
Takotsubo Cardiomyopathy in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Summary of Included Cases

 , , , , , ,
, , , , , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Reporting and Protocol Registration
2.3. Search Strategy
2.4. Cases and Studies Selection
2.5. Data Extraction and Tabulation
3. Results
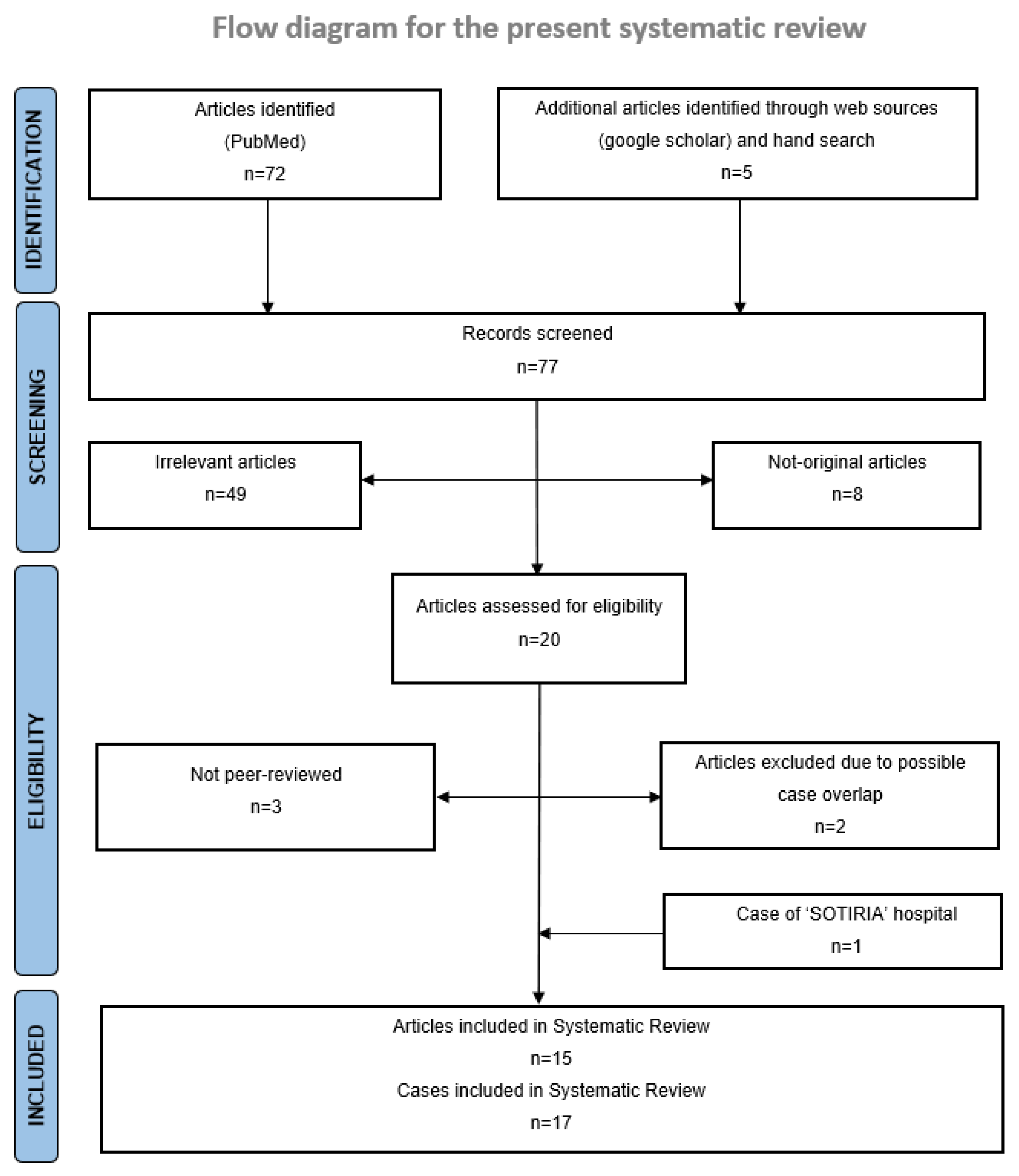
3.1. Literature Search and Selection of Reports
3.2. Baseline Clinicopathologic Characteristics
3.3. Clinical Characteristics and Outcomes of Takotsubo Syndrome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Lipson, E.J.; Drake, C.G. Ipilimumab: An Anti-CTLA-4 Antibody for Metastatic Melanoma. Clin. Cancer Res. 2011, 17, 6958–6962. [Google Scholar] [CrossRef] [PubMed]
- Twomey, J.D.; Zhang, B. Cancer Immunotherapy Update: FDA-Approved Checkpoint Inhibitors and Companion Diagnostics. AAPS J. 2021, 23, 39. [Google Scholar] [CrossRef]
- Conroy, M.; Naidoo, J. Immune-related adverse events and the balancing act of immunotherapy. Nat. Commun. 2022, 13, 392. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.; Ghosh, R.K.; Wongsaengsak, S.; Bandyopadhyay, D.; Ghosh, G.C.; Aronow, W.S.; Fonarow, G.C.; Lenihan, D.J.; Bhatt, D.L. Cardiovascular Toxicities of Immune Checkpoint Inhibitors: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1714–1727. [Google Scholar] [CrossRef] [PubMed]
- Malaty, M.M.; Amarasekera, A.T.; Li, C.; Scherrer-Crosbie, M.; Tan, T.C. Incidence of immune checkpoint inhibitor mediated cardiovascular toxicity: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13831. [Google Scholar] [CrossRef] [PubMed]
- Haanen, J.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K.; Committee, E.G. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv119–iv142. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Bybee, K.A.; Kara, T.; Prasad, A.; Lerman, A.; Barsness, G.W.; Wright, R.S.; Rihal, C.S. Systematic Review: Transient Left Ventricular Apical Ballooning: A Syndrome That Mimics ST-Segment Elevation Myocardial Infarction. Ann. Intern. Med. 2004, 141, 858–865. [Google Scholar] [CrossRef]
- Prasad, A.; Lerman, A.; Rihal, C.S. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am. Heart J. 2008, 155, 408–417. [Google Scholar] [CrossRef]
- Carbone, A.; Bottino, R.; Russo, V.; D’andrea, A.; Liccardo, B.; Maurea, N.; Quagliariello, V.; Cimmino, G.; Golino, P. Takotsubo Cardiomyopathy as Epiphenomenon of Cardiotoxicity in Patients with Cancer: A Meta-summary of Case Reports. J. Cardiovasc. Pharmacol. 2021, 78, e20–e29. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Deshmukh, A.; Kumar, G.; Pant, S.; Rihal, C.; Murugiah, K.; Mehta, J.L. Prevalence of Takotsubo cardiomyopathy in the United States. Am. Heart J. 2012, 164, 66–71.e1. [Google Scholar] [CrossRef] [PubMed]
