

Cisplatin-Containing Combinations Associate with Survival in Women from Appalachian Kentucky with Metastatic, Persistent, or Recurrent Uterine Cervix Cancer


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
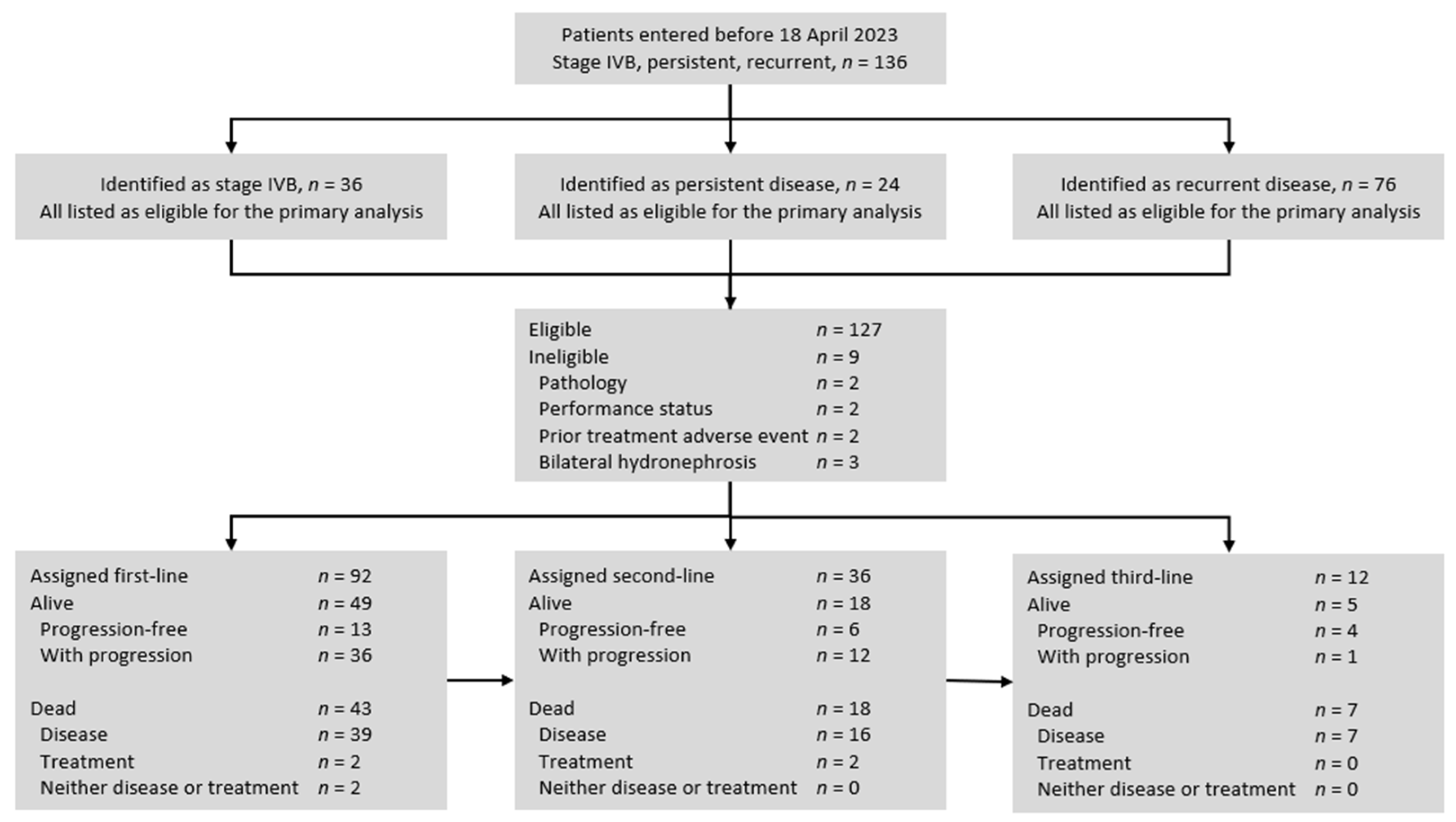
2.1. Study Population
2.2. Treatments
2.3. Assessments
2.4. Endpoints
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Progression-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2023; American Cancer Society: Atlanta, GA, USA, 2023. [Google Scholar]
- Rose, P.G.; Bundy, B.N.; Watkins, E.B.; Thigpen, J.T.; Deppe, G.; Maiman, M.A.; Clarke-Pearson, D.L.; Insalaco, S. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N. Engl. J. Med. 1999, 340, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef]
- Keys, H.M.; Bundy, B.N.; Stehman, F.B.; Muderspach, L.I.; Chafe, W.E.; Suggs, C.L., 3rd; Walker, J.L.; Gersell, D. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N. Engl. J. Med. 1999, 340, 1154–1161, Erratum in N. Engl. J. Med. 1999, 341, 708.. [Google Scholar] [CrossRef] [PubMed]
- Bonomi, P.; Blessing, J.A.; Stehman, F.B.; DiSaia, P.J.; Walton, L.; Major, F.J. Randomized trial of three cisplatin dose schedules in squamous-cell carcinoma of the cervix: A Gynecologic Oncology Group study. J. Clin. Oncol. 1985, 3, 1079–1085. [Google Scholar] [CrossRef]
- Monk, B.J.; Sill, M.W.; McMeekin, D.S.; Cohn, D.E.; Ramondetta, L.M.; Boardman, C.H.; Benda, J.; Cella, D. Phase III trial of four cisplatin-containing doublet combinations in stage IVB, recurrent, or persistent cervical carcinoma: A Gynecologic Oncology Group study. J. Clin. Oncol. 2009, 27, 4649–4655. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.H.; Blessing, J.A.; McQuellon, R.P.; Thaler, H.T.; Cella, D.; Benda, J.; Miller, D.S.; Olt, G.; King, S.; Boggess, J.F.; et al. Phase III study of cisplatin with or without paclitaxel in stage IVB, recurrent, or persistent squamous cell carcinoma of the cervix: A gynecologic oncology group study. J. Clin. Oncol. 2004, 22, 3113–3119. [Google Scholar] [CrossRef]
- Long, H.J., 3rd; Bundy, B.N.; Grendys ECJr Benda, J.A.; McMeekin, D.S.; Sorosky, J.; Miller, D.S.; Eaton, L.A.; Fiorica, J.V.; Gynecologic Oncology Group Study. Randomized phase III trial of cisplatin with or without topotecan in carcinoma of the uterine cervix: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2005, 23, 4626–4633. [Google Scholar] [CrossRef]
- Monk, B.J.; Sill, M.W.; Burger, R.A.; Gray, H.J.; Buekers, T.E.; Roman, L.D. Phase II trial of bevacizumab in the treatment of persistent or recurrent squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. J. Clin. Oncol. 2009, 27, 1069–1074. [Google Scholar] [CrossRef]
- Tewari, K.S.; Sill, M.W.; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; Michael, H.E.; et al. Bevacizumab for advanced cervical cancer: Final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240). Lancet 2017, 390, 1654–1663. [Google Scholar] [CrossRef]
