
Nivolumab as Second-Line Therapy Improves Survival in Patients with Unresectable Hepatocellular Carcinoma

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Participants
2.2. Treatment Administration and Outcome Measures
2.3. Safety Analysis Endpoints
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients
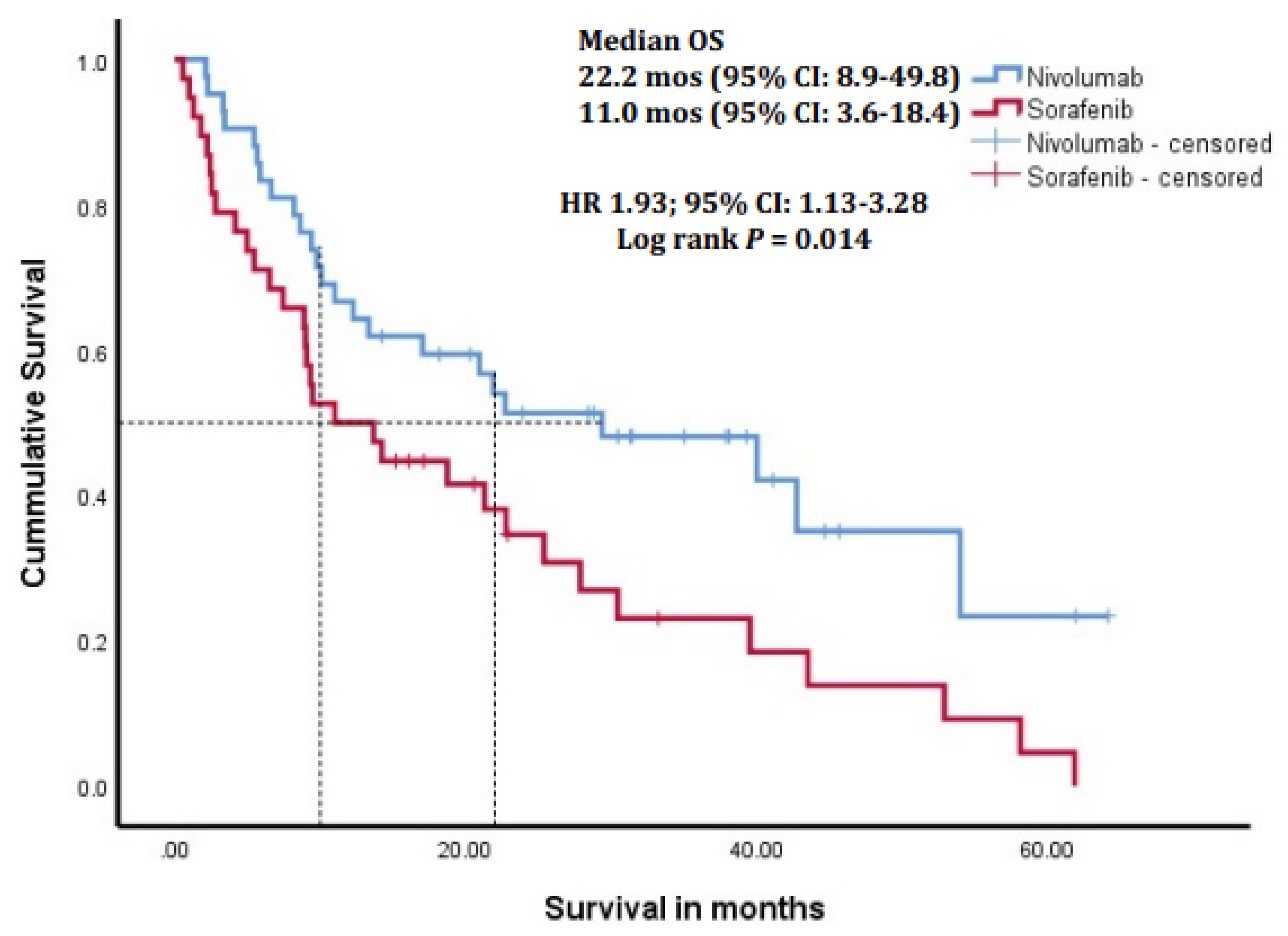
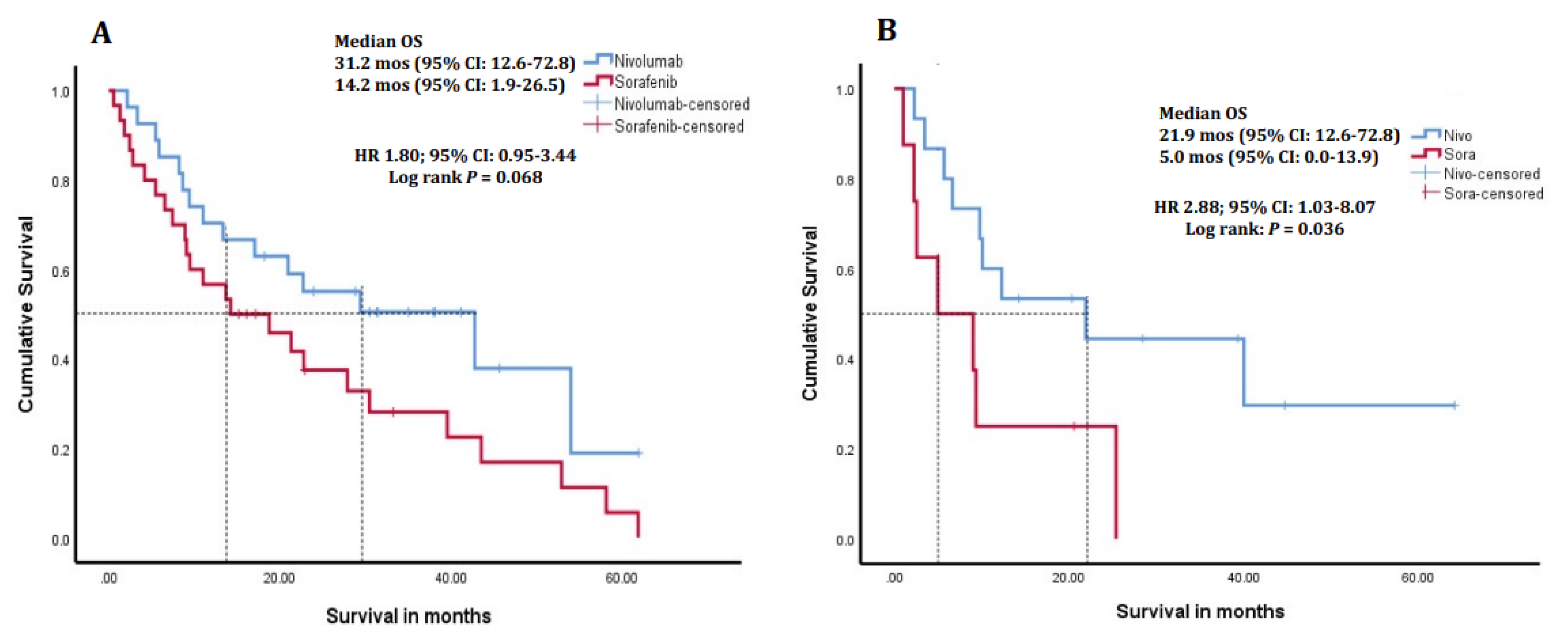
3.2. Treatment Outcomes and Survival
3.3. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bosch, F.X.; Ribes, J.; Borràs, J. Epidemiology of primary liver cancer. Semin. Liver Dis. 1999, 19, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.A.; Sanai, F.M.; Alolayan, A.; Abaalkhail, F.; Alsuhaibani, H.; Hassanain, M.; Alhazzani, W.; Alsuhaibani, A.; Algarni, A.; Forner, A.; et al. Saudi Association for the Study of Liver diseases and Transplantation practice guidelines on the diagnosis and management of hepatocellular carcinoma. Saudi J. Gastroenterol. 2020, 26 (Suppl. S1), S1–S40. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Peck-Radosavljevic, M. Review article: Systemic treatment of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2018, 48, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H., 3rd; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Li, L.; Guo, B.; Liu, D.; Shi, J.; Wu, C.; Chen, J.; Zhang, X.; Wu, J. Mechanisms of resistance to chemotherapy and radiotherapy in hepatocellular carcinoma. Transl. Cancer Res. 2018, 7, 765–781. [Google Scholar] [CrossRef]
- Pinato, D.J.; Guerra, N.; Fessas, P.; Murphy, R.; Mineo, T.; Mauri, F.A.; Mukherjee, S.K.; Thursz, M.; Wong, C.N.; Sharma, R.; et al. Immune-based therapies for hepatocellular carcinoma. Oncogene 2020, 39, 3620–3637. [Google Scholar] [CrossRef]
- Greten, T.F.; Wang, X.W.; Korangy, F. Current concepts of immune based treatments for patients with HCC: From basic science to novel treatment approaches. Gut 2015, 64, 842–848. [Google Scholar] [CrossRef]
