1. Introduction
Some studies have reported that the time trend in survival after childhood cancer in Europe was highest in the north and the west and lowest in the east, and that this ranking among the European regions has not changed in recent decades [
1,
2,
3].
Despite the outcome of childhood cancers showing an improvement and the average survival time of patients increasing, the Hungarian mortality rate of all neoplasms and leukaemia is still high in Europe [
4].
In addition, a highly elevated risk of death in the second 5 years of follow-up was reported for late mortality in survivors of childhood cancer in Hungary [
5].
Centralised treatment protocols and national registration for children with leukaemia and solid tumours were introduced by centres of the Hungarian Paediatric Oncology Network (HPON) in 1971 [
5]. Patients are treated in paediatric oncology centres according to uniform guidelines. The individual centres are in Budapest and five other regional centres of the country. However, no studies have been carried out to investigate regional differences.
The seasonality of disease suggests some effect of environmental factors in aetiology (e.g., infections). Environmental effects were reported in the aetiology of childhood acute leukaemia [
6,
7]. However, the cyclical trend in cancer mortality is rarely investigated.
In the years of the COVID-19 pandemic, a reduction in the number of newly diagnosed paediatric tumours, probably reflecting the delayed access to healthcare services for patients with symptoms suspected to be cancer-related, was observed [
8].
The present ęcological study was performed to determine regional differences and both the annual and cyclic trends in the mortality rate of cancer death among children under the age of 15 years in Hungary during the 21-year interval between 1 January 2001 and 31 December 2021, which includes the two years of the COVID-19 pandemic period.
2. Materials and Methods
2.1. Study Population
The analysis considered a 21-year period from 2001 to 2021. Data on the cause of death were classified according to the 10th revision of the International Classification of Diseases (ICD-10) codes. Annual data on the number of deaths at age 0–14 years due to all neoplasms (ICD-10: C00–D48) were extracted from the nationwide population register maintained by the Hungarian Central Statistical Office (HCSO) [
9]. The HCSO provides data on the number of deaths over the study period by gender, age group, and region for each year.
Male-to-female ratios were calculated as the ratio of the incidence rate for males relative to that for females. Both the number of deaths from cancers and the population data were available broken down by the following age groups: 0–4 years, 5–9 years, and 10–14 years.
Similarly, data on the monthly numbers of deaths from childhood cancers were also obtained from the HCSO. However, no monthly data on the childhood population aged 0–14 years were available. Therefore, we have used annual population data and the monthly birth and death data to estimate the number of people in this age group by month.
Monthly mortality rates for childhood cancer were calculated as the number of deaths divided by the population in the same month of the year. The proportionate childhood cancer mortality rate was calculated as the fraction of all deaths under 15 years due to a specific cause.
Territorial units were based on the second level of the NUTS 2016 (
Nomenclature des unités territoriales statistiques—Nomenclature of Territorial Units for Statistics, 2016 revision) classification [
10]. These statistical regions (second level of the classification; NUTS2) were as follows (
Figure 1): Budapest (the capital region—formerly part of Central Hungary; HU11), Pest County (the surrounding region—formerly part of Central Hungary; HU12), Central Transdanubia (HU21), Western Transdanubia (HU22), Southern Transdanubia (HU23), Northern Hungary (HU31), Northern Great Plain (HU32), and Southern Great Plain (HU33).
2.2. Statistical Methods
Mortality rates were expressed per 100,000 population per year using the annual mid-year population estimates for the relevant year. Age-standardised mortality rates (ASMRs) in Hungary during the study period were calculated according to the direct method [
11] using the Revised European Standard Population (RESP) [
12] for children aged under 15 years (in three age groups: 0–4, 5–9, and 10–14 years) to make regional mortality rates comparable over time.
Data on the month of death were aggregated over the study period and cyclic trends were analysed using the Walter–Elwood and the Poisson regression methods [
13,
14]. Both methods adjust for the population at risk by grouping the data into months and were used to investigate single or double peaks of seasonality. In contrast, the geometrical model by Edwards [
15], which does not take the population into account, was used as a sensitivity analysis to control for population effects on the cyclical trend.
