
Multiethnic Trends in Early Onset Colorectal Cancer


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analyses
3. Results
3.1. Demographic Characteristics
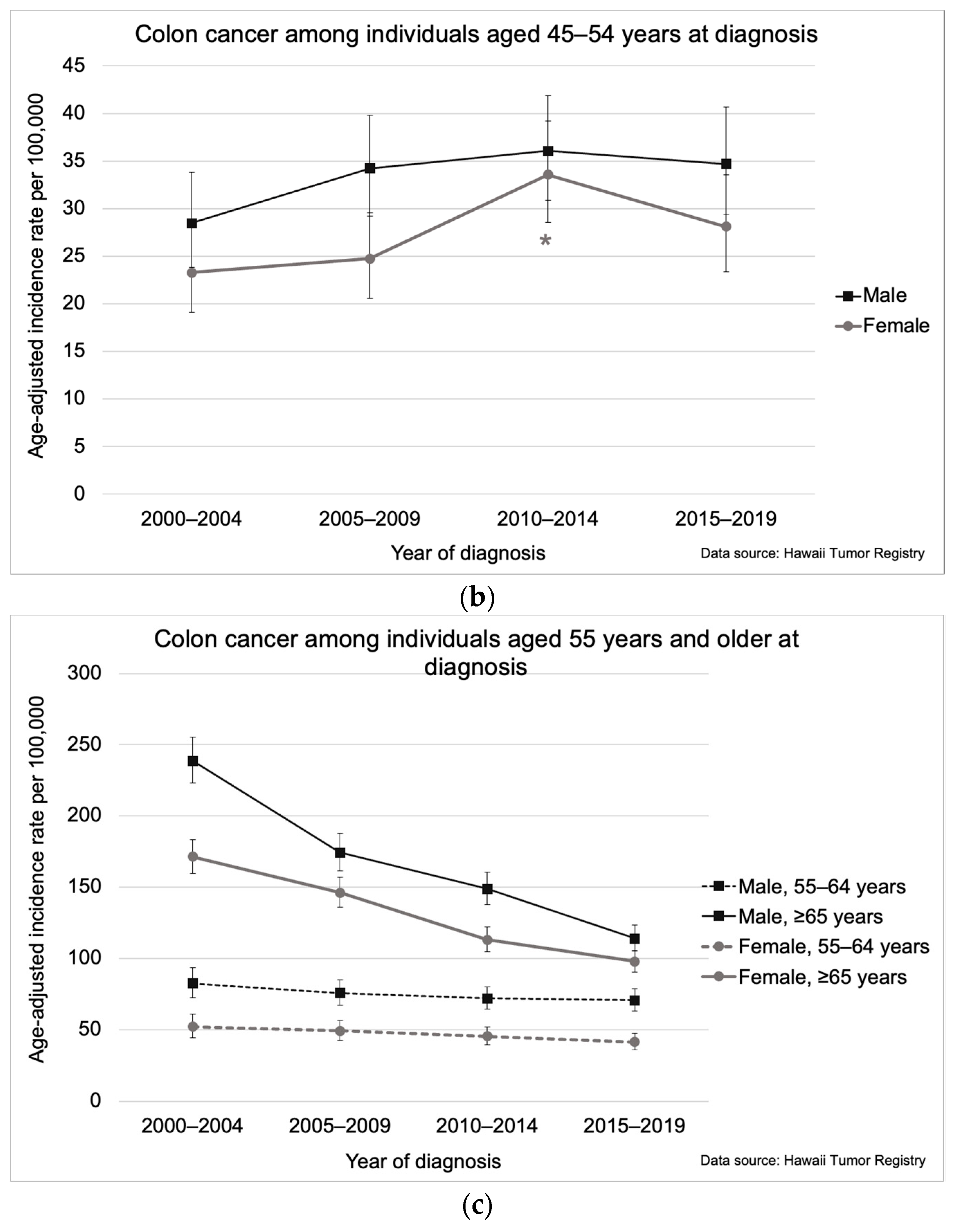