- Hato, T.; Goyal, L.; Greten, T.F.; Duda, D.G.; Zhu, A.X. Immune checkpoint blockade in hepatocellular carcinoma: Current progress and future directions. Hepatology 2014, 60, 1776–1782. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Ngiow, S.F.; Ribas, A.; Teng, M.W. Combination cancer immunotherapies tailored to the tumour microenvironment. Nat. Rev. Clin. Oncol. 2016, 13, 143–158. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.; Shi, M.; Zeng, Z.; Qi, R.Z.; Liu, Z.W.; Zhang, J.Y.; Yang, Y.P.; Tien, P.; Wang, F.S. PD-1 and PD-L1 upregulation promotes CD8+ T-cell apoptosis and postoperative recurrence in hepatocellular carcinoma patients. Int. J. Cancer 2011, 128, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Harding, J.J.; Merle, P.; Rosmorduc, O.; et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): A randomized, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022, 23, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Scheiner, B.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Schulze, K.; von Felden, J.; Fründt, T.W.; Stadler, M.; Heinzl, H.; Shmanko, K.; et al. Programmed cell death protein-1 (PD-1)-targeted immunotherapy in advanced hepatocellular carcinoma: Efficacy and safety data from an international multicentre real-world cohort. Aliment. Pharmacol. Ther. 2019, 49, 1323–1333. [Google Scholar] [CrossRef]
- Finkelmeier, F.; Czauderna, C.; Perkhofer, L.; Ettrich, T.J.; Trojan, J.; Weinmann, A.; Marquardt, J.U.; Vermehren, J.; Waidmann, O. Feasibility and safety of nivolumab in advanced hepatocellular carcinoma: Real-life experience from three German centers. J. Cancer Res. Clin. Oncol. 2019, 145, 253–259. [Google Scholar] [CrossRef]
- Choi, W.M.; Lee, D.; Shim, J.H.; Kim, K.M.; Lim, Y.S.; Lee, H.C.; Yoo, C.; Park, S.R.; Ryu, M.H.; Ryoo, B.Y.; et al. Effectiveness and Safety of Nivolumab in Child–Pugh B Patients with Hepatocellular Carcinoma: A Real-World Cohort Study. Cancers 2020, 12, 1968. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Lee, Y.B.; Kim, M.A.; Jang, H.; Oh, H.; Kim, S.W.; Cho, E.J.; Lee, K.H.; Lee, J.H.; Yu, S.J.; et al. Effectiveness of nivolumab versus regorafenib in hepatocellular carcinoma patients who failed sorafenib treatment. Clin. Mol. Hepatol. 2020, 26, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Fessas, P.; Kaseb, A.; Wang, Y.; Saeed, A.; Szafron, D.; Jun, T.; Dharmapuri, S.; Rafeh Naqash, A.; Muzaffar, M.; Navaid, M.; et al. Post-registration experience of nivolumab in advanced hepatocellular carcinoma: An international study. J. Immunother. Cancer 2020, 8, e001033. