
CXCL13 Positive Cells Localization Predict Response to Anti-PD-1/PD-L1 in Pulmonary Non-Small Cell Carcinoma

 ,
,  , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient’s Clinical Data and Tissue Selection
2.2. Immunohistochemistry
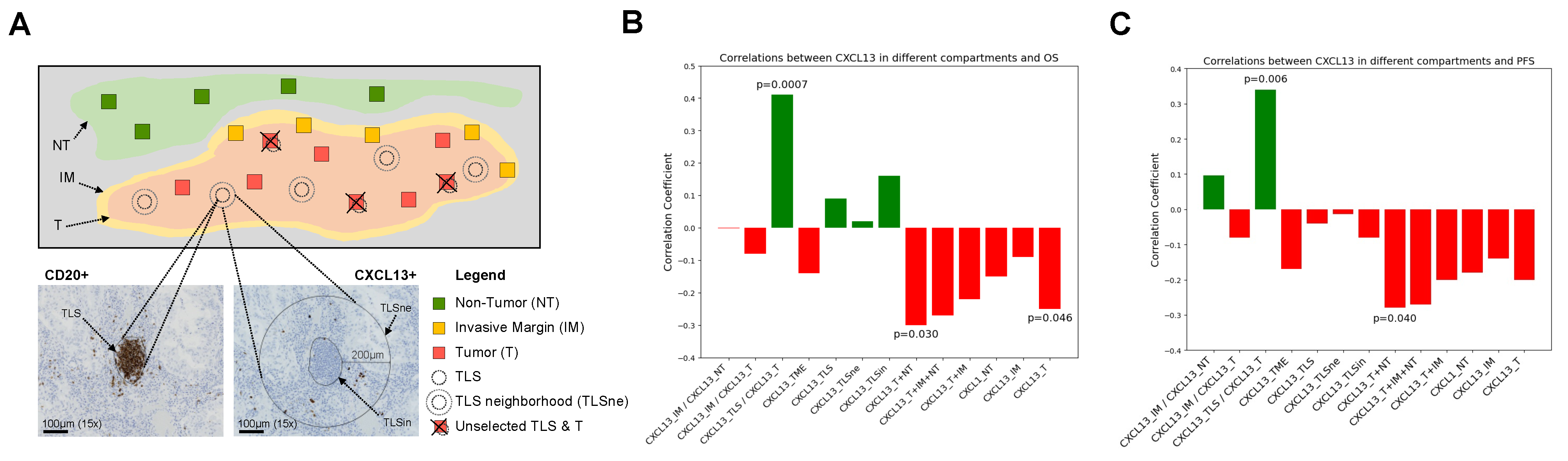
2.3. Slide Digitalization and CXCL13 Scoring in Different Tumor Microenvironments
2.4. Survival Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Features of Treated NSCLC Patients
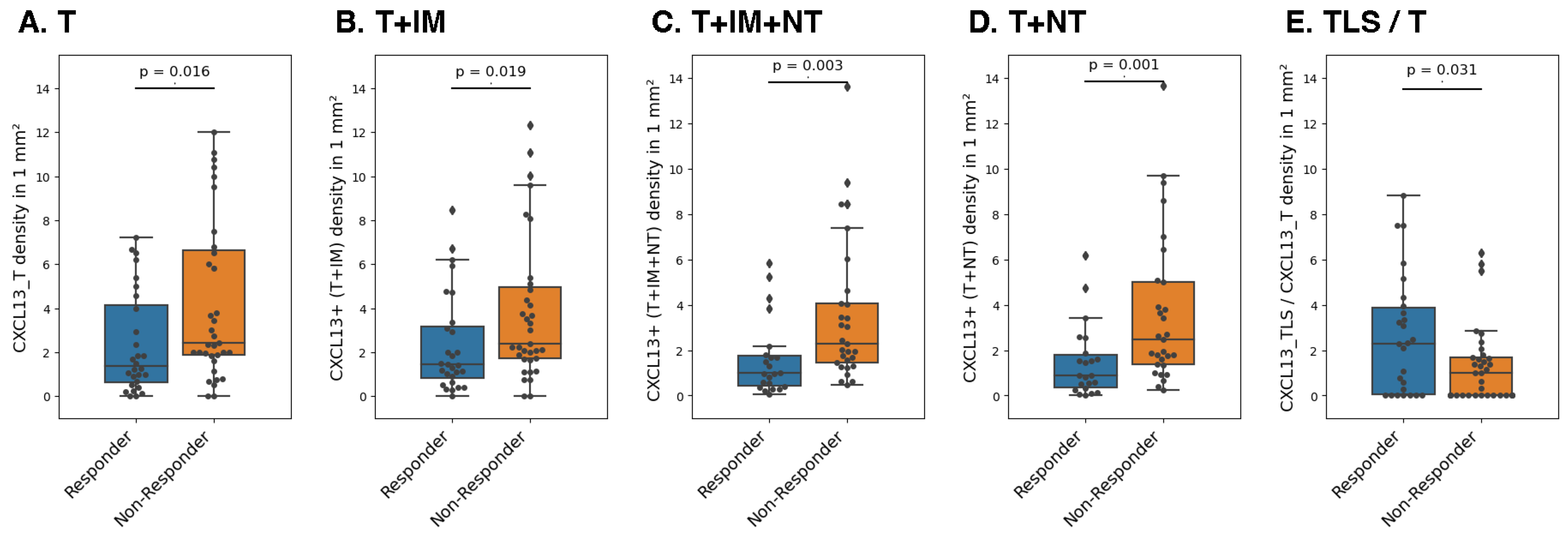
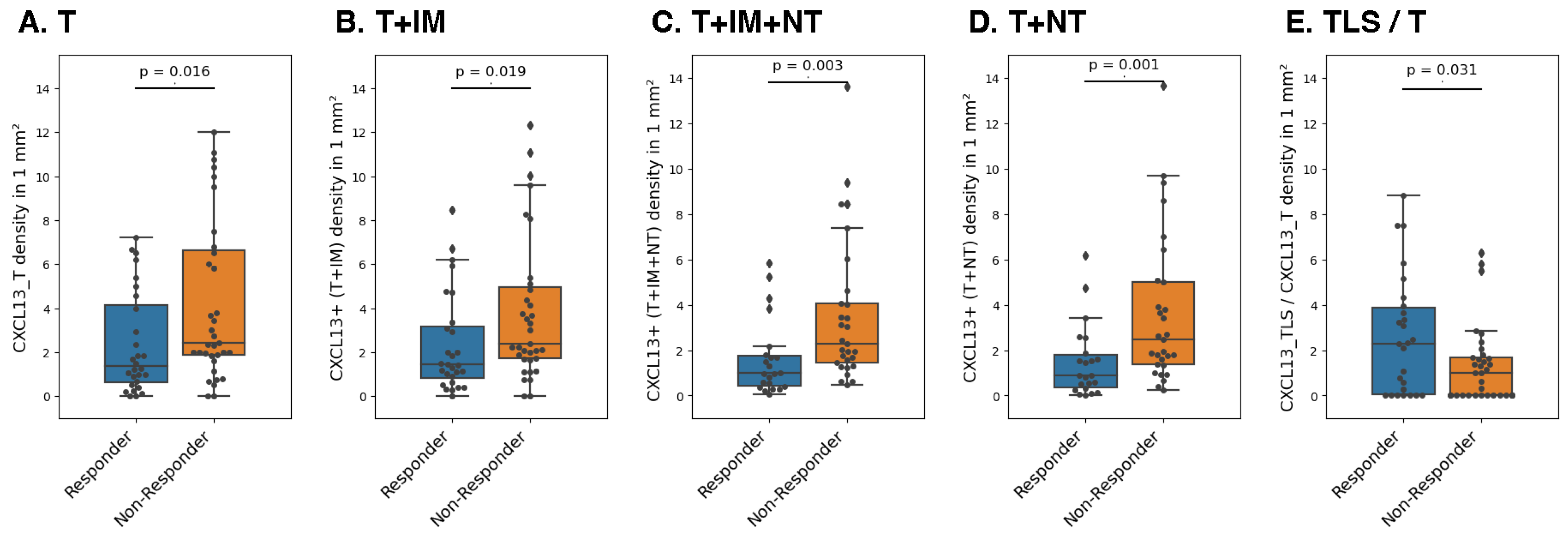
3.2. Association between CXCL13+ Cell Density and Response to ICI
3.3. CXCL13 Is a Factor Predictive of Survival and Progression-Free Survival
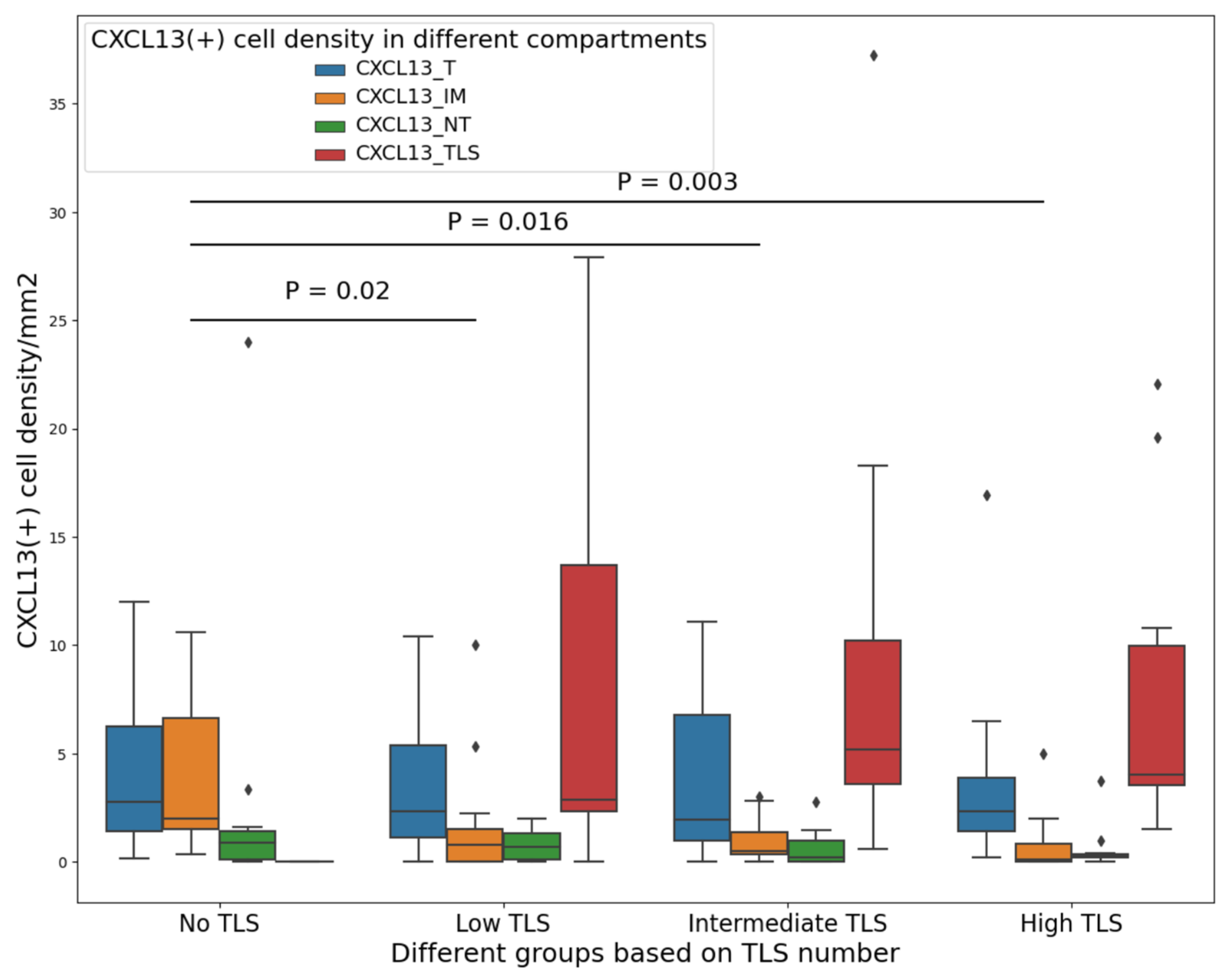
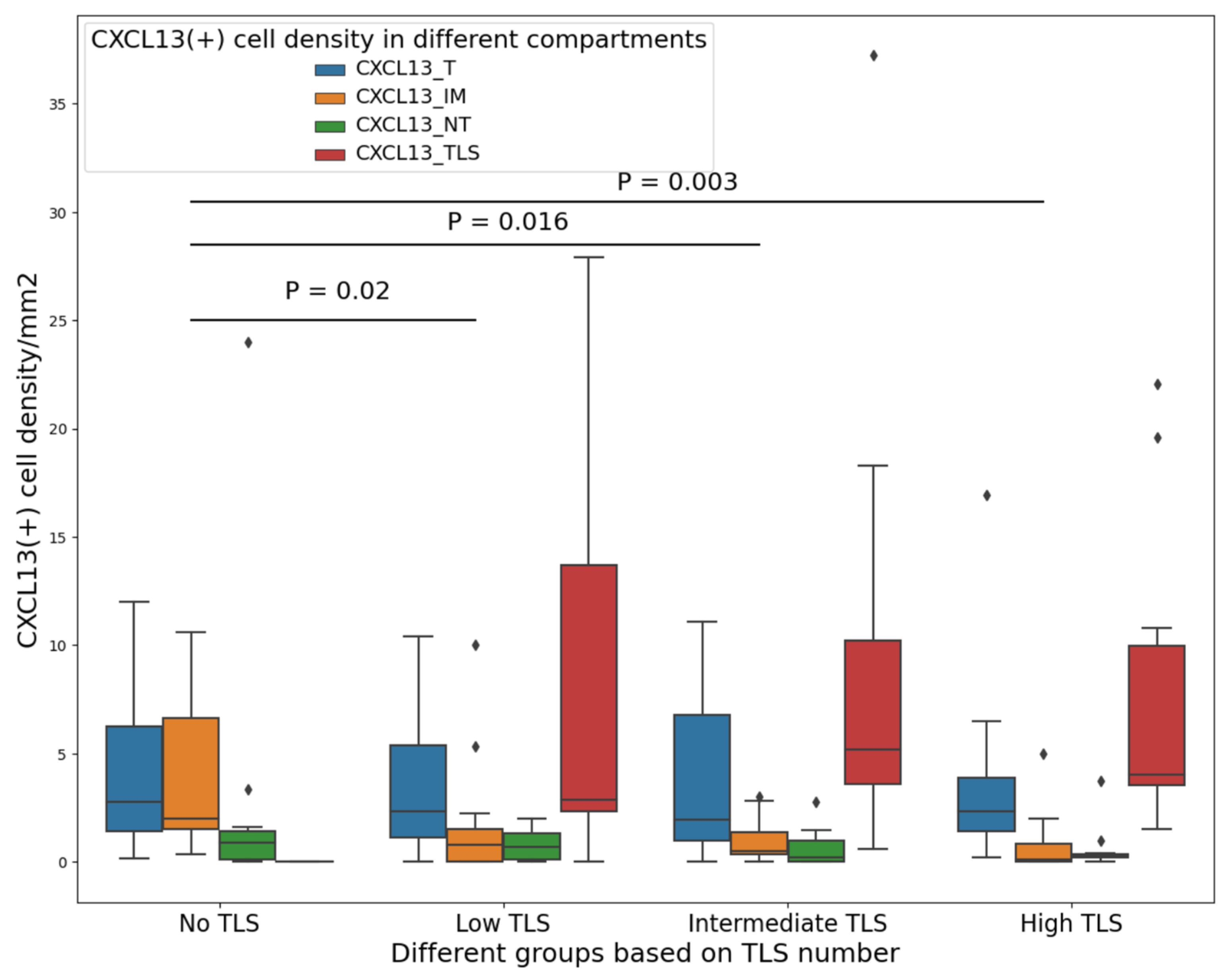
3.4. CXCL13+ Cells in the Tumor Have a Link with Chemotaxis toward TLS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, R.; Manochakian, R.; James, L.; Azzouqa, A.-G.; Shi, H.; Zhang, Y.; Zhao, Y.; Zhou, K.; Lou, Y. Emerging therapeutic agents for advanced non-small cell lung cancer. J. Hematol. Oncol. 2020, 13, 58. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Behrouzieh, S.; Sheida, F.; Rezaei, N. Review of the recent clinical trials for PD-1/PD-L1 based lung cancer immunotherapy. Expert Rev. Anticancer Ther. 2021, 21, 1355–1370. [Google Scholar] [CrossRef]
- Pasello, G.; Pavan, A.; Attili, I.; Bortolami, A.; Bonanno, L.; Menis, J.; Conte, P.; Guarneri, V. Real world data in the era of Immune Checkpoint Inhibitors (ICIs): Increasing evidence and future applications in lung cancer. Cancer Treat. Rev. 2020, 87, 102031. [Google Scholar] [CrossRef]
- Mariathasan, S.; Turley, S.J.; Nickles, D.; Castiglioni, A.; Yuen, K.; Wang, Y.; Kadel, E.E., III; Koeppen, H.; Astarita, J.L.; Cubas, R. TGFβ attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature 2018, 554, 544–548. [Google Scholar] [CrossRef]
- Yang, Q.; Xu, Z.; Zheng, L.; Zhang, L.; You, Q.; Sun, J. Multimodal detection of PD-L1: Reasonable biomarkers for immune checkpoint inhibitor. Am. J. Cancer Res. 2018, 8, 1689. [Google Scholar]
