

Systemic Treatment of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Multicenter Trial

 , , ,
, , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Treatment and Outcome Measurement
2.3. Study Design and Statistical Analysis
3. Results
3.1. Baseline Data
3.2. HCC Recurrence after Liver Transplantation
3.3. Survival Data under Tyrosine Kinase Inhibitors Sorafenib or Lenvatinib
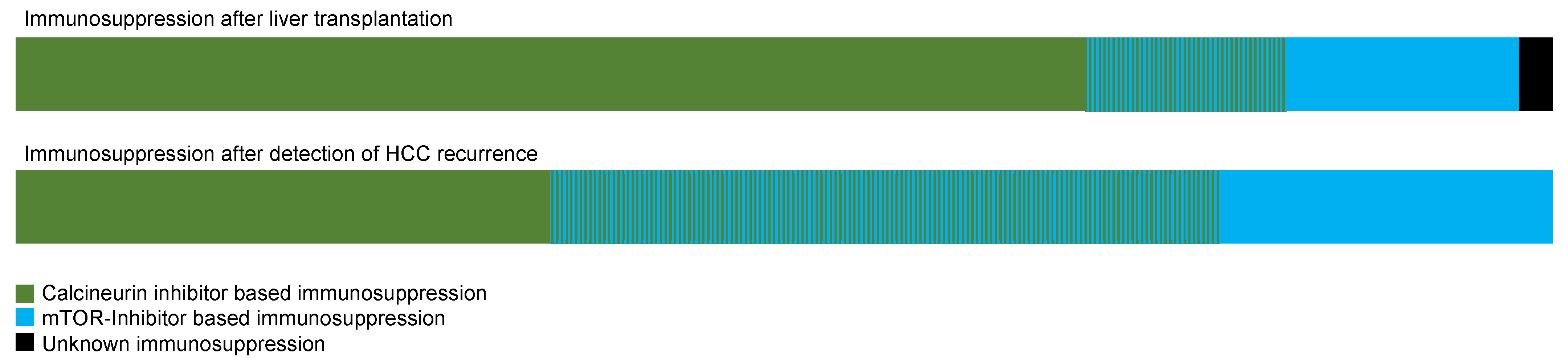
3.4. Survival Data in Dependence on the Immunosuppression
3.5. Survival Data in Dependence on the Time of Recurrence and the Organ Manifestation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernandez-Sevilla, E.; Allard, M.; Selten, J.; Golse, N.; Vibert, E.; Cunha, A.S.; Cherqui, D.; Castaing, D.; Adam, R. Recurrence of hepatocellular carcinoma after liver transplantation: Is there a place for resection? Liver Transplant. 2017, 23, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Lim, H.Y.; Kudo, M.; Breder, V.V.; Merle, P.; et al. IMbrave150: Updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J. Clin. Oncol. 2021, 39 (Suppl. 3), 267. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Van Dao, T.; De Toni, E.N.; et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022, 1, EVIDoa2100070. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Decaens, T.; Kudo, M.; Qin, S.; Fonseca, L.; Sangro, B.; Karachiwala, H.; Park, J.-W.; Gane, E.; Pinter, M.; et al. Nivolumab (NIVO) plus ipilimumab (IPI) vs lenvatinib (LEN) or sorafenib (SOR) as first-line treatment for unresectable hepatocellular carcinoma (uHCC): First results from CheckMate 9DW. J. Clin. Oncol. 2024, 42 (Suppl. S17), LBA4008. [Google Scholar] [CrossRef]
- Chok, K.S. Management of recurrent hepatocellular carcinoma after liver transplant. World J. Hepatol. 2015, 7, 1142. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Scheiner, B.; Peck-Radosavljevic, M. Immunotherapy for advanced hepatocellular carcinoma: A focus on special subgroups. Gut 2021, 70, 204–214. [Google Scholar] [CrossRef] [PubMed]
- López Ortega, S.; González Grande, R.; Santaella Leiva, I.; De la Cruz Lombardo, J.; Jiménez Pérez, M. Efficacy and Safety of Sorafenib after Liver Transplantation: Experience in Our Center. Transplant. Proc. 2020, 52, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.; Yoo, C.; Ryu, M.-H.; Park, S.R.; Kim, H.-D.; Ryoo, B.-Y. Efficacy and safety of lenvatinib in patients with recurrent hepatocellular carcinoma after liver transplantation: A retrospective analysis. J. Clin. Oncol. 2022, 40 (Suppl. S4), 410. [Google Scholar] [CrossRef]
