
The 31-Gene Expression Profile Test Outperforms AJCC in Stratifying Risk of Recurrence in Patients with Stage I Cutaneous Melanoma

 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Survival Analysis
2.3. Statistical Analysis
3. Results
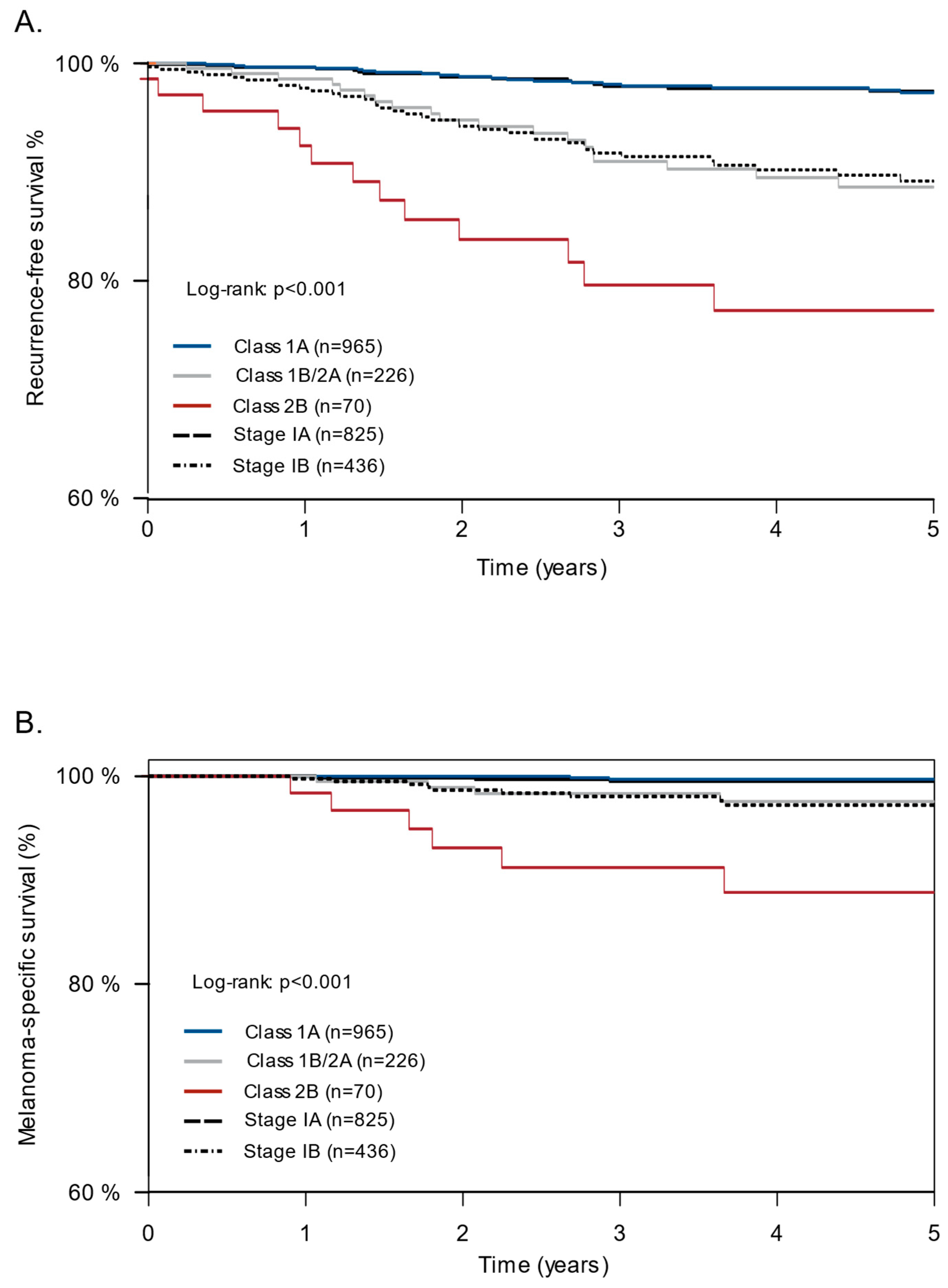
3.1. Survival Analysis in the Combined Cohort
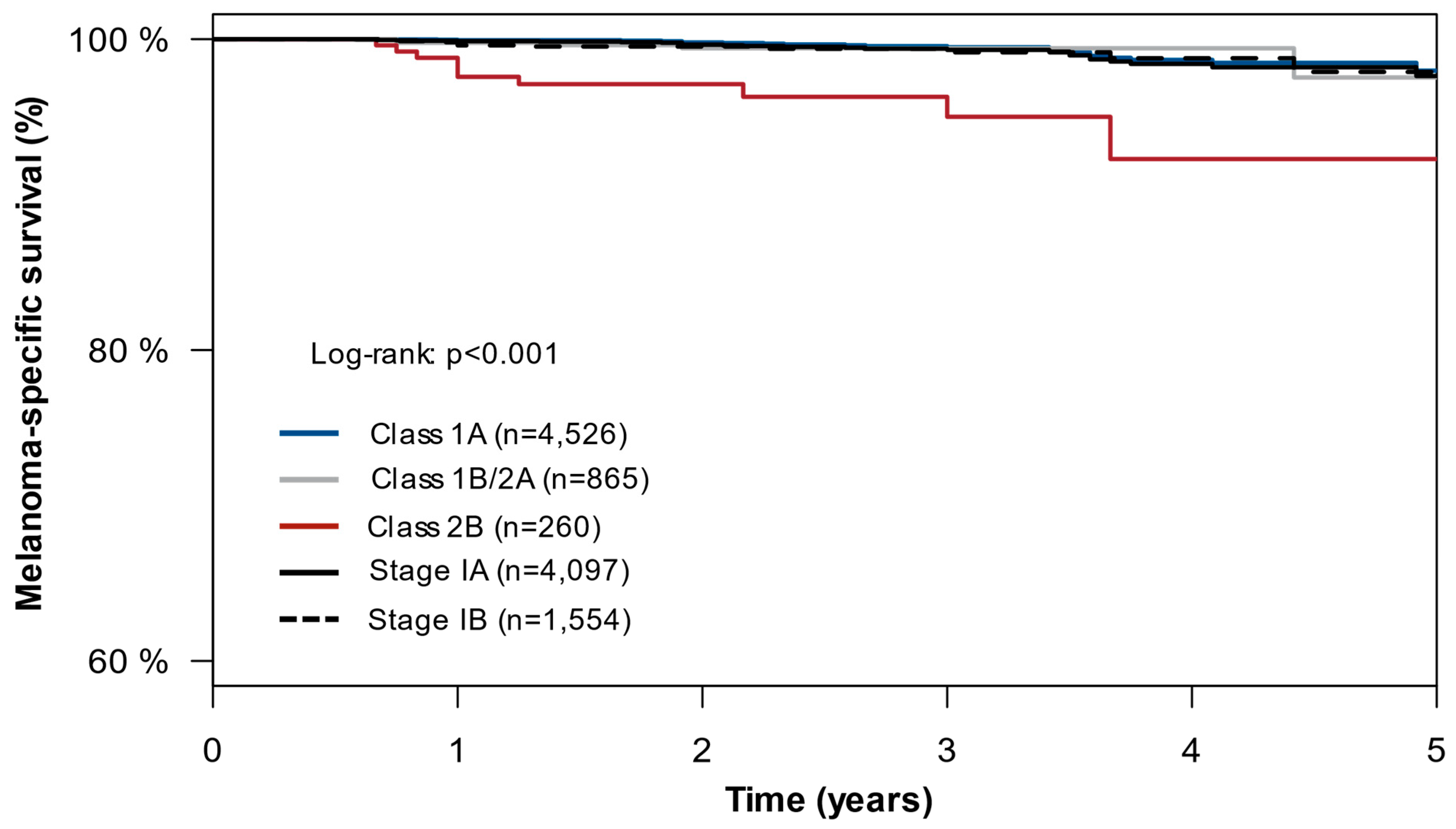
3.2. Survival Analysis in the SEER Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gershenwald, J.E.; Scolyer, R.A. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond. Ann. Surg. Oncol. 2018, 25, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Herbert, A.; Koo, M.M.; Barclay, M.E.; Greenberg, D.C.; Abel, G.A.; Levell, N.J.; Lyratzopoulos, G. Stage-specific incidence trends of melanoma in an English region, 1996–2015: Longitudinal analyses of population-based data. Melanoma Res. 2020, 30, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Kwatra, S.G.; Hines, H.; Semenov, Y.R.; Trotter, S.C.; Holland, E.; Leachman, S. A Dermatologist’s Guide to Implementation of Gene Expression Profiling in the Management of Melanoma. J. Clin. Aesthet. Dermatol. 2020, 13, s3–s14. [Google Scholar] [PubMed]
- Whiteman, D.C.; Baade, P.D.; Olsen, C.M. More people die from thin melanomas (1 mm) than from thick melanomas (>4 mm) in Queensland, Australia. J. Investig. Dermatol. 2015, 135, 1190–1193. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Sakamoto, N.; Yang, L. Melanoma-specific mortality and competing mortality in patients with non-metastatic malignant melanoma: A population-based analysis. BMC Cancer 2016, 16, 413. [Google Scholar] [CrossRef] [PubMed]
- Ertekin, S.; Podlipnik, S.; Loughlin, C.; Barreiro-Capurro, A.; Arance, A.; Carrera, C.; Malvehy, J.; Puig, S. Initial Stage of Cutaneous Primary Melanoma Plays a Key Role in the Pattern and Timing of Disease Recurrence. Acta Derm. Venereol. 2021, 101, adv00502. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, S.; Donnelly, D.; Call, M.; Johannet, P.; Moran, U.; Polsky, D.; Shapiro, R.; Berman, R.; Pavlick, A.; Weber, J.; et al. Melanoma Prognosis: Accuracy of the American Joint Committee on Cancer Staging Manual Eighth Edition. J. Natl. Cancer Inst. 2020, 112, 921–928. [Google Scholar] [CrossRef]