- Yi, M.; Jiao, D.; Xu, H.; Liu, Q.; Zhao, W.; Han, X.; Wu, K. Biomarkers for predicting efficacy of PD-1/PD-L1 inhibitors. Mol. Cancer 2018, 17, 129. [Google Scholar] [CrossRef]
- Solomon, B.; Young, R.J.; Bressel, M.; Urban, D.; Hendry, S.; Thai, A.; Angel, C.; Haddad, A.; Kowanetz, M.; Fua, T. Prognostic significance of PD-L1+ and CD8+ immune cells in HPV+ oropharyngeal squamous cell carcinoma. Cancer Immunol. Res. 2018, 6, 295–304. [Google Scholar] [CrossRef]
- Cabrita, R.; Lauss, M.; Sanna, A.; Donia, M.; Larsen, M.S.; Mitra, S.; Johansson, I.; Phung, B.; Harbst, K.; Vallon-Christersson, J. Tertiary lymphoid structures improve immunotherapy and survival in melanoma. Nature 2020, 577, 561–565. [Google Scholar] [CrossRef]
- Petitprez, F.; de Reyniès, A.; Keung, E.Z.; Chen, T.W.-W.; Sun, C.-M.; Calderaro, J.; Jeng, Y.-M.; Hsiao, L.-P.; Lacroix, L.; Bougoüin, A. B cells are associated with survival and immunotherapy response in sarcoma. Nature 2020, 577, 556–560. [Google Scholar] [CrossRef]
- Helmink, B.A.; Reddy, S.M.; Gao, J.; Zhang, S.; Basar, R.; Thakur, R.; Yizhak, K.; Sade-Feldman, M.; Blando, J.; Han, G. B cells and tertiary lymphoid structures promote immunotherapy response. Nature 2020, 577, 549–555. [Google Scholar] [CrossRef]
- Bruno, T.C. New Predictors for Immunotherapy Responses Sharpen Our View of the Tumour Microenvironment; Nature Publishing Group: London, UK, 2020; Volume 577, pp. 474–476. [Google Scholar]
- Cyster, J.G. Chemokines, sphingosine-1-phosphate, and cell migration in secondary lymphoid organs. Annu. Rev. Immunol. 2005, 23, 127–159. [Google Scholar] [CrossRef]
- Ansel, K.M.; McHeyzer-Williams, L.J.; Ngo, V.N.; McHeyzer-Williams, M.G.; Cyster, J.G. In vivo–activated CD4 T cells upregulate CXC chemokine receptor 5 and reprogram their response to lymphoid chemokines. J. Exp. Med. 1999, 190, 1123–1134. [Google Scholar] [CrossRef]
