Simple Summary
This study seeks to assess the efficacy of bevacizumab (BVZ) in the context of glioblastoma treatment, with a particular focus on the identification of a predictive biomarker, rCBVmax. The findings indicate that BVZ demonstrates marked benefits for patients with moderately vascularized tumors, resulting in a substantially extended median survival after tumor progression compared to those who do not receive second-line treatment. The proposed utilization of rCBVmax as a biomarker has the potential to enable personalized treatment decisions, enhancing patient outcomes by guiding the selection of optimal therapy. Additionally, the establishment of a threshold at 7.5 for categorizing patients based on tumor vascularity presents a more refined approach to the selection of second-line treatments. This research holds promise for improving the management of glioblastoma and optimizing treatment strategies for individual patients.
Abstract
Background: Aberrant vascular architecture and angiogenesis are hallmarks of glioblastoma IDH-wildtype, suggesting that these tumors are suitable for antiangiogenic therapy. Bevacizumab was FDA-approved in 2009 following promising results in two clinical trials. However, its use for recurrent glioblastomas remains a subject of debate, as it does not universally improve patient survival. Purposes: In this study, we aimed to analyze the influence of tumor vascularity on the benefit provided by BVZ and propose preoperative rCBVmax at the high angiogenic tumor habitat as a predictive biomarker to select patients who can benefit the most. Methods: Clinical and MRI data from 106 patients with glioblastoma IDH-wildtype have been analyzed. Thirty-nine of them received BVZ, and the remaining sixty-seven did not receive a second-line treatment. The ONCOhabitats method was used to automatically calculate rCBV. Results: We found a median survival from progression of 305 days longer for patients with moderate vascular tumors who received BVZ than those who did not receive any second-line treatment. This contrasts with patients with high-vascular tumors who only presented a median survival of 173 days longer when receiving BVZ. Furthermore, better responses to BVZ were found for the moderate-vascular group with a higher proportion of patients alive at 6, 12, 18, and 24 months after progression. Conclusions: We propose rCBVmax as a potential biomarker to select patients who can benefit more from BVZ after tumor progression. In addition, we propose a threshold of 7.5 to stratify patients into moderate- and high-vascular groups to select the optimal second-line treatment.
1. Introduction
The robust angiogenesis and abnormal vasculature in glioblastoma IDH-wildtype (GBM) are defining features of these highly aggressive gliomas [1,2,3,4,5,6]. GBMs represent the most lethal central nervous system (CNS) tumors in adults [7,8]. However, characterizing their vascularity presents significant challenges due to their heterogeneity at both intratumoral [4,5,6,9,10,11,12] and interpatient [10,13,14] levels. Moreover, this vascular heterogeneity in glioblastomas is further accentuated by tumor dynamics, resulting in significant variations in vascularity between newly diagnosed and recurrent glioblastomas [3].
To determine tumor vascularization profiles in a non-invasive manner at an early stage, magnetic resonance imaging (MRI) and dynamic susceptibility contrast (DSC) play a vital role [15]. MRI-DSC provides valuable insights into the microvascular characteristics of brain tumors and encompasses crucial parameters, like blood volume and flow, proving invaluable in diagnosis and treatment planning [16,17]. It also aids in determining tumor grade, distinguishing between tumor recurrence and radiation necrosis, and assessing treatment responses [18,19]. Multiple studies consistently show a strong connection between measurements of relative cerebral blood volume (rCBV) and microvascular structures in various types of glioma tumors [9,11,13,14,15].
The significance of vascularity in tumors is rooted in their imperative need for a continuous supply of nutrients and oxygen to fuel their relentless growth [4,5,6,10]. Tumors endowed with an extensive blood supply tend to exhibit accelerated and more aggressive growth patterns [20,21], which, in turn, are associated with poorer prognoses—a correlation well-documented in the literature [22,23,24,25,26,27]. It is no wonder that tumor vascularity has garnered substantial attention in drug development over recent decades [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. This pursuit was ignited by the underwhelming outcomes observed with cytotoxic agents. Additionally, GBMs’ rapid vascularization makes them promising for antiangiogenic therapy research.
The go-to antiangiogenic agent for glioblastomas is bevacizumab (BVZ), which received approval in the US BVZ, approved by the FDA in 2009 for recurrent tumor treatment, is a monoclonal antibody that inhibits VEGFR-mediated signaling by binding to VEGF-A. Early studies on recurrent GBMs showed response rates of 28–40% and 6-month progression-free survival rates of 40-50%, a notable improvement compared to prior studies with a median PFS6 of only 15% in recurrent GBMs [28,29,30,31,32]. Encouraged by initial success, multiple trials since 2009 show BVZ benefits in progression-free survival (PFS) but not in overall survival (OS) [28,29,30,31,32]. This disparity raises questions about its utility in primary GBMs. However, the use of this antiangiogenic therapy may prove advantageous as a second-line treatment for specific patient groups characterized by particular tumor vascularity profiles.
Given the vast spectrum of neovascularization processes in GBMs [43,44,45,46], a comprehensive analysis of various vascular patterns becomes imperative when deciding on the most appropriate treatment strategy. Moreover, the ongoing debate surrounding the utility of BVZ in Europe [28,29,30,31,32] underscores the need for a more personalized approach, as it is becoming increasingly clear that not all patients are ideal candidates for antiangiogenic treatment.
Our study is dedicated to identifying a subset of glioblastoma IDH-wildtype patients who could derive substantial benefits from BVZ treatment through the establishment of a preoperative selection criterion. Our key objectives include (1) proposing preoperative rCBV as a valuable biomarker to stratify patients with glioblastoma IDH-wildtype into distinct vascular groups; (2) contrasting the responses to bevacizumab between patient groups with moderate- and high-vascular glioblastoma IDH-wildtype; and (3) determining the vascular subgroup of patients that could reap the maximum benefits from bevacizumab treatment.
2. Material and Methods
2.1. Cohort Description
This study enrolled a cohort of 106 patients diagnosed with GBM IDH-wildtype [3]. These patients were selected from the extensive GLIOCAT database [47], which consists of individuals from six prominent healthcare centers in Cataluña, Spain. The participating centers included (1) Instituto Catalán de Oncología (ICO) de Badalona (Barcelona), (2) Hospital del Mar (Barcelona), (3) Hospital Clínic (Barcelona), (4) ICO Hospitalet (Barcelona), (5) ICO Girona (Girona), and (6) Hospital Sant Pau (Barcelona). A material transfer agreement was approved by all the participating centers, accompanied by an acceptance report issued by the Ethical Committee of each institution. The inclusion criteria for this study were meticulously defined, necessitating that patients meet the following conditions:
Histopathological confirmation of GBM IDH-wildtype, with diagnoses falling between June 2007 and May 2015.
Accessibility of complete MRI studies at the presurgical stage, including pre- and post-gadolinium, T1-weighted and T2-weighted Fluid-Attenuated Inversion Recovery (FLAIR), and dynamic susceptibility contrast (DSC) T2*-weighted perfusion sequences.
- Inclusion in one of two cohorts: the BVZ cohort (comprising patients treated with bevacizumab after tumor progression) or the control cohort (consisting of patients who did not receive additional treatment after tumor progression);
- A minimum survival period of 30 days;
- Compliance with the standard Stupp treatment protocol.
The study employed the RANO criteria to define tumor progression [47]. Patients who were still alive at the time of data analysis were considered as censored observations. The date of censorship was determined as the last contact date with the patient, or if such information was unavailable, the date of the most recent MRI examination.