- Garbe, C.; Keim, U.; Amaral, T.; Berking, C.; Eigentler, T.K.; Flatz, L.; Gesierich, A.; Leiter, U.; Stadler, R.; Sunderkötter, C.; et al. Prognosis of Patients With Primary Melanoma Stage I and II According to American Joint Committee on Cancer Version 8 Validated in Two Independent Cohorts: Implications for Adjuvant Treatment. J. Clin. Oncol. 2022, 40, 3741–3749. [Google Scholar] [CrossRef]
- Bach, A.; Knauer, K.; Graf, J.; Schäffeler, N.; Stengel, A. Psychiatric comorbidities in cancer survivors across tumor subtypes: A systematic review. World J. Psychiatry 2022, 12, 623–635. [Google Scholar] [CrossRef]
- Wang, X.; Li, M.; Shi, Q.; Ji, H.; Kong, S.; Zhu, L.; Zhang, H.-M. Fear of Progression, Anxiety, and Depression in Patients With Advanced Melanoma in the COVID-19 and Post-COVID-19 Era. Front. Psychiatry 2022, 13, 880978. [Google Scholar] [CrossRef]
- Wagner, T.; Augustin, M.; Blome, C.; Forschner, A.; Garbe, C.; Gutzmer, R.; Hauschild, A.; Heinzerling, L.; Livingstone, E.; Loquai, C.; et al. Fear of cancer progression in patients with stage IA malignant melanoma. Eur. J. Cancer Care 2018, 27, e12901. [Google Scholar] [CrossRef]
- Ahmed, K.; Siegel, J.J.; Morgan-Linnell, S.K.; LiPira, K. Attitudes of patients with cutaneous melanoma toward prognostic testing using the 31-gene expression profile test. Cancer Med. 2022, 12, 2008–2015. [Google Scholar] [CrossRef] [PubMed]
- Ontario Health (Quality). Gene Expression Profiling Tests for Early-Stage Invasive Breast Cancer: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2020, 20, 1–234. [Google Scholar]