- Legler, D.F.; Loetscher, M.; Roos, R.S.; Clark-Lewis, I.; Baggiolini, M.; Moser, B. B cell–attracting chemokine 1, a human CXC chemokine expressed in lymphoid tissues, selectively attracts B lymphocytes via BLR1/CXCR5. J. Exp. Med. 1998, 187, 655–660. [Google Scholar] [CrossRef]
- Sautès-Fridman, C.; Petitprez, F.; Calderaro, J.; Fridman, W.H. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat. Rev. Cancer 2019, 19, 307–325. [Google Scholar] [CrossRef]
- Ansel, K.M.; Ngo, V.N.; Hyman, P.L.; Luther, S.A.; Förster, R.; Sedgwick, J.D.; Browning, J.L.; Lipp, M.; Cyster, J.G. A chemokine-driven positive feedback loop organizes lymphoid follicles. Nature 2000, 406, 309–314. [Google Scholar] [CrossRef]
- Gunn, M.D.; Ngo, V.N.; Ansel, K.M.; Ekland, E.H.; Cyster, J.G.; Williams, L.T. A B-cell-homing chemokine made in lymphoid follicles activates Burkitt’s lymphoma receptor-1. Nature 1998, 391, 799–803. [Google Scholar] [CrossRef]
- Cosgrove, J.; Novkovic, M.; Albrecht, S.; Pikor, N.B.; Zhou, Z.; Onder, L.; Mörbe, U.; Cupovic, J.; Miller, H.; Alden, K. B cell zone reticular cell microenvironments shape CXCL13 gradient formation. Nat. Commun. 2020, 11, 3677. [Google Scholar] [CrossRef]
- Fridman, W.H.; Zitvogel, L.; Sautès, C.; Kroemer, G. The immune contexture in cancer prognosis and treatment. Nat. Rev. Clin. Oncol. 2017, 14, 717–734. [Google Scholar] [CrossRef]
- Groeneveld, C.S.; Fontugne, J.; Cabel, L.; Bernard-Pierrot, I.; Radvanyi, F.; Allory, Y.; de Reyniès, A. Tertiary lymphoid structures marker CXCL13 is associated with better survival for patients with advanced-stage bladder cancer treated with immunotherapy. Eur. J. Cancer 2021, 148, 181–189. [Google Scholar] [CrossRef]
- Yang, M.; Lu, J.; Zhang, G.; Wang, Y.; He, M.; Xu, Q.; Xu, C.; Liu, H. CXCL13 shapes immunoactive tumor microenvironment and enhances the efficacy of PD-1 checkpoint blockade in high-grade serous ovarian cancer. J. ImmunoTher. Cancer 2021, 9, e001136. [Google Scholar] [CrossRef] [PubMed]