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kudo, M.; Venook, A.P.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.H.; de Guevara, L.L.; et al. Observational registry of sorafenib use in clinical practice across Child-Pugh subgroups: The GIDEON study. J. Hepatol. 2016, 65, 1140–1147. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Lee, Y.H.; Hsia, C.Y.; Huang, Y.H.; Su, C.W.; Lin, H.C.; Lee, R.C.; Chiou, Y.Y.; Lee, F.Y.; Huo, T.I. Performance status in patients with hepatocellular carcinoma: Determinants, prognostic impact, and ability to improve the Barcelona Clinic Liver Cancer system. Hepatology 2013, 57, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, T.; Kawabe, N.; Ariga, M.; Ohno, E.; Funasaka, K.; Nagasaka, M.; Nakagawa, Y.; Miyahara, R.; Shibata, T.; Takahara, T.; et al. Clinical Outcomes of Cabozantinib in Patients Previously Treated with Atezolizumab/Bevacizumab for Advanced Hepatocellular Carcinoma-Importance of Good Liver Function and Good Performance Status. Cancers 2023, 15, 2952. [Google Scholar] [CrossRef]
- Giannini, E.G.; Bucci, L.; Garuti, F.; Brunacci, M.; Lenzi, B.; Valente, M.; Caturelli, E.; Cabibbo, G.; Piscaglia, F.; Virdone, R.; et al. Patients with advanced hepatocellular carcinoma need a personalized management: A lesson from clinical practice. Hepatology 2018, 67, 1784–1796. [Google Scholar] [CrossRef]
- Finn, R.S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Gerolami, R.; Caparello, C.; et al. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: Additional analyses from the phase III RESORCE trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Lenvatinib as Second-Line Treatment after Atezolizumab Plus Bevacizumab for Unresectable Hepatocellular Carcinoma: Clinical Results Show Importance of Hepatic Reserve Function. Oncology 2023, 101, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Ohama, H.; Hiraoka, A.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; Fukunishi, S.; et al. Comparison between Atezolizumab Plus Bevacizumab and Lenvatinib for Hepatocellular Carcinoma in Patients with Child-Pugh Class B in Real-World Clinical Settings. Oncology 2023, 101, 542–552. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Cheng, A.L.; Zhu, A.X.; Ducreux, M.; Galle, P.R.; Sakamoto, N.; Kato, N.; Nakano, M.; Jia, J.; et al. Albumin-Bilirubin Grade Analyses of Atezolizumab Plus Bevacizumab versus Sorafenib in Patients with Unresectable Hepatocellular Carcinoma: A Post Hoc Analysis of the Phase III IMbrave150 Study. Liver Cancer 2023, 12, 479–493. [Google Scholar] [CrossRef]