- Gerami, P.; Cook, R.W.; Russell, M.C.; Wilkinson, J.; Amaria, R.N.; Gonzalez, R.; Lyle, S.; Jackson, G.L.; Greisinger, A.J.; Johnson, C.E.; et al. Gene expression profiling for molecular staging of cutaneous melanoma in patients undergoing sentinel lymph node biopsy. J. Am. Acad. Dermatol. 2015, 72, 780–785.e3. [Google Scholar] [CrossRef] [PubMed]
- Gerami, P.; Cook, R.W.; Wilkinson, J.; Russell, M.C.; Dhillon, N.; Amaria, R.N.; Gonzalez, R.; Lyle, S.; Johnson, C.E.; Oelschlager, K.M.; et al. Development of a prognostic genetic signature to predict the metastatic risk associated with cutaneous melanoma. Clin. Cancer Res. 2015, 21, 175–183. [Google Scholar] [CrossRef]
- Zager, J.S.; Gastman, B.R.; Leachman, S.; Gonzalez, R.C.; Fleming, M.D.; Ferris, L.K.; Ho, J.; Miller, A.R.; Cook, R.W.; Covington, K.R.; et al. Performance of a prognostic 31-gene expression profile in an independent cohort of 523 cutaneous melanoma patients. BMC Cancer 2018, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Greenhaw, B.N.; Covington, K.R.; Kurley, S.J.; Yeniay, Y.; Cao, N.A.; Plasseraud, K.M.; Cook, R.W.; Hsueh, E.C.; Gastman, B.R.; Wei, M.L. Molecular risk prediction in cutaneous melanoma: A meta-analysis of the 31-gene expression profile prognostic test in 1,479 patients. J. Am. Acad. Dermatol. 2020, 83, 745–753. [Google Scholar] [CrossRef]
- Gastman, B.R.; Gerami, P.; Kurley, S.J.; Cook, R.W.; Leachman, S.; Vetto, J.T. Identification of patients at risk of metastasis using a prognostic 31-gene expression profile in subpopulations of melanoma patients with favorable outcomes by standard criteria. J. Am. Acad. Dermatol. 2019, 80, 149–157.e4. [Google Scholar] [CrossRef]
- Hsueh, E.C.; DeBloom, J.R.; Lee, J.H.; Sussman, J.J.; Covington, K.R.; Caruso, H.G.; Quick, A.P.; Cook, R.W.; Slingluff, C.L.; McMasters, K.M. Long-Term Outcomes in a Multicenter, Prospective Cohort Evaluating the Prognostic 31-Gene Expression Profile for Cutaneous Melanoma. JCO Precis. Oncol. 2021, 5, 589–601. [Google Scholar] [CrossRef]