- Sposito, C.; Mariani, L.; Germini, A.; Reyes, M.F.; Bongini, M.; Grossi, G.; Bhoori, S.; Mazzaferro, V. Comparative efficacy of sorafenib versus best supportive care in recurrent hepatocellular carcinoma after liver transplantation: A case-control study. J. Hepatol. 2013, 59, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R. New data supporting modified RECIST (mRECIST) for hepatocellular carcinoma. Clin. Cancer Res. 2013, 19, 1312–1314. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.M.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.M.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Leone, M.S.; Biolato, M.; Liguori, A.; Bianco, G.; Spoletini, G.; Gasbarrini, A.; Miele, L.; Pompili, M. Therapeutic Approach to Post-Transplant Recurrence of Hepatocellular Carcinoma: Certainties and Open Issues. Cancers 2023, 15, 5593. [Google Scholar] [CrossRef] [PubMed]
- Wassmer, C.-H.; El Hajji, S.; Papazarkadas, X.; Compagnon, P.; Tabrizian, P.; Lacotte, S.; Toso, C. Immunotherapy and Liver Transplantation: A Narrative Review of Basic and Clinical Data. Cancers 2023, 15, 4574. [Google Scholar] [CrossRef] [PubMed]
- Riella, L.V.; Paterson, A.M.; Sharpe, A.H.; Chandraker, A. Role of the PD-1 pathway in the immune response. Am. J. Transplant. 2012, 12, 2575–2587. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Dalmau, A.; Campistol, J.M. Immunosuppressive therapy and malignancy in organ transplant recipients: A systematic review. Drugs 2007, 67, 1167–1198. [Google Scholar] [CrossRef] [PubMed]
- Toso, C.; Merani, S.; Bigam, D.L.; Shapiro, A.M.J.; Kneteman, N.M. Sirolimus-based immunosuppression is associated with increased survival after liver transplantation for hepatocellular carcinoma. Hepatology 2010, 51, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Matter, M.S.; Decaens, T.; Andersen, J.B.; Thorgeirsson, S.S. Targeting the mTOR pathway in hepatocellular carcinoma: Current state and future trends. J. Hepatol. 2014, 60, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kudo, M.; Assenat, E.; Cattan, S.; Kang, Y.-K.; Lim, H.Y.; Poon, R.T.P.; Blanc, J.-F.; Vogel, A.; Chen, C.-L.; et al. Effect of Everolimus on Survival in Advanced Hepatocellular Carcinoma After Failure of Sorafenib. JAMA 2014, 312, 57. [Google Scholar] [CrossRef] [PubMed]