- Camastra, G.; Arcari, L.; Ciolina, F.; Danti, M.; Cacciotti, L. Cardiac magnetic resonance imaging of transient myocardial dysfunction in a patient treated with checkpoint-targeted immunotherapy. Eur. J. Cancer 2021, 144, 389–391. [Google Scholar] [CrossRef]
- Okamatsu, Y.; Tsubouchi, K.; Ibusuki, R.; Maehara-Keshino, E.; Shimauchi, A.; Kayukawa, T.; Eto, D.; Inoue, K.; Harada, T. Rapid Onset of Takotsubo Cardiomyopathy Induced by an Infusion Reaction to Pembrolizumab in a Patient with NSCLC. JTO Clin. Res. Rep. 2020, 1, 100055. [Google Scholar] [CrossRef]
- Tan, N.Y.L.; Anavekar, N.S.; Wiley, B.M. Concomitant myopericarditis and takotsubo syndrome following immune checkpoint inhibitor therapy. BMJ Case Rep. 2020, 13, e235265. [Google Scholar] [CrossRef]
- Oldfield, K.; Jayasinghe, R.; Niranjan, S.; Chadha, S. Immune checkpoint inhibitor-induced takotsubo syndrome and diabetic ketoacidosis: Rare reactions. BMJ Case Rep. 2021, 14, e237217. [Google Scholar] [CrossRef] [PubMed]
- Geisler, B.P.; Raad, R.A.; Esaian, D.; Sharon, E.; Schwartz, D.R. Apical ballooning and cardiomyopathy in a melanoma patient treated with ipilimumab: A case of takotsubo-like syndrome. J. Immunother. Cancer 2015, 3, 4. [Google Scholar] [CrossRef]
- Elikowski, W.; Małek-Elikowska, M.; Łazowski, S.; Zawodna, M.; Fertała, N.; Bryl, M. Takotsubo cardiomyopathy in a young male with lung cancer and neoplastic embolization of the coronary microcirculation. Polski Merkur. Lek. Organ Polskiego Towar. Lek. 2018, 44, 54–59. [Google Scholar]
- Khan, N.A.J.; Pacioles, T.; Alsharedi, M. Atypical Takotsubo Cardiomyopathy Secondary to Combination of Chemo-Immunotherapy in a Patient with Non-Small Cell Lung Cancer. Cureus 2020, 12, e9429. [Google Scholar] [CrossRef] [PubMed]
- Tsuruda, T.; Yoshikawa, N.; Kai, M.; Yamaguchi, M.; Toida, R.; Kodama, T.; Kajihara, K.; Kawabata, T.; Nakamura, T.; Sakata, K.; et al. The Cytokine Expression in Patients with Cardiac Complication after Immune Checkpoint Inhibitor Therapy. Intern. Med. 2021, 60, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Serzan, M.; Rapisuwon, S.; Krishnan, J.; Chang, I.C.; Barac, A. Takotsubo Cardiomyopathy Associated with Checkpoint Inhibitor Therapy: Endomyocardial Biopsy Provides Pathological Insights to Dual Diseases. JACC Cardio Oncol. 2021, 3, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Ederhy, S.; Cautela, J.; Ancedy, Y.; Escudier, M.; Thuny, F.; Cohen, A. Takotsubo-Like Syndrome in Cancer Patients Treated with Immune Checkpoint Inhibitors. JACC Cardiovasc. Imaging 2018, 11, 1187–1190. [Google Scholar] [CrossRef]
- Anderson, R.D.; Brooks, M. Apical takotsubo syndrome in a patient with metastatic breast carcinoma on novel immunotherapy. Int. J. Cardiol. 2016, 222, 760–761. [Google Scholar] [CrossRef]
- Schwab, K.S.; Kristiansen, G.; Isaak, A.; Held, S.E.A.; Heine, A.; Brossart, P. Long Term Remission and Cardiac Toxicity of a Combination of Ipilimumab and Nivolumab in a Patient with Metastatic Head and Neck Carcinoma After Progression Following Nivolumab Monotherapy. Front. Oncol. 2019, 9, 403. [Google Scholar] [CrossRef]