Trends in the annual numbers of deaths were also investigated using Poisson regression. Incidence rate ratios (IRRs) were calculated together with their corresponding 95% confidence intervals (95% CIs). The main requirement of this model is that the variance of the dependent variable is equal to its mean (“equidispersion”). Since the likelihood ratio test for equidispersion was non-significant, the model assumptions were fulfilled. In a sensitivity analysis, joinpoint regression was also applied to describe the tendency in annual childhood cancer mortality rates.
The death rate from childhood cancers during the two years of the COVID-19 pandemic (2020–2021) was compared using Poisson regression with the death rate from childhood cancers during the previous nearly two decades of the non-pandemic period between 2001 and 2019. Furthermore, to investigate cyclic trends, the non-pandemic study period between 2001 and 2019 was divided into two sub-periods: 2001–2010 and 2011–2019.
A p-value of less than 0.05 was taken to indicate a significant effect. All analyses were performed with the STATA software, version 17.0 (Stata Corp LP, College Station, TX, USA).
3. Results
Overall, 14,931 deaths were registered during the study period among children aged 0–14 years, of which 1092 (7.3%) were deaths from childhood cancer. The most frequent causes of death from childhood cancers were the following: 303 (27.7%) malignant tumours of the central nervous system (C71), 180 (16.5%) lymphoid leukaemia (C91), 92 (8.4%) myeloid leukaemia (C92) and 53 (4.9%) non-Hodgkin lymphoma (C82–C85, C88, C96). In addition, 66 (6%) deaths from childhood cancer occurred during the years of the coronavirus pandemic.
The childhood cancer death rate was significantly higher for boys, as there were 610 (56%) and 482 (44%) deaths in the groups of boys and girls, respectively (
Table 1). The ratio of men to women was 1.27 (95% CI: 1.13–1.143), which slightly decreased to 1.19 in the COVID-19 pandemic period.
During the study period, the age-standardised childhood cancer mortality rate (ASMR) was 3.49 (SE = 0.18) deaths per 100,000 children aged 0–14 years in Hungary; it was significantly (p = 0.02) higher in the non-pandemic period (3.57 per 100,000 children; SE = 0.19) than in the COVID-19 period (2.38 per 100,000 children; SE = 0.5). Similarly, ASMR was significantly (p = 0.02) higher in boys (3.80 deaths per 100,000 children and SE = 0.27) than in girls (3.16 deaths per 100,000 children and SE = 0.25). The risk of childhood cancer mortality was significantly lower in older age groups (5–9 years and 10–14 years) than in children aged under five years (IRR = 0.816; 95% CI: 0.756–0.879; p < 0.001). However, during the COVID-19 pandemic period, the risk of childhood cancer mortality was not significantly different in the age groups (IRR = 0.917; 95% CI: 0.685–1.227; p = 0.56).
Table 1 summarises the main characteristics of childhood mortality for those aged 0–14 years.
The territorial proportions of age-standardised deaths from childhood cancer varied significantly (
p = 0.023), between 2.82 and 4.36 deaths per 100,000 children in the non-pandemic study period. The lowest and highest mortality rates were detected in the regions of Budapest (capital) and Northern Hungary/Northern Great Plain, respectively. The mortality rates remained high in the regions of Northern Hungary and Northern Great Plain during the coronavirus pandemic period in Hungary. However, during the COVID-19 pandemic period, the highest territorial mortality rate of 3.11 deaths per 100,000 children was observed in the Capital region in Hungary (
Figure 1A,B). There were 82 (27%) of 303 deaths from CNS tumours in the regions of Northern Hungary and Northern Great Plain during the study period.
