Effect of Direct Acting Antiviral Drugs on the Occurrence and Recurrence of Intra- and Extra-Hepatic Malignancies in Patients with Chronic Hepatitis C Virus Infection

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
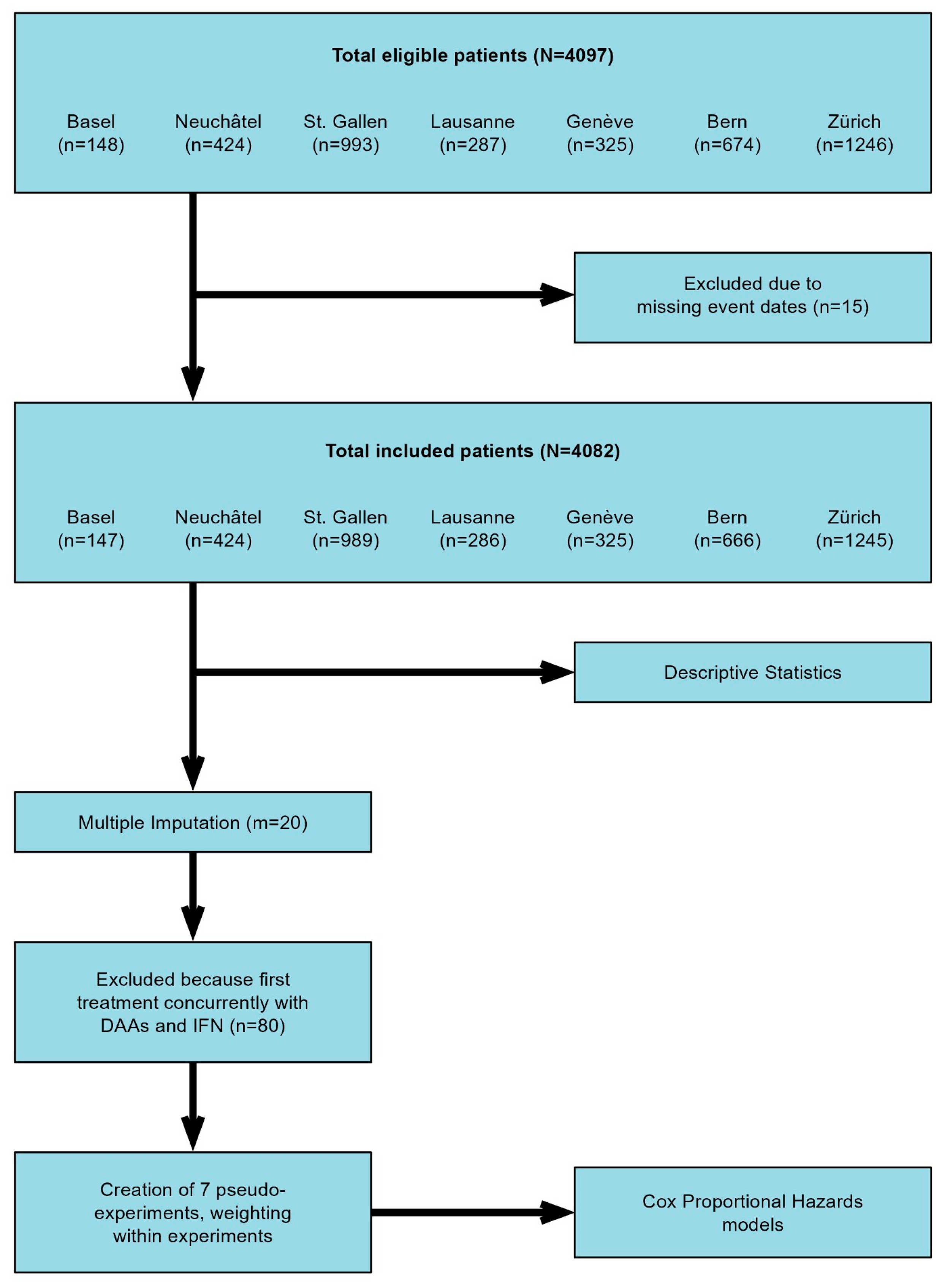
2.1. Study Population and Design
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Outcome after HCV Therapy
3.3. Analysis of the Risk for IHT during Anti HCV Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
References
- Stanciu, C.; Muzica, C.M.; Girleanu, I.; Cojocariu, C.; Sfarti, C.; Singeap, A.M.; Huiban, L.; Chiriac, S.; Cuciureanu, T.; Trifan, A. An update on direct antiviral agents for the treatment of hepatitis C. Expert Opin. Pharmacother. 2021, 22, 1729–1741. [Google Scholar] [CrossRef]
- van der Meer, A.J.; Feld, J.J.; Hofer, H.; Almasio, P.L.; Calvaruso, V.; Fernandez-Rodriguez, C.M.; Aleman, S.; Ganne-Carrie, N.; D’Ambrosio, R.; Pol, S.; et al. Risk of cirrhosis-related complications in patients with advanced fibrosis following hepatitis C virus eradication. J. Hepatol. 2017, 66, 485–493. [Google Scholar] [CrossRef]
- Vaziri, A.; Gimson, A.; Agarwal, K.; Aldersley, M.; Bathgate, A.; MacDonald, D.; McPherson, S.; Mutimer, D.; Gelson, W. Liver transplant listing for hepatitis C-associated cirrhosis and hepatocellular carcinoma has fallen in the United Kingdom since the introduction of direct-acting antiviral therapy. J. Viral Hepat. 2019, 26, 231–235. [Google Scholar] [CrossRef]
- Morgan, R.L.; Baack, B.; Smith, B.D.; Yartel, A.; Pitasi, M.; Falck-Ytter, Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: A meta-analysis of observational studies. Ann. Intern. Med. 2013, 158, 329–337. [Google Scholar] [CrossRef]
- European Union, H.C.V.C. Hepatitis C virus prevalence and level of intervention required to achieve the WHO targets for elimination in the European Union by 2030: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 325–336. [Google Scholar] [CrossRef]
- Rockey, D.C.; Friedman, S.L. Fibrosis Regression After Eradication of Hepatitis C Virus: From Bench to Bedside. Gastroenterology 2021, 160, 1502–1520.e1. [Google Scholar] [CrossRef]
- Lens, S.; Baiges, A.; Alvarado-Tapias, E.; LLop, E.; Martinez, J.; Fortea, J.I.; Ibanez-Samaniego, L.; Marino, Z.; Rodriguez-Tajes, S.; Gallego, A.; et al. Clinical outcome and hemodynamic changes following HCV eradication with oral antiviral therapy in patients with clinically significant portal hypertension. J. Hepatol. 2020, 73, 1415–1424. [Google Scholar] [CrossRef]