- Jarell, A.; Skenderis, B.; Dillon, L.D.; Dillon, K.; Martin, B.; Quick, A.P.; Siegel, J.J.; Rackley, B.B.; Cook, R.W. The 31-gene expression profile stratifies recurrence and metastasis risk in patients with cutaneous melanoma. Future Oncol. 2021, 17, 5023–5031. [Google Scholar] [CrossRef]
- Lawson, D.H.; Cook, R.W.; Johnson, C.; Russell, M.C.; Amaria, R.N.; Wilkinson, J.; Gerami, P.; Maetzold, D.; Ferris, L.; Oelschlager, K.M.; et al. Continued evaluation of a 31-gene expression profile test (GEP) for prediction of distant metastasis (DM) in cutaneous melanoma (CM). J. Clin. Oncol. 2015, 33, 9066. [Google Scholar] [CrossRef]
- Ferris, L.K.; Farberg, A.S.; Middlebrook, B.; Johnson, C.E.; Lassen, N.; Oelschlager, K.M.; Maetzold, D.J.; Cook, R.W.; Rigel, D.S.; Gerami, P. Identification of high-risk cutaneous melanoma tumors is improved when combining the online American Joint Committee on Cancer Individualized Melanoma Patient Outcome Prediction Tool with a 31-gene expression profile-based classification. J. Am. Acad. Dermatol. 2017, 76, 818–825.e3. [Google Scholar] [CrossRef] [PubMed]
- Dillon, L.D.; Gadzia, J.E.; Davidson, R.S.; McPhee, M.; Covington, K.R.; Cook, R.W.; Johnson, C.; Monzon, F.A.; Milanese, E.D.; Vetto, J.; et al. Prospective, Multicenter Clinical Impact Evaluation of a 31-Gene Expression Profile Test for Management of Melanoma Patients. SKIN J. Cutan. Med. 2018, 2, 111–121. [Google Scholar] [CrossRef]
- Greenhaw, B.N.; Zitelli, J.A.; Brodland, D.G. Estimation of Prognosis in Invasive Cutaneous Melanoma: An Independent Study of the Accuracy of a Gene Expression Profile Test. Dermatol. Surg. 2018, 44, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Schwartz, T.L.; Lizalek, J.M.; Chang, E.; Patel, A.D.; Hurley, M.Y.; Hsueh, E.C. Prospective validation of the prognostic 31-gene expression profiling test in primary cutaneous melanoma. Cancer Med. 2019, 8, 2205–2212. [Google Scholar] [CrossRef] [PubMed]