- Sorin, M.; Karimi, E.; Rezanejad, M.; Miranda, W.Y.; Desharnais, L.; McDowell, S.A.; Doré, S.; Arabzadeh, A.; Breton, V.; Fiset, B. Single-cell spatial landscape of immunotherapy response reveals mechanisms of CXCL13 enhanced antitumor immunity. J. Immunother. Cancer 2023, 11, e005545. [Google Scholar] [CrossRef] [PubMed]
- Dai, S.; Zeng, H.; Liu, Z.; Jin, K.; Jiang, W.; Wang, Z.; Lin, Z.; Xiong, Y.; Wang, J.; Chang, Y. Intratumoral CXCL13+ CD8+ T cell infiltration determines poor clinical outcomes and immunoevasive contexture in patients with clear cell renal cell carcinoma. J. Immunother. Cancer 2021, 9, e001823. [Google Scholar] [CrossRef] [PubMed]
- Jin, K.; Cao, Y.; Gu, Y.; Fang, H.; Fei, Y.; Wang, J.; Liu, X.; Lv, K.; He, X.; Lin, C. Poor clinical outcomes and immunoevasive contexture in CXCL13+ CD8+ T cells enriched gastric cancer patients. Oncoimmunology 2021, 10, 1915560. [Google Scholar] [CrossRef] [PubMed]
- Fend, L.; Remy-Ziller, C.; Foloppe, J.; Kempf, J.; Cochin, S.; Barraud, L.; Accart, N.; Erbs, P.; Fournel, S.; Préville, X. Oncolytic virotherapy with an armed vaccinia virus in an orthotopic model of renal carcinoma is associated with modification of the tumor microenvironment. Oncoimmunology 2016, 5, e1080414. [Google Scholar] [CrossRef] [PubMed]
- Shiroyama, T.; Nagatomo, I.; Koyama, S.; Hirata, H.; Nishida, S.; Miyake, K.; Fukushima, K.; Shirai, Y.; Mitsui, Y.; Takata, S. Impact of sarcopenia in patients with advanced non–small cell lung cancer treated with PD-1 inhibitors: A preliminary retrospective study. Sci. Rep. 2019, 9, 2447. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Emmett, L.; Lo, S.; Liu, V.; Kapoor, R.; Carlino, M.; Guminski, A.; Long, G.; Menzies, A. FDG-PET response and outcome from anti-PD-1 therapy in metastatic melanoma. Ann. Oncol. 2018, 29, 2115–2120. [Google Scholar] [CrossRef] [PubMed]
- Mody, R.; Alice, L.Y.; Naranjo, A.; Zhang, F.F.; London, W.B.; Shulkin, B.L.; Parisi, M.T.; Diccianni, M.B.; Hank, J.A.; Felder, M. Irinotecan, temozolomide, and dinutuximab with GM-CSF in children with refractory or relapsed neuroblastoma: A report from the Children’s Oncology Group. J. Clin. Oncol. 2020, 38, 2160. [Google Scholar] [CrossRef]