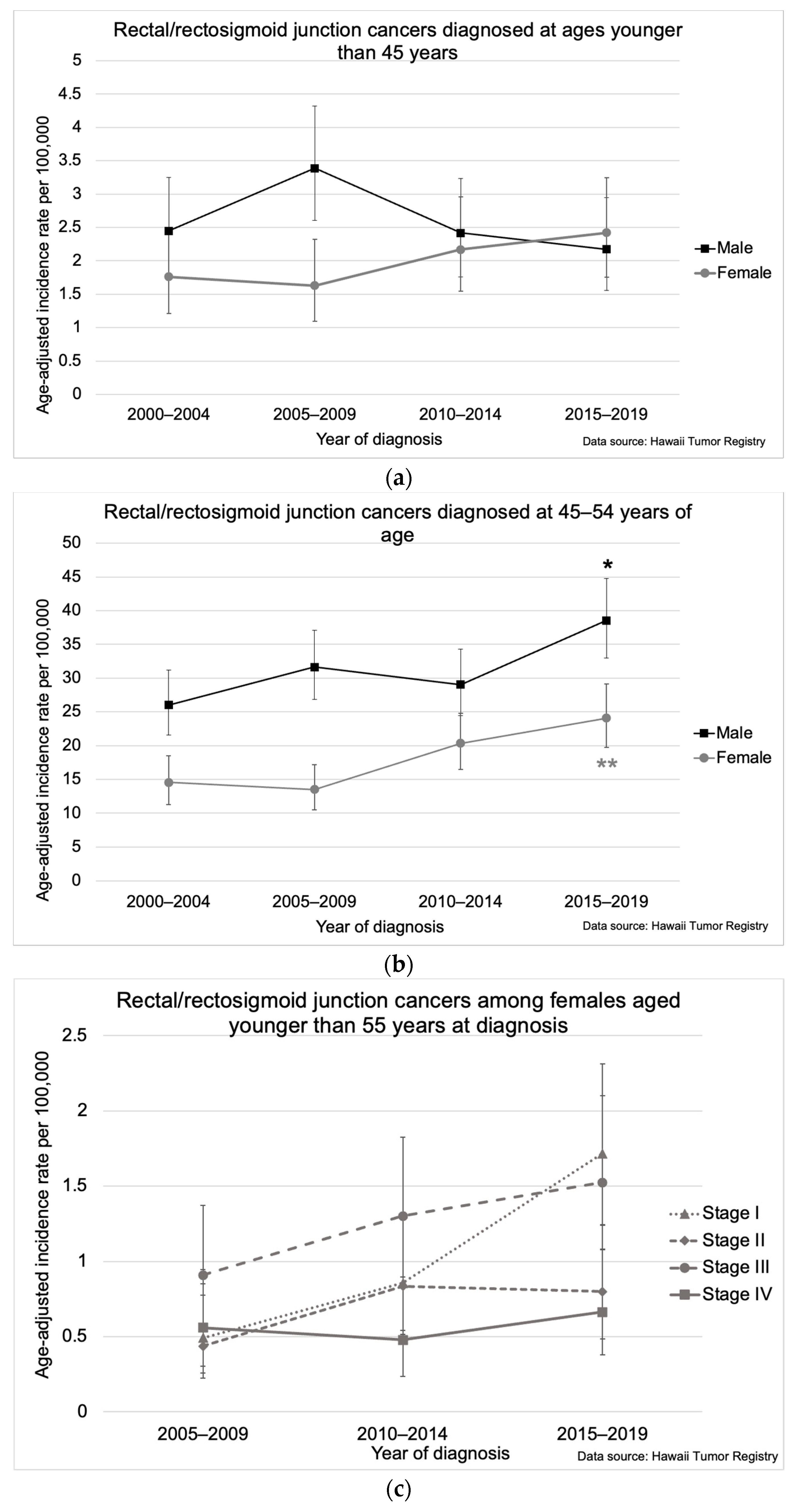
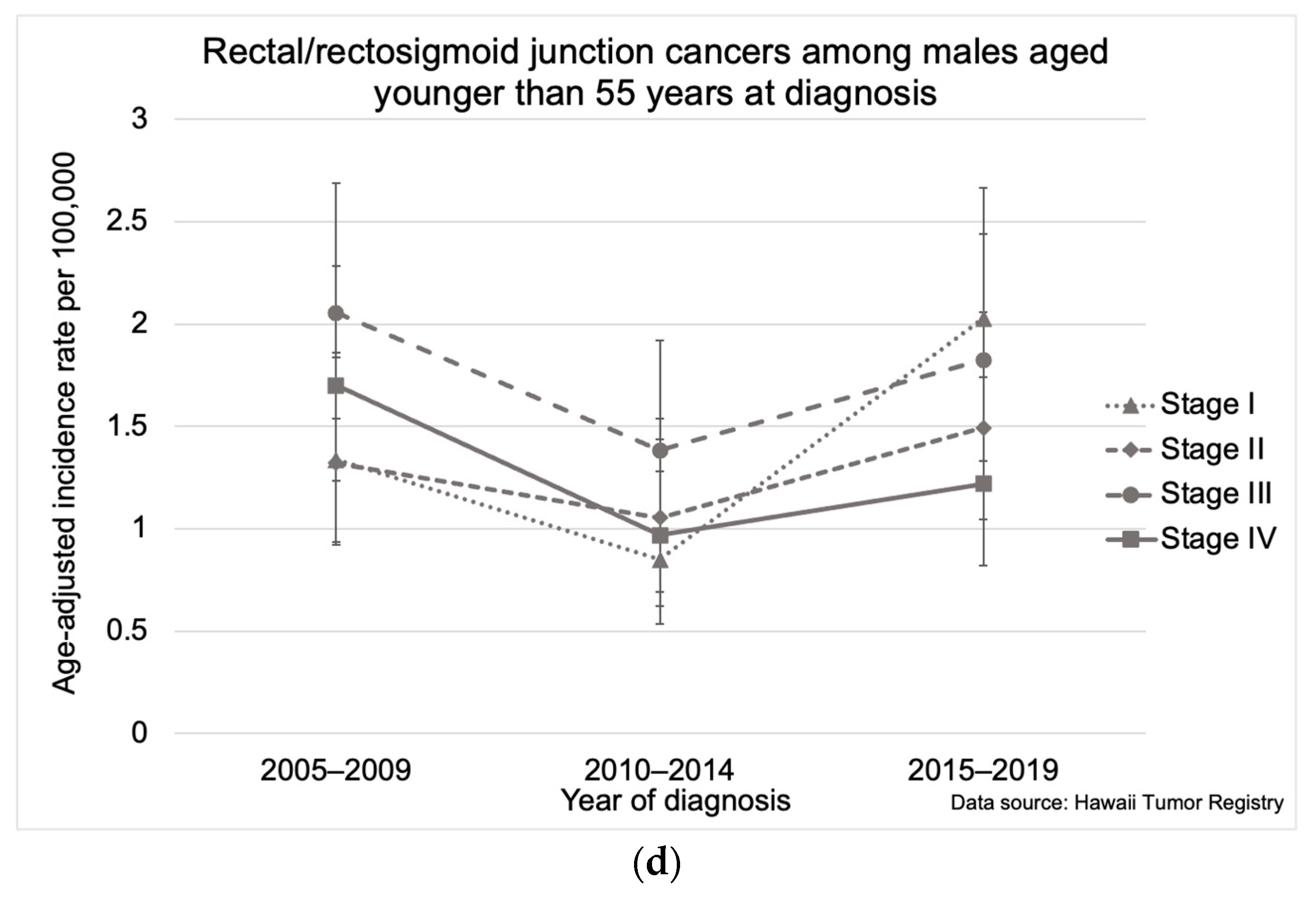
3.2. Colorectal Cancer Trends
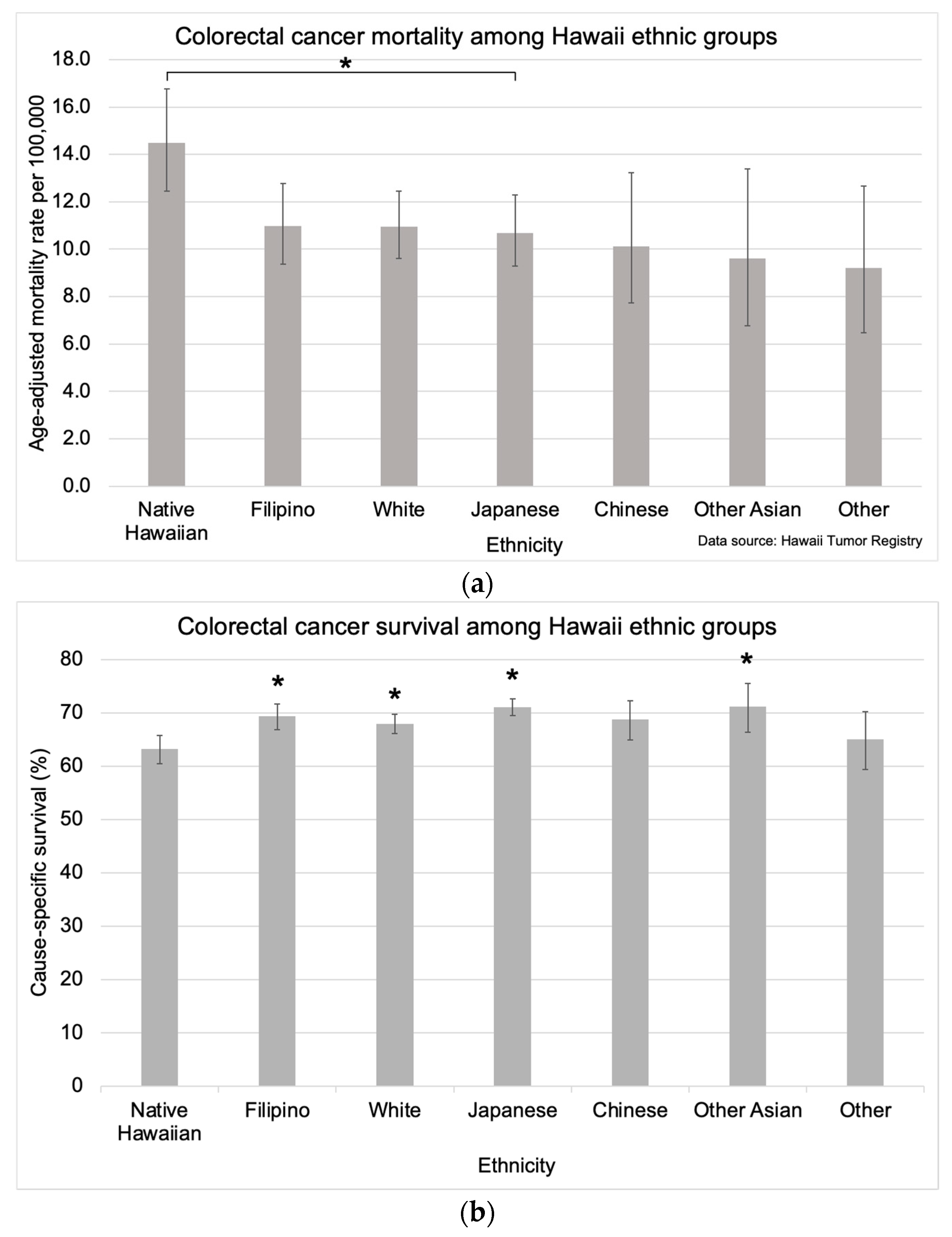
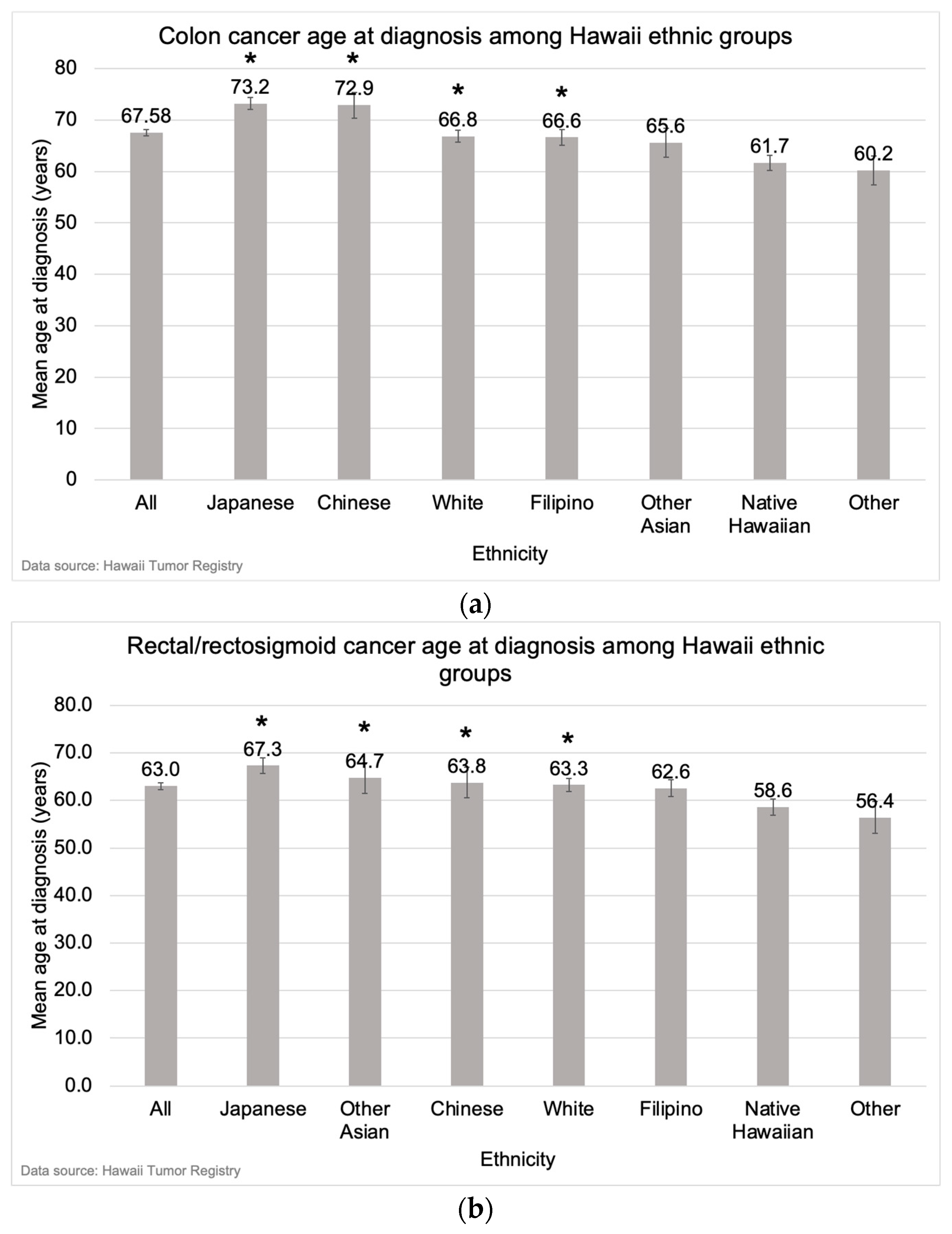
3.3. Ethnic Variation in Colorectal Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, N.; Lu, B.; Luo, C.; Cai, J.; Lu, M.; Zhang, Y.; Chen, H.; Dai, M. Incidence, mortality, survival, risk factor and screening of colorectal cancer: A comparison among China, Europe, and northern America. Cancer Lett. 2021, 522, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A. Increasing Incidence of Early-Onset Colorectal Cancer. N. Engl. J. Med. 2022, 386, 1547–1558. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. Colorectal Cancer. 2020. Available online: https://gco.iarc.fr/today/fact-sheets-cancers (accessed on 1 May 2023).