2.2. Magnetic Resonance Imaging (MRI)
Prior to surgery, each patient underwent standard-of-care MR examinations, which encompassed a pre- and post-gadolinium-based contrast agent-enhanced T1-weighted MRI, as well as T2-weighted FLAIR and DSC T2* perfusion MRI scans. A sole set of DSC-MRI images, obtained within a single imaging session, were utilized to compute the relative cerebral blood volume (rCBV) for individual patients (refer to Figure S1 in the Supplementary Materials).
2.3. MRI Processing and rCBV Calculation
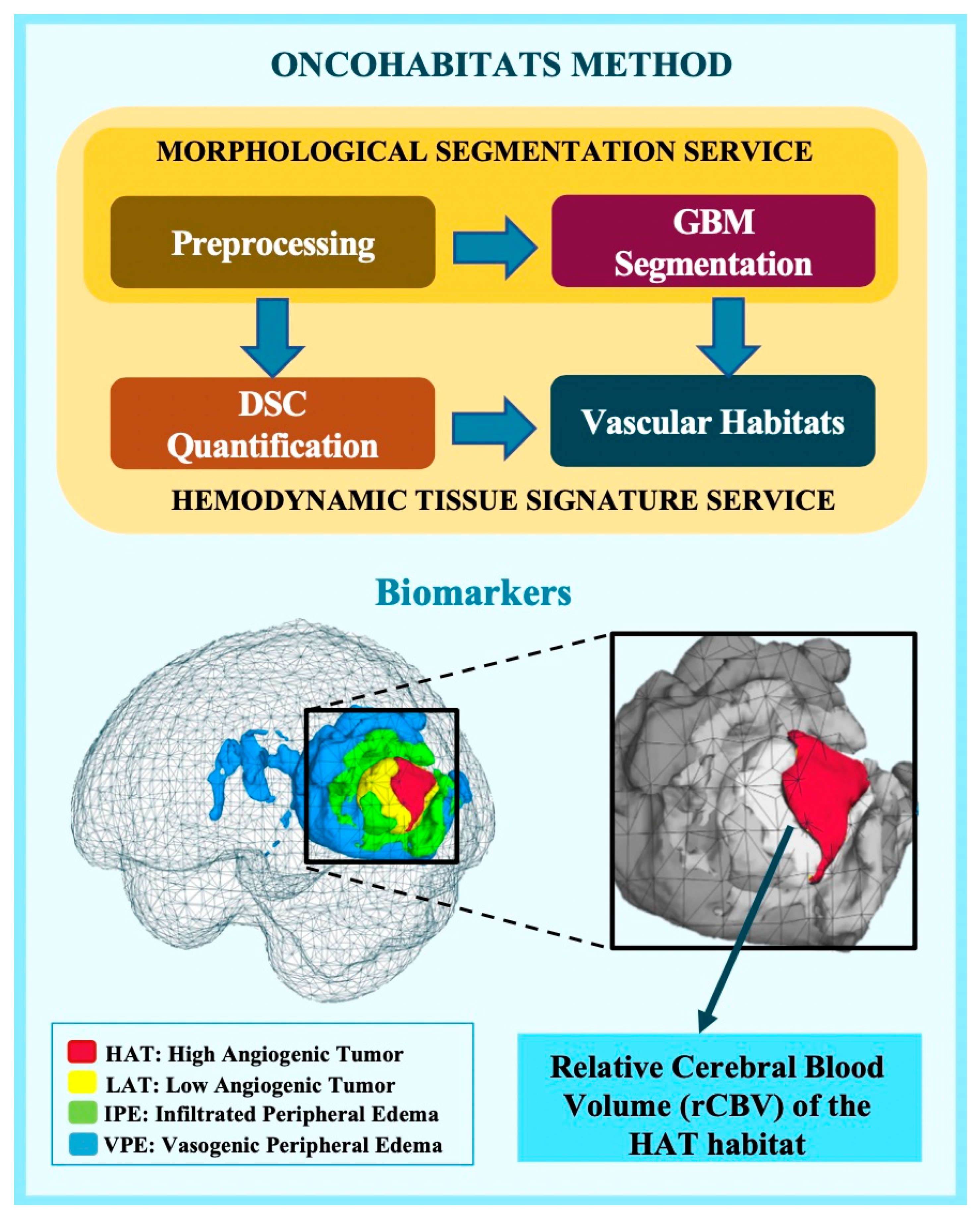
To process the MRI data and compute vascular markers, we utilized ONCOhabitats [18] (www.oncohabitats.upv.es, accessed on 1 July 2022), an automated unsupervised method designed to characterize the heterogeneity of enhancing tumor and edema tissues at both morphological and vascular levels while deriving vascular biomarkers. This method consists of four key stages (Figure 1):
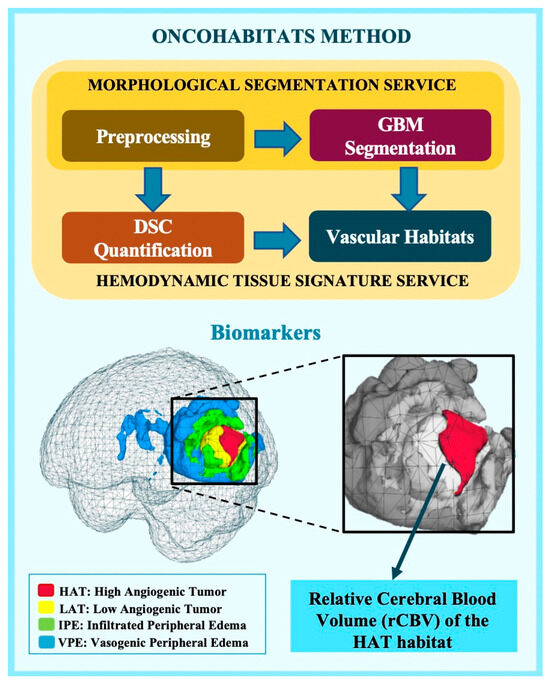
Figure 1.
Schematic representation of the ONCOhabitats method, which encompasses four key stages: 1. pre-processing of morphological MRIs (T1, T1c, T2, and flair); 2. segmentation of glioblastoma tissue; 3. quantification of DSC perfusion; and 4. establishment of HTS vascular habitats, including HAT (High Angiogenic Tumor), LAT (Low Angiogenic Tumor), IPE (Infiltrated Peripheral Edema), and VPE (Vasogenic Peripheral Edema). MRI biomarkers, such as the relative cerebral blood volume (rCBV), are obtained from each vascular habitat.
1. MRI Pre-processing: This phase includes voxel isotropic resampling of all MR images, correction of magnetic field inhomogeneities and noise, rigid intra-patient MRI registration, and skull stripping;
2. Tissue segmentation of glioblastomas: Achieved through an unsupervised segmentation method that employs a state-of-the-art deep learning 3D convolutional neural network (CNN), taking T1c, T2, and FLAIR MRIs as inputs;
3. DSC perfusion quantification: In this stage, we compute biomarkers like rCBV maps, relative cerebral blood flow (rCBF), or Mean Transit Time (MTT) for each patient. T1-weighted leakage effects are automatically corrected using the Boxerman method, while gamma-variate curve fitting corrects for the T2 extravasation phase. rCBV maps are generated by numerically integrating the area under the gamma-variate curve;
4. Hemodynamic Tissue Signature (HTS) habitats: The HTS provides an automated unsupervised method to characterize the heterogeneity of enhancing tumor and edema tissues in terms of the angiogenic process within these regions. Four sub-compartments for GBM are identified: two within the active tumor, High Angiogenic Tumor habitat (HAT) and Low Angiogenic Tumor habitat (LAT), and two within the edema, Infiltrated Peripheral Edema habitat (IPE) and Vasogenic Peripheral Edema habitat (VPE).