- Lim, S.Y.; Rizos, H. Immune cell profiling in the age of immune checkpoint inhibitors: Implications for biomarker discovery and understanding of resistance mechanisms. Mamm. Genome 2018, 29, 866–878. [Google Scholar] [CrossRef]
- Khan, M.; Du, K.; Ai, M.; Wang, B.; Lin, J.; Ren, A.; Chen, C.; Huang, Z.; Qiu, W.; Yuan, Y. PD-L1 expression as biomarker of efficacy of PD-1/PD-L1 checkpoint inhibitors in metastatic triple negative breast cancer: A systematic review and meta-analysis. Front. Immunol. 2023, 14, 1060308. [Google Scholar] [CrossRef]
- Berghmans, T.; Durieux, V.; Hendriks, L.E.; Dingemans, A.-M. Immunotherapy: From advanced NSCLC to early stages, an evolving concept. Front. Med. 2020, 7, 90. [Google Scholar] [CrossRef]
- Necchi, A.; Raggi, D.; Gallina, A.; Ross, J.S.; Farè, E.; Giannatempo, P.; Marandino, L.; Colecchia, M.; Luciano, R.; Bianchi, M. Impact of molecular subtyping and immune infiltration on pathological response and outcome following neoadjuvant pembrolizumab in muscle-invasive bladder cancer. Eur. Urol. 2020, 77, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Cha, H.; Kim, H.S.; Lee, B.; Kim, S.; Kim, T.M.; Jung, H.A.; Sun, J.M.; Ahn, J.S.; Ahn, M.J. Transcriptional upregulation of CXCL13 is correlated with a favorable response to immune checkpoint inhibitors in lung adenocarcinoma. Cancer Med. 2023, 12, 7639–7650. [Google Scholar] [CrossRef]
- Malhotra, J.; Jabbour, S.K.; Aisner, J. Current state of immunotherapy for non-small cell lung cancer. Transl. Lung Cancer Res. 2017, 6, 196. [Google Scholar] [CrossRef]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T. Ado-trastuzumab emtansine for patients with HER2-mutant lung cancers: Results from a phase II basket trial. J. Clin. Oncol. 2018, 36, 2532. [Google Scholar] [CrossRef] [PubMed]