- Krassenburg, L.A.P.; Maan, R.; Ramji, A.; Manns, M.P.; Cornberg, M.; Wedemeyer, H.; de Knegt, R.J.; Hansen, B.E.; Janssen, H.L.A.; de Man, R.A.; et al. Clinical outcomes following DAA therapy in patients with HCV-related cirrhosis depend on disease severity. J. Hepatol. 2021, 74, 1053–1063. [Google Scholar] [CrossRef]
- van der Meer, A.J.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.F.; Lammert, F.; Duarte-Rojo, A.; Heathcote, E.J.; Manns, M.P.; Kuske, L.; et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA 2012, 308, 2584–2593. [Google Scholar] [CrossRef]
- Reig, M.; Marino, Z.; Perello, C.; Inarrairaegui, M.; Ribeiro, A.; Lens, S.; Diaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef]
- Conti, F.; Buonfiglioli, F.; Scuteri, A.; Crespi, C.; Bolondi, L.; Caraceni, P.; Foschi, F.G.; Lenzi, M.; Mazzella, G.; Verucchi, G.; et al. Early occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals. J. Hepatol. 2016, 65, 727–733. [Google Scholar] [CrossRef]
- The ANRS Collaborative Study Group on Hepatocellular Carcinoma (ANRS CO22 HEPATHER, CO12 CirVir and CO23 CUPILT Cohorts). Lack of evidence of an effect of direct-acting antivirals on the recurrence of hepatocellular carcinoma: Data from three ANRS cohorts. J. Hepatol. 2016, 65, 734–740. [Google Scholar] [CrossRef]
- Sapena, V.; Enea, M.; Torres, F.; Celsa, C.; Rios, J.; Rizzo, G.E.M.; Nahon, P.; Marino, Z.; Tateishi, R.; Minami, T.; et al. Hepatocellular carcinoma recurrence after direct-acting antiviral therapy: An individual patient data meta-analysis. Gut 2022, 71, 593–604. [Google Scholar] [CrossRef]
- Waziry, R.; Hajarizadeh, B.; Grebely, J.; Amin, J.; Law, M.; Danta, M.; George, J.; Dore, G.J. Hepatocellular carcinoma risk following direct-acting antiviral HCV therapy: A systematic review, meta-analyses, and meta-regression. J. Hepatol. 2017, 67, 1204–1212. [Google Scholar] [CrossRef]
- Lu, M.; Salgia, R.; Li, J.; Trudeau, S.; Rupp, L.B.; Wu, T.; Daida, Y.G.; Schmidt, M.A.; Gordon, S.C. Dynamic risk assessment for hepatocellular carcinoma in patients with chronic hepatitis C. J. Viral Hepat. 2023, 30, 746–755. [Google Scholar] [CrossRef]
- Hamdane, N.; Juhling, F.; Crouchet, E.; El Saghire, H.; Thumann, C.; Oudot, M.A.; Bandiera, S.; Saviano, A.; Ponsolles, C.; Roca Suarez, A.A.; et al. HCV-Induced Epigenetic Changes Associated with Liver Cancer Risk Persist After Sustained Virologic Response. Gastroenterology 2019, 156, 2313–2329.e2317. [Google Scholar] [CrossRef]
