
Neoadjuvant Chemotherapy in Breast Cancer: Evaluation of the Impact on Surgical Outcomes and Prognosis
 ,
,  ,
,  , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Demographics and Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Mougalian, S.S.; Soulos, P.R.; Killelea, B.K.; Lannin, D.R.; Abu-Khalaf, M.M.; DiGiovanna, M.P.; Sanft, T.B.; Pusztai, L.; Gross, C.P.; Chagpar, A.B. Use of neoadjuvant chemotherapy for patients with stage I to III breast cancer in the United States. Cancer 2015, 121, 2544–2552. [Google Scholar] [CrossRef] [PubMed]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Golshan, M.; Loibl, S.; Wong, S.M.; Houber, J.B.; O’Shaughnessy, J.; Rugo, H.S.; Wolmark, N.; McKee, M.D.; Maag, D.; Sullivan, D.M.; et al. Breast conservation after neoadjuvant chemotherapy for triple-negative breast cancer: Surgical results from the BrighTNess randomized clinical trial. JAMA Surg 2020, 155, e195410. [Google Scholar] [CrossRef]
- Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/31161190/ (accessed on 19 August 2023).
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Long-Term Outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Clough, K.B.; Acosta-Marín, V.; Nos, C. Rates of neoadjuvant chemotherapy and oncoplastic surgery for breast cancer surgery: A French national survey. Ann. Surg. Oncol. 2015, 11, 3504–3511. [Google Scholar] [CrossRef]
- Qin, Q.; Gao, F.; Jiang, W.; Tan, Q.; Mo, Q.; Wei, C. Effect of neoadjuvant chemotherapy on expressions of estrogen receptor, progesterone receptor, human epidermal growth factor receptor 2, and Ki-67 in breast cancer. Chin. Med. J. 2014, 127, 3272–3277. [Google Scholar]
- Finkelman, B.S.; Zhang, H.; Hicks, D.G.; Turner, B.M. The Evolution of Ki-67 and Breast Carcinoma: Past Observations, Present Directions, and Future Considerations. Cancers 2023, 15, 808. [Google Scholar] [CrossRef]
- Mh, R.; Gm, F. Neoadjuvant chemotherapy in the treatment of breast cancer. Surg. Clin. N. Am. 2013, 93, 493–499. [Google Scholar] [CrossRef]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.A.; Reynolds, K.L.; Smith, B.L.; Alexander, B.M.; Moy, B.; Isakoff, S.J.; et al. Pathological complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: A comprehensive meta-analysis. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Huang, C.-S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Han, D.; Wang, X.; Wang, Q.; Tian, J.; Yao, J.; Yuan, L.; Qian, K.; Zou, Q.; Yi, W.; et al. Prognostic values of Ki-67 in neoadjuvant setting for breast cancer: A systematic review and meta-analysis. Future Oncol. 2017, 13, 1021–1034. [Google Scholar] [CrossRef] [PubMed]
- Inwald, E.C.; Klinkhammer-Schalke, M.; Hofstädter, F.; Zeman, F.; Koller, M.; Gerstenhauer, M.; Ortmann, O. Ki-67 is a prognostic parameter in breast cancer patients: Results of a large population- based cohort of a cancer registry. Breast Cancer Res. Treat. 2013, 139, 539–552. [Google Scholar] [CrossRef]
- Milde-Langosch, K.; Karn, T.; Müller, V.; Witzel, I.; Rody, A.; Schmidt, M.; Wirtz, R.M. Validity of the proliferation markers Ki67, TOP2A, and RacGAP1 in molecular subgroups of breast cancer. Breast Cancer Res. Treat. 2013, 137, 57–67. [Google Scholar] [CrossRef]