- Gadaleta, R.M.; Moschetta, A. Dark and bright side of targeting fibroblast growth factor receptor 4 in the liver. J. Hepatol. 2021, 75, 1440–1451. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Galle, P.R.; Zhu, A.X.; Ducreux, M.; Cheng, A.L.; Ikeda, M.; Tsuchiya, K.; Aoki, K.I.; Jia, J.; et al. IMbrave150: Efficacy and Safety of Atezolizumab plus Bevacizumab Versus Sorafenib in Patients with Barcelona Clinic Liver Cancer Stage B Unresectable Hepatocellular Carcinoma: An Exploratory Analysis of the Phase III Study. Liver Cancer 2022, 12, 238–250. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, D.; Zhao, B.; Ren, L.; Huang, R.; Feng, B.; Chen, H. The predictive value of PD-L1 expression in patients with advanced hepatocellular carcinoma treated with PD-1/PD-L1 inhibitors: A systematic review and meta-analysis. Cancer Med. 2023, 12, 9282–9292. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 80) | Sorafenib (n = 38) | Nivolumab (n = 42) | p |
|---|---|---|---|---|
| Age (yrs) | 72.4 ± 10.1 | 75.0 ± 9.8 | 70.0 ± 9.8 | 0.024 |
| Male gender | 70 (87.5) | 34 (89.5) | 36 (85.7) | 0.74 |
| BMI (kg/m2) | 25.4 ± 5.4 | 25.7 ± 6.0 | 25.2 ± 4.9 | 0.69 |
| Comorbidities | ||||
| Diabetes | 24 (30.0) | 5 (13.2) | 19 (45.2) | 0.002 |
| Hypertension | 24 (30.0) | 6 (15.8) | 18 (42.9) | 0.008 |
| CKD | 5 (6.3) | 0 (0.0) | 5 (11.9) | 0.06 |
| Cardiac disease | 5 (6.3) | 2 (5.3) | 3 (7.1) | 1.00 |
| ECOG | ||||
| PS 0–1 | 65 (81.3) | 32 (84.2) | 33 (78.6) | 0.52 |
| PS 2–3 | 15 (18.8) | 6 (15.8) | 9 (21.4) | |
| AFP (ng/mL) | 41.4 (6–1501) | 28.9 (6.3–790.2) | 50.6 (6.0–2670.0) | 0.82 |
| <400 | 52 (65.0) | 26 (68.4) | 26 (61.9) | 0.54 |
| ≥400 | 28 (35.0) | 12 (31.6) | 16 (38.1) | |
| Etiology | ||||
| HBV | 27 * (33.8) | 16 * (42.1) | 11 (26.2) | 0.13 |
| HCV | 20 * (25.0) | 10 * (26.3) | 10 (23.8) | 0.80 |
| Non-viral | 34 (42.5) | 13 (34.2) | 21 (50.0) | 0.15 |
| CTP class A/B | 57 (71.3)/23 (28.8) | 30 (78.9)/8 (21.1) | 27 (64.3)/15 (35.7) | 0.15 |
