
Impact of Cryopreserved Placental Allografts on Biochemical Recurrence in Prostate Cancer

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definitions
2.3. Inclusion/Exclusion Criteria
2.4. Study End Points:
2.5. Prostate Cancer Cell Lines
2.6. Cell Proliferation Assay
2.7. Statistical Analysis—Clinical Data
2.8. Statistical Analysis—Cell Culture Data
3. Results
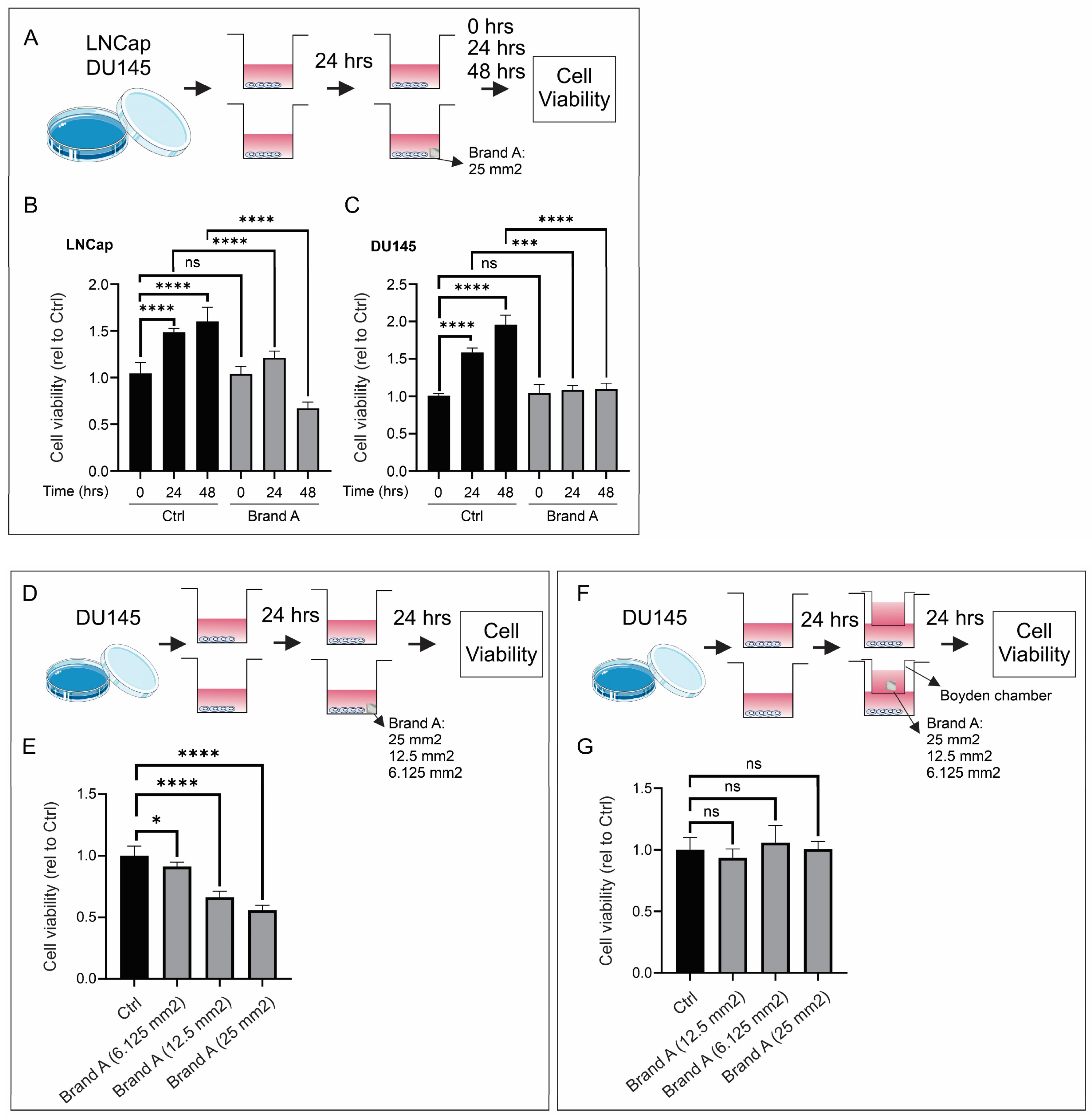
In Vitro Prostate Cancer Cell Growth Assay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International WCRF. Prostate Cancer Statistics. 2020. Available online: https://www.wcrf.org/cancer-trends/prostate-cancer-statistics/ (accessed on 14 March 2024).