For a more in-depth understanding of the ONCOhabitats method, please refer to [7,19]. The method’s multisite robustness and prognostic capability were validated in an international multicenter study, and the results were published in [8].
2.4. rCBV Threshold to Define Vascular Groups
To stratify patients according to tumor vascularity, we used the maximum relative cerebral blood volume (rCBVmax) calculated at the HAT habitat (Figure 1) since our previous studies shown it to be the most relevant prognostic marker calculated with the ONCOhabitats method, and it was used in previous studies to define the vascular groups [7,8,25,45]. The optimum cutoff threshold was determined by the C-index method [8,13].
2.5. Statistical Analyses
2.5.1. Dataset Description: Distinctions between Moderate- and High-Vascularity Groups
We provided a comprehensive overview of key demographic, clinical, and molecular factors for the complete cohort and for the stratified groups, specifically the moderate-vascular and high-vascular groups, as well as those who received BVZ second-line treatment and those in the control group. The variables examined for each subgroup included gender, age at diagnosis, overall survival duration, extent of tumor resection, and MGMT methylation status.
2.5.2. Analysis of Survival Differences among Groups
First, to analyze the global benefit of providing BVZ for the entire cohort and then each vascular group, Kaplan–Meier curves were performed. In this analysis, we assessed differences in survival from tumor progression to exitus depending on whether BVZ was provided, and tumor vascularity. A log-rank test was used to determine any statistical differences between the estimated survival functions of the vascular populations. The number of patients included in each group, the median survival times from the progression of each group, the differential survival times, and the p-values are reported.
2.5.3. Comparison of Responses to BVZ between Vascular Groups
To compare the response to BVZ between the two vascular groups, basic metrics related to survival were defined. We compared the proportions of patients from each group with survival from tumor progression at 3, 6, 12, 18, and 24 months.
3. Results
3.1. Benefit of Providing BVZ for the Entire Cohort
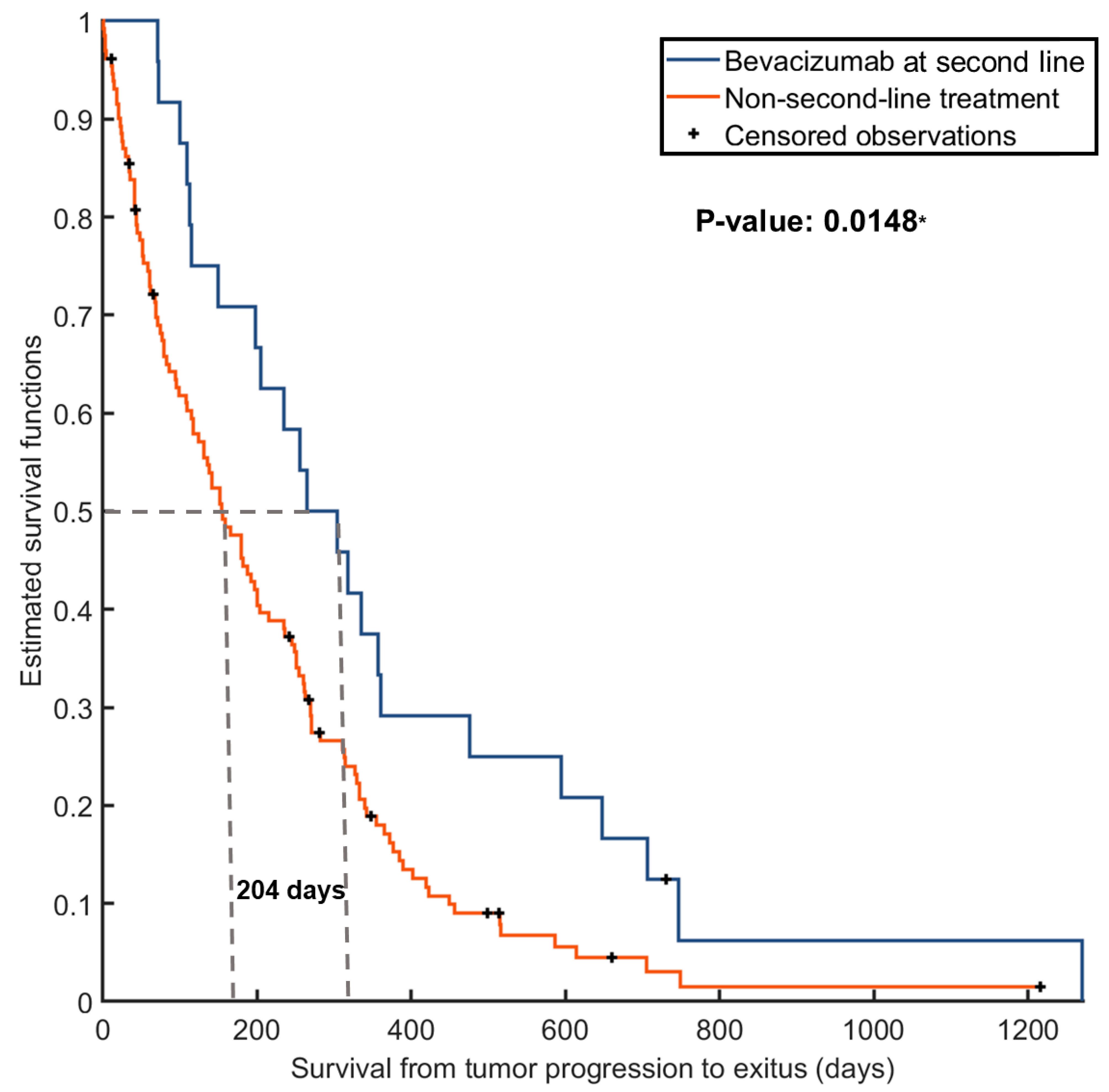
Given that BVZ was administered after tumor progression, we assessed survival differences by analyzing the time from progression to exitus, measured in days. The median survival from progression to exitus for the entire cohort was 114 days. However, after conducting a log-rank test, we observed significant differences between patients treated with BVZ and those who did not receive treatment (265 days vs. 61 days from progression to exitus, respectively). These disparities in survival are visually depicted in Figure 2.

Figure 2.
Kaplan–Meier survival curves illustrating significant differences in survival times from progression to exitus based on the provision or absence of bevacizumab treatment after tumor progression. The asterisk indicates significance at p < 0.05.
3.2. Cohort and Group Description
This study included a total of 106 patients diagnosed with glioblastoma IDH-wildtype and treated with the standard Stupp treatment. The entire cohort was stratified into two groups based on tumor vascularity, as determined by rCBVmax in HAT. An optimal cutoff value of 7.5 was used. Patients with rCBVmax in HAT < 7.5 were categorized into the moderate-vascular group, while those with rCBVmax in HAT > 7.5 were placed in the high-vascular group. Figure S1 in the Supplementary Materials showcases three MRI examples for each vascular group.
Table 1 provides an overview of the primary demographic, clinical, and molecular variables for the entire cohort and the vascular groups. Statistical analysis revealed non-significant differences between these groups.

Table 1.
Basic characteristics of the entire cohort and the moderate- and high-vascular groups.
Out of the 106 patients, 39 received second-line treatment with the antiangiogenic agent BVZ following tumor progression, while the remaining 67 patients did not receive any additional treatment. Table 2 summarizes the data concerning demographic, clinical, and molecular variables for these two groups, along with the corresponding statistical comparisons.
Table 2.
Basic characteristics of groups defined by the second-line treatment (bevacizumab versus control).
