
Extracellular Vesicles May Predict Response to Atezolizumab Plus Bevacizumab in Patients with Advanced Hepatocellular Carcinoma
 ,
,  , , ,
, , ,  ,
, 
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Design of Study and Patient Cohort
2.2. Clinical and Laboratory Assessment
2.3. Measurement of EV Characteristics
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Cohort
3.2. Size, Concentration and Zeta Potential of EVs in Patients with Advanced HCC
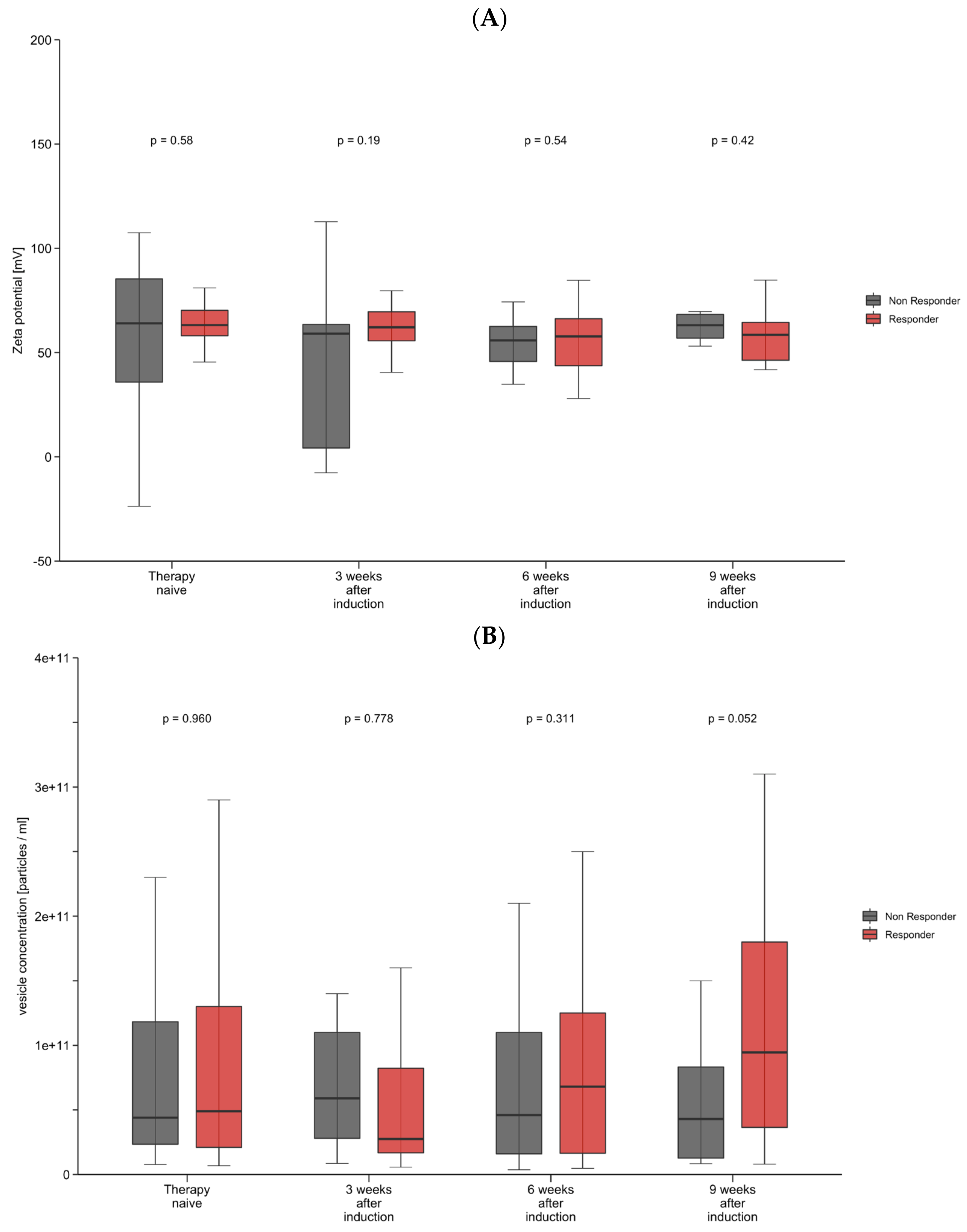
3.3. Decrease in Zeta Potential and Increase in Vesicle Concentration May Predict Treatment Outcome
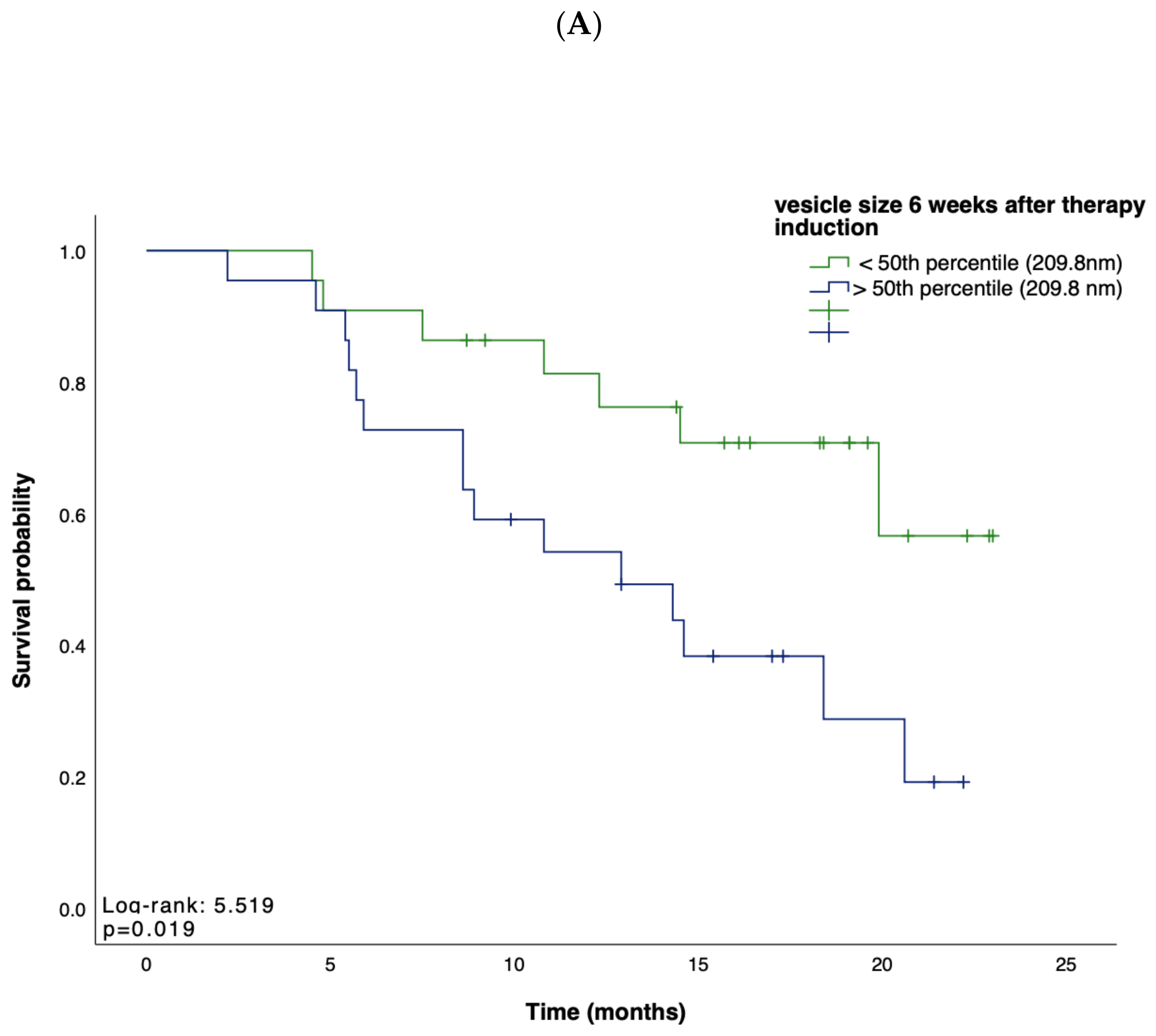
3.4. Small Vesicles Indicate a Favorable Prognosis
3.5. Changes in Vesicle Size Might Serve as a Marker for the Duration of Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2016, 2, 16018. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Finn, R.S.; Bentley, G.; Britten, C.D.; Amado, R.; Busuttil, R.W. Targeting vascular endothelial growth factor with the monoclonal antibody bevacizumab inhibits human hepatocellular carcinoma cells growing in an orthotopic mouse model. Liver Int. 2009, 29, 284–290. [Google Scholar] [CrossRef]
- Herbst, R.S.; Soria, J.C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014, 515, 563–567. [Google Scholar] [CrossRef]
- Motz, G.T.; Santoro, S.P.; Wang, L.P.; Garrabrant, T.; Lastra, R.R.; Hagemann, I.S.; Lal, P.; Feldman, M.D.; Benencia, F.; Coukos, G. Tumor endothelium FasL establishes a selective immune barrier promoting tolerance in tumors. Nat. Med. 2014, 20, 607–615. [Google Scholar] [CrossRef]
- Voron, T.; Colussi, O.; Marcheteau, E.; Pernot, S.; Nizard, M.; Pointet, A.L.; Latreche, S.; Bergaya, S.; Benhamouda, N.; Tanchot, C.; et al. VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J. Exp. Med. 2015, 212, 139–148. [Google Scholar] [CrossRef]
- Hegde, P.S.; Wallin, J.J.; Mancao, C. Predictive markers of anti-VEGF and emerging role of angiogenesis inhibitors as immunotherapeutics. Semin. Cancer Biol. 2018, 52, 117–124. [Google Scholar] [CrossRef]