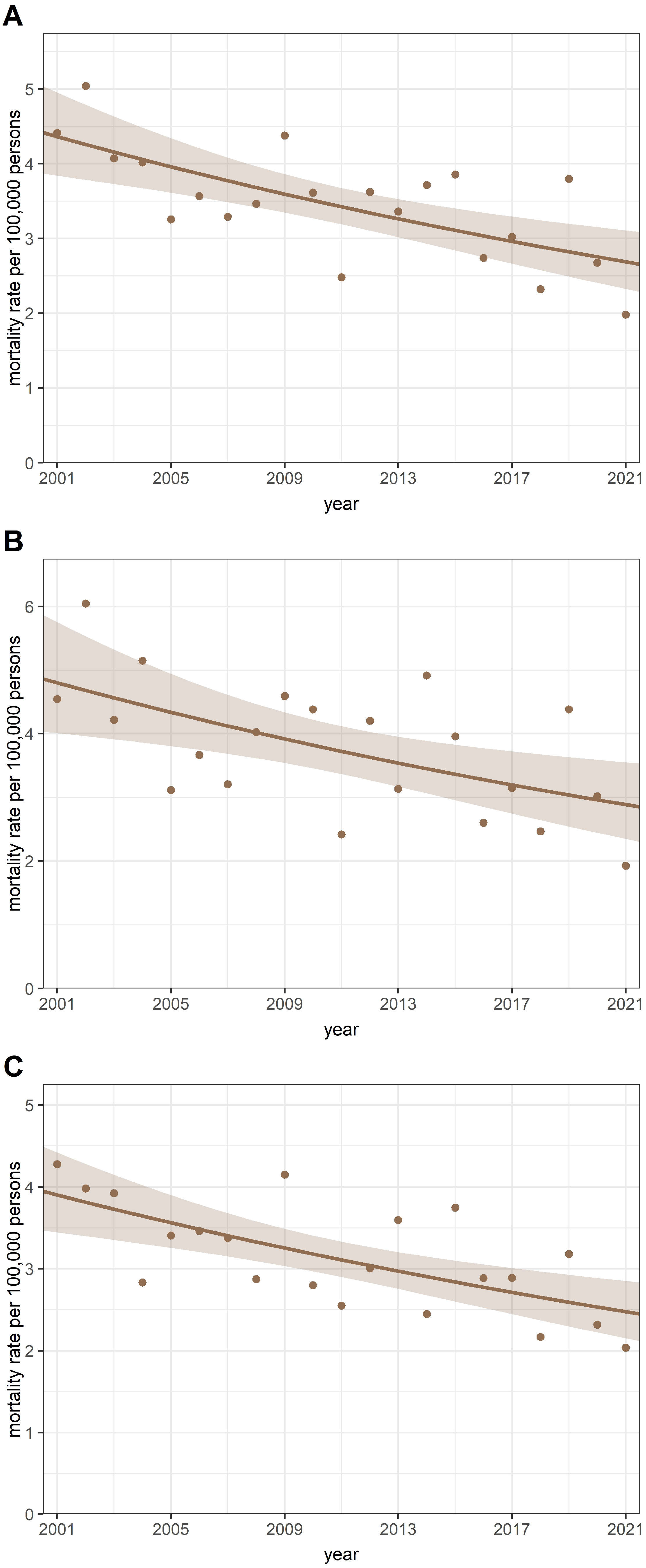
3.1. Annual Trends in Childhood Cancer Mortality Rates
The crude annual mortality rate in children aged 0–14 years declined from a maximum of 66.82 per 100,000 children in 2001 to a minimum of 31.33 per 100,000 children in 2021, and there was a significant IRR trend per annum of 0.963 (95% CI: 0.961–0.966;
p < 0.001). Furthermore, a significantly decreasing trend from a maximum of 5.04 per 100,000 children in 2002 to a minimum of 1.98 per 100,000 children in 2021 was detected for the annual rate of childhood cancer mortality, with an annual IRR of 0.976 (95% CI: 0.966–0.986;
p < 0.001) (
Figure 2A). A similar decreasing annual trend was observed in boys and girls during the study period in Hungary (
Figure 2B,C). The findings of the joinpoint regression analysis confirmed that the coronavirus pandemic did not change the downward trend in childhood cancer mortality in Hungary.