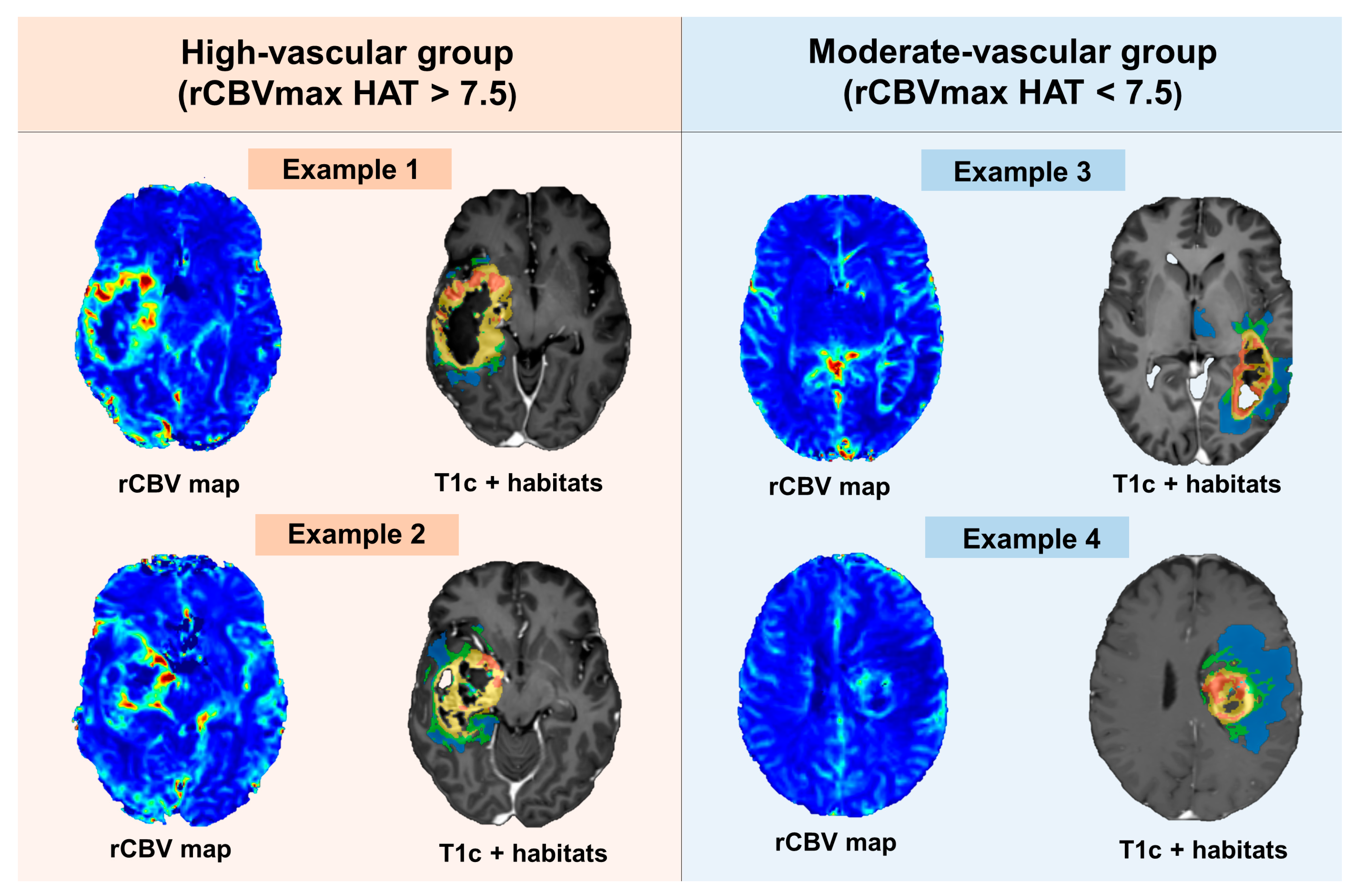
Figure 3 showcases a selection of rCBV maps and vascular habitats, processed using the ONCOhabitats method, for both the high-vascular and moderate-vascular groups.
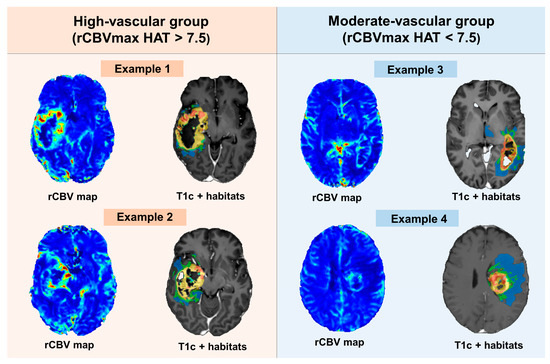
Figure 3.
Examples of rCBV maps and vascular habitats delineated by the ONCOhabitats method for the high- and moderate-vascular groups.
When considering both vascularity and second-line treatment, the cohort was further divided into four distinct groups:
Moderate vascularity with second-line BVZ treatment: 11 patients;
High vascularity with second-line BVZ treatment: 28 patients;
Moderate vascularity without second-line BVZ treatment: 14 patients;
High vascularity without second-line BVZ treatment: 53 patients.
3.3. Survival Differences between Vascular Groups
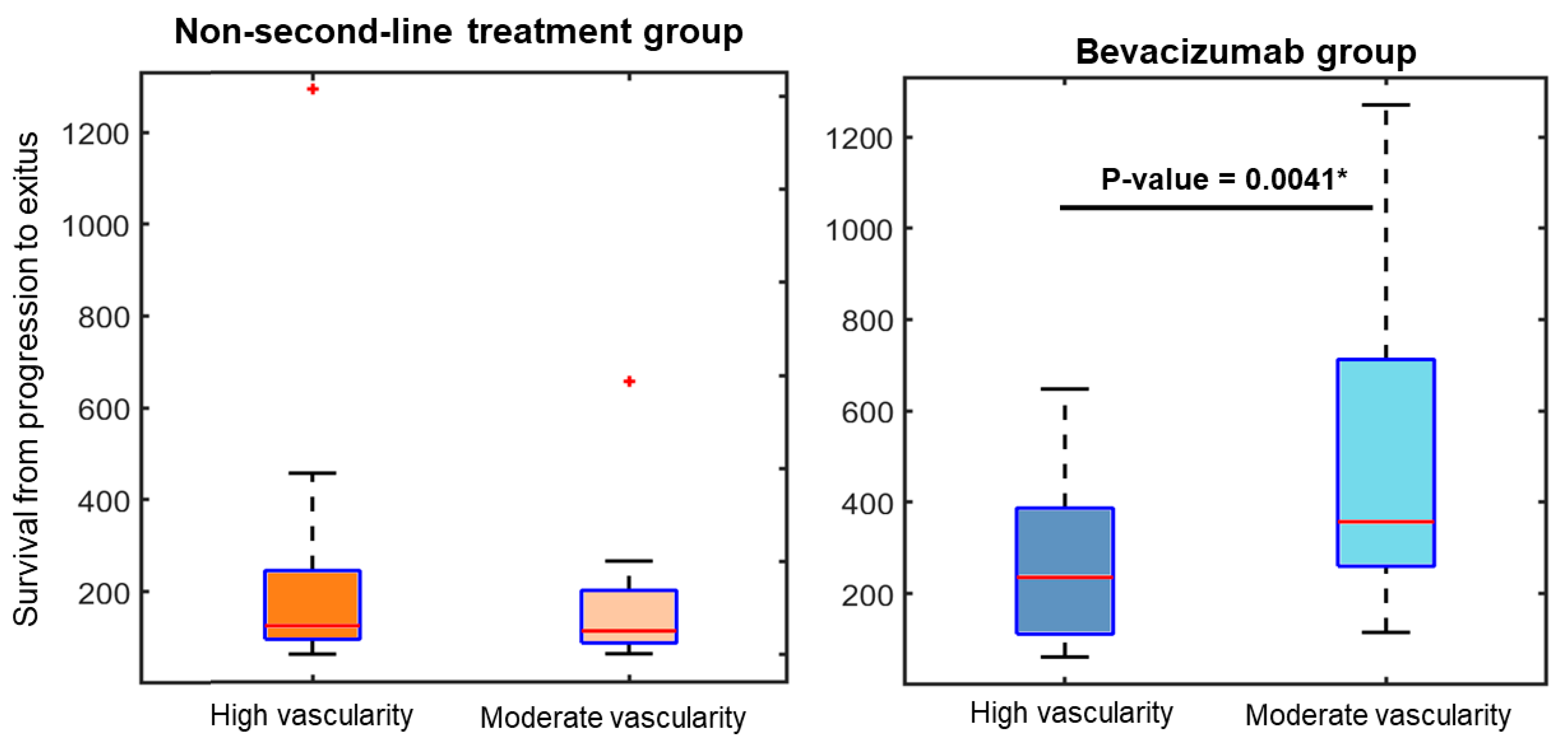
To assess variations in survival times across the vascular groups, Mann–Whitney tests were conducted. Figure 4 illustrates boxplots depicting the disparities in survival from progression to exitus among the four groups, which take into account tumor vascularity and second-line treatment. The respective p-values derived from the Mann–Whitney tests are presented to highlight statistically significant differences.