- Wallin, J.J.; Bendell, J.C.; Funke, R.; Sznol, M.; Korski, K.; Jones, S.; Hernandez, G.; Mier, J.; He, X.; Hodi, F.S.; et al. Atezolizumab in combination with bevacizumab enhances antigen-specific T-cell migration in metastatic renal cell carcinoma. Nat. Commun. 2016, 7, 12624. [Google Scholar] [CrossRef]
- Donnini, S.; Filippelli, A.; Ciccone, V.; Spini, A.; Ristori, E.; Ziche, M.; Morbidelli, L. Antiangiogenic drugs: Chemosensitizers for combination cancer therapy. In Antiangiogenic Drugs as Chemosensitizers in Cancer Therapy; Elsevier: Amsterdam, The Netherlands, 2022; pp. 29–66. [Google Scholar]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin(R)) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Pinyol, R.; Kelley, R.K.; El-Khoueiry, A.; Reeves, H.L.; Wang, X.W.; Gores, G.J.; Villanueva, A. Molecular pathogenesis and systemic therapies for hepatocellular carcinoma. Nat. Cancer 2022, 3, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Finn, R.S.; Qin, S.; Ikeda, M.; Zhu, A.X.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.; et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma (IMbrave150): An open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Scheiner, B.; Pomej, K.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Waidmann, O.; Himmelsbach, V.; Schulze, K.; von Felden, J.; Frundt, T.W.; et al. Prognosis of patients with hepatocellular carcinoma treated with immunotherapy—Development and validation of the CRAFITY score. J. Hepatol. 2022, 76, 353–363. [Google Scholar] [CrossRef]
- Wang, J.; Wang, X.; Zhang, X.; Shao, T.; Luo, Y.; Wang, W.; Han, Y. Extracellular Vesicles and Hepatocellular Carcinoma: Opportunities and Challenges. Front. Oncol. 2022, 12, 884369. [Google Scholar] [CrossRef]
- Margolis, L.; Sadovsky, Y. The biology of extracellular vesicles: The known unknowns. PLoS Biol. 2019, 17, e3000363. [Google Scholar] [CrossRef]
- Kogure, T.; Lin, W.L.; Yan, I.K.; Braconi, C.; Patel, T. Intercellular nanovesicle-mediated microRNA transfer: A mechanism of environmental modulation of hepatocellular cancer cell growth. Hepatology 2011, 54, 1237–1248. [Google Scholar] [CrossRef]
- Webber, J.; Yeung, V.; Clayton, A. Extracellular vesicles as modulators of the cancer microenvironment. Semin. Cell Dev. Biol. 2015, 40, 27–34. [Google Scholar] [CrossRef]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding light on the cell biology of extracellular vesicles. Nat. Rev. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar] [CrossRef]