- Wong, M.C.; Ding, H.; Wang, J.; Chan, P.S.; Huang, J. Prevalence and risk factors of colorectal cancer in Asia. Intest. Res. 2019, 17, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Salvatore, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef]
- Akimoto, N.; Ugai, T.; Zhong, R.; Hamada, T.; Fujiyoshi, K.; Giannakis, M.; Wu, K.; Cao, Y.; Ng, K.; Ogino, S. Rising incidence of early-onset colorectal cancer—A call to action. Nat. Rev. Clin. Oncol. 2021, 18, 230–243. [Google Scholar] [CrossRef]
- O’Sullivan, D.E.; Sutherland, R.L.; Town, S.; Chow, K.; Fan, J.; Forbes, N.; Heitman, S.J.; Hilsden, R.J.; Brenner, D.R. Risk Factors for Early-Onset Colorectal Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1229–1240.e5. [Google Scholar] [CrossRef]
- Gu, J.; Li, Y.; Yu, J.; Hu, M.; Ji, Y.; Li, L.; Hu, C.; Wei, G.; Huo, J. A risk scoring system to predict the individual incidence of early-onset colorectal cancer. BMC Cancer 2022, 22, 122. [Google Scholar] [CrossRef]
- Hua, H.; Jiang, Q.; Sun, P.; Xu, X. Risk factors for early-onset colorectal cancer: Systematic review and meta-analysis. Front. Oncol. 2023, 13, 1132306. [Google Scholar] [CrossRef] [PubMed]
- Gausman, V.; Dornblaser, D.; Anand, S.; Hayes, R.B.; O’Connell, K.; Du, M.; Liang, P.S. Risk Factors Associated With Early-Onset Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 2752–2759.e2. [Google Scholar] [CrossRef]
- Reif de Paula, T.; Haas, E.M.; Keller, D.S. Colorectal cancer in the 45-to-50 age group in the United States: A National Cancer Database (NCDB) analysis. Surg. Endosc. 2022, 36, 6629–6637. [Google Scholar] [CrossRef]
- Muller, C.; Ihionkhan, E.; Stoffel, E.M.; Kupfer, S.S. Disparities in Early-Onset Colorectal Cancer. Cells 2021, 10, 1018. [Google Scholar] [CrossRef]
- Petrick, J.L.; Barber, L.E.; Warren Andersen, S.; Florio, A.A.; Palmer, J.R.; Rosenberg, L. Racial Disparities and Sex Differences in Early- and Late-Onset Colorectal Cancer Incidence, 2001–2018. Front. Oncol. 2021, 11, 734998. [Google Scholar] [CrossRef] [PubMed]
- Ollberding, N.J.; Nomura, A.M.Y.; Wilkens, L.R.; Henderson, B.E.; Kolonel, L.N. Racial/ethnic differences in colorectal cancer risk: The multiethnic cohort study. Int. J. Cancer 2011, 129, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Quick Profile: Hawaii. National Cancer Institute State Cancer Profiles. Available online: https://statecancerprofiles.cancer.gov/quick-profiles/index.php?tabSelected=2&statename=hawaii (accessed on 17 May 2023).
- Park, S.Y.; Wilkens, L.R.; Setiawan, V.W.; Monroe, K.R.; Haiman, C.A.; Le Marchand, L. Alcohol Intake and Colorectal Cancer Risk in the Multiethnic Cohort Study. Am. J. Epidemiol. 2019, 188, 67–76. [Google Scholar] [CrossRef]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Available online: https://seer.cancer.gov/ (accessed on 11 July 2023).
- World Health Organization. International Classification of Diseases for Oncology (ICD-O), 3rd ed.; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/96612 (accessed on 11 July 2023).
- Adamo, M.; Groves, C.; Dickie, L.; Ruhl, J. SEER Program Coding and Staging Manual 2023. Natl. Cancer Inst. 2022. Available online: https://seer.cancer.gov/manuals/2023/SPCSM_2023_MainDoc.pdf (accessed on 26 June 2023).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Statist Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Surveillance, Epidemiology, and End Results Program. U.S. Census Tract Population Data. Available online: https://seer.cancer.gov/censustract-pops/ (accessed on 13 December 2023).