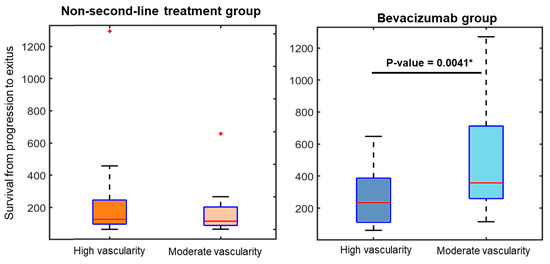
Figure 4.
Boxplots revealing substantial variations in survival times from progression to exitus for the group receiving bevacizumab treatment in relation to tumor vascularity. The asterisk in the boxplot represents outlier data points not included within the box.
Notably, among the group of patients receiving BVZ treatment, a significant discrepancy in survival was observed based on the initial vascularity measurement at the high angiogenic tumor habitat. Patients with lower initial vascularity levels demonstrated significantly longer survival times following BVZ administration.
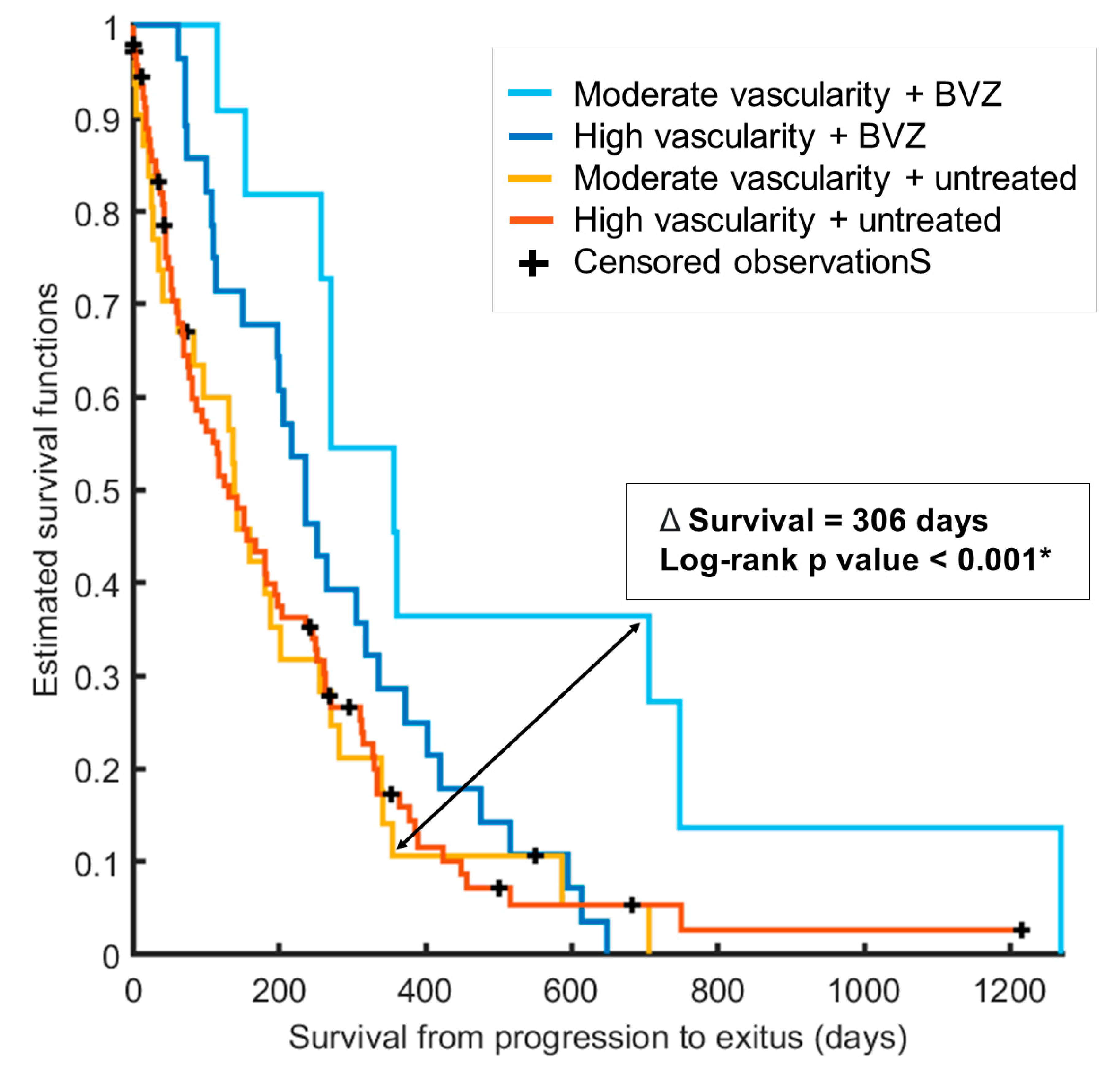
Furthermore, Kaplan–Meier curves were generated for the four groups (Figure 5), revealing substantial distinctions in the benefits conferred by BVZ depending on whether the patient had a moderate-vascular or high-vascular tumor. Patients with high-vascular tumors experienced a median survival benefit of 173 days when comparing median survival times between those who received BVZ treatment and those who did not (median survival of 235 and 62 days, respectively; log-rank p-value: 0.0027). In contrast, patients with tumors displaying moderate vascularity and undergoing BVZ treatment had a survival period that was 306 days longer than those with moderate vascularity who went untreated in the second line (median survival of 357 and 51 days, respectively; log-rank p-value: 0.0014). The survival benefit following BVZ second-line treatment was notably more pronounced for patients with moderate tumor vascularity, with a survival difference that was nearly twice as long (173 vs. 306 days) compared to untreated patients.