- Podlipnik, S.; Carrera, C.; Boada, A.; Richarz, N.A.; López-Estebaranz, J.L.; Pinedo-Moraleda, F.; Elosua-González, M.; Martín-González, M.M.; Carrillo-Gijón, R.; Redondo, P.; et al. Early outcome of a 31-gene expression profile test in 86 AJCC stage IB-II melanoma patients. A prospective multicentre cohort study. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 857–862. [Google Scholar] [CrossRef]
- Zakria, D.; Brownstone, N.; Rigel, D. The Integrated 31-Gene Expression Profile (i31-GEP) Test for Cutaneous Melanoma Outperforms a Clinicopathologic-only Nomogram at Identifying Patients who can Forego Sentinel Lymph Node Biopsy. J. Ski. 2022, 6, 463–473. [Google Scholar] [CrossRef]
- Wong, S.L.; Kattan, M.W.; McMasters, K.M.; Coit, D.G. A nomogram that predicts the presence of sentinel node metastasis in melanoma with better discrimination than the American Joint Committee on Cancer staging system. Ann. Surg. Oncol. 2005, 12, 282–288. [Google Scholar] [CrossRef]
- Lo, S.N.; Ma, J.; Scolyer, R.A.; Haydu, L.E.; Stretch, J.R.; Saw, R.P.M.; Nieweg, O.E.; Shannon, K.F.; Spillane, A.J.; Ch’ng, S.; et al. Improved Risk Prediction Calculator for Sentinel Node Positivity in Patients With Melanoma: The Melanoma Institute Australia Nomogram. J. Clin. Oncol. 2020, 38, 2719–2727. [Google Scholar] [CrossRef]
- Hosein, S.; Drebin, H.M.; Kurtansky, N.R.; Olofsson Bagge, R.; Coit, D.G.; Bartlett, E.K.; Marchetti, M.A. Are the MIA and MSKCC nomograms useful in selecting patients with melanoma for sentinel lymph node biopsy? J. Surg. Oncol. 2023, 127, 1167–1173. [Google Scholar] [CrossRef]
- Amaral, T.; Sinnberg, T.; Chatziioannou, E.; Niessner, H.; Leiter, U.; Keim, U.; Forschner, A.; Dwarkasing, J.; Tjien-Fooh, F.; Wever, R.; et al. Identification of stage I and II melanoma patients at high risk for recurrence using a model combining clinicopathologic factors with gene expression profiling (CP-GEP). Eur. J. Cancer 2023, 182, 155–162. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology: Melanoma: Cutaneous Version 1; NCCN: Plymouth Meeting, PA, USA, 2023.