- Colombo, N.; Dubot, C.; Lorusso, D.; Caceres, M.V.; Hasegawa, K.; Shapira-Frommer, R.; Tewari, K.S.; Salman, P.; Hoyos Usta, E.; Yañez, E.; et al. Pembrolizumab for Persistent, Recurrent, or Metastatic Cervical Cancer. N. Engl. J. Med. 2021, 385, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.C.; Ros, W.; Delord, J.P.; Perets, R.; Italiano, A.; Shapira-Frommer, R.; Manzuk, L.; Piha-Paul, S.A.; Xu, L.; Zeigenfuss, S.; et al. Efficacy and Safety of Pembrolizumab in Previously Treated Advanced Cervical Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2019, 37, 1470–1478. [Google Scholar] [CrossRef]
- Penson, R.T.; Huang, H.Q.; Wenzel, L.B.; Monk, B.J.; Stockman, S.; Long, H.J., 3rd; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; et al. Bevacizumab for advanced cervical cancer: Patient-reported outcomes of a randomised, phase 3 trial (NRG Oncology-Gynecologic Oncology Group protocol 240). Lancet Oncol. 2015, 16, 301–311. [Google Scholar] [CrossRef]
- Monk, B.J.; Tewari, K.S.; Dubot, C.; Caceres, M.V.; Hasegawa, K.; Shapira-Frommer, R.; Salman, P.; Yañez, E.; Gümüş, M.; Hurtado de Mendoza, M.O.; et al. Health-related quality of life with pembrolizumab or placebo plus chemotherapy with or without bevacizumab for persistent, recurrent, or metastatic cervical cancer (KEYNOTE-826): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2023, 24, 392–402. [Google Scholar] [CrossRef]
- Kunos, C.A. Novel Radiosensitization Strategies in Uterine Cervix Cancer. Semin. Radiat. Oncol. 2020, 30, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Kunos, C.A.; Fabian, D.; Piecoro, D.W.; Napier, D.; Miller, R.W.; Ueland, F.R. Human epidermal growth factor receptor 2 expression in women with uterine cervix adenocarcinoma from Appalachian Kentucky. Front. Oncol. 2023, 13, 948348. [Google Scholar] [CrossRef]
- Kunos, C.A.; Fabian, D.; Napier, D.; Stonecypher, M.S.; Duncan, R.M.; Hurt, J. Human gastrin-releasing peptide receptor expression in women with uterine cervix cancer. Front. Oncol. 2023, 13, 1126426. [Google Scholar] [CrossRef] [PubMed]
- Kunos, C.A.; Fabian, D.; Kudrimoti, M.; Miller, R.W.; Ueland, F.R.; Randall, M.E. Characterization of Uterine Cervix Cancers in Women from Appalachian Kentucky. Front. Oncol. 2021, 11, 808081. [Google Scholar] [CrossRef]
- Dodd, L.E.; Korn, E.L.; Freidlin, B.; Jaffe, C.C.; Rubinstein, L.V.; Dancey, J.; Mooney, M.M. Blinded independent central review of progression-free survival in phase III clinical trials: Important design element or unnecessary expense? J. Clin. Oncol. 2008, 26, 3791–3796. [Google Scholar] [CrossRef]
- Tewari, K.S.; Monk, B.J.; Vergote, I.; Miller, A.; de Melo, A.C.; Kim, H.S.; Kim, Y.M.; Lisyanskaya, A.; Samouëlian, V.; Lorusso, D. Survival with Cemiplimab in Recurrent Cervical Cancer. N. Engl. J. Med. 2022, 386, 544–555. [Google Scholar] [CrossRef]