- Koeberle, D.; Dufour, J.-F.; Demeter, G.; Li, Q.; Ribi, K.; Samaras, P.; Saletti, P.; Roth, A.; Horber, D.; Buehlmann, M.; et al. Sorafenib with or without everolimus in patients with advanced hepatocellular carcinoma (HCC): A randomized multicenter, multinational phase II trial (SAKK 77/08 and SASL 29). Ann. Oncol. 2016, 27, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Pallotta, D.P.; Sansone, V.; Iavarone, M.; De Giorgio, M.; Ielasi, L.; Di Costanzo, G.G.; Giuffrida, P.; Sacco, R.; Pressiani, T.; et al. Outcomes of Sorafenib for Recurrent Hepatocellular Carcinoma After Liver Transplantation in the Era of Combined and Sequential Treatments. Transplantation 2023, 107, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Weinmann, A.; Niederle, I.M.; Koch, S.; Hoppe-Lotichius, M.; Heise, M.; Düber, C.; Schuchmann, M.; Otto, G.; Galle, P.R.; Wörns, M.-A. Sorafenib for recurrence of hepatocellular carcinoma after liver transplantation. Dig. Liver Dis. 2012, 44, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Martin, C.; Bustamante, J.; Castroagudin, J.F.; Salcedo, M.; Garralda, E.; Testillano, M.; Herrero, I.; Matilla, A.; Sangro, B. Efficacy and safety of sorafenib in combination with mammalian target of rapamycin inhibitors for recurrent hepatocellular carcinoma after liver transplantation. Liver Transplant. 2012, 18, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Ryoo, B.-Y.; Ryu, M.-H.; Lee, S.-G.; Hwang, S.; Suh, D.J.; Lee, H.C.; Kim, T.W.; Ahn, C.-S.; Kim, K.-H.; et al. Sorafenib for Recurrent Hepatocellular Carcinoma after Liver Transplantation. Jpn. J. Clin. Oncol. 2010, 40, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Kornberg, A.; Küpper, B.; Tannapfel, A.; Katenkamp, K.; Thrum, K.; Habrecht, O.; Wilberg, J. Long-term survival after recurrent hepatocellular carcinoma in liver transplant patients: Clinical patterns and outcome variables. Eur. J. Surg. Oncol. 2010, 36, 275–280. [Google Scholar] [CrossRef]
- Zhu, A.X.; Abrams, T.A.; Miksad, R.; Blaszkowsky, L.S.; Meyerhardt, J.A.; Zheng, H.; Ma, A.M.; Clark, J.W.; Kwak, E.L.; Schrag, D.; et al. Phase 1/2 study of everolimus in advanced hepatocellular carcinoma. Cancer 2011, 117, 5094–5102. [Google Scholar] [CrossRef] [PubMed]
- Welker, M.W.; Bechstein, W.O.; Zeuzem, S.; Trojan, J. Recurrent hepatocellular carcinoma after liver transplantation—An emerging clinical challenge. Transpl. Int. 2013, 26, 109–118. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