- Norikane, T.; Mitamura, K.; Yamamoto, Y.; Takami, Y.; Fujimoto, K.; Noma, T.; Nishiyama, Y. Immune checkpoint inhibitor myocarditis mimicking Takotsubo cardiomyopathy on MPI. J. Nucl. Cardiol. 2020, 29, 2694–2698. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Patel, G.; Singh, R.B.; Goyal, A.; Avgush, K.; Koka, J. Atezolizumab-induced autoimmune diabetes mellitus presenting as diabetic ketoacidosis and Takotsubo cardiomyopathy. BMJ Case Rep. 2022, 15, e250662. [Google Scholar] [CrossRef]
- Airò, G.; Maffezzoli, M.; Lazzarin, A.; Bianconcini, M.; Greco, A.; Buti, S.; Leonetti, A. Takotsubo syndrome in a patient with metastatic renal cell carcinoma treated with pembrolizumab plus axitinib. Immunotherapy 2022, 14, 1297–1305. [Google Scholar] [CrossRef]
- Ederhy, S.; Dolladille, C.; Thuny, F.; Alexandre, J.; Cohen, A. Takotsubo syndrome in patients with cancer treated with immune checkpoint inhibitors: A new adverse cardiac complication. Eur. J. Heart Fail. 2019, 21, 945–947. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A.; et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor–Related Cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Noor, A.; Joshi, S.; Kim, A.S. Takotsubo cardiomyopathy in cancer patients. Cardio-Oncology 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Joy, P.S.; Guddati, A.K.; Shapira, I. Outcomes of Takotsubo cardiomyopathy in hospitalized cancer patients. J. Cancer Res. Clin. Oncol. 2018, 144, 1539–1545. [Google Scholar] [CrossRef]
- Keramida, K.; Farmakis, D.; Filippatos, G. Cancer and Takotsubo syndrome: From rarity to clinical practice. ESC Heart Fail. 2021, 8, 4365–4369. [Google Scholar] [CrossRef]
- Tajiri, K.; Ieda, M. Cardiac Complications in Immune Checkpoint Inhibition Therapy. Front. Cardiovasc. Med. 2019, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Shalata, W.; Abu-Salman, A.; Steckbeck, R.; Mathew Jacob, B.; Massalha, I.; Yakobson, A. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers 2021, 13, 5218. [Google Scholar] [CrossRef]
- Mocan-Hognogi, D.L.; Trancǎ, S.; Farcaş, A.D.; Mocan-Hognogi, R.F.; Pârvu, A.V.; Bojan, A.S. Immune Checkpoint Inhibitors and the Heart. Front. Cardiovasc. Med. 2021, 8, 726426. [Google Scholar] [CrossRef]
- Khunger, A.; Battel, L.; Wadhawan, A.; More, A.; Kapoor, A.; Agrawal, N. New Insights into Mechanisms of Immune Checkpoint Inhibitor-Induced Cardiovascular Toxicity. Curr. Oncol. Rep. 2020, 22, 65. [Google Scholar] [CrossRef]
- Frayberg, M.; Yung, A.; Zubiri, L.; Zlotoff, D.A.; Reynolds, K.L. What the Cardiologist Needs to Know About Cancer Immunotherapies and Complications. Curr. Treat. Options Oncol. 2021, 22, 53. [Google Scholar] [CrossRef]
- Doherty, M. Algorithms for assessing the probability of an Adverse Drug Reaction. Respir. Med. CME 2009, 2, 63–67. [Google Scholar] [CrossRef]