- American Community Survey. Public Use Microdata Sample. Available online: https://www.census.gov/programs-surveys/acs/microdata/access.html (accessed on 18 August 2023).
- Chang, S.H.; Patel, N.; Du, M.; Liang, P.S. Trends in Early-onset vs Late-onset Colorectal Cancer Incidence by Race/Ethnicity in the United States Cancer Statistics Database. Clin. Gastroenterol. Hepatol. 2022, 20, e1365–e1377. [Google Scholar] [CrossRef]
- Lorenzon, L.; Ferri, M.; Pilozzi, E.; Torrisi, M.R.; Ziparo, V.; French, D. Human papillomavirus and colorectal cancer: Evidences and pitfalls of published literature. Int. J. Colorectal. Dis. 2011, 26, 135–142. [Google Scholar] [CrossRef]
- Baandrup, L.; Thomsen, L.T.; Olesen, T.B.; Andersen, K.K.; Norrild, B.; Kjaer, S.K. The prevalence of human papillomavirus in colorectal adenomas and adenocarcinomas: A systematic review and meta-analysis. Eur. J. Cancer. 2014, 50, 1446–1461. [Google Scholar] [CrossRef]
- Damin, D.C.; Ziegelmann, P.K.; Damin, A.P. Human papillomavirus infection and colorectal cancer risk: A meta-analysis. Colorectal Dis. 2013, 15, e420–e428. [Google Scholar] [CrossRef]
- National Cancer Institute. State Cancer Profiles. State Cancer Profiles. Available online: https://statecancerprofiles.cancer.gov/historicaltrend/index.php?0&2115&999&7599&001&057&00&2&0&0&1&0&1&1#results (accessed on 24 November 2023).
- Murphy, N.; Newton, C.C.; Song, M.; Papadimitriou, N.; Hoffmeister, M.; Phipps, A.I.; Harrison, T.A.; Newcomb, P.A.; Aglago, E.K.; Berndt, S.I.; et al. Body mass index and molecular subtypes of colorectal cancer. JNCI J. Natl. Cancer Inst. 2023, 115, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Wele, P.; Wu, X.; Shi, H. Sex-Dependent Differences in Colorectal Cancer: With a Focus on Obesity. Cells 2022, 11, 3688. [Google Scholar] [CrossRef]
- Hawai‘i Health Data Warehouse. Overweight and Obesity. Hawai‘i Health Data Warehouse. Available online: https://hhdw.org/health-topics/obesity-2/ (accessed on 24 November 2023).
- Low, E.E.; Demb, J.; Liu, L.; Earles, A.; Bustamante, R.; Williams, C.D.; Provenzale, D.; Kaltenbach, T.; Gawron, A.J.; Martinez, M.E.; et al. Risk Factors for Early-Onset Colorectal Cancer. Gastroenterology 2020, 159, 492–501.e7. [Google Scholar] [CrossRef] [PubMed]
- Zaki, T.A.; Liang, P.S.; May, F.P.; Murphy, C.C. Racial and Ethnic Disparities in Early-Onset Colorectal Cancer Survival. Clin. Gastroenterol. Hepatol. 2023, 21, 497–506.e3. [Google Scholar] [CrossRef] [PubMed]
- Rahman, R.; Schmaltz, C.; Jackson, C.S.; Simoes, E.J.; Jackson-Thompson, J.; Ibdah, J.A. Increased risk for colorectal cancer under age 50 in racial and ethnic minorities living in the United States. Cancer Med. 2015, 4, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Medina, H.N.; Callahan, K.E.; Morris, C.R.; Thompson, C.A.; Siweya, A.; Pinheiro, P.S. Cancer Mortality Disparities among Asian American and Native Hawaiian/Pacific Islander Populations in California. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 1387–1396. [Google Scholar] [CrossRef]