- Oaknin, A.; Monk, B.J.; Vergote, I.; Cristina de Melo, A.; Kim, Y.M.; Lisyanskaya, A.S.; Samouëlian, V.; Kim, H.S.; Gotovkin, E.A.; Damian, F.; et al. EMPOWER CERVICAL-1: Effects of cemiplimab versus chemotherapy on patient-reported quality of life, functioning and symptoms among women with recurrent cervical cancer. Eur. J. Cancer 2022, 174, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Lorusso, D.; Gennigens, C.; González-Martín, A.; Randall, L.; Cibula, D.; Lund, B.; Woelber, L.; Pignata, S.; Forget, F.; et al. Efficacy and safety of tisotumab vedotin in previously treated recurrent or metastatic cervical cancer (innovaTV 204/GOG-3023/ENGOT-cx6): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2021, 22, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.Y.; Banerjee, S.; González-Martín, A.; Jung, K.H.; Ługowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J. Clin. Oncol. 2024, 42, 47–58. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peters, W.A., 3rd; Liu, P.Y.; Barrett, R.J., 2nd; Stock, R.J.; Monk, B.J.; Berek, J.S.; Souhami, L.; Grigsby, P.; Gordon, W., Jr.; Alberts, D.S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J. Clin. Oncol. 2000, 18, 1606–1613. [Google Scholar] [CrossRef]
- Whitney, C.W.; Sause, W.; Bundy, B.N.; Malfetano, J.H.; Hannigan, E.V.; Fowler WCJr Clarke-Pearson, D.L.; Liao, S.Y. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: A Gynecologic Oncology Group and Southwest Oncology Group study. J. Clin. Oncol. 1999, 17, 1339–1348. [Google Scholar] [CrossRef]
- Thomas, G.M. Improved treatment for cervical cancer--concurrent chemotherapy and radiotherapy. N. Engl. J. Med. 1999, 340, 1198–1200. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Number | Mean ± SD | % |
|---|---|---|---|
| Age, years | 127 | 53 ± 13 | 100 |
| Residence in Appalachian Kentucky | 77 | 61 | |
| Race | |||
| White | 119 | 94 | |
| Black or African American | 7 | 5 | |
| Asian/Pacific | 1 | 1 | |
| Ethnicity | |||
| Hispanic | 5 | 4 | |
| Non-Hispanic | 122 | 96 | |
| Performance status | |||
| 0 | 77 | 61 | |
| 1 | 32 | 25 | |
| 2 | 18 | 14 | |
| Cell Type | |||
| Squamous | 91 | 72 | |
| Adenosquamous | 10 | 8 | |
| Adenocarcinoma | 26 | 20 | |
| Tumor Grade | |||
| 1 | 2 | 2 | |
| 2 | 32 | 25 | |
| 3 | 93 | 73 | |
| Primary tumor size, centimeters | 6.0 ± 1.4 | ||
| <6 cm | 54 | 43 | |
| ≥6 cm | 73 | 57 | |
| Pelvic nodal metastasis at diagnosis | 84 | 66 | |
| Para-aortic nodal metastasis at diagnosis | 50 | 39 | |
| Prior primary cisplatin and radiation | 120 | 94 | |
| Duration of primary radiochemotherapy, days | 56 ± 19 | ||
| <60 | 65 | 54 | |
| ≥60 | 55 | 46 | |
| Uncorrected creatinine pretherapy, mg dL−1 | |||
| ≥2.0 | 11 | 9 | |
| 1.5–2.0 | 6 | 4 | |