- Akashi, Y.J.; Nef, H.M.; Lyon, A.R. Epidemiology and pathophysiology of Takotsubo syndrome. Nat. Rev. Cardiol. 2015, 12, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, N.D.; Tarantino, N.; Guastafierro, F.; De Gennaro, L.; Correale, M.; Stiermaier, T.; Möller, C.; Di Biase, M.; Eitel, I.; Santoro, F. Malignancies and outcome in Takotsubo syndrome: A meta-analysis study on cancer and stress cardiomyopathy. Heart Fail. Rev. 2019, 24, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Gallegos, C.; Rottmann, D.; Nguyen, V.Q.; Baldassarre, L.A. Myocarditis with checkpoint inhibitor immunotherapy: Case report of late gadolinium enhancement on cardiac magnetic resonance with pathology correlate. Eur. Heart J.—Case Rep. 2019, 3, yty149. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, W. Cardiovascular immune-related adverse events: Evaluation, diagnosis and management. Asia-Pacific J. Clin. Oncol. 2020, 16, 232–240. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ref | Gender, Age | Tumor Type (Stage) | Potential Stressors * | Line/Cycle of Therapy | ICIs Targets (Agents) | Concurrent/Previous Systemic Therapies | Time on Treatment at TTS Presentation (Days) | Time from Last ICI Treatment (Days) |
|---|---|---|---|---|---|---|---|---|
| Tan et al., 2020 [15] | M, 62 | HCC (IV) | Active smoking | 1st line, C1 | PD-1 (nivolumab) | - | 21 | 21 |
| Oldfield et al., 2020 [16] | M, 76 | Melanoma (IV) | Underlying DKA, CVS comorbidities (hypertension, diabetes mellitus, hyperlipidemia) | 1st line, 1st event after C1, 2nd event after C2 | PD-1 (nivolumab), CTLA-4 (ipilimumab) | - | NR | 2nd event 4 days after C2 (1st event NR) |
| Geisler et al., 2015 [17] | F, 83 | Melanoma (IV) | Hypertension | 1st line, C4 | CTLA-4 (ipilimumab) | - | ≈84 | ≈21 |
| Elikowski et al., 2018 [18] | M, 30 | NSCLC (IV) | Cardiac carcinomatous infiltration, carcinomatous embolization of coronary arteries | Patient received ICIs in 1st line, TTS presented after 2nd line ChT | PD-L1 (durvalumab), CTLA-4 (tremelimumab) | Cisplatin/gemcitabine (1st line in combination with ICIs), carboplatin/paclitaxel (2nd line) | NR | NR |
| Khan et al., 2020 [19] | F, 57 | NSCLC (IV) | Underlying pneumonia | 1st line, C4 | PD-1 (pembrolizumab) | Carboplatin/pemetrexed (combination with ICIs) | ≈77 | 14 |
| Tsuruda et al., 2021 [20] | M, 75 | NSCLC | Myocarditis | 1st line, C1 | PD-1 (pembrolizumab) | Adjuvant cisplatin/vinorelbine 6 months ago | 136 | 136 |
| Serzan et al., 2021 [21] | F, 66 | Melanoma (I) | - | Adjuvant, C7 | PD-1 (nivolumab), CTLA4 (ipilimumab) | - | ≈112 | NR |
| Ederhy et al., 2017 [22] | M, 45 | Melanoma (advanced) | NR | Line NR, C1 | PD-1 (nivolumab), CTLA4 (ipilimumab) | - | 5 | 5 |
| M, 77 | Melanoma (advanced) | NR | Line NR, C3 | PD-1 (nivolumab), CTLA-4 (ipilimumab) | - | 65 | NR | |