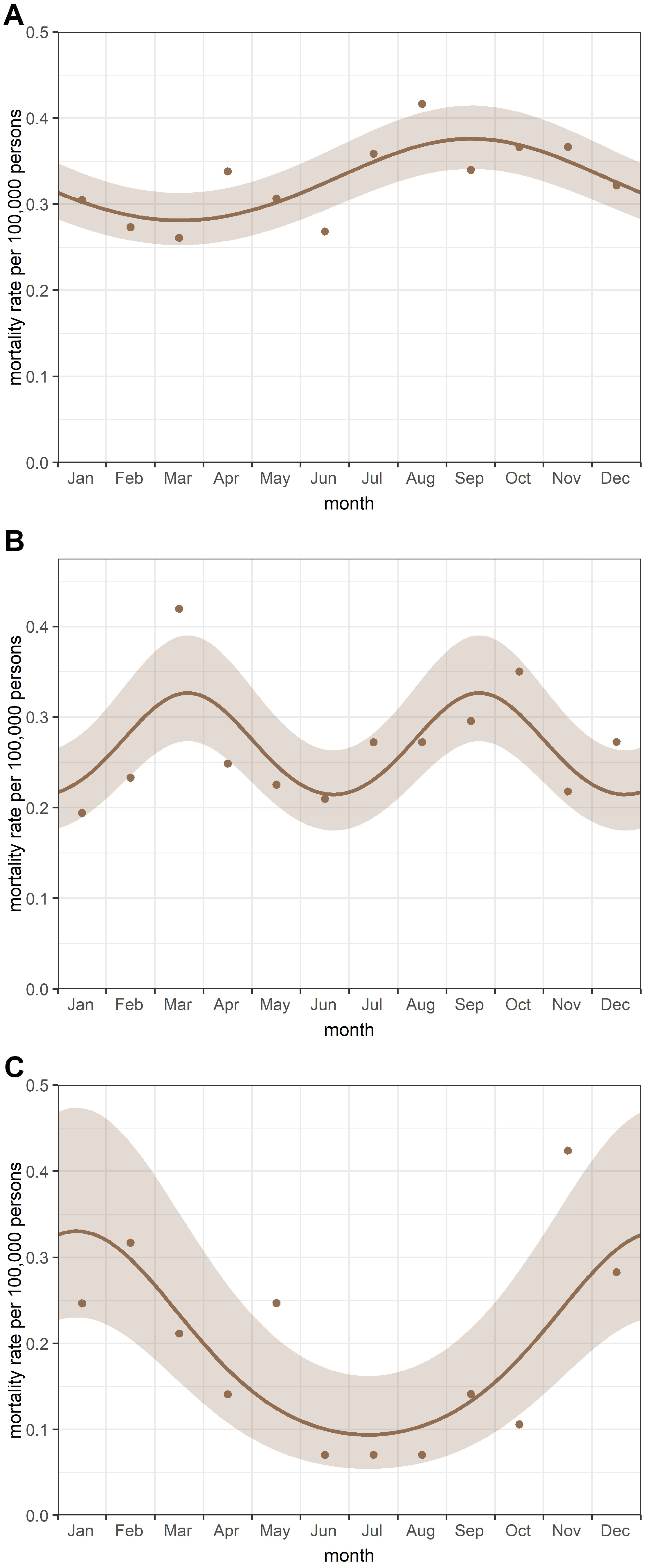
3.2. Cyclic Trends in Childhood Cancer Mortality Rates
No cyclic pattern was observed for the entire study period (i.e., between 2001 and 2021). A significant (
p = 0.039) single peak in September was found in childhood cancer mortality rates in the period 2001–2010 (
Figure 3A). In contrast, a double-peak model was fitted to characterise the seasonal variation in childhood cancer mortality between 2011 and 2019. The peaks were observed in March and September (
p = 0.014) (
Figure 3B). In addition, a significant (
p < 0.001) single peak in January was observed in childhood cancer mortality rates during the coronavirus pandemic period (
Figure 3C). All models had a reasonable goodness-of-fit statistic.