- Buzas, E.I. The roles of extracellular vesicles in the immune system. Nat. Rev. Immunol. 2023, 23, 236–250. [Google Scholar] [CrossRef]
- Marar, C.; Starich, B.; Wirtz, D. Extracellular vesicles in immunomodulation and tumor progression. Nat. Immunol. 2021, 22, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Szatanek, R.; Baj-Krzyworzeka, M.; Zimoch, J.; Lekka, M.; Siedlar, M.; Baran, J. The Methods of Choice for Extracellular Vesicles (EVs) Characterization. Int. J. Mol. Sci. 2017, 18, 1153. [Google Scholar] [CrossRef] [PubMed]
- Clogston, J.D.; Patri, A.K. Zeta potential measurement. Methods Mol. Biol. 2011, 697, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Jost-Brinkmann, F.; Demir, M.; Wree, A.; Luedde, T.; Loosen, S.H.; Muller, T.; Tacke, F.; Roderburg, C.; Mohr, R. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma: Results from a German real-world cohort. Aliment. Pharmacol. Ther. 2023, 57, 1313–1325. [Google Scholar] [CrossRef]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 871–873. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Seymour, L.; Litière, S.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Standardisation and disease-specific adaptations: Perspectives from the RECIST Working Group. Eur. J. Cancer 2016, 62, 138–145. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef]
- Yamamoto, S.; Niida, S.; Azuma, E.; Yanagibashi, T.; Muramatsu, M.; Huang, T.T.; Sagara, H.; Higaki, S.; Ikutani, M.; Nagai, Y.; et al. Inflammation-induced endothelial cell-derived extracellular vesicles modulate the cellular status of pericytes. Sci. Rep. 2015, 5, 8505. [Google Scholar] [CrossRef]
- Mehdiani, A.; Maier, A.; Pinto, A.; Barth, M.; Akhyari, P.; Lichtenberg, A. An innovative method for exosome quantification and size measurement. J. Vis. Exp. 2015, 95, 50974. [Google Scholar] [CrossRef]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA A Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.-y.; Leung, T.W.; Liew, C.