- Amezcua-Gálvez, J.E.; Lopez-Garcia, C.A.; Villarreal-Garza, C.; Lopez-Rivera, V.; Canavati-Marcos, M.; Santuario-Facio, S.; Dono, A.; Monroig-Bosque, P.D.C.; Ortiz-López, R.; Leal-Lopez, A.; et al. Concordance between Ki-67 index in invasive breast cancer and molecular signatures: EndoPredict and MammaPrint. Mol. Clin. Oncol. 2022, 17, 132. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. Breast Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr Cancer Netw. JNCCN 2020, 18, 452–478. [Google Scholar] [CrossRef]
- Magnoni, F.; Galimberti, V.; Corso, G.; Intra, M.; Sacchini, V.; Veronesi, P. Axillary surgery in breast cancer: An updated historical perspective. Semin. Oncol. 2020, 47, 341–352. [Google Scholar] [CrossRef]
- Balic, M.; Thomssen, C.; Gnant, M.; St. Harbeck, N. Gallen/Vienna 2023: Optimization of Treatment for Patients with Primary Breast Cancer—A Brief Summary of the Consensus Discussion. Breast Care 2023, 18, 213–222. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Regan, M.; Aebi, S.; André, F.; Barrios, C.; Bergh, J.; Bonnefoi, H.; Morales, D.B.; Brucker, S.; Burstein, H.; Cameron, D.; et al. Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Van Nijnatten, T.J.A.; Simons, J.M.; Moossdorff, M.; De Munck, L.; Lobbes, M.B.I.; Van Der Pol, C.C.; Koppert, L.B.; Luiten, E.J.T.; Smidt, M.L. Prognosis of residual axillary disease after neoadjuvant chemotherapy in clinically node-positive breast cancer patients: Isolated tumor cells and micrometastases carry a better prognosis than macrometastases. Breast Cancer Res. Treat. 2017, 163, 159–166. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Ballman, K.; McCall, L.; Beitsch, P.; Whitworth, P.W.; Blumencranz, P.; Leitch, A.M.; Saha, S.; Morrow, M.; Hunt, K.K. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: Long-term follow-up from the american college of surgeons oncology group (Alliance) ACOSOG Z0011 Randomized Trial. Ann. Surg. 2016, 264, 413–420. [Google Scholar] [CrossRef]
- Tinterri, C.; Canavese, G.; Bruzzi, P.; Dozin, B. NEONOD 2: Rationale and design of a multicenter non-inferiority trial to assess the effect of axillary surgery omission on the outcome of breast cancer patients presenting only micrometastasis in the sentinel lymph node after neoadjuvant chemotherapy. Contemp. Clin. Trials Commun. 2019, 17, 100496. [Google Scholar] [CrossRef]
- Comparison of Axillary Lymph Node Dissection with Axillary Radiation for Patients with Node-Positive Breast Cancer Treated with Chemotherapy. ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01901094 (accessed on 2 July 2023).
- Weber, W.P.; Matrai, Z.; Hayoz, S.; Tausch, C.; Henke, G.; Zimmermann, F.; Montagna, G.; Fitzal, F.; Gnant, M.; Ruhstaller, T.; et al. Association of Axillary Dissection with Systemic Therapy in Patients with Clinically Node-Positive Breast Cancer. JAMA Surg. 2023, 158, 1013–1021. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Axillary Pathologic Complete Response After Neoadjuvant Systemic Therapy by Breast Cancer Subtype in Patients with Initially Clinically Node-Positive Disease: A Systematic Review and Meta-analysis. PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33881478/ (accessed on 20 August 2023).