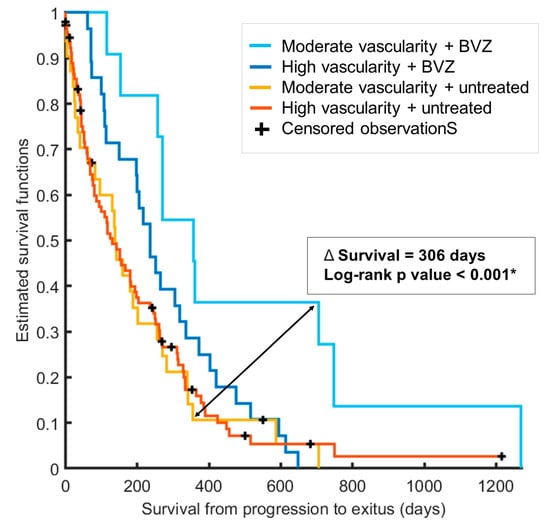
Figure 5.
Kaplan–Meier survival curves for the four defined groups based on rCBVmax within the high angiogenic tumor habitat (high or moderate vascularity) and the presence or absence of bevacizumab treatment. These curves highlight significantly extended survival for patients with moderate tumor vascularity who received bevacizumab treatment. The asterisk indicates significance at p < 0.05.
3.4. Enhanced Responses to BVZ in Patients with Moderate-Vascular Tumors
To assess the responses to BVZ treatment in the two vascular groups, we established key survival metrics: survival from tumor progression at 3, 6, 12, 18, and 24 months. The percentages of patients achieving these specific survival durations after BVZ administration are detailed in Table 3.
Table 3.
The proportion of patients after BVZ administration from each vascular group (moderate and high vascularity, respectively) alive at different times from tumor progression (3, 6, 12, 18, and 24 months).
It is noteworthy that only 14.3% of patients with high-vascular tumors achieved a full 3 months of survival following BVZ treatment, which failed to realize a significant survival benefit. Furthermore, merely 28.6% of patients with highly vascular tumors managed to reach the one-year survival mark, with no patients reaching the two-year milestone. In contrast, more favorable responses were observed in the moderate-vascularity group when BVZ treatment was administered after progression.
4. Discussion
The debate surrounding the use of bevacizumab as a second-line treatment for patients with glioblastoma IDH-wildtype has persisted for over a decade [47]. The uncertainty in survival benefits stems from varying results across different clinical trials [29,32,38,39,40,41,44].
In this study, we set out to address three primary objectives: (1) analyze the benefits of administering BVZ following tumor recurrence in a retrospective, multicenter cohort of 39 patients (compared to 67 control patients) with glioblastoma IDH-wildtype; (2) assess the significance of tumor vascularity in the benefits derived from BVZ administration; and (3) propose preoperative rCBV as a valuable biomarker for stratifying patients based on their tumor vascularity, providing pertinent insights from the presurgical stages to guide second-line treatment decisions.
For these purposes, we have analyzed differences in survival times from progression to death in the two treatment arms and groups stratified by preoperative rCBVmax in HAT calculated with ONCOhabitats. Recent studies have demonstrated the utility of this biomarker in selecting those patients who can benefit from an extended treatment with temozolomide (more than the standard six cycles) [24,45].
A “one-size-fits-all” approach does not work for glioblastoma, and this includes BVZ treatment. Previous clinical trials found limited overall benefits. We advocate for a personalized approach using non-invasive biomarkers, like rCBVmax in HAT, to select patient groups from the early stages. Our study shows that selecting patients based on a threshold (7.5) for moderate vascularity significantly extends survival. Patients with moderate vascularity receiving BVZ lived 10 months longer than those who were untreated, which is substantial given the tumor’s poor prognosis.
It is important to note that considering the proposed biomarker and threshold, only 25 of the 106 patients analyzed were considered to be moderate vascular. The authors speculate that this may be one of the possible reasons why the clinical trials did not yield strong conclusions about the benefit of BVZ for patients with glioblastomas. Only a reduced subset (~25%) of patients benefited the most. Although we have seen a benefit in providing BVZ for patients with high-vascular tumors, it is not as remarkable for patients with moderate tumor vascularity. Therefore, the major effect could be hidden if the entire cohort is analyzed as opposed to the adequate group of patients.
No useful therapeutic target has been identified to distinguish patients who benefit from treatment. While some authors have suggested the potential role of rCBV as a predictive biomarker for bevacizumab response [45,46,47,48], our study takes a step further by proposing the use of preoperative rCBVmax in HAT, which is calculated using an automated and validated method and a specific threshold (7.5). It is essential to emphasize that our results suggest the potential benefit of second-line BVZ treatment in patients whose newly diagnosed tumors exhibit a specific vascularization profile.
A notable limitation of this study is that despite having a sufficiently large cohort of 106 patients, when stratified into four groups, some groups consist of a smaller number of patients. Furthermore, it is essential to consider that the vasculature of tumors may differ between newly diagnosed and recurrent glioblastoma. Analyzing follow-up MRIs could provide more accurate information for patient stratification. Future prospective studies will address these limitations and incorporate additional factors, such as patient age, to validate the accuracy of these biomarkers for the selection of BVZ second-line treatment. Furthermore, in future studies involving larger cohorts, the possibility of including an intermediate vascular subgroup will be analyzed.
5. Conclusions
In conclusion, our study proposes a valuable biomarker for the stratification of patients based on their tumor vascularization profile from the presurgical stage. Moreover, we have demonstrated that patients with an rCBVmax in HAT lower than 7.5 exhibit significantly longer survival from progression when BVZ is administered as a second-line treatment. This research opens the door to future prospective studies aimed at validating these findings and assessing the potential of this biomarker for the selection of second-line BVZ treatment. Positive outcomes in these studies could pave the way for a more personalized approach to second-line treatment for patients with glioblastoma IDH-wildtype, ultimately enhancing prognosis and quality of life.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/cancers16010161/s1, Figure S1: Sets of MRI examples from three patients included in the low-vascular group and three for the high-vascular group.
Author Contributions
Conceptualization: M.d.M.Á.-T.; data curation: M.d.M.Á.-T.; formal analysis: M.d.M.Á.-T., J.M.G.-G., E.F.-G., C.B. and J.P.; funding acquisition: J.M.G.-G.; investigation: M.d.M.Á.-T., J.M.G.-G. and E.F.-G.; methodology: M.d.M.Á.-T., J.M.G.-G. and E.F.-G.; project administration: J.M.G.-G.; resources: M.d.M.Á.-T., J.M.G.-G., E.F.-G., C.B. and J.P.; software: J.M.G.-G., E.F.-G. and M.d.M.Á.-T.; supervision: J.M.G.-G. and E.F.-G.; validation: C.B. and J.P.; visualization: M.d.M.Á.-T., J.M.G.-G., E.F.-G., C.B. and J.P.; roles/writing—original draft: M.d.M.Á.-T.; writing—review and editing: M.d.M.Á.-T., J.M.G.-G., E.F.-G., C.B. and J.P. All authors have read and agreed to the published version of the manuscript.
Funding
M.Á-T was supported by DPI2016-80054-R (Programa Estatal de Promoción del Talento y su Empleabilidad en I + D + i). This work was partially supported by the ALBATROSS project (National Plan for Scientific and Technical Research and Innovation 2017–2020, No. PID2019-104978RB-I00). This study was partially funded by the Fundació La Marató TV3 (665/C/2013). Grant PID2021-127110OA-I00 (PROGRESS) was funded by MCIN/AEI/10.13039/501100011033 and ERDF, a way of making Europe.
Institutional Review Board Statement
This study was approved by the Institutional Review Board of the Hospital Germans Trias i Pujol (PI-14-016) and the Ethics Committees of all the participating institutions and their Biobanks and was conducted in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent Statement
All patients or their representatives gave their written informed consent to participate in this study.