- Gettinger, S.; Rizvi, N.A.; Chow, L.Q.; Borghaei, H.; Brahmer, J.; Ready, N.; Gerber, D.E.; Shepherd, F.A.; Antonia, S.; Goldman, J.W. Nivolumab monotherapy for first-line treatment of advanced non–small-cell lung cancer. J. Clin. Oncol. 2016, 34, 2980. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Brahmer, J.R.; Juergens, R.A.; Borghaei, H.; Gettinger, S.; Chow, L.Q.; Gerber, D.E.; Laurie, S.A.; Goldman, J.W. Nivolumab in combination with platinum-based doublet chemotherapy for first-line treatment of advanced non–small-cell lung cancer. J. Clin. Oncol. 2016, 34, 2969. [Google Scholar] [CrossRef] [PubMed]
- Panse, J.; Friedrichs, K.; Marx, A.; Hildebrandt, Y.; Luetkens, T.; Bartels, K.; Horn, C.; Stahl, T.; Cao, Y.; Milde-Langosch, K. Chemokine CXCL13 is overexpressed in the tumour tissue and in the peripheral blood of breast cancer patients. Br. J. Cancer 2008, 99, 930–938. [Google Scholar] [CrossRef]
- Bindea, G.; Mlecnik, B.; Tosolini, M.; Kirilovsky, A.; Waldner, M.; Obenauf, A.C.; Angell, H.; Fredriksen, T.; Lafontaine, L.; Berger, A. Spatiotemporal dynamics of intratumoral immune cells reveal the immune landscape in human cancer. Immunity 2013, 39, 782–795. [Google Scholar] [CrossRef]
- Luther, S.A.; Ansel, K.M.; Cyster, J.G. Overlapping roles of CXCL13, interleukin 7 receptor α, and CCR7 ligands in lymph node development. J. Exp. Med. 2003, 197, 1191–1198. [Google Scholar] [CrossRef]
- Luther, S.A.; Lopez, T.; Bai, W.; Hanahan, D.; Cyster, J.G. BLC expression in pancreatic islets causes B cell recruitment and lymphotoxin-dependent lymphoid neogenesis. Immunity 2000, 12, 471–481. [Google Scholar] [CrossRef]
- Van de Pavert, S.A.; Mebius, R.E. New insights into the development of lymphoid tissues. Nat. Rev. Immunol. 2010, 10, 664–674. [Google Scholar] [CrossRef]
- Goc, J.; Germain, C.; Vo-Bourgais, T.K.D.; Lupo, A.; Klein, C.; Knockaert, S.; de Chaisemartin, L.; Ouakrim, H.; Becht, E.; Alifano, M. Dendritic Cells in Tumor-Associated Tertiary Lymphoid Structures Signal a Th1 Cytotoxic Immune Contexture and License the Positive Prognostic Value of Infiltrating CD8+ T CellsMature DC Coordinate Intratumoral Immune Reaction. Cancer Res. 2014, 74, 705–715. [Google Scholar] [CrossRef]