| Okamatsu et al., 2020 [14] | F, 76 | NSCLC (IIIC) | Infusion reaction | 1st line, C1 | PD-1 (pembrolizumab) | - | 1 (6 h after C1) | 1 (6 h after C1) |
| Anderson & Brooks, 2016 [23] | F, 56 | HER2 breast cancer (IV) | Colitis | 1st line | PD-1 (pembrolizumab) | Trastuzumab along with ICI, previous adjuvant treatment with anthracycline based ChT and trastuzumab (about 8 months before ICI) | ≈247 | NR |
| Schwab et al., 2019 [24] | M, 69 | HNSCC (IV) | - | 2nd line, C7 | PD-1 (nivolumab), CTLA-4 (ipilimumab) | Previous ChT with cisplatin, 5-FU, cetuximab (at least 1 month before ICIs) | ≈450 | NR |
| Camastra et al., 2020 [13] | M, 70 | Lung cancer | Possible myocarditis, immune-induced nausea/vomiting | Line NR, C1 | PD-L1 (atezolizumab) | Previous ChT | 7 | 7 |
| Norikane et al., 2020 [25] | M, 73 | RCC (advanced) | Myocarditis | NR | PD-1 (nivolumab), CTLA-4 (ipilimumab) | NR | 7 | 7 |
| Singhal et al., 2022 [26] | F, ≈80 | HCC (IV) | Underlying DKA, hypertension | 2nd line | PD-L1 (atezolizumab) | Bevacizumab along with ICI, previous line with multi-TKI (sorafenib) at least 6 months before | ≈180 | NR |
| Airo et al., 2022 [27] | M, 49 | RCC (IV) | - | 1st line, C1 | PD-1 (pembrolizumab) | VEGFR-TKI (axitinib) along with ICI | 6 | 6 |
| ‘Sotiria’ case | F, 74 | NSCLC (IIIC) | Active smoking, major depression, CVS comorbidities (PAD, hypertension, CAD) | 1st line, C8 | PD-1 (pembrolizumab) | - | ≈175 (2nd event 360 days after C1) | 7 (2nd event 180 days after C8) |
| Ref | Clinical Presentation | Diagnostic Workup | Concurrent Cardiac Complications | Other irAEs | Management | Outcome | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Echocardiography | ↓LVEF | ECG Findings | ↑Cardiac Enzymes | CAG | TTS Outcome | Re-Introduction of ICIs | |||||
| Tan et al., 2020 [15] | Chest pain, nausea, vomiting | Apical ballooning | + | ST elevation (V5-6, II-III), RBBB, LAFB | + (Trop & BNP) | Non-obstructive CAD | Myopericarditis, VT | Pneumonitis | Corticosteroids | Resolution (clinical on 3 days, imaging on 42 days) | - |
| Oldfield et al., 2020 [16] | Chest pain, diaphoresis | Apical ballooning, hyperkinetic basal and mid segments | + | ST elevation (V2-6) | + (Trop) | Non-obstructive CAD | − (no biopsy or MRI performed for exclusion of myocarditis) | DKA, colitis, hepatitis | MI management, corticosteroids | Resolution (but 2nd event after C2) | − (interrupted after 2nd event) |
| Geisler et al., 2015 [17] | Chest pain, dyspnea | Apical ballooning, hyperkinetic base, and septum | + | ST elevation (I, V2-3), VT | + (Trop) | Non-obstructive CAD | − (no biopsy or MRI performed for exclusion of myocarditis) | Colitis, pruritus, malaise | β-blocker | Clinical resolution (5 days, but apical ballooning persisted) | NR |
| Elikowski et al., 2018 [18] | Dyspnea, weakness | LV contractility disturbances typical of apical TTS | NR | Negative T-waves (V1-6) | + (Trop & BNP) | NR | Myopericardial malignant infiltration, malignant embolization of coronary arteries | NR | HF management | Resolution, but patient died after few days | - |