Data Availability Statement
Data are available upon request due to privacy restrictions.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- McGahan, B.G.; Neilsen, B.K.; Kelly, D.L.; McComb, R.D.; Kazmi, S.A.J.; White, M.L.; Zhang, Y.; Aizenberg, M.R. Assessment of vascularity in glioblastoma and its implications on patient outcomes. J. Neuro-Oncol. 2017, 132, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Birner, P.; Piribauer, M.; Fischer, I.; Gatterbauer, B.; Marosi, C.; Ambros, P.F.; Ambros, I.M.; Bredel, M.; Oberhuber, G.; Rössler, K.; et al. Vascular Patterns in Glioblastoma Influence Clinical Outcome and Associate with Variable Expression of Angiogenic Proteins: Evidence for Distinct Angiogenic Subtypes. Brain Pathol. 2003, 13, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Marsden, P.A. Angiogenesis in glioblastoma. N. Engl. J. Med. 2013, 369, 1561–1563. [Google Scholar] [CrossRef] [PubMed]
- Folkerth, R.D. Histologic measures of angiogenesis in human primary brain tumors. In Angiogenesis in Brain Tumors; Cancer Treatment and Research Series; Springer: Berlin/Heidelberg, Germany, 2004; Volume 117, pp. 79–95. [Google Scholar]
- De Palma, M.; Biziato, D.; Petrova, T.V. Microenvironmental regulation of tumour angiogenesis. Nat. Rev. Cancer 2017, 17, 457–474. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Juan-Albarracín, J.; Fuster-Garcia, E.; Pérez-Girbés, A.; Aparici-Robles, F.; Alberich-Bayarri, Á.; Revert-Ventura, A.; Martí-Bonmatí, L.; García-Gómez, J.M. Glioblastoma: Vascular Habitats Detected at Preoperative Dynamic Susceptibility-weighted Contrast-enhanced Perfusion MR Imaging Predict Survival. Radiology 2018, 287, 944–954. [Google Scholar] [CrossRef]
- lvarez-Torres, M.; Juan-Albarracín, J.; Fuster-Garcia, E.; Bellvís-Bataller, F.; Lorente, D.; Reynés, G.; Font de Mora, J.; Aparici-Robles, F.; Botella, C.; Muñoz-Langa, J.; et al. Robust association between vascular habitats and patient prognosis in glioblastoma: An international multi-center study. J. Magn. Reson. Imaging 2020, 51, 1478–1486. [Google Scholar] [CrossRef]
- Malik, D.G.; Rath, T.J.; Urcuyo Acevedo, J.C.; Canoll, P.D.; Swanson, K.R.; Boxerman, J.L.; Quarles, C.C.; Schmainda, K.M.; Burns, T.C.; Hu, L.S. Advanced MRI Protocols to Discriminate Glioma from Treatment Effects: State of the Art and Future Directions. Front. Radiol. 2022, 2, 809373. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Clavreul, A.; Menei, P. Intratumoral heterogeneity in glioblastoma: Don’t forget the peritumoral brain zone. Neuro-Oncology 2015, 17, 1322–1332. [Google Scholar] [CrossRef] [PubMed]
- Soeda, A.; Hara, A.; Kunisada, T.; Yoshimura, S.; Iwama, T.; Park, D.M. The evidence of glioblastoma heterogeneity. Sci. Rep. 2015, 5, 7979. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Torres, M.d.M.; Fuster-García, E.; Juan-Albarracín, J.; Reynés, G.; Aparici-Robles, F.; Ferrer-Lozano, J.; García-Gómez, J.M. Local detection of microvessels in IDH-wildtype glioblastoma using relative cerebral blood volume: An imaging marker useful for astrocytoma grade 4 classification. BMC Cancer 2022, 22, 40. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, O.M.; Del Mar Álvarez-Torres, M.; Figueiredo, P.; Hangel, G.; Keil, V.C.; Nechifor, R.E.; Riemer, F.; Schmainda, K.M.; Warnert, E.A.H.; Wiegers, E.C.; et al. High-Grade Glioma Treatment Response Monitoring Biomarkers: A Position Statement on the Evidence Supporting the Use of Advanced MRI Techniques in the Clinic, and the Latest Bench-to-Bedside Developments. Part 1: Perfusion and Diffusion Techniques. Front. Oncol. 2022, 12, 810263. [Google Scholar] [CrossRef] [PubMed]
- Stumpo, V.; Guida, L.; Bellomo, J.; Van Niftrik, C.H.B.; Sebök, M.; Berhouma, M.; Bink, A.; Weller, M.; Kulcsar, Z.; Regli, L.; et al. Hemodynamic Imaging in Cerebral Diffuse Glioma-Part B: Molecular Correlates, Treatment Effect Monitoring, Prognosis, and Future Directions. Cancers 2022, 14, 1342. [Google Scholar] [CrossRef] [PubMed]
- Guida, L.; Stumpo, V.; Bellomo, J.; Van Niftrik, C.H.B.; Sebök, M.; Berhouma, M.; Bink, A.; Weller, M.; Kulcsar, Z.; Regli, L.; et al. Hemodynamic Imaging in Cerebral Diffuse Glioma-Part A: Concept, Differential Diagnosis and Tumor Grading. Cancers 2022, 14, 1432. [Google Scholar] [CrossRef] [PubMed]
- Juan-Albarracín, J.; Fuster-Garcia, E.; García-Ferrando, G.A.; García-Gómez, J.M. ONCOhabitats: A system for glioblastoma heter-ogeneity assessment through MRI. Int. J. Med. Inform. 2019, 128, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Despotović, I.; Goossens, B.; Philips, W. MRI segmentation of the human brain: Challenges, methods, and applications. Comput. Math. Methods Med. 2015, 2015, 450341. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Clavreul, A.; Aubry, M.; Com, E.; De Tayrac, M.; Eliat, P.-A.; Henry, C.; Rousseau, A.; Mosser, J.; Menei, P. Characterizing the peritumoral brain zone in glioblastoma: A multidisciplinary analysis. J. Neuro-Oncol. 2015, 122, 53–61. [Google Scholar] [CrossRef]
- Schoenegger, K.; Oberndorfer, S.; Wuschitz, B.; Struhal, W.; Hainfellner, J.; Prayer, D.; Heinzl, H.; Lahrmann, H.; Marosi, C.; Grisold, W. Peritumoral edema on MRI at initial diagnosis: An independent prognostic factor for glioblastoma? Eur. J. Neurol. 2009, 16, 874–878. [Google Scholar] [CrossRef]
- Akbari, H.; Macyszyn, L.; Da, X.; Wolf, R.L.; Bilello, M.; Verma, R.; O’Rourke, D.M.; Davatzikos, C. Pattern analysis of dynamic suscep-tibility contrast-enhanced MR imaging demonstrates peritumoral tissue heterogeneity. Radiology 2014, 273, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Weis, S.M.; Cheresh, D.A. Tumor angiogenesis: Molecular pathways and therapeutic targets. Nat. Med. 2011, 17, 1359–1370. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Torres, M.d.M.; Fuster-García, E.; Balaña, C.; Puig, J.; García-Gómez, J.M. Lack of Benefit of Extending Temozolomide Treatment in Patients with High Vascular Glioblastoma with Methylated MGMT. Cancers 2021, 13, 5420. [Google Scholar] [CrossRef]