-t.; Ho, S.K.; Simon, C.; Tang, A.M. Preoperative systemic chemoimmunotherapy and sequential resection for unresectable hepatocellular carcinoma. Ann. Surg. 2001, 233, 236. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Dao, T.V.; Toni, E.N.D.; et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022, 1, EVIDoa2100070. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Fu, H.; Hao, J.; Yang, Z.; Qiao, X.; Li, Y.; Zhao, R.; Lin, T.; Wang, Y.; Wang, M. Tumor-derived exosomal PD-L1: A new perspective in PD-1/PD-L1 therapy for lung cancer. Front. Immunol. 2024, 15, 1342728. [Google Scholar] [CrossRef] [PubMed]
- Abhange, K.; Makler, A.; Wen, Y.; Ramnauth, N.; Mao, W.; Asghar, W.; Wan, Y. Small extracellular vesicles in cancer. Bioact. Mater. 2021, 6, 3705–3743. [Google Scholar] [CrossRef]
- Kwok, Z.H.; Ni, K.; Jin, Y. Extracellular Vesicle Associated Non-Coding RNAs in Lung Infections and Injury. Cells 2021, 10, 965. [Google Scholar] [CrossRef]
- Scholer, D.; Castoldi, M.; Jordens, M.S.; Schulze-Hagen, M.; Kuhl, C.; Keitel, V.; Luedde, T.; Roderburg, C.; Loosen, S.H. Enlarged extracellular vesicles are a negative prognostic factor in patients undergoing TACE for primary or secondary liver cancer-a case series. PLoS ONE 2021, 16, e0255983. [Google Scholar] [CrossRef]
- Wu, D.; Zhu, H.; Wang, H. Extracellular Vesicles in Non-alcoholic Fatty Liver Disease and Alcoholic Liver Disease. Front. Physiol. 2021, 12, 707429. [Google Scholar] [CrossRef]
- Grossini, E.; Smirne, C.; Venkatesan, S.; Tonello, S.; D’Onghia, D.; Minisini, R.; Cantaluppi, V.; Sainaghi, P.P.; Comi, C.; Tanzi, A.; et al. Plasma Pattern of Extracellular Vesicles Isolated from Hepatitis C Virus Patients and Their Effects on Human Vascular Endothelial Cells. Int. J. Mol. Sci. 2023, 24, 10197. [Google Scholar] [CrossRef]
- Zhang, S.; Yu, J.; Rao, K.; Cao, J.; Ma, L.; Yu, Y.; Li, Z.; Zeng, Z.; Qian, Y.; Chen, M.; et al. Liver-derived extracellular vesicles from patients with hepatitis B virus-related acute-on-chronic liver failure impair hepatic regeneration by inhibiting on FGFR2 signaling via miR-218-5p. Hepatol. Int. 2023, 17, 833–849. [Google Scholar] [CrossRef]