| BCLC stage B/C | 28 (35)/52 (65) | 20 (52.6)/18 (47.4) | 8 (19.0)/34 (81.0) | 0.002 |
| PV thrombosis | 36 (45.0) | 16 (42.1) | 20 (47.6) | 0.62 |
| Metastases | 31 (38.8) | 8 (21.1) | 23 (54.8) | 0.002 |
| Hepatic decompensation | ||||
| Variceal bleeding | 9 (11.3) | 4 (10.5) | 5 (11.9) | 1.00 |
| Ascites | 12 (15.0) | 5 (13.2) | 7 (16.7) | 0.66 |
| PSE | 3 ** (3.8) | 1 ** (2.6) | 2 ** (4.8) | 1.00 |
| Creatinine | 81.0 ± 33.7 | 76.7 ± 17.8 | 84.9 ± 43.2 | 0.28 |
| Variable | Total (n = 57) | Sorafenib (n = 30) | Nivolumab (n = 27) | p |
|---|---|---|---|---|
| Age (yrs) | 74.9 ± 8.8 | 76.6 ± 9.8 | 73.0 ± 7.2 | 0.13 |
| Male gender | 51 (89.5) | 27 (90.0) | 24 (88.9) | 0.89 |
| Comorbidities | ||||
| Diabetes | 14 (24.6) | 4 (13.3) | 10 (37.0) | 0.038 |
| Hypertension | 16 (28.1) | 11 (40.7) | 5 (16.7) | 0.043 |
| CKD | 3 (5.3) | 0 (0) | 3 (11.1) | 0.06 |
| Cardiac disease | 3 (5.3) | 2 (6.7) | 1 (3.7) | 0.62 |
| ECOG | ||||
| PS 0–1 | 46 (80.7) | 26 (86.7) | 20 (74.1) | 0.23 |
| PS 2–3 | 11 (19.3) | 4 (13.3) | 7 (25.9) | |
| AFP (ng/mL) | 55.5 (6.2–4058) | 28.9 (6.8–688.2) | 690.2 (6–16480) | 0.99 |
| <400 | 34 (59.6) | 21 (70.0) | 13 (48.1) | 0.09 |
| ≥400 | 23 (40.4) | 9 (30.0) | 14 (51.9) | |
| Etiology | ||||
| HBV | 20 * (35.1) | 12 * (40.0) | 8 (29.6) | 0.41 |
| HCV | 11 * (19.3) | 6 * (20.0) | 5 (18.5) | 0.89 |
| Non-viral | 27 (47.4) | 13 (43.3) | 14 (51.9) | 0.52 |
| BCLC stage B/C | 20(35)/37(65) | 15 (50)/15(50) | 5 (18.5)/22 (81.5) | 0.013 |
| PV thrombosis | 27 (47.7) | 13 (43.3) | 14 (51.9) | 0.52 |
| Metastases | 24 (42.1) | 7 (21.3) | 17 (63.0) | 0.002 |
| Variceal bleeding | 6 (10.5) | 3 (11.1) | 3 (10.0) | 0.89 |
| PSE | 2 ** (3.5) | 1 ** (3.7) | 1 ** (3.3) | 0.94 |
| Creatinine | 79.6 ± 27.4 | 76.2 ± 16.2 | 84.4 ± 36.1 | 0.33 |
| Variable | Total (n = 28) | Sorafenib (n = 20) | Nivolumab (n = 8) | p |
|---|---|---|---|---|
| Age (yrs) | 72.7 ± 9.0 | 74.6 ± 8.9 | 64.9 ± 8.9 | 0.07 |
| Male gender | 23 (82.1) | 17 (85.0) | 6 (75.0) | 0.53 |
| Comorbidities | ||||
| Diabetes | 9 (32.1) | 4 (20.0) | 5 (62.5) | 0.07 |
| Hypertension | 9 (32.1) | 4 (20.0) | 5 (62.5) | 0.07 |
| CKD | 1 (3.6) | 0 (0) | 1 (12.5) | 0.29 |
| Cardiac disease | 2 (7.1) | 1 (5.0) | 1 (12.5) | 0.50 |
| ECOG | ||||
| PS 0–1 | 26 (92.9) | 18 (90.0) | 8 (100) | 1.00 |