- Perez, S.; Kaspi, A.; Domovitz, T.; Davidovich, A.; Lavi-Itzkovitz, A.; Meirson, T.; Alison Holmes, J.; Dai, C.Y.; Huang, C.F.; Chung, R.T.; et al. Hepatitis C virus leaves an epigenetic signature post cure of infection by direct-acting antivirals. PLoS Genet. 2019, 15, e1008181. [Google Scholar] [CrossRef]
- Matsuura, K.; Sawai, H.; Ikeo, K.; Ogawa, S.; Iio, E.; Isogawa, M.; Shimada, N.; Komori, A.; Toyoda, H.; Kumada, T.; et al. Genome-Wide Association Study Identifies TLL1 Variant Associated with Development of Hepatocellular Carcinoma After Eradication of Hepatitis C Virus Infection. Gastroenterology 2017, 152, 1383–1394. [Google Scholar] [CrossRef]
- Aoyagi, H.; Iijima, H.; Gaber, E.S.; Zaitsu, T.; Matsuda, M.; Wakae, K.; Watashi, K.; Suzuki, R.; Masaki, T.; Kahn, J.; et al. Hepatocellular organellar abnormalities following elimination of hepatitis C virus. Liver Int. 2023, 43, 1677–1690. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Leyrat, C.; Seaman, S.R.; White, I.R.; Douglas, I.; Smeeth, L.; Kim, J.; Resche-Rigon, M.; Carpenter, J.R.; Williamson, E.J. Propensity score analysis with partially observed covariates: How should multiple imputation be used? Stat. Methods Med. Res. 2019, 28, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Celsa, C.; Calvaruso, V.; Petta, S.; Cacciola, I.; Cannavo, M.R.; Madonia, S.; Rossi, M.; Magro, B.; Rini, F.; et al. Direct-acting antivirals after successful treatment of early hepatocellular carcinoma improve survival in HCV-cirrhotic patients. J. Hepatol. 2019, 71, 265–273. [Google Scholar] [CrossRef]
- Singal, A.G.; Rich, N.E.; Mehta, N.; Branch, A.D.; Pillai, A.; Hoteit, M.; Volk, M.; Odewole, M.; Scaglione, S.; Guy, J.; et al. Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection Is Associated with Increased Survival in Patients with a History of Hepatocellular Carcinoma. Gastroenterology 2019, 157, 1253–1263.e2. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Kanwal, F.; Richardson, P.; Kramer, J. Risk of hepatocellular carcinoma after sustained virological response in Veterans with hepatitis C virus infection. Hepatology 2016, 64, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.L.; Li, B.; Zhang, X.X.; Chen, Y.; Fu, Y.L.; Lv, J.; Liu, Y.M.; Yu, Z.J. Clinical Model for Predicting Hepatocellular Carcinomas in Patients with Post-Sustained Virologic Responses of Chronic Hepatitis C: A Case Control Study. Gut Liver 2016, 10, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Song, H.J.; Chang, C.Y.; Wilson, D.L.; Lo-Ciganic, W.H.; Park, H. Impact of Direct-acting Antivirals on Hepatocellular Carcinoma and Mortality Among Medicaid Beneficiaries with Hepatitis C. Med. Care 2023, 61, 505–513. [Google Scholar] [CrossRef]
