock, S.; Wheatley-Price, P. Patients With Advanced Non-Small Cell Lung Cancer Requiring Inpatient Medical Oncology Consultation: Characteristics, Referral Patterns, and Outcomes. Clin. Lung Cancer 2016, 17, 292–300. [Google Scholar] [CrossRef]
- Gotfrit, J.; Jonker, C.; Zhang, T.; Goss, G.; Nicholas, G.; Laurie, S.; Wheatley-Price, P. Inpatients versus outpatients with advanced non-small cell lung cancer: Characteristics and outcomes. Cancer Treat. Res. Commun. 2019, 19, 100130. [Google Scholar] [CrossRef]
- Barth, C.; Soares, M.; Toffart, A.C.; Timsit, J.F.; Burghi, G.; Irrazabal, C.; Pattison, N.; Tobar, E.; Almeida, B.F.; Silva, U.V.; et al. Characteristics and outcome of patients with newly diagnosed advanced or metastatic lung cancer admitted to intensive care units (ICUs). Ann. Intensive Care 2018, 8, 80. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef] [PubMed]
- Kerr, K.M.; Bibeau, F.; Thunnissen, E.; Botling, J.; Ryška, A.; Wolf, J.; Öhrling, K.; Burdon, P.; Malapelle, U.; Büttner, R. The evolving landscape of biomarker testing for non-small cell lung cancer in Europe. Lung Cancer 2021, 154, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Holguin, R.A.P.; Schaefer, E.; Zhou, S.; Belani, C.P.; Ma, P.C.; Reed, M.F. Utilization and costs of epidermal growth factor receptor mutation testing and targeted therapy in Medicare patients with metastatic lung adenocarcinoma. BMC Health Serv. Res. 2022, 22, 470. [Google Scholar] [CrossRef]
- D’Ardia, A.; Caputo, A.; Fumo, R.; Ciaparrone, C.; Gaeta, S.; Picariello, C.; Zeppa, P.; D’Antonio, A. Advanced non-small cell lung cancer: Rapid evaluation of EGFR status on fine-needle cytology samples using Idylla. Pathol. Res. Pract. 2021, 224, 153547. [Google Scholar] [CrossRef] [PubMed]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Yu, H.; Yang, L.; Yang, H.; Cao, H.; Lei, L.; Ma, L.; Liu, S.; Tian, L.; Wang, S. Combined early palliative care for non-small-cell lung cancer patients: A randomized controlled trial in Chongqing, China. Front. Oncol. 2023, 13, 1184961. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2023. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2023-cancer-facts-figures.html (accessed on 14 March 2024).


{kind=link}
{kind=link}
| Characteristic | Findings |
|---|---|
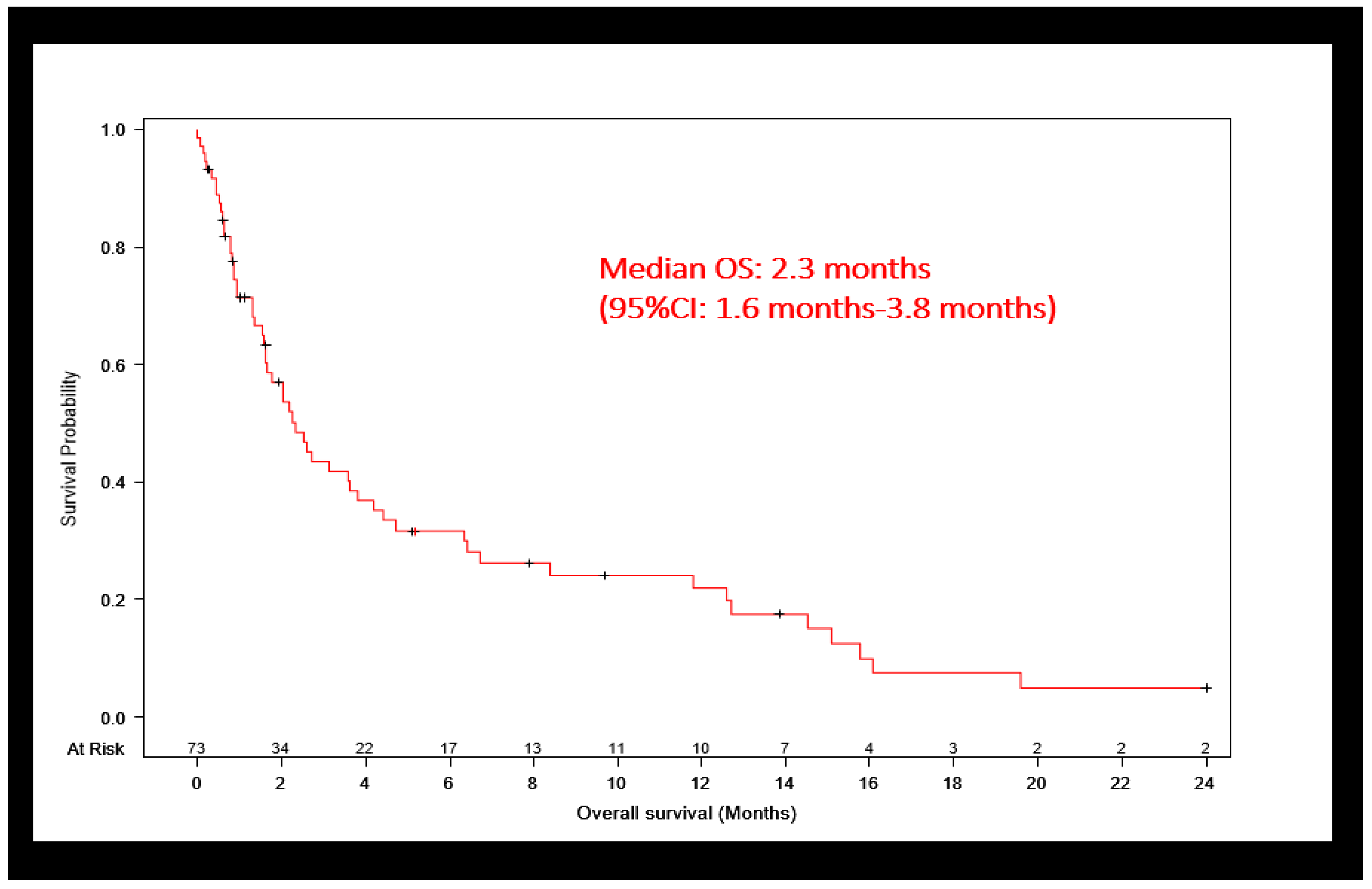
| Number of patients | 73 |
| Median age (min, max) | 64 years (32, 85) |
| Median BMI (min, max) | 25.2 kg/m2 (12.2, 46.8) |
| Gender, n (%) | |
| Male | 40 (54.8%) |
| Female | 33 (45.2%) |
| Race, n (%) | |
| Caucasian | 61 (83.6) |
| African American | 7 (9.6%) |
| Other | 5 (6.8%) |
| Smoking status, n (%) | |
| Current | 32 (43.8%) |
| Former | 32 (43.8%) |
| Never | 9 (12.3%) |
| Histology, n (%) | |
| Adenocarcinoma | 33 (49.3%) |
| Squamous cell | 14 (20.9%) |
| Other | 26 (35.6%) |
| Chief complaint, n (%) | |
| Shortness of breath | 27 (37.0%) |
| Pain | 14 (19.2%) |