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Metcalfe, C.; Davis, M.; Turner, E.L.; Martin, R.M.; Young, G.J.; Walsh, E.I.; Bryant, R.J.; et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N. Engl. J. Med. 2023, 388, 1547–1558. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Yang, Z.; Qi, L.; Chen, M. Robot-assisted and laparoscopic vs. open radical prostatectomy in clinically localized prostate cancer: Perioperative, functional, and oncological outcomes: A Systematic review and meta-analysis. Medicine 2019, 98, e15770. [Google Scholar] [CrossRef]
- Moschovas, M.C.; Brady, I.; Noel, J.; Zeinab, M.A.; Kaviani, A.; Kaouk, J.; Crivellaro, S.; Joseph, J.; Mottrie, A.; Patel, V. Contemporary techniques of da Vinci SP radical prostatectomy: Multicentric collaboration and expert opinion. Int. Braz. J. Urol. 2022, 48, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.R.; Samavedi, S.; Bates, A.S.; Kumar, A.; Coelho, R.; Rocco, B.; Palmer, K. Dehydrated Human Amnion/Chorion Membrane Allograft Nerve Wrap Around the Prostatic Neurovascular Bundle Accelerates Early Return to Continence and Potency Following Robot-assisted Radical Prostatectomy: Propensity Score-matched Analysis. Eur. Urol. 2015, 67, 977–980. [Google Scholar] [CrossRef]
- Koizumi, N.J.; Inatomi, T.J.; Sotozono, C.J.; Fullwood, N.J.; Quantock, A.J.; Kinoshita, S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr. Eye Res. 2000, 20, 173–177. [Google Scholar] [CrossRef]
- Tseng, S.C. Amniotic membrane transplantation for ocular surface reconstruction. Biosci. Rep. 2001, 21, 481–489. [Google Scholar] [CrossRef]
- Zhu, Y.T.; Li, F.; Zhang, Y.; Chen, S.Y.; Tighe, S.; Lin, S.Y.; Tseng, S.C.G. HC-HA/PTX3 Purified From Human Amniotic Membrane Reverts Human Corneal Fibroblasts and Myofibroblasts to Keratocytes by Activating BMP Signaling. Investig. Ophthalmol. Vis. Sci. 2020, 61, 62. [Google Scholar] [CrossRef]
- Gao, M.; Zhao, H.; Tian, D.; Yu, K.; Bai, J.; Dong, R.; Zhang, G. [Experimental study on human amniotic membrane for repairing tendon sheath defect]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2013, 27, 335–339. [Google Scholar] [PubMed]
- Snyder, R.J.; Shimozaki, K.; Tallis, A.; Kerzner, M.; Reyzelman, A.; Lintzeris, D.; Bell, D.; Rutan, R.L.; Rosenblum, B. A Prospective, Randomized, Multicenter, Controlled Evaluation of the Use of Dehydrated Amniotic Membrane Allograft Compared to Standard of Care for the Closure of Chronic Diabetic Foot Ulcer. Wounds 2016, 28, 70–77. [Google Scholar]
- Pacaccio, D.J.; Cazzell, S.M.; Halperin, G.J.; Kasper, M.A.; Neutel, J.M.; O’Carroll, B.D.; Reyzelman, A.M. Human placental membrane as a wound cover for chronic diabetic foot ulcers: A prospective, postmarket, CLOSURE study. J. Wound Care 2018, 27 (Suppl. 7), S28–S37. [Google Scholar] [CrossRef]