In the sensitivity analyses, the effect of the population on the seasonal variation was investigated. We applied the Edwards test without a population at risk and the Poisson regression using the proportional rate of childhood cancer mortality. The same cyclic trends were revealed using the Edwards test. Similar seasonal variations were also found in the proportionate childhood cancer mortality rates; however, the seasonal effect was not significant in the period between 2001 and 2010. The monthly death rate of children aged 0–14 did not show a cyclical trend during the study period. All models had a reasonable goodness of fit. The aggregate monthly numbers of deaths from childhood cancers between 2001 and 2021 in Hungary are summarised in
Table 2.
4. Discussion
4.1. Main Findings
The ASMR for childhood cancer was 3.49 deaths per 100,000 children aged 0–14 years in Hungary; it was significantly higher in the non-pandemic period (3.57 per 100,000 children) than in the COVID-19 period (2.38 per 100,000 children). The risk of childhood cancer mortality was significantly higher among boys than among girls. Additionally, the risk of childhood cancer mortality was significantly lower in older age groups (5–9 years and 10–14 years) than in children aged under five years.
Changes in the spatial distribution of childhood cancer mortality were also observed in the years before and during the coronavirus pandemic. Although the mortality rate of childhood cancer remained high in the regions of Northern Hungary and Northern Great Plain, during the coronavirus pandemic, the capital (Budapest) had the highest regional mortality in Hungary.
A significant decrease in annual mortality rates for childhood cancers in those under 15 years was found in Hungary during 2001–2021. This trend was not influenced by the coronavirus pandemic.
However, different patterns of seasonal variation were detected in the mortality rates of childhood cancers during the two years of the COVID-19 pandemic and the preceding two-decade non-pandemic period. Significant seasonality was observed in monthly childhood cancer mortality rates, with peaks in September for the 2001–2010 period, March, and September for the 2011–2019 period, and January for the 2020–2021 period.
4.2. Comparison with Other Studies
The ASMR for childhood cancer was 3.49 deaths per 100,000 children aged 0–14 years in Hungary, which was similar to the ASMR of 3.56 per 100,000 children (aged 0–14) reported by Bertuccio et al. [
4]. Similarly, our study also demonstrated that the mortality rates from all neoplasms were significantly higher in males than in females [
16].
Although the mortality rate for childhood cancer remained high in the regions of Northern Hungary and Northern Great Plain, the capital had the highest regional mortality in Hungary during the coronavirus pandemic. The standard of living in Budapest is much higher than in the eastern regions of Hungary. The regions of Northern Hungary and Northern Great Plain are predominantly agricultural areas. Furthermore, in North-Eastern Hungary, Jakab et al. reported a higher incidence of central nervous system tumours in children [
17]. The EUROCARE-5 study reported that childhood cancer survival time in Hungary was below the European average for both leukaemias and CNS tumours during the period 1999–2007 [
18]. In a recent study, Jakab et al. [
5] reported a similarly lower survival time than that reported in a French study [
19]. Additionally, this study reported regional differences in cancer mortality among children under 15 years old [
19]. Although we did not have morbidity data, our results showed that tumours of the central nervous system were the most common cause of childhood cancer deaths during the study period.
Childhood cancer death rates have declined in many developed countries [
18]. Despite the downward trend, the Hungarian ASMR is still higher than in other EU countries [
4].
Seasonal variation in cancer mortality is rarely investigated. In a previous study, Nyári and McNally also revealed no seasonal trend [
20] in mortality rates of childhood cancers. Similarly, we have not found seasonality for the entire study period (2001–2021). However, we have revealed significant changes in the cyclical pattern of childhood cancer deaths in the sub-periods. A significant single peak in childhood cancer mortality rates was found in the periods from 2001 to 2010 and between 2020 and 2021 in Hungary, and double-peak seasonality was observed from 2011 to 2019. A significant peak in September was detected during the nearly two decades of the non-pandemic period between 2001 and 2019. We hypothesise that the effect of the “early autumn depression” might affect the increased accumulation of deaths from childhood cancers. According to several studies, seasonal affective disorder (SAD) can occur not only in winter but also in summer [
21,
22]. Therefore, the life expectancy of patients may deteriorate by the end of summer. In addition, Virág and Nyári described a significant cyclical variation in proportionate mortality for all cancer sites examined, with a peak in August or September in adults [
23]. This suggests that the cancer death rate was higher at the end of August or at the beginning of September. In addition, higher average temperature changes were also observed in these months in Hungary [
24].