- Jensen, R.L.; Mumert, M.L.; Gillespie, D.L.; Kinney, A.Y.; Schabel, M.C.; Salzman, K.L. Preoperative dynamic contrast-enhanced MRI correlates with molecular markers of hypoxia and vascularity in specific areas of intratumoral microenvironment and is pre-dictive of patient outcome. Neuro-Oncology 2014, 16, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.S.; Eschbacher, J.M.; Dueck, A.C.; Heiserman, J.E.; Liu, S.; Karis, J.P.; Smith, K.A.; Shapiro, W.R.; Pinnaduwage, D.S.; Coons, S.W.; et al. Correlations between Perfusion MR Imaging Cerebral Blood Volume, Microvessel Quantification, and Clinical Outcome Using Stereotactic Analysis in Recurrent High-Grade Glioma. Am. J. Neuroradiol. 2012, 33, 69–76. [Google Scholar] [CrossRef]
- Lev, M.H.; Ozsunar, Y.; Henson, J.W.; Rasheed, A.A.; Barest, G.D.; Harsh, G.R., 4th; Fitzek, M.M.; Chiocca, E.A.; Rabinov, J.D.; Csavoy, A.N.; et al. Glial tumor grading and outcome prediction using dynamic spin-echo MR susceptibility mapping compared with conventional contrast-enhanced MR: Confounding effect of elevated rCBV of oligodendrogliomas [corrected]. Am. J. Neuroradiol. 2004, 25, 214–221. [Google Scholar] [PubMed]
- Reardon, D.A.; Desjardins, A.; Peters, K.B.; Gururangan, S.; Sampson, J.H.; McLendon, R.E.; Herndon, J.E., 2nd; Bulusu, A.; Threatt, S.; Friedman, A.H.; et al. Phase II study of carboplatin, irinotecan, and bevacizumab for bevacizumab naïve, recurrent glioblastoma. J. Neurooncol. 2012, 107, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef]
- Vredenburgh, J.J.; Desjardins, A.; Herndon, J.E., 2nd; Marcello, J.; Reardon, D.A.; Quinn, J.A.; Rich, J.N.; Sathornsumetee, S.; Gururangan, S.; Sampson, J.; et al. Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J. Clin. Oncol. 2007, 25, 4722–4729. [Google Scholar] [CrossRef]
- Kreisl, T.N.; Kim, L.; Moore, K.; Duic, P.; Royce, C.; Stroud, I.; Garren, N.; Mackey, M.; Butman, J.A.; Camphausen, K.; et al. Phase II Trial of Single-Agent Bevacizumab Followed by Bevacizumab Plus Irinotecan at Tumor Progression in Recurrent Glioblastoma. J. Clin. Oncol. 2009, 27, 740–745. [Google Scholar] [CrossRef]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.; Won, M.; et al. A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef]
- Schiff, D.; Abrey, L.E.; Yung, W.K.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; Vredenburgh, J.; Huang, J.; Zheng, M.; Cloughesy, T. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef]
- Ali, S.A.; McHayleh, W.M.; Ahmad, A.; Sehgal, R.; Braffet, M.; Rahman, M.; Bejjani, G.; Friedland, D.M.; Neil, D.; Ajlan, A.; et al. Bevacizumab and irinotecan therapy in glioblastoma multiforme: A series of 13 cases. J. Neurosurg. 2008, 109, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Bokstein, F.; Shpigel, S.; Blumenthal, D.T. Treatment with bevacizumab and irinotecan for recurrent high-grade glial tumors. Cancer 2008, 112, 2267–2273. [Google Scholar] [CrossRef] [PubMed]
- Gutin, P.H.; Iwamoto, F.M.; Beal, K.; Mohile, N.A.; Karimi, S.; Hou, B.L.; Lymberis, S.; Yamada, Y.; Chang, J.; Abrey, L.E. Safety and Efficacy of Bevacizumab with Hypofractionated Stereotactic Irradiation for Recurrent Malignant Gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Sathornsumetee, S.; Desjardins, A.; Vredenburgh, J.J.; McLendon, R.E.; Marcello, J.; Herndon, J.E.; Mathe, A.; Hamilton, M.; Rich, J.N.; Norfleet, J.A.; et al. Phase II trial of bevacizumab and erlotinib in patients with recurrent malignant glioma. Neuro-Oncology 2010, 12, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Drappatz, J.; Lee, E.Q.; Hammond, S.; Grimm, S.A.; Norden, A.D.; Beroukhim, R.; Gerard, M.; Schiff, D.; Chi, A.S.; Batchelor, T.T.; et al. Phase I study of panobinostat in combination with bevacizumab for recurrent high-grade glioma. J. Neuro-Oncol. 2012, 107, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Desjardins, A.; Vredenburgh, J.J.; Gururangan, S.; Sampson, J.H.; Sathornsumetee, S.; McLendon, R.E.; Herndon, J.E., 2nd; Marcello, J.E.; Norfleet, J.; et al. Metronomic chemotherapy with daily, oral etoposide plus bevacizumab for recurrent malignant glioma: A phase II study. Br. J. Cancer. 2009, 101, 1986–1994. [Google Scholar] [CrossRef] [PubMed]
- Galanis, E.; Anderson, S.K.; Lafky, J.M.; Uhm, J.H.; Giannini, C.; Kumar, S.K.; Kimlinger, T.K.; Northfelt, D.W.; Flynn, P.J.; Jaeckle, K.A.; et al. Phase II study of bevacizumab in combination with sorafenib in recurrent glioblastoma (N0776): A north central cancer treatment group trial. Clin. Cancer Res. 2013, 19, 4816–4823. [Google Scholar] [CrossRef]
- Cabrera, A.R.; Cuneo, K.C.; Vredenburgh, J.J.; Sampson, J.H.; Kirkpatrick, J.P. Stereotactic radiosurgery and bevacizumab for recurrent glioblastoma multiforme. J. Natl. Compr. Cancer Netw. 2012, 10, 695–699. [Google Scholar] [CrossRef]
- Zuniga, R.M.; Torcuator, R.; Jain, R.; Anderson, J.; Doyle, T.; Ellika, S.; Schultz, L.; Mikkelsen, T. Efficacy, safety and patterns of response and recurrence in patients with recurrent high-grade gliomas treated with bevacizumab plus irinotecan. J. Neuro-Oncol. 2009, 91, 329–336. [Google Scholar] [CrossRef]
- Balaña, C.; Estival, A.; Pineda, E.; Sepúlveda, J.; Mesía, C.; del Barco, S.; Gil-Gil, M.; Hardy, M.; Indacoechea, A.; Cardona, A.F. Prolonged survival after bevacizumab rechallenge in glioblastoma patients with previous response to bevacizumab. Neuro-Oncol. Pract. 2017, 4, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Dimberg, A. The glioblastoma vasculature as a target for cancer therapy. Biochem. Soc. Trans. 2014, 42, 1647–1652. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Wiestler, B.; Burth, S.; Wick, A.; Nowosielski, M.; Heiland, S.; Schlemmer, H.-P.; Wick, W.; Bendszus, M.; Radbruch, A. Relative cerebral blood volume is a potential predictive imaging biomarker of bevacizumab efficacy in recurrent glioblastoma. Neuro-Oncology 2015, 17, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Pineda, E.; Esteve-Codina, A.; Martinez-Garcia, M.; Alameda, F.; Carrato, C.; Arpi, O.; Balana, C. Glioblastoma gene expression subtypes and correlation with clinical, molecular and immunohistochemical characteristics in a homogenously treated cohort: GLIOCAT project. J. Clin. Oncol. 2019, 37, 2029. [Google Scholar] [CrossRef]
- Boxerman, J.L.; Snyder, B.S.; Barboriak, D.P.; Schmainda, K.M. Early post-bevacizumab change in rCBV from DSC-MRI identifies pseudore-sponse in recurrent glioblastoma: Results from ACRIN 6677/RTOG 0625. Front. Oncol. 2023, 26, 1061502. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).