- Singh, R.; Purohit, S.; Chacharkar, M.P.; Bhandari, P.S.; Bath, A.S. Microbiological safety and clinical efficacy of radiation sterilized amniotic membranes for treatment of second-degree burns. Burns 2007, 33, 505–510. [Google Scholar] [CrossRef]
- Puyana, S.; Elkbuli, A.; Ruiz, S.; Bernal, E.; McKenney, M.; Lim, R.; Askari, M.; Mir, H. The Use of Dehydrated Human Amniotic/Chorionic Membrane Skin Substitute in the Treatment of Pediatric Facial Burn. J. Craniofac. Surg. 2019, 30, 2551–2554. [Google Scholar] [CrossRef] [PubMed]
- Fesli, A.; Sari, A.; Yilmaz, N.; Comelekoglu, U.; Tasdelen, B. Enhancement of nerve healing with the combined use of amniotic membrane and granulocyte-colony-stimulating factor. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Karaman, M.; Tuncel, A.; Sheidaei, S.; Senol, M.G.; Karabulut, M.H.; Deveci, I.; Karaman, N. Amniotic membrane covering for facial nerve repair. Neural Regen. Res. 2013, 8, 975–982. [Google Scholar] [PubMed]
- Noël, J.; Mascarenhas, A.; Patel, E.; Reddy, S.; Sandri, M.; Bhat, S.; Moschovas, M.; Rogers, T.; Ahmed, S.; Stirt, D.; et al. Nerve spare robot assisted laparoscopic prostatectomy with amniotic membranes: Medium term outcomes. J. Robot. Surg. 2022, 16, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Noël, J.; Ahmed, S.; Mascarenhas, A.; Stirt, D.; Moschovas, M.; Patel, E.; Reddy, S.; Bhat, S.; Rogers, T.; Patel, V. Impact of human placental derivative allografts on functional and oncological outcomes after radical prostatectomy: A literature review. J. Robot. Surg. 2023, 17, 265–273. [Google Scholar] [CrossRef]
- Razdan, S.; Bajpai, R.R.; Sanchez, M.A. A matched and controlled longitudinal cohort study of dehydrated human amniotic membrane allograft sheet used as a wraparound nerve bundles in robotic-assisted laparoscopic radical prostatectomy: A puissant adjunct for enhanced potency outcomes. J. Robot. Surg. 2019, 13, 475–481. [Google Scholar] [CrossRef]
- Ahmed, M.; Esposito, M.; Lovallo, G. A single-center, retrospective review of robot-assisted laparoscopic prostatectomy with and without cryopreserved umbilical cord allograft in improving continence recovery. J. Robot. Surg. 2020, 14, 283–289. [Google Scholar] [CrossRef]
- Elliott, P.A.; Hsiang, S.; Narayanan, R.; Bierylo, J.; Chang, S.C.; Twardowski, P.; Wilson, T.G. Cryopreserved placental tissue allograft accelerates time to continence following robot-assisted radical prostatectomy. J. Robot. Surg. 2021, 15, 877–883. [Google Scholar] [CrossRef]
- Alvim, R.G.; Hughes, C.; Somma, A.; Nagar, K.K.; Wong, N.C.; La Rosa, S.; Monette, S.; Kim, K.; Coleman, J.A. The potential risk of tumor progression after use of dehydrated human amnion/chorion membrane allograft in a positive margin resection model. Ther. Adv. Urol. 2019, 11, 1756287219837771. [Google Scholar] [CrossRef]