- Arbelaiz, A.; Azkargorta, M.; Krawczyk, M.; Santos-Laso, A.; Lapitz, A.; Perugorria, M.J.; Erice, O.; Gonzalez, E.; Jimenez-Aguero, R.; Lacasta, A.; et al. Serum extracellular vesicles contain protein biomarkers for primary sclerosing cholangitis and cholangiocarcinoma. Hepatology 2017, 66, 1125–1143. [Google Scholar] [CrossRef] [PubMed]
- Thietart, S.; Rautou, P.E. Extracellular vesicles as biomarkers in liver diseases: A clinician’s point of view. J. Hepatol. 2020, 73, 1507–1525. [Google Scholar] [CrossRef] [PubMed]
- Loric, S.; Denis, J.A.; Desbene, C.; Sabbah, M.; Conti, M. Extracellular Vesicles in Breast Cancer: From Biology and Function to Clinical Diagnosis and Therapeutic Management. Int. J. Mol. Sci. 2023, 24, 7208. [Google Scholar] [CrossRef] [PubMed]
- Szajnik, M.; Derbis, M.; Lach, M.; Patalas, P.; Michalak, M.; Drzewiecka, H.; Szpurek, D.; Nowakowski, A.; Spaczynski, M.; Baranowski, W.; et al. Exosomes in Plasma of Patients with Ovarian Carcinoma: Potential Biomarkers of Tumor Progression and Response to Therapy. Gynecol Obs. 2013, 3, 3. [Google Scholar] [CrossRef]
- Sato, S.; Weaver, A.M. Extracellular vesicles: Important collaborators in cancer progression. Essays Biochem. 2018, 62, 149–163. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 53) | Responders (n = 39) | Non-Responders (n = 14) | p-Value | |
|---|---|---|---|---|
| Male n (%) | 47 (89) | 35 (90) | 12 (86) | 0.683 |
| Age at diagnosis (median/IQR) | 64 (58, 71) | 63 (58, 70) | 68 (60, 73) | 0.369 |
| BMI (median/IQR) | 26.4 (23.8, 29.6) | 26.2 (24.0, 29.0) | 28.4 (23.3, 31.7) | 0.490 |
| ECOG score n (%) | ||||
| ECOG 0 | 39 (74) | 29 (74) | 10 (71) | 0.831 |
| ECOG ≥ 1 | 14 (27) | 10 (26) | 4 (28) | 0.924 |
| Liver cirrhosis n (%) | 43 (81) | 31 (80) | 12 (86) | 0.609 |
| Child–Pugh score n (%) | ||||
| Child–Pugh Score A | 32 (60) | 23 (59) | 9 (64) | 0.727 |
| Child–Pugh Score B | 11 (21) | 8 (21) | 3 (21) | 0.943 |
| Viral hepatitis n (%) | 23 (43) | 19 (49) | 4 (29) | 0.129 |
| Hepatitis B | 10 (19) | 7 (18) | 3 (21) | 0.775 |
| Hepatitis C | 13 (25) | 12 (31) | 1 (7) | 0.078 |
| Hepatitis B/D | 1 (2) | 1 (3) | 0 (0) | 0.545 |
| ALD n (%) | 20 (38) | 14 (36) | 6 (43) | 0.645 |
| MASH n (%) | 4 (8) | 3 (8) | 1 (7) | 0.947 |
| Barcelona Clinic Liver Cancer Classification n (%) | ||||