- Minami, T.; Tateishi, R.; Fujiwara, N.; Nakagomi, R.; Nakatsuka, T.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; Fujinaga, H.; et al. Impact of Obesity and Heavy Alcohol Consumption on Hepatocellular Carcinoma Development after HCV Eradication with Antivirals. Liver Cancer 2021, 10, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Pelusi, S.; Bianco, C.; Colombo, M.; Cologni, G.; Del Poggio, P.; Pugliese, N.; Prati, D.; Pigozzi, M.G.; D’Ambrosio, R.; Lampertico, P.; et al. Metabolic dysfunction outperforms ultrasonographic steatosis to stratify hepatocellular carcinoma risk in patients with advanced hepatitis C cured with direct-acting antivirals. Liver Int. 2023, 43, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Sanduzzi-Zamparelli, M.; Marino, Z.; Lens, S.; Sapena, V.; Iserte, G.; Pla, A.; Granel, N.; Bartres, C.; Llarch, N.; Vilana, R.; et al. Liver cancer risk after HCV cure in patients with advanced liver disease without non-characterized nodules. J. Hepatol. 2022, 76, 874–882. [Google Scholar] [CrossRef]
- Villani, R.; Facciorusso, A.; Bellanti, F.; Tamborra, R.; Piscazzi, A.; Landriscina, M.; Vendemiale, G.; Serviddio, G. DAAs Rapidly Reduce Inflammation but Increase Serum VEGF Level: A Rationale for Tumor Risk during Anti-HCV Treatment. PLoS ONE 2016, 11, e0167934. [Google Scholar] [CrossRef]
- Sangiovanni, A.; Alimenti, E.; Gattai, R.; Filomia, R.; Parente, E.; Valenti, L.; Marzi, L.; Pellegatta, G.; Borgia, G.; Gambato, M.; et al. Undefined/non-malignant hepatic nodules are associated with early occurrence of HCC in DAA-treated patients with HCV-related cirrhosis. J. Hepatol. 2020, 73, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Khaderi, S.; Singal, A.G.; Marrero, J.A.; Loo, N.; Asrani, S.K.; Amos, C.I.; Thrift, A.P.; Gu, X.; Luster, M.; et al. Risk factors for HCC in contemporary cohorts of patients with cirrhosis. Hepatology 2023, 77, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (Based on Data Available) | Both Therapies (Combined or Sequential Use) | DAAs Only | IFN-Based Only | Untreated during FU | p-Value * | |
|---|---|---|---|---|---|---|
| N | 4082 | 357 (140 combined) | 1180 | 1026 | 1519 | |
| Age, years | 45 [37–53] | 47 [41–53] | 48 [40–55] | 43 [35–50] | 44 [36–52] | <0.001 |
| Gender, Male | 2575 (63.1) | 249 (69.7) | 728 (61.7) | 673 (65.6) | 925 (61) | 0.004 |