- Houssami, N.; Macaskill, P.; von Minckwitz, G.; Marinovich, M.L.; Mamounas, E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur. J. Cancer 2012, 48, 3342–3354. [Google Scholar] [CrossRef]
- Teshome, M.; Hunt, K.K. Neoadjuvant therapy in the treatment of breast cancer. Surg. Oncol. Clin. N. Am. 2014, 23, 505. [Google Scholar] [CrossRef]
- Meyers, M.O.; Klauber-DeMore, N.; Ollila, D.W.; Amos, K.D.; Moore, D.T.; Drobish, A.A.; Burrows, E.M.; Dees, E.C.; Carey, L.A. Impact of breast cancer molecular subtypes on locoregional recurrence in patients treated with neoadjuvant chemotherapy for locally advanced breast cancer. Ann. Surg. Oncol. 2011, 18, 2851–2857. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SNLB | ALND | SNLB + ALND | TOT | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N° | % | N° | % | N° | % | N° | p-value | ||
| Patients | 90 | 33.1% | 179 | 65.8% | 3 | 1.1% | 272 | ||
| Period | P1 | 22 | 19.8% | 88 | 79.3% | 1 | 0.9% | 111 | 0.0002 |
| P2 | 68 | 42.2% | 91 | 56.5% | 2 | 1.2% | 161 | ||
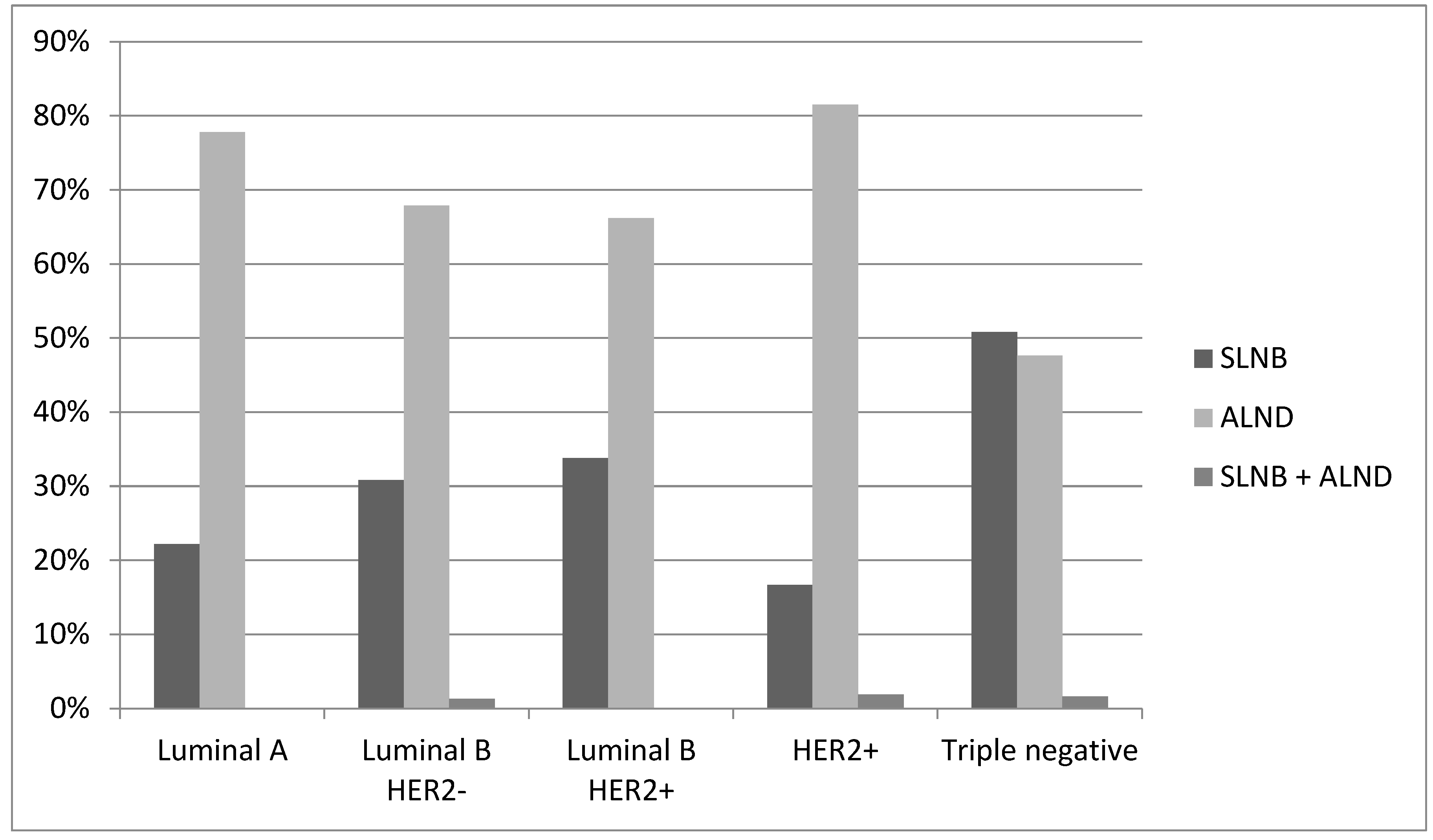
| Histotype | Luminal A | 2 | 22.2% | 7 | 77.8% | 0 | 0% | 9 | 0.0054 |
| Luminal B HER2− | 24 | 30.8% | 53 | 67.9% | 1 | 1.3% | 78 | ||
| Luminal B HER2+ | 23 | 33.8% | 45 | 66.2% | 0 | 0% | 68 | ||
| HER2+ | 9 | 16.7% | 44 | 81.5% | 1 | 1.9% | 54 | ||
