
Steroid-Refractory Immune-Related Adverse Events Induced by Checkpoint Inhibitors

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
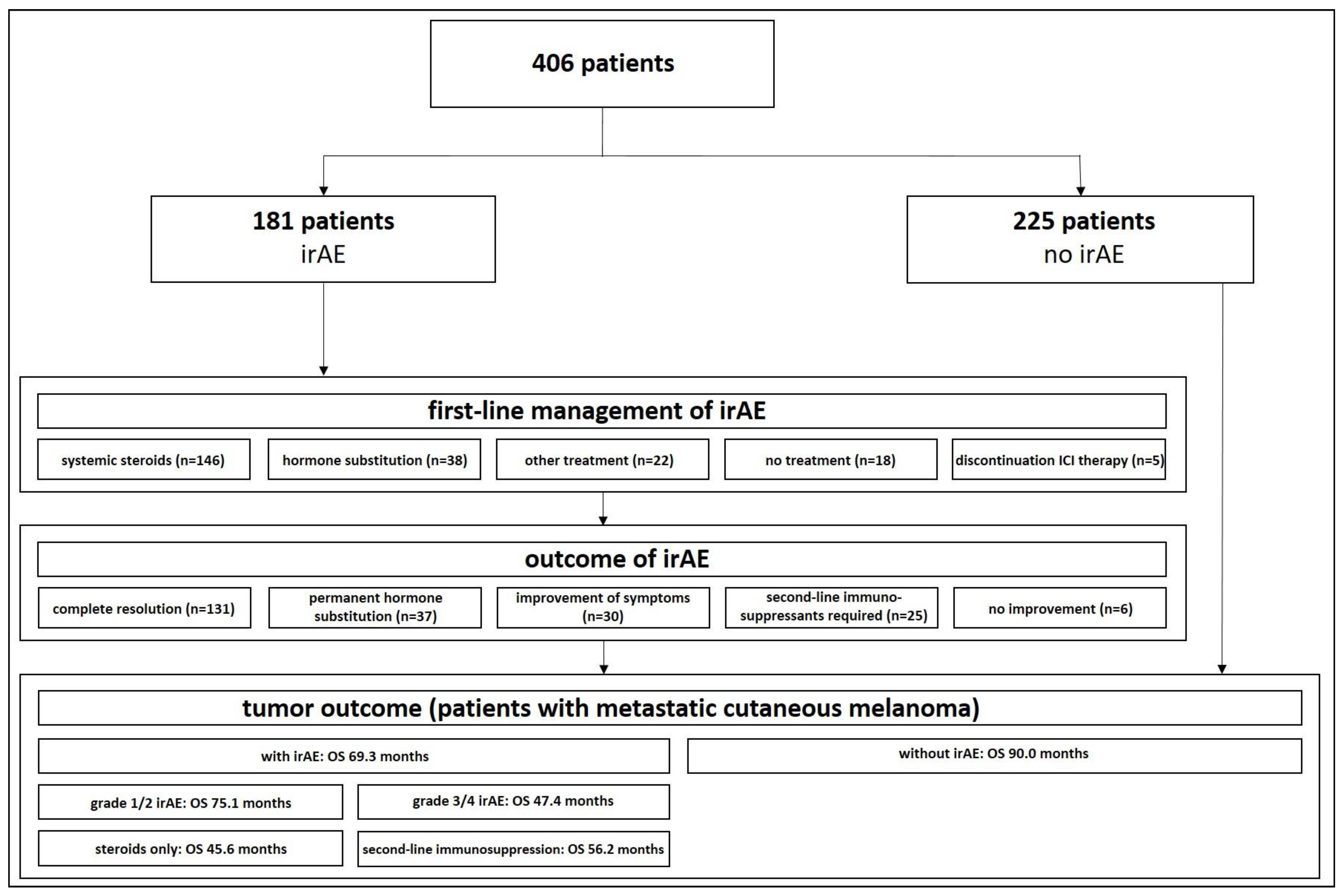
3. Results
3.1. Patients’ Characteristics
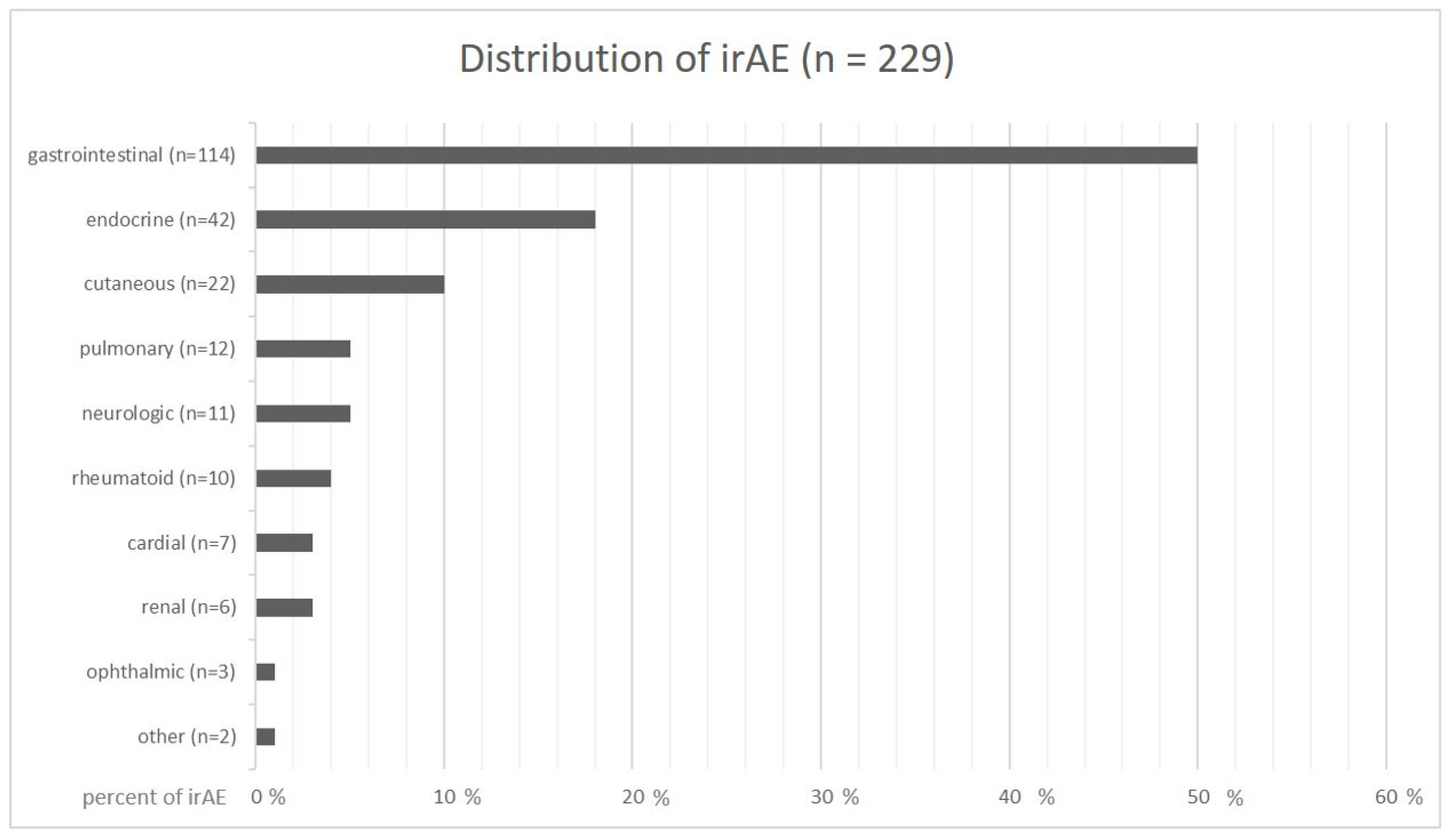
3.2. Distribution and Classification of irAEs
3.3. First-Line Management and Outcome of irAEs
3.4. Incidence of sr-/sd-irAEs
3.5. Second-Line Management
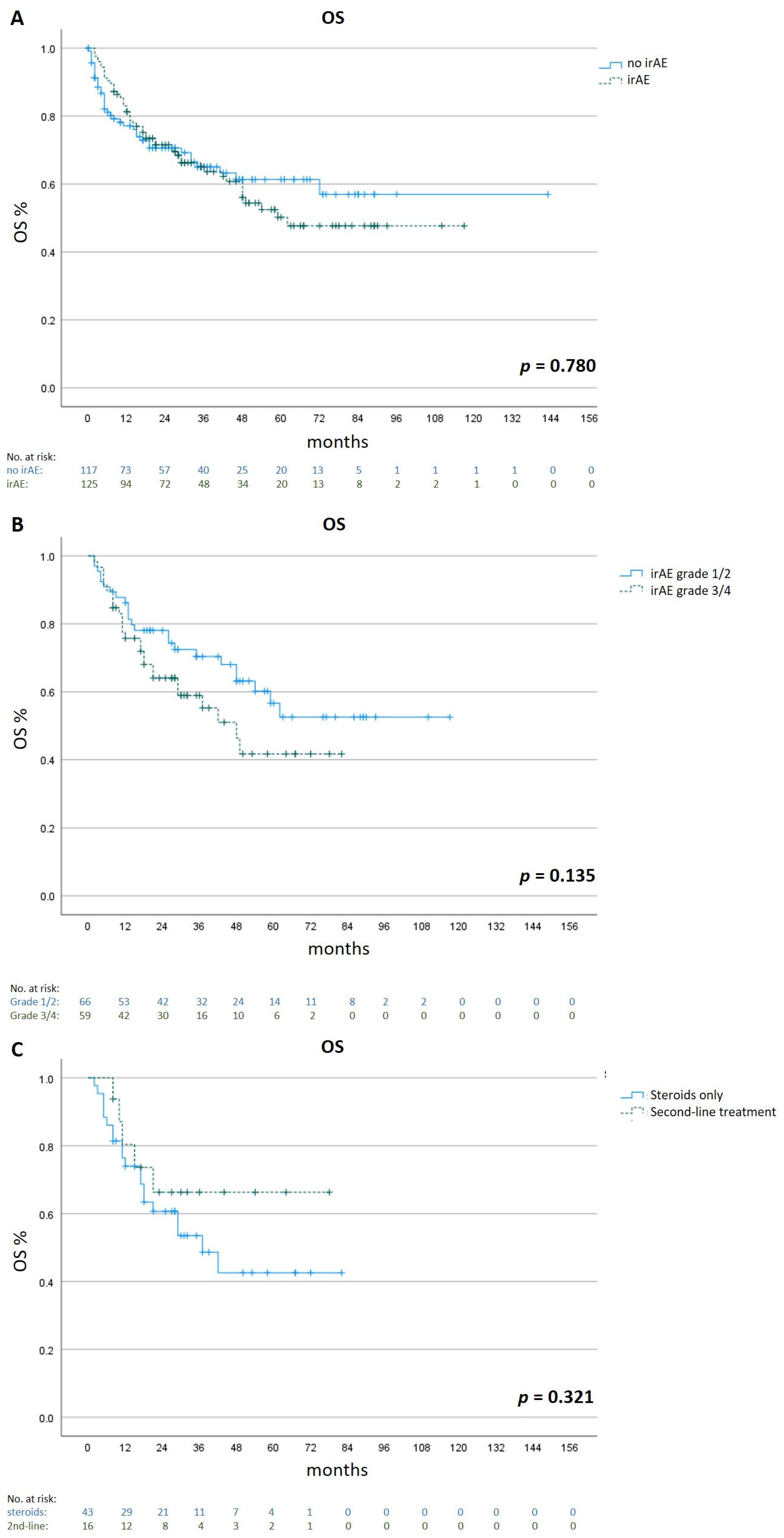
3.6. Survival
3.7. Comparison with Guidelines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vafaei, S.; Zekiy, A.O.; Khanamir, R.A.; Zaman, B.A.; Ghayourvahdat, A.; Azimizonuzi, H.; Zamani, M. Combination therapy with immune checkpoint inhibitors (ICIs); a new frontier. Cancer Cell Int. 2022, 22, 2. [Google Scholar] [CrossRef]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Russell, J.