- Moody, J.A.; Ali, R.F.; Carbone, A.C.; Singh, S.; Hardwicke, J.T. Complications of sentinel lymph node biopsy for melanoma—A systematic review of the literature. Eur. J. Surg. Oncol. 2017, 43, 270–277. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Descriptor | Class 1A (n = 965) | Class 1B/2A (n = 226) | Class 2B (n = 70) | Combined (n = 1261) |
|---|---|---|---|---|
| Age (years), median (Range) | 60 (13–91) | 63 (19–95) | 67 (25–88) | 61 (13–95) |
| Sex | ||||
| Female | 299 (31.0%) | 52 (23.0%) | 14 (20.0%) | 365 (28.9%) |
| Male | 331 (34.3%) | 71 (31.4%) | 19 (27.1%) | 421 (33.4%) |
| Unknown | 335 (34.7%) | 103 (45.6%) | 37 (52.9%) | 475 (37.7%) |
| Tumor Location | ||||
| Extremity | 453 (46.9%) | 111 (49.1%) | 31 (44.3%) | 595 (47.2%) |
| Head and neck | 192 (19.9%) | 55 (24.3%) | 20 (28.6%) | 267 (21.2%) |
| Trunk | 320 33.2%) | 60 (26.5%) | 19 (27.1%) | 399 (31.6%) |
| Breslow thickness (mm), median (Range) | 0.6 (0.08–2.03) | 1.0 (0.1–2.0) | 1.2 (0.18–2.03) | 0.7 (0.08–2.03) |
| Ulceration | ||||
| No | 883 (91.5%) | 196 (86.7%) | 59 (84.3%) | 1138 (90.2%) |
| Yes | 19 (2.0%) | 11 (4.9%) | 7 (10.0%) | 37 (2.9%) |
| Unknown | 63 (6.5%) | 19 (8.4%) | 4 (5.7%) | 86 (6.8%) |
| Mitotic rate (1/mm2), median (Range) | 0.0 (0.0–10.0) | 1.0 (0.0–10.0) | 1.0 (0.0–10.0) | 0.0 (0.0–10.0) |
| Recurrence | ||||
| No | 940 (97.4%) | 205 (90.7%) | 57 (81.4%) | 1202 (95.3%) |
| Yes | 25 (2.6%) | 21 (9.3%) | 13 (18.6%) | 59 (4.7%) |
| Melanoma-specific death | ||||
| No | 960 (99.5%) | 222 (98.2%) | 64 (91.4%) | 1246 (98.8%) |
| Yes | 5 (0.5%) | 4 (1.8%) | 6 (8.6%) | 15 (1.2%) |
| T-stage | ||||
| T1a | 581 (60.2%) | 56 (24.8%) | 11 (15.7%) | 648 (51.4%) |
| T1b | 206 (21.3%) | 64 (28.3%) | 16 (22.9%) | 286 (22.7%) |
| T2a | 178 (18.4%) | 106 (46.9%) | 43 (61.4%) | 327 (25.9%) |
| AJCC 8th edition * | ||||
| Stage IA | 713 (73.9%) | 92 (40.7%) | 20 (28.6%) | 825 (65.4%) |
| Stage IB | 252 (26.1%) | 134 (59.3%) | 50 (71.4%) | 436 (34.6%) |
| Factor | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| RFS-Combined cohort | ||
| 31-GEP | ||
| Class 1A | Reference | -- |
| Class 1B/2A | 2.63 (1.43–4.83) | 0.002 |
| Class 2B | 5.16 (2.54–10.47) | <0.001 |
| AJCC | ||
| Stage IA | Reference | -- |
| Stage IB | 2.98 (1.64–5.40) | <0.001 |
| MSS-Combined cohort | ||
| 31-GEP | ||
| Class 1A | Reference | -- |
| Class 1B/2A | 2.35 (0.60–9.29) | 0.223 |
| Class 2B | 11.08 (3.10–39.63) | <0.001 |
| AJCC | ||
| Stage IA | Reference | -- |
| Stage IB | 3.00 (0.87–10.37) | 0.082 |
| MSS-SEER cohort | ||
| 31-GEP | ||
| Class 1A | Reference | -- |
| Class 1B/2A | 1.37 (0.50–3.71) | 0.542 |
| Class 2B | 9.23 (4.23–20.18) | <0.001 |
| AJCC | ||
| Stage IA | Reference | -- |
| Stage IB | 0.82 (0.39–1.74) | 0.609 |
| Group | Likelihood Ratio | p-Value |
|---|---|---|
| RFS-Combined cohort | ||
| 31-GEP (Combined) | 39.11 | p < 0.001 |
| AJCC (Combined) | 32.05 | p < 0.001 |
| 31-GEP added to AJCC (Combined) | 52.99 | p < 0.001 |
| MSS-Combined cohort | ||
| 31-GEP (Combined) | 19.29 | p < 0.001 |
| AJCC (Combined) | 9.95 | p = 0.002 |