| BCLC B | 17 (32) | 14 (36) | 3 (21) | 0.320 |
| BCLC C | 36 (68) | 24 (62) | 11 (79) | 0.248 |
| MVI n (%) | 25 (47) | 15 (39) | 10 (71) | 0.034 |
| EHS n (%) | 18 (34) | 13 (33) | 5 (36) | 0.872 |
| Previous locoregional therapies n (%) | 28 (53) | 20 (51) | 8 (57) | 0.709 |
| TACE | 16 (30) | 12 (31) | 4 (29) | 0.878 |
| RFA | 4 (8) | 4 (10) | 0 (0) | 0.213 |
| AL | 21 (40) | 14 (36) | 7 (50) | 0.355 |
| SIRT | 2 (4) | 2 (5) | 0 (0) | 0.388 |
| Previous surgery | 17 (32) | 12 (31) | 5 (36) | 0.734 |
| Lab values prior to immunotherapy (median/IQR) | ||||
| AFP [μg/L] | 32.8 (7.8, 561.0) | 31.1 (7.7, 658.0) | 78.6 (6.8, 742.0) | 0.948 |
| Albumin [g/L] | 39.5 (34.2, 42.3) | 39.1 (34.0, 42.9) | 40.7 (35.7, 42.2) | 0.521 |
| Bilirubin [mg/dL] | 0.8 (0.5, 1.1) | 0.7 (0.5, 1.3) | 0.9 (0.6, 1.1) | 0.348 |
| Lymphocytes [/nL] | 1.4 (0.9, 2.3) | 1.5 (1.1, 2.2) | 1.2 (0.8, 2.0) | 0.376 |
| Neutrophiles [/nL] | 4.7 (3.1, 6.0) | 4.1 (3.0, 5.0) | 5.7 (4.2, 7.7) | 0.026 |
| NLR score | 3.3 (2.0, 4.5) | 2.6 (1.7, 4.3) | 4.1 (3.1, 6.9) | 0.012 |
| ALBI-score | −2.6 (−2.9, −2.1) | −2.6 (−2.8, −2.1) | −2.6 (−2.9, −2.4) | 0.791 |
| Clinical outcomes (median/IQR) | ||||
| PFS in months | 7.6 (3.5, 12.9) | 9.3 (7.0, 14.3) | 3.2 (2.8, 3.4) | <0.001 |
| OS in months | 17.9 (10.6, 23.9) | 18.7 (12.8, 22.2) | 12.6 (5.6, 28.1) | 0.225 |
| All Patients (n = 53) | Responders (n = 39) | Non-Responders (n = 14) | p-Value | |
|---|---|---|---|---|
| Vesicle size (median/IQR) [nm] | ||||
| Therapy naive | 204.5 (185.4, 227.2) | 207.9 (184.6, 229.1) | 202.6 (184.5, 224.6) | 0.626 |
| 3 weeks after induction | 207.4 (193.1, 216.9) | 207.0 (192.0, 223.7) | 209.0 (193.5, 213.8) | 0.826 |
| 6 weeks after induction | 209.8 (186.3, 230.3) | 211.3 (180.9, 227.2) | 203.1 (190.9, 233.9) | 0.961 |
| 9 weeks after induction | 209.9 (187.9, 230.5) | 197.2 (186.1, 219.3) | 221.8 (208.0, 244.0) | 0.035 |
| Vesicle concentration (median/IQR) [particles/mL] | ||||
| Therapy naive | 5.00 × 1010 (2.15 × 1010, 1.38 × 1011) | 5.25 × 1010 (2.05 × 1010, 1.40 × 1011) | 4.40 × 1010 (2.20 × 1010, 1.43 × 1011) | 0.960 |
| 3 weeks after induction | 3.00 × 1010 (1.68 × 1010, 1.10 × 1011) | 2.80 × 1010 (1.65 × 1010, 1.04 × 1011) | 5.90 × 1010 (2.00 × 1010, 1.20 × 1011) | 0.778 |