- Lauss, M.; Donia, M.; Svane, I.M.; Jonsson, G. B Cells and Tertiary Lymphoid Structures: Friends or Foes in Cancer Immunotherapy? Clin. Cancer Res. 2022, 28, 1751–1758. [Google Scholar] [CrossRef]
- Griss, J.; Bauer, W.; Wagner, C.; Simon, M.; Chen, M.; Grabmeier-Pfistershammer, K.; Maurer-Granofszky, M.; Roka, F.; Penz, T.; Bock, C. B cells sustain inflammation and predict response to immune checkpoint blockade in human melanoma. Nat. Commun. 2019, 10, 4186. [Google Scholar] [CrossRef]
- Heinig, K.; Gätjen, M.; Grau, M.; Stache, V.; Anagnostopoulos, I.; Gerlach, K.; Niesner, R.A.; Cseresnyes, Z.; Hauser, A.E.; Lenz, P. Access to Follicular Dendritic Cells Is a Pivotal Step in Murine Chronic Lymphocytic Leukemia B-cell Activation and ProliferationCXCR5 and Lymphotoxin-Dependent Leukemia Growth. Cancer Discov. 2014, 4, 1448–1465. [Google Scholar] [CrossRef] [PubMed]
- Ticchioni, M.; Essafi, M.; Jeandel, P.; Davi, F.; Cassuto, J.; Deckert, M.; Bernard, A. Homeostatic chemokines increase survival of B-chronic lymphocytic leukemia cells through inactivation of transcription factor FOXO3a. Oncogene 2007, 26, 7081–7091. [Google Scholar] [CrossRef] [PubMed]
- Chunsong, H.; Yuling, H.; Li, W.; Jie, X.; Gang, Z.; Qiuping, Z.; Qingping, G.; Kejian, Z.; Li, Q.; Chang, A.E. CXC chemokine ligand 13 and CC chemokine ligand 19 cooperatively render resistance to apoptosis in B cell lineage acute and chronic lymphocytic leukemia CD23+ CD5+ B cells. J. Immunol. 2006, 177, 6713–6722. [Google Scholar] [CrossRef] [PubMed]
- Vickers, N.J. Animal communication: When i’m calling you, will you answer too? Curr. Biol. 2017, 27, R713–R715. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Shen, J.; Zhang, G.; Chen, X.; Wu, J.; Chen, W. CD40 controls CXCR5-induced recruitment of myeloid-derived suppressor cells to gastric cancer. Oncotarget 2015, 6, 38901. [Google Scholar] [CrossRef] [PubMed]
- LL CD23. CCL19 and CXCL13 Synergistically Regulate. J. Immunol. 2007, 179, 2880–2888.