| 31-GEP added to AJCC (Combined) | 22.64 | p < 0.001 |
| MSS-SEER cohort | ||
| 31-GEP (SEER) | 22.52 | p < 0.001 |
| AJCC (SEER) | 0.20 | p = 0.653 |
| 31-GEP added to AJCC (SEER) | 22.79 | p < 0.001 |
| Descriptor | Class 1A (n = 4526) | Class 1B/2A (n = 865) | Class 2B (n = 260) | Combined (n = 5651) |
|---|---|---|---|---|
| Age (years), median (Range) | 60 (18–90+) | 64 (18–90+) | 65 (22–90+) | 61 (18–90+) |
| Sex | ||||
| Female | 2089 (46.2%) | 383 (44.3%) | 96 (36.9%) | 2568 (45.4%) |
| Male | 2437 (53.8%) | 482 (55.7%) | 164 (63.1%) | 3083 (54.6%) |
| Tumor Location | ||||
| Extremity | 2054 (45.3%) | 430 (49.7%) | 141 (54.2%) | 2625 (46.5%) |
| Head and neck | 799 (17.6%) | 209 (24.2%) | 59 (22.7%) | 1067 (18.9%) |
| Trunk | 1648 (36.3%) | 222 (25.7%) | 60 (23.1%) | 1930 (34.2%) |
| Not specified | 25 (0.6%) | 4 (0.5%) | 0 (0.0%) | 29 (0.5%) |
| Breslow thickness (mm), median (Range) | 0.6 (0–2.0) | 1.1 (0.1–2.0) | 1.1 (0.1–2.0) | 0.7 (0–2.0) |
| Ulceration | ||||
| No | 3745 (82.7%) | 667 (77.1%) | 168 (64.6%) | 4580 (81.0%) |
| Yes | 92 (2.0%) | 39 (4.5%) | 30 (11.5%) | 161 (2.8%) |
| Unknown | 689 (15.2%) | 159 (18.4%) | 62 (23.8%) | 910 (16.1%) |
| Mitotic rate (1/mm2), median (Range) | 0 (0–11) | 1 (0–11) | 1 (0–11) | 0 (0–11) |
| Melanoma-specific death | ||||
| No | 4504 (99.5%) | 860 (99.4%) | 250 (96.2%) | 5614 (99.3%) |
| Yes | 22 (0.5%) | 5 (0.6%) | 10 (3.8%) | 37 (0.7%) |
| T-stage | ||||
| T1a | 2850 (63.0%) | 199 (23.0%) | 71 (27.3%) | 3120 (55.2%) |
| T1b | 936 (20.7%) | 216 (25.0%) | 52 (20.0%) | 1204 (21.3%) |
| T2a | 740 (16.3%) | 450 (52.0%) | 137 (52.7%) | 1327 (23.5%) |
| AJCC 8th edition * | ||||
| Stage IA | 3606 (79.7%) | 375 (43.4%) | 116 (44.6%) | 4097 (72.5%) |
| Stage IB | 920 (20.3%) | 490 (56.6%) | 144 (55.4%) | 1554 (27.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podlipnik, S.; Martin, B.J.; Morgan-Linnell, S.K.; Bailey, C.N.; Siegel, J.J.; Petkov, V.I.; Puig, S. The 31-Gene Expression Profile Test Outperforms AJCC in Stratifying Risk of Recurrence in Patients with Stage I Cutaneous Melanoma. Cancers 2024, 16, 287. https://doi.org/10.3390/cancers16020287
Podlipnik S, Martin BJ, Morgan-Linnell SK, Bailey CN, Siegel JJ, Petkov VI, Puig S. The 31-Gene Expression Profile Test Outperforms AJCC in Stratifying Risk of Recurrence in Patients with Stage I Cutaneous Melanoma. Cancers. 2024; 16(2):287. https://doi.org/10.3390/cancers16020287
Chicago/Turabian StylePodlipnik, Sebastian, Brian J. Martin, Sonia K. Morgan-Linnell, Christine N. Bailey, Jennifer J. Siegel, Valentina I. Petkov, and Susana Puig. 2024. "The 31-Gene Expression Profile Test Outperforms AJCC in Stratifying Risk of Recurrence in Patients with Stage I Cutaneous Melanoma" Cancers 16, no. 2: 287. https://doi.org/10.3390/cancers16020287
APA StylePodlipnik, S., Martin, B. J., Morgan-Linnell, S. K., Bailey, C. N., Siegel, J. J., Petkov, V. I., & Puig, S. (2024). The 31-Gene Expression Profile Test Outperforms AJCC in Stratifying Risk of Recurrence in Patients with Stage I Cutaneous Melanoma. Cancers, 16(2), 287. https://doi.org/10.3390/cancers16020287