| PS 2–3 | 2 (7.1) | 2 (10.0) | 0 (0) | |
| AFP (ng/mL) | 9.2 (6.0–611.7) | 9.2 (6.0–848.7) | 10.8 (6.0–42.5) | 0.36 |
| <400 | 21 (75.0) | 14 (70.0) | 7 (87.5) | 0.63 |
| ≥400 | 7 (25.0) | 6 (30.0) | 1 (12.5) | |
| Etiology | ||||
| HBV | 7 (25.0) | 6 (30.0) | 1 (12.5) | 0.63 |
| HCV | 6 (21.4) | 4 (20.0) | 2 (25.0) | 1.00 |
| Non-viral | 15 (53.6) | 10 (50.0) | 5 (62.5) | 0.69 |
| CTP class A/B | 20 (71.4)/8 (28.6) | 15 (75)/5 (25) | 5 (62.5)/3 (37.5) | 0.65 |
| Hepatic decompensation | ||||
| Variceal bleeding | 4 (14.3) | 2 (10.0) | 2 (25.0) | 0.56 |
| Ascites | 3 (10.7) | 3 (15.0) | 0 (0) | 0.54 |
| PSE | 0 (0) | - | - | - |
| Creatinine | 81.7 ± 32.2 | 79.7 ± 19.1 | 86.8 ± 54.4 | 0.61 |
| Tumor Response | Sorafenib (n = 38) | Nivolumab (n = 42) | p |
|---|---|---|---|
| Stable disease | 13 (34.2) | 10 (23.8) | 0.409 |
| Partial response | 3 (7.9) | 1 (2.4) | |
| Progressive disease | 14 (36.8) | 18 (42.9) | |
| Not evaluable | 2 (5.3) | 3 (7.1) | |
| Missing | 6 (15.8) | 10 (23.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanai, F.M.; Odah, H.O.; Alshammari, K.; Alzanbagi, A.; Alsubhi, M.; Tamim, H.; Alolayan, A.; Alshehri, A.; Alqahtani, S.A. Nivolumab as Second-Line Therapy Improves Survival in Patients with Unresectable Hepatocellular Carcinoma. Cancers 2024, 16, 2196. https://doi.org/10.3390/cancers16122196
Sanai FM, Odah HO, Alshammari K, Alzanbagi A, Alsubhi M, Tamim H, Alolayan A, Alshehri A, Alqahtani SA. Nivolumab as Second-Line Therapy Improves Survival in Patients with Unresectable Hepatocellular Carcinoma. Cancers. 2024; 16(12):2196. https://doi.org/10.3390/cancers16122196
Chicago/Turabian StyleSanai, Faisal M., Hassan O. Odah, Kanan Alshammari, Adnan Alzanbagi, Murooj Alsubhi, Hani Tamim, Ashwaq Alolayan, Ahmed Alshehri, and Saleh A. Alqahtani. 2024. "Nivolumab as Second-Line Therapy Improves Survival in Patients with Unresectable Hepatocellular Carcinoma" Cancers 16, no. 12: 2196. https://doi.org/10.3390/cancers16122196
APA StyleSanai, F. M., Odah, H. O., Alshammari, K., Alzanbagi, A., Alsubhi, M., Tamim, H., Alolayan, A., Alshehri, A., & Alqahtani, S. A. (2024). Nivolumab as Second-Line Therapy Improves Survival in Patients with Unresectable Hepatocellular Carcinoma. Cancers, 16(12), 2196. https://doi.org/10.3390/cancers16122196