| Triple negative | 32 | 50.8% | 30 | 47.6% | 1 | 1.6% | 63 | ||
| cN | cN0 | 86 | 78.9% | 20 | 18.3% | 3 | 2.8% | 109 | <0.0001 |
| cN1 | 4 | 3.2% | 121 | 96.8% | 0 | 0% | 125 | ||
| cN2 | 0 | 0% | 6 | 100% | 0 | 0% | 6 | ||
| cN3 | 0 | 0% | 32 | 100% | 0 | 0% | 32 | ||
| cT | cT1 | 23 | 38.3% | 37 | 61.7% | 0 | 0% | 60 | <0.0001 |
| cT2 | 61 | 38.6% | 95 | 60.1% | 2 | 1.3% | 158 | ||
| cT3 | 6 | 30% | 13 | 65% | 1 | 5% | 20 | ||
| cT4 | 0 | 0% | 31 | 100% | 0 | 0% | 31 | ||
| cTx | 0 | 0% | 3 | 100% | 0 | 0% | 3 | ||
| cN0 patients | 86 | 78.9% | 20 | 18.3% | 3 | 2.8% | 109 | ||
| Period | P1 | 22 | 71% | 8 | 25.8% | 1 | 3.2% | 31 | 0.4148 |
| P2 | 64 | 82.1% | 13 | 12% | 2 | 2.6% | 78 | ||
| Histotype | Luminal A | 2 | 66.7% | 1 | 33.3% | 0 | 0% | 3 | 0.5479 |
| Luminal B HER2− | 23 | 71.9% | 8 | 25% | 1 | 3.1% | 32 | ||
| Luminal B HER2+ | 22 | 88% | 4 | 16% | 0 | 0% | 25 | ||
| HER2+ | 9 | 64.3% | 3 | 21.4% | 1 | 7.1% | 14 | ||
| Triple negative | 30 | 81.1% | 4 | 10.8% | 1 | 2.7% | 37 | ||
| cT | cT1 | 23 | 92% | 2 | 8% | 0 | 0% | 25 | 0.0115 |
| cT2 | 59 | 77.6% | 14 | 18.4% | 2 | 2.6% | 76 | ||
| cT3 | 6 | 85.7% | 1 | 14.3% | 1 | 14.3% | 7 | ||
| cT4 | 0 | 0% | 3 | 100% | 0 | 0% | 3 | ||
| cTx | 0 | 0% | 0 | 0% | 0 | 0% | 0 |
| CI 95% | |||||
|---|---|---|---|---|---|