| Patients; n | 46 |
| Male/female; n, (%) | 36 (78.3)/10 (21.7) |
| Age at recurrence [y]; median, (range) | 57.5 (44–73) |
| BMI; median, (range) | 25.4 (18.1–41.5) |
| Etiology of liver disease | |
| Alcohol; n, (%) | 10 (21.7) |
| NASH/NAFLD; n, (%) | 6 (13.0) |
| Hepatitis B; n, (%) | 8 (17.4) |
| Hepatitis C; n, (%) | 24 (52.2) |
| Autoimmune hepatitis; n, (%) | 1 (2.2) |
| Prior therapy before oLT; n, (%) | 35 (76.1) |
| Resection; n, (%) | 4 (8.7) |
| Ablation; n, (%) | 7 (15.2) |
| TACE; n, (%) | 31 (71.7) |
| Tumor stage at oLT | |
| T1; n, (%) | 8 (17.4) |
| T2; n, (%) | 18 (39.1) |
| T3; n, (%) | 15 (32.6) |
| T4; n, (%) | 2 (4.3) |
| Unknown; n, (%) | 3 (6.5) |
| Tumor grade at oLT | |
| 1; n, (%) | 2 (4.3) |
| 2; n, (%) | 20 (43.5) |
| 3; n, (%) | 12 (26.1) |
| Unknown; n, (%) | 12 (26.1) |
| Within the Milan criteria; n, (%) | 11 (23.9) |
| Within the up-to-seven criteria; n, (%) | 18 (39.1) |
| AFP at oLT [ng/mL]; median, (range) | 59.2 (1.0–60,500.0) |
| Immunosuppression before HCC recurrence | |
| Ciclosporin; n, (%) | 2 (4.3) |
| dose [mg/d]; median, (range) | 140 (80–200) |
| Tacrolimus; n, (%) | 36 (78.3) |
| dose [mg/d]; median, (range) | 4 (0.5–10) |
| Sirolimus; n, (%) | 5 (10.9) |
| dose [mg/d]; median, (range) | 2 (2–3) |
| Everolimus; n, (%) | 9 (19.6) |
| dose [mg/d]; median, (range) | 2,5 (1–6) |
| Mycophenolat mofetil; n, (%) | 17 (37.0) |
| dose [mg/d]; median, (range) | 1000 (500–2000) |
| Dexamethason; n, (%) | 1 (2.2) |
| dose [mg/d] | 8 |
| Prednisolon; n, (%) | 8 (17.4) |
| dose [mg/d]; median, (range) | 6.25 (2.5–20) |
| Unknown; n, (%) | 1 (2.2) |
| Time to relapse [months]; median, (range) | 11.8 (0–117.7) |
| Organs affected by recurrence | |
| Liver graft; n, (%) | 21 (45.7) |
| Extrahepatic metastases; n, (%) | 36 (78.3) |
| Lung; n, (%) | 25 (54.3) |
| Bone; n, (%) | 7 (15.2) |
| Peritoneum; n, (%) | 7 (15.2) |
| Adrenal gland; n, (%) | 5 (10.9) |
| Intra- and extrahep. recurrence; n, (%) | 11 (23.9) |
| BCLC stage | |
| A; n, (%) | 3 (6.5) |
| B; n, (%) | 5 (10.9) |
| C; n, (%) | 38 (82.6) |
| D; n, (%) | 0 (0) |
| Local treatment; n, (%) | 25 (54.3) |
| Resection; n, (%) | 15 (32.6) |
| Ablation; n, (%) | 2 (4.34) |
| TACE; n, (%) | 5 (10.8) |
| SIRT; n, (%) | 4 (8.7) |
| Systemic first-line therapy | |
| Sorafenib; n, (%) | 39 (84.8) |
| Initial dose [mg/d]; median, (range) | 400 (200–800) |
| Lenvatinib; n, (%) | 7 (15.2) |