| <1.5 | 110 | 87 |
| Treatment Line, n (%) * | |||
|---|---|---|---|
| Regimen | First (n = 92) | Second (n = 36) | Third (n = 12) |
| Cis + Pac + Bev + Pem | 4 (4) | 0 (0) | 0 (0) |
| Cis + Pac + Bev | 36 (39) | 4 (11) | 1 (8) |
| Cis + Pac | 13 (14) | 0 (0) | 0 (0) |
| Carbo + Pac | 10 (11) | 3 (8) | 0 (0) |
| Another doublet | 3 (3) | 2 (6) | 2 (16) |
| Pem | 3 (3) | 7 (19) | 3 (25) |
| Bev | 0 (0) | 2 (6) | 0 (0) |
| Other singlet | 0 (0) | 4 (11) | 1 (8) |
| Radiotherapy | 9 (10) | 6 (17) | 5 (42) |
| Surgery | 14 (15) | 8 (22) | 0 (0) |
| Trial (Reference) | Year Started | Stage | Histology | Number | Treatment | Response Rate (%) | Progression-Free Survival (Months) |
|---|---|---|---|---|---|---|---|
| KEYNOTE-826 [13] | 2018 | IVB, R, P | SQ, AS, A | 308 | Cis + Pac + Bev + Pem | 68 | 10.4 (95% CI: 9.7–12.3) |
| KEYNOTE-158 [14] | 2016 | IVB, R, P | SQ, AS, A | 98 | Pem | 12 | 2.1 (95% CI: 2.0–2.2) |
| GOG-0240 [12] | 2009 | IVB, R, P | SQ, AS, A, O | 115 | Cis + Pac + Bev | 50 | 8.2 (95% CI: NR) |
| GOG-227C [11] | 2002 | R, P | SQ, AS | 46 | BEV | 11 | 3.4 (95% CI: 2.5–4.5) |
| GOG-0169 [9] | 1997 | IVB, R, P | SQ | 129 | Cis + Pac | 36 | 4.8 (95% CI: NR) |
| GOG-0204 [8] | 2003 | IVB, R, P | SQ, AS, A | 103 | Cis + Pac | 29 | 5.8 (95% CI: 4.5–7.6) |
| 108 | Cis + Vin | 26 | 3.9 (95% CI: 3.2–5.2) | ||||
| 112 | Cis + Gem | 22 | 4.7 (95% CI: 3.6–5.6) | ||||
| 111 | Cis + Topo | 23 | 4.6 (95% CI: 3.7–5.8) | ||||
| GOG-0179 [10] | 1999 | IVB, R, P | SQ, AS, A, O | 147 | Cis + Topo | 27 | 4.6 (95% CI: NR) |
| GOG-0049 [7] | 1978 | IVB, R, P | SQ | 150 | Cis 50 | 21 | 3.7 (95% CI: NR) |
| 166 | Cis 100 | 31 | 4.6 (95% CI: NR) | ||||
| 128 | Cis 20 × 5 | 25 | 3.9 (95% CI: NR) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunos, C.A.; Miller, R.W.; Fabian, D. Cisplatin-Containing Combinations Associate with Survival in Women from Appalachian Kentucky with Metastatic, Persistent, or Recurrent Uterine Cervix Cancer. Cancers 2024, 16, 3319. https://doi.org/10.3390/cancers16193319
Kunos CA, Miller RW, Fabian D. Cisplatin-Containing Combinations Associate with Survival in Women from Appalachian Kentucky with Metastatic, Persistent, or Recurrent Uterine Cervix Cancer. Cancers. 2024; 16(19):3319. https://doi.org/10.3390/cancers16193319
Chicago/Turabian StyleKunos, Charles A., Rachel W. Miller, and Denise Fabian. 2024. "Cisplatin-Containing Combinations Associate with Survival in Women from Appalachian Kentucky with Metastatic, Persistent, or Recurrent Uterine Cervix Cancer" Cancers 16, no. 19: 3319. https://doi.org/10.3390/cancers16193319
APA StyleKunos, C. A., Miller, R. W., & Fabian, D. (2024). Cisplatin-Containing Combinations Associate with Survival in Women from Appalachian Kentucky with Metastatic, Persistent, or Recurrent Uterine Cervix Cancer. Cancers, 16(19), 3319. https://doi.org/10.3390/cancers16193319