- Pilozzi, E.; Maresca, C.; Duranti, E.; Giustiniani, M.C.; Catalanotto, C.; Lucarelli, M.; Cogoni, C.; Ferri, M.; Ruco, L.; Zardo, G. Left-Sided Early-Onset vs Late-Onset Colorectal Carcinoma. Am. J. Clin. Pathol. 2015, 143, 374–384. [Google Scholar] [CrossRef]
- Park, K.S.; Hong, Y.K.; Choi, Y.J.; Kang, J.G. Clinicopathologic characteristics of early-onset colorectal cancer. Ann. Coloproctol. 2022, 38, 362–369. [Google Scholar] [CrossRef]
- Siegel, R.L.; Jakubowski, C.D.; Fedewa, S.A.; Davis, A.; Azad, N.S. Colorectal Cancer in the Young: Epidemiology, Prevention, Management. Am. Soc. Clin. Oncol. Educ. Book. 2020, 40, e75–e88. [Google Scholar] [CrossRef]
- Abdelsattar, Z.M.; Wong, S.L.; Regenbogen, S.E.; Jomaa, D.M.; Hardiman, K.M.; Hendren, S. Colorectal cancer outcomes and treatment patterns in patients too young for average-risk screening. Cancer 2016, 122, 929–934. [Google Scholar] [CrossRef]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef]
- He, J.; Stram, D.O.; Kolonel, L.N.; Henderson, B.E.; Le Marchand, L.; Haiman, C.A. The association of diabetes with colorectal cancer risk: The Multiethnic Cohort. Br. J. Cancer 2010, 103, 120–126. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | No. (%) a n = 3524 | Mean (SD) Age at Diagnosis, Years | p-Value b |
|---|---|---|---|
| Age at diagnosis | 66.0 (14.7) | – | |
| <45 | 228 (6.5) | ||
| 45–54 | 560 (15.9) | ||
| 55–64 | 846 (24.0) | ||
| ≥65 | 1890 (53.6) | ||
| Gender | <0.001 | ||
| Male | 1932 (54.8) | 64.6 (13.5) | |
| Female | 1592 (45.2) | 67.7 (15.8) | |
| Ethnicity | <0.001 | ||
| White | 959 (27.5) | 65.6 (14.0) | |
| Japanese | 873 (25.0) | 71.3 (14.5) | |
| Filipino | 570 (16.3) | 65.0 (14.0) | |
| Native Hawaiian | 534 (15.3) | 60.6 (13.3) | |
| Chinese | 221 (6.3) | 69.5 (15.4) | |
| Other Asian | 155 (4.4) | 65.3 (13.2) | |
| Other | 181 (5.2) | 58.9 (15.0) | |
| Cancer stage c | <0.001 | ||
| I | 779 (26.3) | 63.6 (14.4) | |
| II | 705 (23.8) | 68.9 (13.8) | |
| III | 847 (28.6) | 65.5 (14.3) | |
| IV | 629 (21.3) | 65.3 (14.2) | |
| Tumor subsite | <0.001 | ||
| Colon | 2271 (64.4) | 67.6 (15.1) | |
| Rectum/rectosigmoid junction | 1253 (35.6) | 63.0 (13.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagata, M.; Miyagi, K.; Hernandez, B.Y.; Kuwada, S.K. Multiethnic Trends in Early Onset Colorectal Cancer. Cancers 2024, 16, 398. https://doi.org/10.3390/cancers16020398
Nagata M, Miyagi K, Hernandez BY, Kuwada SK. Multiethnic Trends in Early Onset Colorectal Cancer. Cancers. 2024; 16(2):398. https://doi.org/10.3390/cancers16020398
Chicago/Turabian StyleNagata, Michelle, Kohei Miyagi, Brenda Y. Hernandez, and Scott K. Kuwada. 2024. "Multiethnic Trends in Early Onset Colorectal Cancer" Cancers 16, no. 2: 398. https://doi.org/10.3390/cancers16020398
APA StyleNagata, M., Miyagi, K., Hernandez, B. Y., & Kuwada, S. K. (2024). Multiethnic Trends in Early Onset Colorectal Cancer. Cancers, 16(2), 398. https://doi.org/10.3390/cancers16020398