- Peak, T.C.; Praharaj, P.P.; Panigrahi, G.K.; Doyle, M.; Su, Y.; Schlaepfer, I.R.; Singh, R.; Griend, D.J.V.; Alickson, J.; Hemal, A.; et al. Exosomes secreted by placental stem cells selectively inhibit growth of aggressive prostate cancer cells. Biochem. Biophys. Res. Commun. 2018, 499, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Bustos, M.A.; Yokoe, T.; Shoji, Y.; Kobayashi, Y.; Mizuno, S.; Murakami, T.; Zhang, X.; Sekhar, S.C.; Kim, S.; Ryu, S.; et al. MiR-181a targets STING to drive PARP inhibitor resistance in BRCA- mutated triple-negative breast cancer and ovarian cancer. Cell Biosci. 2023, 13, 200. [Google Scholar] [CrossRef] [PubMed]
- Shoji, Y.; Yokoe, T.; Kobayashi, Y.; Murakami, T.; Bostick, P.J.; Shiloh, Y.; Hoon, D.S.; Bustos, M.A. UBQLN4 promotes STING proteasomal degradation during cisplatin-induced DNA damage in triple-negative breast cancer. Clin. Transl. Med. 2022, 12, e985. [Google Scholar] [CrossRef]
- Bauer, D.; Wasmuth, S.; Hennig, M.; Baehler, H.; Steuhl, K.P.; Heiligenhaus, A. Amniotic membrane transplantation induces apoptosis in T lymphocytes in murine corneas with experimental herpetic stromal keratitis. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3188–3198. [Google Scholar] [CrossRef]
- He, H.; Li, W.; Tseng, D.Y.; Zhang, S.; Chen, S.Y.; Day, A.J.; Tseng, S.C. Biochemical characterization and function of complexes formed by hyaluronan and the heavy chains of inter-alpha-inhibitor (HC*HA) purified from extracts of human amniotic membrane. J. Biol. Chem. 2009, 284, 20136–20146. [Google Scholar] [CrossRef]
- He, H.; Zhang, S.; Tighe, S.; Son, J.; Tseng, S.C.G. Immobilized heavy chain-hyaluronic acid polarizes lipopolysaccharide-activated macrophages toward M2 phenotype. J. Biol. Chem. 2013, 288, 25792–25803. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Sacchetti, M.; Bonini, S. Nerve growth factor therapy for corneal disease. Curr. Opin. Ophthalmol. 2012, 23, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Iwao, A.; Saijo, H.; Nakayama, T.; Higashi, A.; Kashiyama, K.; Mitsutake, N.; Tanaka, K. Fresh human amniotic membrane wrapping promotes peripheral nerve regeneration in PGA-collagen tubes. J. Plast. Surg. Hand Surg. 2023, 58, 13–17. [Google Scholar] [CrossRef]
- Chen, L.; Song, X.; Yao, Z.; Zhou, C.; Yang, J.; Yang, Q.; Chen, J.; Wu, J.; Sun, Z.; Gu, L.; et al. Gelatin nanofiber-reinforced decellularized amniotic membrane promotes axon regeneration and functional recovery in the surgical treatment of peripheral nerve injury. Biomaterials 2023, 300, 122207. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Cohort | Negative Control | Brand A | Brand B | |
|---|---|---|---|---|
| Number of Patients in Each Group | 362 | 143 | 142 | 77 |
| Median (IQR) Follow-up Time | 41 months (27–56 months) | |||
| Survival Status at Most Recent Follow-up | ||||
| Alive without disease | 325 (90%) | 126 (88%) | 133 (94%;) | 66 (85%) |
| Alive with disease | 33 (9%) | 16 (11%) | 7 (5%) | 10 (13%) |