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbé, C.; Linette, G.P.; Milella, M.; et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: A multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 1374–1385. [Google Scholar] [CrossRef]
- Migden, M.R.; Rischin, D.; Schmults, C.D.; Guminski, A.; Hauschild, A.; Lewis, K.D.; Chung, C.H.; Hernandez-Aya, L.F.; Lim, A.M.; Chang, A.L.S.; et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 341–351. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356, Erratum in N. Engl. J. Med. 2018, 379, 2185. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Schadendorf, D.; Lipson, E.J.; Ascierto, P.A.; Matamala, L.; Gutiérrez, E.C.; Rutkowski, P.; Gogas, H.J.; Lao, C.D.; De Menezes, J.J.; et al. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N. Engl. J. Med. 2022, 386, 24–34. [Google Scholar] [CrossRef]
- Schneider, B.J.; Naidoo, J.; Santomasso, B.D.; Lacchetti, C.; Adkins, S.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 4073–4126, Erratum in J. Clin. Oncol.2022, 40, 315. [Google Scholar] [CrossRef]
- Thompson, J.A.; Schneider, B.J.; Brahmer, J.; Achufusi, A.; Armand, P.; Berkenstock, M.K.; Bhatia, S.; Budde, L.E.; Chokshi, S.; Davies, M.; et al. Management of Immunotherapy-Related Toxicities, Version 1.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 387–405. [Google Scholar] [CrossRef]
- Haanen, J.; Obeid, M.; Spain, L.; Carbonnel, F.; Wang, Y.; Robert, C.; Lyon, A.; Wick, W.; Kostine, M.; Peters, S.; et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 1217–1238. [Google Scholar] [CrossRef]
- Husain, B.; Kirchberger, M.C.; Erdmann, M.; Schüpferling, S.; Abolhassani, A.-R.; Fröhlich, W.; Berking, C.; Heinzerling, L. Inflammatory markers in autoimmunity induced by checkpoint inhibitors. J. Cancer Res. Clin. Oncol. 2021, 147, 1623–1630. [Google Scholar] [CrossRef]