| Khan et al., 2020 [19] | Chest pain, palpitations, dyspnea | Hypokinesia of septum and anterior wall with sparing of apical and basal segments (atypical TTS) | + | Sinus tachycardia | + (Trop) | Chronic RCA obstruction | − (no biopsy or MRI performed for exclusion of myocarditis) | - | HF management | Resolution | NR |
| Tsuruda et al., 2021 [20] | NR | Apical ballooning | NR | T-wave inversion, QT prolongation | + (Trop) | Not done | Myocarditis, pericardial effusion (cardiac MRI with late gadolinium enhancement and suggestive endomyocardial biopsies) | - | Corticosteroids | Death | - |
| Serzan et al., 2021 [21] | Dyspnea, generalized pain | Apical ballooning, hyperdynamic basal LV segments | NR | Sinus tachycardia, inferolateral T-wave inversions | + (Trop & BNP) | Non-obstructive CAD | − (endomyocardial biopsy ruled out concurrent myocarditis) | Pneumonitis | β-blocker | Resolution | NR |
| Ederhy et al., 2017 [22] | NR | Apical ballooning along with mid-ventricular akinesia | + | Sinus tachycardia, T-wave inversion in anteroseptal leads | + (Trop) | No obstruction | − (cardiac MRI did not reveal any signs of myocarditis) | - | Corticosteroids | Resolution (6 days) | NR |
| NR | Basal and median segment akinesia (atypical TTS) | + | T-wave inversion in V2-4 | + (Trop) | Chronic DCA obstruction | Possible myocarditis (diffuse myocardial edema on MRI; biopsy was not performed for exclusion of concurrent myocarditis) | - | Corticosteroids, HF management | Resolution (28 days) | NR | |
| Okamatsu et al., 2020 [14] | Fever, dyspnea, wheezing | Apical ballooning, ventricular hyperconstriction | + | ST elevation in V4-5, T-wave inversion in II-III, aVF, V3-6 | + (Trop) | NR | − (no biopsy or MRI performed for exclusion of myocarditis) | Infusion reaction | Corticosteroids, vassopressors | Resolution (28 days, but died 62 days after due to PD) | - |
| Anderson & Brooks, 2016 [23] | Chest pain, abdominal cramping, diarrhea (colitis) | Left ventricular dysfunction | - | Widespread T-wave inversion | + (Trop) | No obstruction | − (no biopsy or MRI performed for exclusion of myocarditis) | - | HF management | Resolution | + |
| Schwab et al., 2019 [24] | Chest pain, dyspnea | Apical ballooning | + | NR | NR | No obstruction | − (no detailed description of MRI findings for myocarditis exclusion) | Nephritis | Corticosteroids, HF management | Resolution | + |
| Camastra et al., 2020 [13] | Dyspnea | Apical ballooning (akinesia of mid-apical segments) | + | ST elevation in antero-lateral leads, T-wave inversion V2-4, QT prolongation | + (Trop) | No obstruction | Possible myocarditis (diffuse myocardial edema on MRI; biopsy was not performed for exclusion of concurrent myocarditis) | Nausea, vomiting | NR | Resolution (8 days) | NR |