| Missing data | 2 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (0.1) | |
| BMI | 24.06 [21.71–26.79] | 25.0 [22.65–27.40] | 24.30 [21.8–27] | 23.77 [21.51–26.56] | 23.83 [21.48–26.48] | <0.001 |
| Genotype | <0.001 | |||||
| 1 | 1981 (48.5) | 225 (63) | 641 (54.3) | 437 (42.6) | 678 (44.6) | |
| 2 | 266 (6.5) | 12 (3.4) | 57 (4.8) | 90 (8.8) | 107 (7) | |
| 3 | 1003(24.6) | 71 (19.9) | 204 (17.3) | 392 (38.2) | 336 (22.1) | |
| 4 | 405 (9.9) | 38 (10.6) | 125 (10.6) | 78 (7.6) | 164 (10.8) | |
| 5 | 6 (0.1) | 0 (0.0) | 3 (0.3) | 2 (0.2) | 1 (0.1) | |
| 6 | 3 (0.1) | 0 (0.0) | 1 (0.1) | 2 (0.2) | 0 (0.0) | |
| Missing data | 418 | 11 | 149 | 25 | 233 | |
| Comorbidities | ||||||
| Diabetes, Yes | 212 (5.2) | 21 (5.9) | 60 (5.1) | 60 (5.8) | 71 (4.7) | 0.577 |
| Missing data | 18 | 1 | 6 | 0 | 11 | |
| Heavy Drinking, Yes | 2061 (50.5) | 172 (48.2) | 613 (51.9) | 517 (50.4) | 759 (50) | 0.517 |
| Missing data | 9 | 1 | 4 | 0 | 4 | |
| Co-infection | ||||||
| HIV infection Yes | 258 (6.9) | 27 (7.8) | 50 (4.8) | 37 (3.8) | 144 (10.6) | <0.001 |
| Missing data | 355 | 12 | 128 | 53 | 162 | |
| Anti-HBc Yes | 1473 (39.9) | 142 (41.5) | 390 (37.1) | 392 (41.1) | 549 (40.8) | 0.175 |
| Missing | 390 | 15 | 128 | 73 | 174 | |
| HBsAg, Yes | 901 (24.1) | 94 (27.3) | 195 (18.7) | 209 (21.2) | 403 (29.5) | <0.001 |
| Missing | 345 (8.5) | 13 (3.6) | 139 (11.8) | 41 (4.0) | 152 (10) | |
| Cirrhosis, yes | 654 (16.1) | 97 (27.2) | 192 (16.3) | 178 (17.4) | 187 (12.4) | <0.001 |
| Missing | 14 | 0 | 4 | 5 | 5 | |
| Liver stiffness, kPa | 6.60 [4.80–10.40] | 8.60 [6.10–14.40] | 7.00 [5.03–11] | 6.20 [4.70–10.40] | 5.90 [4.60–7.85] | <0.001 |
| Child Pugh score | 5 [5–6] | 5 [5–6] | 5 [5–5] | 5 [5–6] | 5 [5–6] | 0.025 |
| PLT <150.000, Yes | 2527 (75.2) | 210 (66) | 620 (79.4) | 652 (67.2) | 1045 (81) | <0.001 |
| Missing | 723 | 39 | 399 | 56 | 229 | |
| SVR | <0.001 | |||||
| Yes | 1860 (76.9) | 277 (92.3) | 933 (96) | 650 (78) | <0.001 | |
| Unknown ** | 458 (11.2) | 57 (16) | 208 (17.3) | 193 (18.8) | ||
| History of cancer (IHT or EHT) | ||||||
| Yes | 80 (3.5) | 13 (6) | 14 (1.8) | 26 (4.5) | 27 (3.7) | 0.006 |
| Missing | 1781 | 142 | 401 | 442 | 796 | |
| Development of events in the follow-up | ||||||
| EHT (yes) | 168 (4.1) | 22 (6.2) | 39 (3.3) | 47 (4.6) | 60 (3.9) | 0.093 |
| IHT (yes) | 179 (4.4) | 36 (10.1) | 42 (3.6) | 59 (5.8) | 42 (2.8) | <0.001 |
| Death (yes) | 613 (15.0) | 38 (10.6) | 64 (5.4) | 199 (19.4) | 312 (20.5) | <0.001 |