Furthermore, the role of the respiratory syncytial virus (RSV) can also be assumed in the cyclical trend [
25]. In a study, double peaks of RSV infection were reported in spring and autumn in temperate regions [
25] and Bloom-Feshbach et al. found the peak of the flu epidemic and the RSV epidemic in the continental climate in the northern hemisphere was in February [
26]. Studies from France, the United Kingdom, and Hungary described the role of infections around the time of birth in the aetiology of some childhood cancers [
27,
28,
29,
30]. However, the role of environmental effects in the aetiology of mortality from childhood cancers has not yet been investigated in detail.
During the years of the pandemic, the change in the cyclic trend can be clearly explained by active protection. Travel restrictions also reduced the number of infectious diseases brought home. In addition, patients were treated to a high standard and according to treatment protocols.
4.3. Strengths and Limitations of Our Study
Mortality data were obtained from the vital register of Hungary, which has one of the best statistics performance indices in the world [
31]. The Hungarian Central Statistical Office applies the rules adopted by the World Health Assembly (WHA) regarding the selection of a single cause or condition, from death certificates, for the routine tabulation of mortality statistics to standardise the production of mortality data. Thus, there were no public data available on secondary cancers as a cause of death. Although trends in cancer mortality may be a combined result of incidence and survival, morbidity data were not available for all neoplasms in children aged 0–14 years.
Our study demonstrated significant regional and seasonal differences in the pattern of childhood all-cancer mortality in Hungary. However, there were no analyses carried out to differentiate mortality by cancer type. In this ęcological study, we have investigated the annual and seasonal pattern of mortality from childhood cancers in children aged 0–14 years. Although the number of events (deaths) was somewhat small in the ‘pandemic period’ (covering two years), the Walter–Elwood test is a powerful method in cases of extreme values.
Significant single-peak and significant double-peak models were observed to characterise the seasonal variation in mortality rates for childhood cancers. Despite the lack of direct evidence for respiratory syncytial virus infections in the analyses, we can speculate that these infections may play a role in the aetiology of mortality from childhood cancers [
23]. Furthermore, the reliability of the fitted models was high. In addition, the investigation of seasonality is an important component in understanding the aetiological description of certain diseases.
Although seasonal patterns in all-cancer mortality have already been examined by other investigators, to the best of our knowledge, this is the first epidemiological study to report territorial differences and the effect of seasonality in mortality for childhood cancers in those aged 0–14 years in Hungary.
5. Conclusions
We provided a detailed description of seasonal effects related to mortality rates for childhood cancer deaths among children under 15 years. Although the annual trend in childhood cancer mortality was not affected by the coronavirus pandemic, there was a significant change in the mortality pattern of childhood cancer in Hungary during the two years of the COVID-19 pandemic and the preceding two-decade non-pandemic period. During the years of the pandemic, the cyclic trend in mortality from childhood cancer has also changed. Differences in the regional distribution of childhood cancer mortality were also observed by comparing periods before and during the pandemic.
Since cyclic trends in the aetiology of mortality may show some effect of environmental factors, we speculate that mortality from childhood cancer might have been (at least partly) related to respiratory infections. These findings could prove useful in preventive strategies, but further cohort studies should be carried out to investigate this hypothesis using detailed individual data.
Author Contributions
Conceptualization, T.L. and T.A.N.; methodology, T.L. and T.A.N.; software, T.L. and K.N.; formal analysis, K.N., T.L. and T.A.N.; investigation, K.N.; data curation, K.N.; writing—original draft preparation, K.N., T.L. and T.A.N.; writing—review and editing, K.N., T.L. and T.A.N.; visualization, T.L.; supervision, T.A.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
No ethics approval was necessary according to the Hungarian Law in usage of statistical data (Act CLV of 2016 on Official Statistics).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in this article.