| 6 weeks after induction | 6.80 × 1010 (1.60 × 1010, 1.30 × 1011) | 6.80 × 1010 (1.60 × 1010, 1.30 × 1011) | 6.80 × 1010 (1.55 × 1010, 1.40 × 1011) | 0.311 |
| 9 weeks after induction | 5.90 × 1010 (1.78 × 1010, 1.45 × 1011) | 9.45 × 1010 (2.55 × 1010, 1.80 × 1011) | 4.30 × 1010 (1.23 × 1010, 9.38 × 1011) | 0.052 |
| Zeta potential (median/IQR) [mV] | ||||
| Therapy naive | 63.2 (54.7, 71.4) | 63.2 (57.3, 70.5) | 64.0 (29.5, 89.6) | 0.580 |
| 3 weeks after induction | 61.3 (44.9, 69.6) | 62.4 (55.6, 74.7) | 59.1 (4.2, 64.3) | 0.191 |
| 6 weeks after induction | 57.8 (43.7, 70.0) | 57.8 (42.6, 67.0) | 57.4 (43.0, 73.4) | 0.536 |
| 9 weeks after induction | 60.3 (47.8, 67.3) | 58.5 (43.3, 65.1) | 63.12 (54.4, 69.2) | 0.423 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egerer, M.; Schuch, K.; Schöler, D.; Artusa, F.; Püngel, T.; Holtman, T.M.; Loosen, S.H.; Demir, M.; Wree, A.; Luedde, T.; et al. Extracellular Vesicles May Predict Response to Atezolizumab Plus Bevacizumab in Patients with Advanced Hepatocellular Carcinoma. Cancers 2024, 16, 3651. https://doi.org/10.3390/cancers16213651
Egerer M, Schuch K, Schöler D, Artusa F, Püngel T, Holtman TM, Loosen SH, Demir M, Wree A, Luedde T, et al. Extracellular Vesicles May Predict Response to Atezolizumab Plus Bevacizumab in Patients with Advanced Hepatocellular Carcinoma. Cancers. 2024; 16(21):3651. https://doi.org/10.3390/cancers16213651
Chicago/Turabian StyleEgerer, Mara, Kathrin Schuch, David Schöler, Fabian Artusa, Tobias Püngel, Theresa Maria Holtman, Sven H. Loosen, Münevver Demir, Alexander Wree, Tom Luedde, and et al. 2024. "Extracellular Vesicles May Predict Response to Atezolizumab Plus Bevacizumab in Patients with Advanced Hepatocellular Carcinoma" Cancers 16, no. 21: 3651. https://doi.org/10.3390/cancers16213651
APA StyleEgerer, M., Schuch, K., Schöler, D., Artusa, F., Püngel, T., Holtman, T. M., Loosen, S. H., Demir, M., Wree, A., Luedde, T., Tacke, F., Roderburg, C., & Mohr, R. (2024). Extracellular Vesicles May Predict Response to Atezolizumab Plus Bevacizumab in Patients with Advanced Hepatocellular Carcinoma. Cancers, 16(21), 3651. https://doi.org/10.3390/cancers16213651