| Norikane et al., 2020 [25] | Dyspnea | Apical ballooning, severe hypokinesis on anterior-septal wall | NR | ST elevation in II, III, aVF, V2-4 | + (BNP) | No obstruction | Myocarditis (cardiac MRI with late gadolinium enhancement and suggestive endomyocardial biopsy) | - | Corticosteroids | Clinical resolution (35 days, but apical ballooning persisted 1 year after) | NR |
| Singhal et al., 2022 [26] | Diarrhea, confusion, fatigue | Apical ballooning, vigorous systolic contraction of mid zones and anterior and inferior walls | + | ST-elevation | + (Trop) | No obstruction | − (no biopsy or MRI performed for exclusion of myocarditis) | DKA | Insulin for DKA | Resolution | + |
| Airo et al., 2022 [27] | Dyspnea, diaphoresis | Apical ballooning, anterior wall and septum akinesis | + | T-wave inversion in V2-4, QT prolongation | + (Trop & BNP) | Non-significant CAD | − (no biopsy or MRI performed for exclusion of myocarditis) | Hepatitis | Corticosteroids, MI and HF management | Resolution (14 days) | + |
| ‘Sotiria’ case | Chest pain, dyspnea, cardiogenic shock | Decreased contractility of left ventricle with apical ballooning | + | ST-elevation V3-6 | + (Trop & BNP) | Non-significant CAD | − (no biopsy or MRI performed for exclusion of myocarditis) | Hepatitis, skin toxicity | Supportive care for cardiogenic shock, anxiolytics | Resolution (7 days, but 2nd event 6 months after which resolved after 10) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trontzas, I.P.; Vathiotis, I.A.; Kyriakoulis, K.G.; Sofianidi, A.; Spyropoulou, Z.; Charpidou, A.; Kotteas, E.A.; Syrigos, K.N.; ImmunoTTS Collaborative Group. Takotsubo Cardiomyopathy in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Summary of Included Cases. Cancers 2023, 15, 2637. https://doi.org/10.3390/cancers15092637
Trontzas IP, Vathiotis IA, Kyriakoulis KG, Sofianidi A, Spyropoulou Z, Charpidou A, Kotteas EA, Syrigos KN, ImmunoTTS Collaborative Group. Takotsubo Cardiomyopathy in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Summary of Included Cases. Cancers. 2023; 15(9):2637. https://doi.org/10.3390/cancers15092637
Chicago/Turabian StyleTrontzas, Ioannis P., Ioannis A. Vathiotis, Konstantinos G. Kyriakoulis, Amalia Sofianidi, Zoi Spyropoulou, Andriani Charpidou, Elias A. Kotteas, Konstantinos N. Syrigos, and ImmunoTTS Collaborative Group. 2023. "Takotsubo Cardiomyopathy in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Summary of Included Cases" Cancers 15, no. 9: 2637. https://doi.org/10.3390/cancers15092637
APA StyleTrontzas, I. P., Vathiotis, I. A., Kyriakoulis, K. G., Sofianidi, A., Spyropoulou, Z., Charpidou, A., Kotteas, E. A., Syrigos, K. N., & ImmunoTTS Collaborative Group. (2023). Takotsubo Cardiomyopathy in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Summary of Included Cases. Cancers, 15(9), 2637. https://doi.org/10.3390/cancers15092637