- Chen, X.; Takemoto, Y.; Deng, H.; Middelhoff, M.; Friedman, R.A.; Chu, T.H.; Churchill, M.J.; Ma, Y.; Nagar, K.K.; Tailor, Y.H. Histidine decarboxylase (HDC)-expressing granulocytic myeloid cells induce and recruit Foxp3+ regulatory T cells in murine colon cancer. Oncoimmunology 2017, 6, e1290034. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | Number of Patients (%) |
|---|---|
| Sex Male Female | 31 (48%) 34 (52%) |
| Smoking habit Former Current Never | 49 (75%) 14 (22%) 2 (3%) |
| Histology groups Adenocarcinoma Squamous | 54 (83%) 11 (17%) |
| Ecog-status 0 1 2 3 | 18 (28%) 41 (63%) 4 (6%) 2 (3%) |
| Type of immunotherapy Nivolumab Pembrolizumab Pembrolizumab + chemotherapy Nivolumab + Pembrolizumab | 31 (48%) 27 (42%) 6 (9%) 1 (1%) |
| Stage at the start of immunotherapy II III IV | 2 (3%) 6 (9%) 57 (88%) |
| PFS >1 year <1 year | 28 (43%) 37 (57%) |
| Variables | Number of Patients | HR | CI 95% Lower | CI 95% Upper | p |
|---|---|---|---|---|---|
| CXCL13-NT | 52 | 1.13 | 1.02 | 1.26 | 0.02 |
| CXCL13-T+IM+NT | 52 | 1.22 | 1.04 | 1.42 | 0.01 |
| CXCL13-T+NT | 52 | 1.23 | 1.07 | 1.42 | <0.005 |
| Overall Model HR | Overall Model p | ||||
| 1.23 | 0.08 | ||||
| Variables | Number of Patients | HR | CI 95% Lower | CI 95% Upper | p |
| CXCL13-NT | 52 | 1.05 | 0.92 | 1.20 | 0.49 |
| CXCL13-T+IM+NT | 52 | 1.18 | 0.98 | 1.41 | 0.09 |
| Variables | Number of Patients | HR | CI 95% Lower | CI 95% Upper | p |
|---|---|---|---|---|---|
| CXCL13-NT | 52 | 1.31 | 1.04 | 1.64 | 0.02 |
| CXCL13-T+IM+NT | 52 | 1.16 | 1.02 | 1.32 | 0.02 |
| CXCL13-T+NT | 52 | 1.15 | 1.02 | 1.30 | 0.02 |
| CXCL13-TLS/CXCL13-T | 63 | 0.84 | 0.73 | 0.98 | 0.03 |
| Overall Model HR | Overall Model p | ||||
| 1.16 | 0.56 | ||||
| Variables | Number of Patients | HR | CI 95% Lower | CI 95% Upper | p |
| CXCL13-NT | 50 | 1.25 | 0.99 | 1.57 | 0.06 |
| CXCL13-T+IM+NT | 50 | 1.05 | 0.89 | 1.23 | 0.56 |
| CXCL13-TLS/CXCL13-T | 50 | 0.89 | 0.75 | 1.05 | 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vahidian, F.; Lamaze, F.C.; Bouffard, C.; Coulombe, F.; Gagné, A.; Blais, F.; Tonneau, M.; Orain, M.; Routy, B.; Manem, V.S.K.; et al. CXCL13 Positive Cells Localization Predict Response to Anti-PD-1/PD-L1 in Pulmonary Non-Small Cell Carcinoma. Cancers 2024, 16, 708. https://doi.org/10.3390/cancers16040708
Vahidian F, Lamaze FC, Bouffard C, Coulombe F, Gagné A, Blais F, Tonneau M, Orain M, Routy B, Manem VSK, et al. CXCL13 Positive Cells Localization Predict Response to Anti-PD-1/PD-L1 in Pulmonary Non-Small Cell Carcinoma. Cancers. 2024; 16(4):708. https://doi.org/10.3390/cancers16040708
Chicago/Turabian StyleVahidian, Fatemeh, Fabien C. Lamaze, Cédrik Bouffard, François Coulombe, Andréanne Gagné, Florence Blais, Marion Tonneau, Michèle Orain, Bertrand Routy, Venkata S. K. Manem, and et al. 2024. "CXCL13 Positive Cells Localization Predict Response to Anti-PD-1/PD-L1 in Pulmonary Non-Small Cell Carcinoma" Cancers 16, no. 4: 708. https://doi.org/10.3390/cancers16040708
APA StyleVahidian, F., Lamaze, F. C., Bouffard, C., Coulombe, F., Gagné, A., Blais, F., Tonneau, M., Orain, M., Routy, B., Manem, V. S. K., & Joubert, P. (2024). CXCL13 Positive Cells Localization Predict Response to Anti-PD-1/PD-L1 in Pulmonary Non-Small Cell Carcinoma. Cancers, 16(4), 708. https://doi.org/10.3390/cancers16040708