| SLNB vs. ALND | p-Value | OR | Inferior | Superior | |
| Histotype | Luminal A | 0.5096 | 3.11 | 0.11 | 90.54 |
| Luminal B HER2− | 1.00 (ref) | ||||
| Luminal B HER2+ | 0.4364 | 1.624 | 0.48 | 5.51 | |
| HER2 + | 0.519 | 0.64 | 0.17 | 2.47 | |
| Triple negative | 0.0957 | 2.91 | 0.83 | 10.25 | |
| cT | cT1 | 1.00 (ref) | |||
| cT2 | 0.7627 | 0.84 | 0.26 | 2.67 | |
| cT3 | 0.3525 | 0.43 | 0.07 | 2.58 | |
| cT4 | Ns | ||||
| cN | cN0 | 1.00 (ref) | |||
| cN ≥ 1 | <0.0001 | 0.01 | 0.00 | 0.02 | |
| Period | P1 | 1.00 (ref) | |||
| P2 | 0.2242 | 1.83 | 0.69 | 4.87 | |
| ypT0-is | ypT ≥ 1 | TOT | ||||
|---|---|---|---|---|---|---|
| N° | % | N° | % | N° | p-Value | |
| 39.7% | 164 | 60.3% | 272 | |||
| P1 | 108 | 34.2% | 73 | 65.8% | 111 | 0.1324 |
| P2 | 38 | 43.5% | 91 | 56.5% | 161 | |
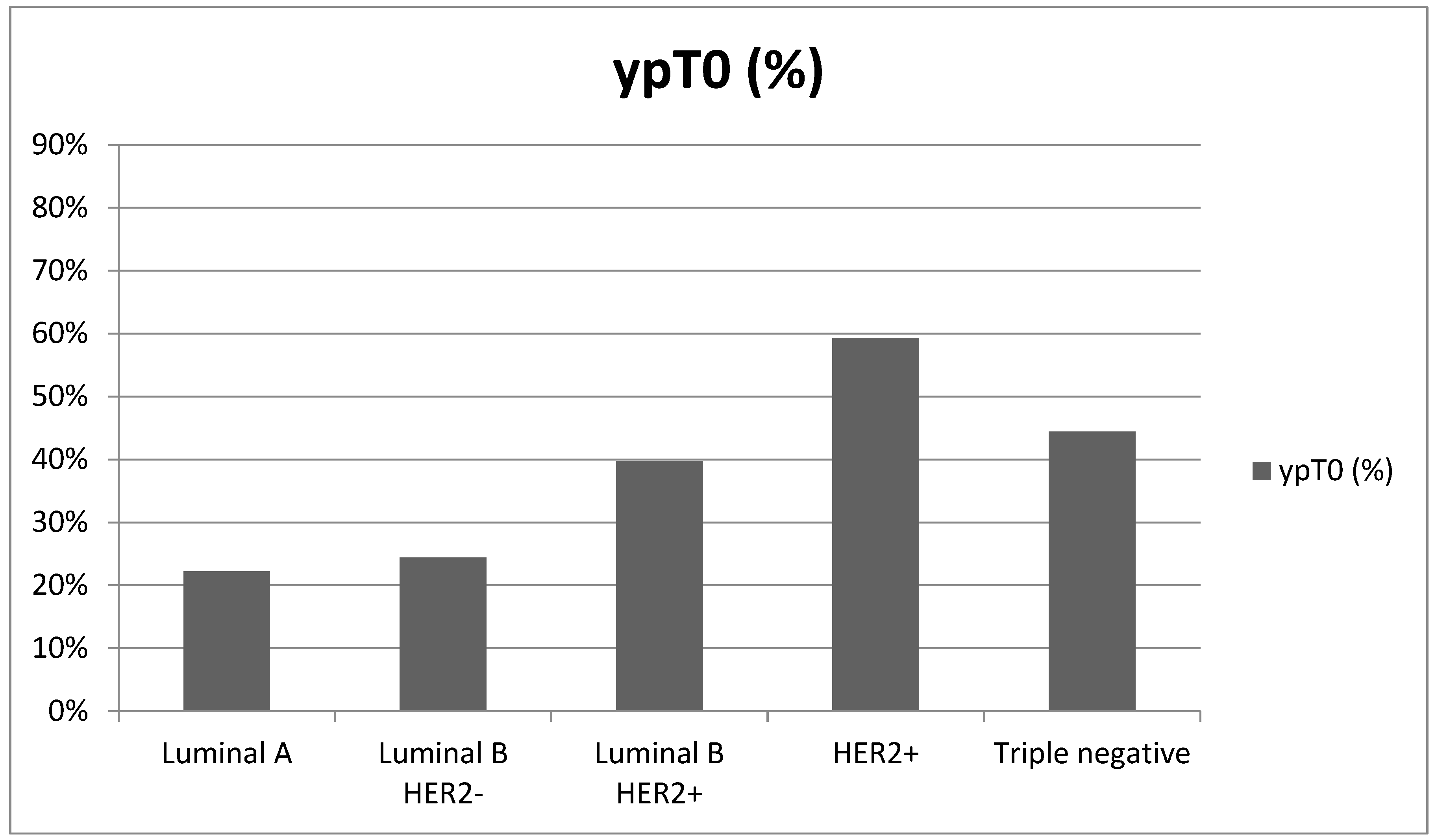
| Luminal A | 70 | 22.2% | 7 | 77.8% | 9 | 0.001 |
| Luminal B HER2− | 2 | 24.4% | 59 | 75.8% | 78 | |
| Luminal B HER2+ | 19 | 39.7% | 41 | 75.6% | 68 | |
| HER2+ | 27 | 59.3% | 22 | 60.3% | 54 | |
| Triple negative | 32 | 44.4% | 35 | 55.6% | 63 | |
| cT1 | 33 | 55.0% | 27 | 45.0% | 60 | 0.0096 |
| cT2 | 59 | 37.3% | 99 | 62.7% | 158 | |
| cT3 | 3 | 15.0% | 17 | 85.0% | 20 | |
| cT4 | 11 | 35.5% | 20 | 64.5% | 31 | |