Acknowledgments
Special thanks to the Managing Editor for her help.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Magnani, C.; Pastore, G.; Coebergh, J.W.; Viscomi, S.; Spix, C.; Steliarova-Foucher, E. Trends in survival after childhood cancer in Europe, 1978–1997: Report from the Automated Childhood Cancer Information System project (ACCIS). Eur. J. Cancer 2006, 42, 1981–2005. [Google Scholar] [CrossRef] [PubMed]
- Botta, L.; Gatta, G.; Capocaccia, R.; Stiller, C.; Canete, A.; Dal Maso, L.; Innos, K.; Mihor, A.; Erdmann, F.; Spix, C.; et al. Long-term survival and cure fraction estimates for childhood cancer in Europe (EUROCARE-6): Results from a population-based study. Lancet Oncol. 2022, 23, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.S.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995-2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef] [PubMed]
- Bertuccio, P.; Alicandro, G.; Malvezzi, M.; Carioli, G.; Boffetta, P.; Levi, F.; La Vecchia, C.; Negri, E. Childhood cancer mortality trends in Europe, 1990–2017, with focus on geographic differences. Cancer Epidemiol. 2020, 67, 101768. [Google Scholar] [CrossRef]
- Jakab, Z.; Garami, M.; Bartyik, K.; Csoka, M.; Erdelyi, D.J.; Hauser, P.; Juhasz, A.; Kelemen, A.; Krivan, G.; Masat, P.; et al. Late mortality in survivors of childhood cancer in Hungary. Sci. Rep. 2020, 10, 10761. [Google Scholar] [CrossRef]
- Feltbower, R.G.; Pearce, M.S.; Dickinson, H.O.; Parker, L.; McKinney, P.A. Seasonality of birth for cancer in Northern England, UK. Paediatr. Perinat. Epidemiol. 2001, 15, 338–345. [Google Scholar] [CrossRef]
- Ottoffy, G.; Szigeti, E.; Bartyik, K.; Nyari, C.; Parker, L.; McNally, R.J.; Nyari, T.A. Investigating the relationship between mortality from respiratory diseases and childhood acute lymphoblastic leukaemia in Hungary. Pathol. Oncol. Res. 2015, 21, 53–57. [Google Scholar] [CrossRef]
- Terenziani, M.; Massimino, M.; Biassoni, V.; Casanova, M.; Chiaravalli, S.; Ferrari, A.; Luksch, R.; Meazza, C.; Podda, M.; Schiavello, E.; et al. SARS-CoV-2 disease and children under treatment for cancer. Pediatr. Blood Cancer 2020, 67, e28346. [Google Scholar] [CrossRef]
- Hungarian Central Statistical Office. Dissemination Database. Available online: https://statinfo.ksh.hu/Statinfo/themeSelector.jsp?&lang=en (accessed on 24 September 2024).
- Eurostat. Regions in the European Union. Available online: https://ec.europa.eu/eurostat/documents/3859598/9397402/KS-GQ-18-007-EN-N.pdf (accessed on 24 September 2024).
- Association of Public Health Epidemiologists in Ontario. Standardization of Rates. Available online: http://core.apheo.ca/resources/indicators/Standardization%20report_NamBains_FINALMarch16.pdf (accessed on 24 September 2024).
- Eurostat. Revision of the European Standard Population. Available online: https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8f (accessed on 24 September 2024).