| Initial dose [mg/d]; median, (range) | 4 (4–12) |
| Immunosuppression under first-line treatment | |
| Ciclosporin; n, (%) | 2 (4.3) |
| dose [mg/d] | 200 |
| Tacrolimus; n, (%) | 34 (73.9) |
| dose [mg/d]; median, (range) | 3 (0.5–10) |
| Sirolimus; n, (%) | 11 (23.9) |
| dose [mg/d]; median, (range) | 1 (0.5–2) |
| Everolimus; n, (%) | 19 (41.3) |
| dose [mg/d]; median, (range) | 2 (0.5–6) |
| Mycophenolat mofetil; n, (%) | 7 (15.2) |
| dose [mg/d]; median, (range) | 1000 (500–2000) |
| Dexamethason; n, (%) | 1 (2.2) |
| dose [mg/d] | 8.0 |
| Prednisolon; n, (%) | 5 (10.9) |
| dose [mg/d]; median, (range) | 5.0 (2.5–10) |
| Laboratory results at treatment initiation | |
| AFP [ng/mL]; median, (range) | 59.2 (1.0–60,500) |
| Response to TKI Therapy, n = 46 | |
|---|---|
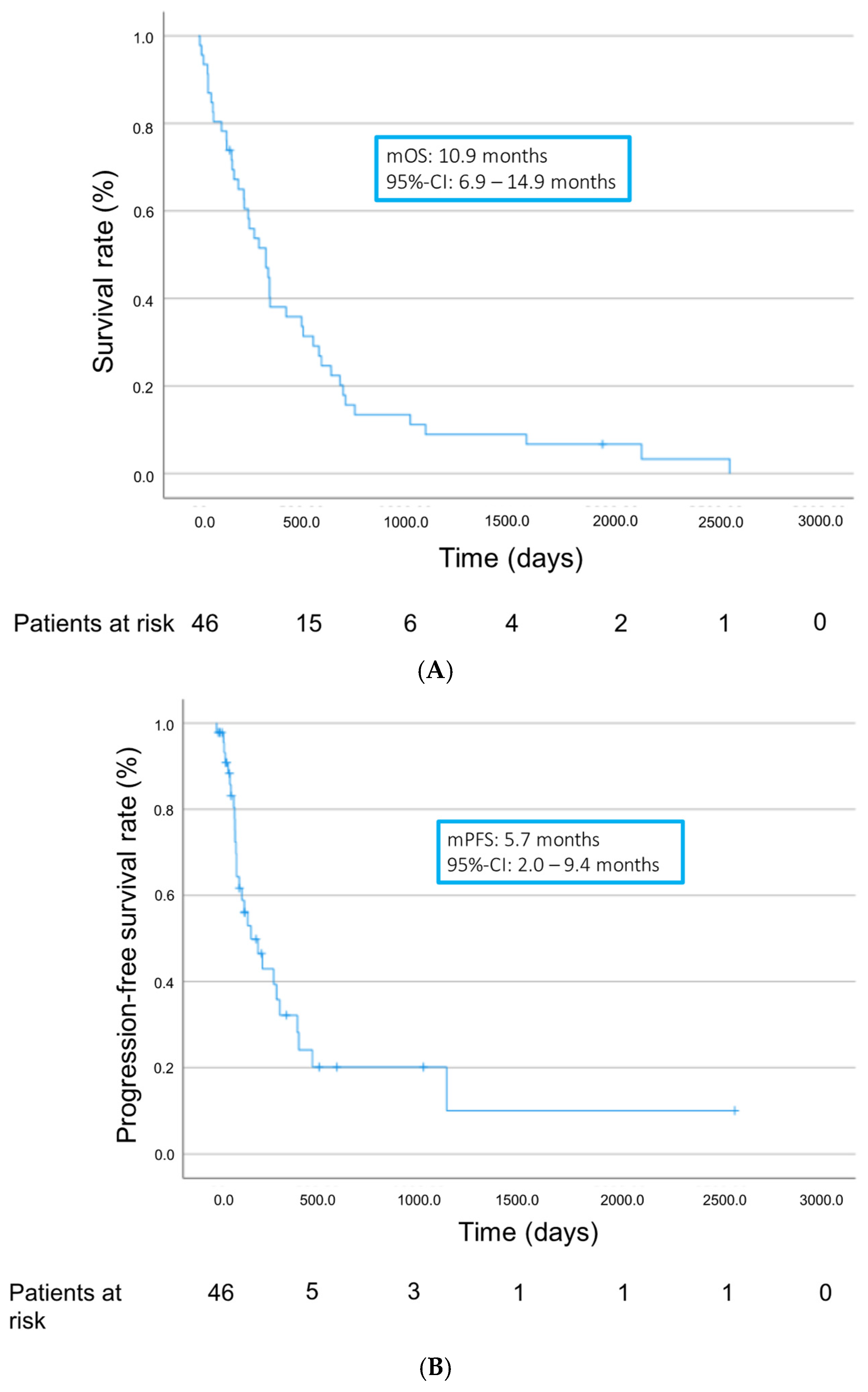
| mOS [months]; (95% CI) | 10.9 (6.9–14.9) |
| mPFS [months]; (95% CI) | 5.7 (2.0–9.4) |
| Stable disease; n, (%) | 8 (17.4) |
| Progressive disease; n, (%) | 23 (50.0) |
| No staging performed; n, (%) | 15 (32.6) |
| Disease control rate [%] | 17.4 |
| mTTP [months]; median, (range) | 3.5 (1.1–38) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Himmelsbach, V.; Jeschke, M.; Lange, C.M.; Scheiner, B.; Pinter, M.; Sinner, F.; Venerito, M.; Queck, A.; Trojan, J.; Waidmann, O.; et al. Systemic Treatment of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Multicenter Trial. Cancers 2024, 16, 2442. https://doi.org/10.3390/cancers16132442
Himmelsbach V, Jeschke M, Lange CM, Scheiner B, Pinter M, Sinner F, Venerito M, Queck A, Trojan J, Waidmann O, et al. Systemic Treatment of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Multicenter Trial. Cancers. 2024; 16(13):2442. https://doi.org/10.3390/cancers16132442
Chicago/Turabian StyleHimmelsbach, Vera, Matthias Jeschke, Christian M. Lange, Bernhard Scheiner, Matthias Pinter, Friedrich Sinner, Marino Venerito, Alexander Queck, Jörg Trojan, Oliver Waidmann, and et al. 2024. "Systemic Treatment of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Multicenter Trial" Cancers 16, no. 13: 2442. https://doi.org/10.3390/cancers16132442
APA StyleHimmelsbach, V., Jeschke, M., Lange, C. M., Scheiner, B., Pinter, M., Sinner, F., Venerito, M., Queck, A., Trojan, J., Waidmann, O., & Finkelmeier, F. (2024). Systemic Treatment of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Multicenter Trial. Cancers, 16(13), 2442. https://doi.org/10.3390/cancers16132442