| Time | IFN-Based Regimens Cumulative Incidence (95% CI) | DAA Cumulative Incidence (95% CI) | Untreated Cumulative Incidence (95% CI) |
|---|---|---|---|
| 1 year | 0.17 [0.04–0.68] | 0.82 [0.43–1.58] | 0.18 [0.03–1.3] |
| 3 years | 0.89 [0.48–1.64] | 2 [1.29–3.09] | 0.65 [0.25–1.74] |
| 5 years | 1.55 [0.96–2.48] | 4.27 [2.93–6.2] | 0.89 [0.4–1.99] |
| 10 years | 4.78 [3.59–6.38] | 2.07 [1.29–3.31] | |
| 15 years | 9.02 [6.96–11.68] | 3.3 [2.33–4.68] | |
| 20 years | 4.94 [3.72–6.57] | ||
| Cirrhosis | |||
| IFN-based regimens Cumulative Incidence (95% CI) | DAA Cumulative Incidence (95% CI) | Untreated Cumulative Incidence (95% CI) | |
| 1 year | 0.43 [0.06–3.06] | 2.80 [1.18–6.65] | 2.38 [0.34–16.51] |
| 3 years | 2.22 [0.93–5.28] | 7.52 [4.46–12.59] | 2.38 [0.34–16.51] |
| 5 years | 4.95 [2.78–8.81] | 12.45 [8.08–19.18] | 4.54 [1.39–14.82] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radu, P.; Becchetti, C.; Schropp, J.; Schmid, P.; Künzler-Heule, P.; Mertens, J.; Moradpour, D.; Müllaupt, B.; Semela, D.; Negro, F.; et al. Effect of Direct Acting Antiviral Drugs on the Occurrence and Recurrence of Intra- and Extra-Hepatic Malignancies in Patients with Chronic Hepatitis C Virus Infection. Cancers 2024, 16, 2573. https://doi.org/10.3390/cancers16142573
Radu P, Becchetti C, Schropp J, Schmid P, Künzler-Heule P, Mertens J, Moradpour D, Müllaupt B, Semela D, Negro F, et al. Effect of Direct Acting Antiviral Drugs on the Occurrence and Recurrence of Intra- and Extra-Hepatic Malignancies in Patients with Chronic Hepatitis C Virus Infection. Cancers. 2024; 16(14):2573. https://doi.org/10.3390/cancers16142573
Chicago/Turabian StyleRadu, Pompilia, Chiara Becchetti, Jonas Schropp, Patrick Schmid, Patrizia Künzler-Heule, Joachim Mertens, Darius Moradpour, Beat Müllaupt, David Semela, Francesco Negro, and et al. 2024. "Effect of Direct Acting Antiviral Drugs on the Occurrence and Recurrence of Intra- and Extra-Hepatic Malignancies in Patients with Chronic Hepatitis C Virus Infection" Cancers 16, no. 14: 2573. https://doi.org/10.3390/cancers16142573
APA StyleRadu, P., Becchetti, C., Schropp, J., Schmid, P., Künzler-Heule, P., Mertens, J., Moradpour, D., Müllaupt, B., Semela, D., Negro, F., Heim, M., Clerc, O., Roelens, M., Keiser, O., Berzigotti, A., & Swiss Hepatitis C Cohort Study. (2024). Effect of Direct Acting Antiviral Drugs on the Occurrence and Recurrence of Intra- and Extra-Hepatic Malignancies in Patients with Chronic Hepatitis C Virus Infection. Cancers, 16(14), 2573. https://doi.org/10.3390/cancers16142573