- Walter, S.D.; Elwood, J.M. A test for seasonality of events with a variable population at risk. Br. J. Prev. Soc. Med. 1975, 29, 18–21. [Google Scholar] [CrossRef]
- Stolwijk, A.M.; Straatman, H.; Zielhuis, G.A. Studying seasonality by using sine and cosine functions in regression analysis. J. Epidemiol. Community Health 1999, 53, 235–238. [Google Scholar] [CrossRef]
- Edwards, J.H. The recognition and estimation of cyclic trends. Ann. Hum. Genet. 1961, 25, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.S.; Parker, L. Childhood cancer registrations in the developing world: Still more boys than girls. Int. J. Cancer 2001, 91, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Jakab, Z.; Balogh, E.; Kiss, C.; Olah, E. Epidemiologic studies in a population-based childhood cancer registry in Northeast Hungary. Med. Pediatr. Oncol. 2002, 38, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Botta, L.; Rossi, S.; Aareleid, T.; Bielska-Lasota, M.; Clavel, J.; Dimitrova, N.; Jakab, Z.; Kaatsch, P.; Lacour, B.; et al. Childhood cancer survival in Europe 1999–2007: Results of EUROCARE-5—A population-based study. Lancet Oncol. 2014, 15, 35–47. [Google Scholar] [CrossRef]
- Poulalhon, C.; Goujon, S.; Marquant, F.; Faure, L.; Guissou, S.; Bonaventure, A.; Desandes, E.; Rios, P.; Lacour, B.; Clavel, J. Factors associated with 5- and 10-year survival among a recent cohort of childhood cancer survivors (France, 2000–2015). Cancer Epidemiol. 2021, 73, 101950. [Google Scholar] [CrossRef]
- Nyari, T.A.; McNally, R. Seasonal variation in childhood mortality. J. Matern. Fetal Neonatal Med. 2020, 33, 4055–4061. [Google Scholar] [CrossRef] [PubMed]
- Fonte, A.; Coutinho, B. Seasonal sensitivity and psychiatric morbidity: Study about seasonal affective disorder. BMC Psychiatry 2021, 21, 317. [Google Scholar] [CrossRef]
- Boyce, P.; Parker, G. Seasonal affective disorder in the southern hemisphere. Am. J. Psychiatry 1988, 145, 96–99. [Google Scholar] [CrossRef]
- Virag, K.; Nyari, T.A. Seasonal variation of cancer mortality in Hungary between 1984 and 2013. Scand J. Public Health 2019, 47, 492–496. [Google Scholar] [CrossRef]
- Hungarian Meteorological Service. Monthly Mean Temperature of Hungary Between 1971 and 2000. Available online: https://www.met.hu/en/eghajlat/magyarorszag_eghajlata/altalanos_eghajlati_jellemzes/homerseklet/ (accessed on 24 September 2024).
- Borchers, A.T.; Chang, C.; Gershwin, M.E.; Gershwin, L.J. Respiratory syncytial virus—A comprehensive review. Clin. Rev. Allergy Immunol. 2013, 45, 331–379. [Google Scholar] [CrossRef]
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal variations in seasonal activity of influenza and respiratory syncytial virus (RSV): A global comparative review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef] [PubMed]
- Bamouni, S.; Hemon, D.; Faure, L.; Clavel, J.; Goujon, S. Seasonal variations in childhood leukaemia incidence in France, 1990–2014. Cancer Causes Control 2021, 32, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Awounou, D.; Lacour, B.; Desandes, E.; Guissou, S.; Cassoux, N.; Doz, F.; Dufour, C.; Minard-Colin, V.; Schleiermacher, G.; Taque, S.; et al. Seasonality of main childhood embryonal tumours and rhabdomyosarcoma, France, 2000–2015. Cancer Med. 2023, 12, 8789–8803. [Google Scholar] [CrossRef] [PubMed]
- Nyari, T.A.; Kajtar, P.; Bartyik, K.; Thurzo, L.; McNally, R.; Parker, L. Seasonal variation of childhood acute lymphoblastic leukaemia is different between girls and boys. Pathol. Oncol. Res. 2008, 14, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, H.O.; Nyari, T.A.; Parker, L. Childhood solid tumours in relation to infections in the community in Cumbria during pregnancy and around the time of birth. Br. J. Cancer 2002, 87, 746–750. [Google Scholar] [CrossRef]
- Phillips, D.E.; Lozano, R.; Naghavi, M.; Atkinson, C.; Gonzalez-Medina, D.; Mikkelsen, L.; Murray, C.J.; Lopez, A.D. A composite metric for assessing data on mortality and causes of death: The vital statistics performance index. Popul. Health Metr. 2014, 12, 14. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}
{kind=link}