| Deceased without disease | 3 (1%) | 1 (1%) | 2 (1%) | 0 |
| Deceased with disease | 1 (0.3%) | 0 | 0 | 1 (1%) |
| BCR | ||||
| Yes | 72 (20%) | 32 (22%) | 27 (19%) | 13 (17%) |
| No | 290 (80%) | 111 (78%) | 115 (81%) | 64 (83%) |
| Any Salvage Therapy Given (ADT, RT, and/or chemo) | 70 (20%; N = 358) | 35 (25%; N = 141) | 27 (19%; N = 142) | 8 (12%; N = 75) |
| Salvage ADT | 46 (66%; N = 70) | 21 (60%; N = 35) | 18 (67%; N = 27) | 7 (88%; N = 8) |
| Salvage RT | 62 (89%; N = 70) | 33 (94%; N = 35) | 22 (82%; N = 27) | 7 (88%; N = 8) |
| Salvage Chemotherapy | 9 (3%; N = 70) | 9 (26%; N = 35) | 0 | 0 |
| Post-operative Continence Achieved (defined as ≤1 security pad per day) | ||||
| Yes | 329 (93%; N = 352) | 125 (91%; N = 137) | 133 (96%; N = 139) | 71 (93%; N = 76) |
| No | 23 (7%; N = 352) | 12 (9%; N = 137) | 6 (4%; N = 139) | 5 (7%; N = 76) |
| N/A | 10 (3%; N = 362) | 6 (4%; N = 143) | 3 (2%; N = 142) | 1 (1%; N = 77) |
| Median (IQR) post-operative Gleason Grade | 2 (2–3) | 2 (2–3) | 3 (2–3) | 2 (2–3) |
| Pathological T Stage | ||||
| pT1 | 3 (1%) | 3 (2%) | 0 | 0 |
| pT2 | 259 (72%) | 110 (77%) | 96 (68%) | 53 (69%) |
| pT3 | 100 (28%) | 30 (21%) | 46 (32%) | 24 (31%) |
| Pathological Nodal Stage | ||||
| pN0 | 187 (83%; N = 225) | 80 (89%; N = 90) | 70 (80%; N = 88) | 37 (79%; N = 47) |
| pN1 | 38 (17%; N = 225) | 10 (11%; N = 90) | 18 (20%; N = 88) | 10 (21%; N = 47) |
| pNx | 137 (38%; N = 362) | 53 (37%; N = 143) | 54 (38%; N = 142) | 30 (39%; N = 77) |
| Margin Status | ||||
| R0 | 227 (63%; N = 359) | 85 (60%; N = 142) | 91 (64%; N = 142) | 51 (68%; N = 75) |
| R1 | 132 (37%; N = 359) | 57 (40%; N = 142) | 51 (36%; N = 142) | 24 (32%; N = 75) |
| RX | 3 (1%; N = 362) | 1 (0.7%; N = 143) | 0 | 2 (3%; N = 77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gottlieb, J.; Hanes, D.A.; Bustos, M.A.; Choe, J.; Luu, A.; Seizer, D.; Hoon, D.S.B.; Wilson, T.G. Impact of Cryopreserved Placental Allografts on Biochemical Recurrence in Prostate Cancer. Cancers 2024, 16, 2973. https://doi.org/10.3390/cancers16172973
Gottlieb J, Hanes DA, Bustos MA, Choe J, Luu A, Seizer D, Hoon DSB, Wilson TG. Impact of Cryopreserved Placental Allografts on Biochemical Recurrence in Prostate Cancer. Cancers. 2024; 16(17):2973. https://doi.org/10.3390/cancers16172973
Chicago/Turabian StyleGottlieb, Josh, Douglas A. Hanes, Matias A. Bustos, Jane Choe, Albert Luu, Daniel Seizer, Dave S. B. Hoon, and Timothy G. Wilson. 2024. "Impact of Cryopreserved Placental Allografts on Biochemical Recurrence in Prostate Cancer" Cancers 16, no. 17: 2973. https://doi.org/10.3390/cancers16172973
APA StyleGottlieb, J., Hanes, D. A., Bustos, M. A., Choe, J., Luu, A., Seizer, D., Hoon, D. S. B., & Wilson, T. G. (2024). Impact of Cryopreserved Placental Allografts on Biochemical Recurrence in Prostate Cancer. Cancers, 16(17), 2973. https://doi.org/10.3390/cancers16172973