| cTx | 2 | 36.7% | 1 | 33.3% | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiappa, C.; Greta, M.; Miriam, L.; Ietto, G.; Inversini, D.; Ballabio, A.; Bonetti, A.; Mangano, A.; Gueli, R.; Carcano, G.; et al. Neoadjuvant Chemotherapy in Breast Cancer: Evaluation of the Impact on Surgical Outcomes and Prognosis. Cancers 2024, 16, 2332. https://doi.org/10.3390/cancers16132332
Chiappa C, Greta M, Miriam L, Ietto G, Inversini D, Ballabio A, Bonetti A, Mangano A, Gueli R, Carcano G, et al. Neoadjuvant Chemotherapy in Breast Cancer: Evaluation of the Impact on Surgical Outcomes and Prognosis. Cancers. 2024; 16(13):2332. https://doi.org/10.3390/cancers16132332
Chicago/Turabian StyleChiappa, Corrado, Maltecca Greta, Leoni Miriam, Giuseppe Ietto, Davide Inversini, Andrea Ballabio, Alice Bonetti, Alberto Mangano, Rossana Gueli, Giulio Carcano, and et al. 2024. "Neoadjuvant Chemotherapy in Breast Cancer: Evaluation of the Impact on Surgical Outcomes and Prognosis" Cancers 16, no. 13: 2332. https://doi.org/10.3390/cancers16132332
APA StyleChiappa, C., Greta, M., Miriam, L., Ietto, G., Inversini, D., Ballabio, A., Bonetti, A., Mangano, A., Gueli, R., Carcano, G., & Rovera, F. A. (2024). Neoadjuvant Chemotherapy in Breast Cancer: Evaluation of the Impact on Surgical Outcomes and Prognosis. Cancers, 16(13), 2332. https://doi.org/10.3390/cancers16132332