| Weakness | 12 (16.4%) |
| Other | 20 (27.3%) |
| Brain metastases, n (%) | |
| Yes | 24 (32.8%) |
| No | 39 (53.4%) |
| Not examined | 10 (13.6%) |
| NGS performed, n (%) | |
| Yes | 60 (82.1%) |
| No | 13 (17.8%) |
| Oncology consult, n (%) | |
| Inpatient | 23 (31.5%) |
| Outpatient | 35 (47.9%) |
| None | 15 (20.5%) |
| Disposition, n (%) | |
| Home | 45 (61.6) |
| Facility | 16 (21.9%) |
| Hospice | 5 (6.8%) |
| Deceased | 4 (5.4%) |
| Against medical advice | 3 (4.1%) |
| Readmitted in next 30 days, n (%) | |
| Yes | 24 (32.8%) |
| Reason for readmission, n (%) | |
| Shortness of breath | 11 (45.8%) |
| Fall | 2 (8.3%) |
| Other | 11 (45.8%) |
| No | 49 (67.1%) |
| Hospice enrollment | |
| At any time | 23 (31.5%) |
| During initial admission | 5 |
| No | 50 (68.5%) |
| Parameter | Parameter Estimate (Standard Error) | Hazard Ratio (95% Confidence Interval) | p-Value |
|---|---|---|---|
| Treatment: No treatment vs. Treatment | 2.629 (0.507) | 13.854 (5.131, 37.405) | <0.0001 |
| Age: 1 year increment | 0.004 (0.022) | 1.004 (0.961, 1.049) | 0.085 |
| Gender: Male vs. Female | 0.213 (0.352) | 1.238 (0.621, 2.466) | 0.545 |
| Histology: Adenocarcinoma vs. Other | −0.322 (0.383) | 0.725 (0.342, 1.535) | 0.401 |
| Histology: Squamous cell vs. Other | 0.046 (0.449) | 1.048 (0.434, 2.526) | 0.918 |
| Smoking: Quit vs. No | −0.042 (0.589) | 0.958 (0.302, 3.038) | 0.943 |
| Smoking: Yes vs. no | 0.038 (0.595) | 1.038 (0.324, 3.331) | 0.949 |
| Brain metastasis: Unknown vs. No | −0.611 (0.660) | 0.543 (0.149, 1.980) | 0.355 |
| Brain metastasis: Yes vs. No | −0.912 (0.375) | 0.402 (0.192, 0.839) | 0.015 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Upadhyay Banskota, S.; Trinh, J.Q.; Lyden, E.; Houlihan, C.; Asif, S.; Abughanimeh, O.; Teply, B.A. Diagnosis of Metastatic Non-Small Cell Lung Cancer during Hospitalization: Missed Opportunity for Optimal Supportive Care? Cancers 2024, 16, 1221. https://doi.org/10.3390/cancers16061221
Upadhyay Banskota S, Trinh JQ, Lyden E, Houlihan C, Asif S, Abughanimeh O, Teply BA. Diagnosis of Metastatic Non-Small Cell Lung Cancer during Hospitalization: Missed Opportunity for Optimal Supportive Care? Cancers. 2024; 16(6):1221. https://doi.org/10.3390/cancers16061221
Chicago/Turabian StyleUpadhyay Banskota, Shristi, Jonathan Q. Trinh, Elizabeth Lyden, Conor Houlihan, Samia Asif, Omar Abughanimeh, and Benjamin A. Teply. 2024. "Diagnosis of Metastatic Non-Small Cell Lung Cancer during Hospitalization: Missed Opportunity for Optimal Supportive Care?" Cancers 16, no. 6: 1221. https://doi.org/10.3390/cancers16061221
APA StyleUpadhyay Banskota, S., Trinh, J. Q., Lyden, E., Houlihan, C., Asif, S., Abughanimeh, O., & Teply, B. A. (2024). Diagnosis of Metastatic Non-Small Cell Lung Cancer during Hospitalization: Missed Opportunity for Optimal Supportive Care? Cancers, 16(6), 1221. https://doi.org/10.3390/cancers16061221