- Dimitriou, F.; Hogan, S.; Menzies, A.M.; Dummer, R.; Long, G.V. Interleukin-6 blockade for prophylaxis and management of immune-related adverse events in cancer immunotherapy. Eur. J. Cancer 2021, 157, 214–224. [Google Scholar] [CrossRef]
- Esfahani, K.; Buhlaiga, N.; Thébault, P.; Lapointe, R.; Johnson, N.A.; Miller, W.H., Jr. Alemtuzumab for Immune-Related Myocarditis Due to PD-1 Therapy. N. Engl. J. Med. 2019, 380, 2375–2376. [Google Scholar] [CrossRef]
- Salem, J.E.; Allenbach, Y.; Vozy, A.; Brechot, N.; Johnson, D.B.; Moslehi, J.J.; Kerneis, M. Abatacept for Severe Immune Checkpoint Inhibitor-Associated Myocarditis. N. Engl. J. Med. 2019, 380, 2377–2379. [Google Scholar] [CrossRef]
- Apostolova, P.; Unger, S.; von Bubnoff, D.; Meiss, F.; Becher, B.; Zeiser, R. Extracorporeal Photopheresis for Colitis Induced by Checkpoint-Inhibitor Therapy. N. Engl. J. Med. 2020, 382, 294–296. [Google Scholar] [CrossRef]
- Thomas, A.S.; Ma, W.; Wang, Y. Ustekinumab for Refractory Colitis Associated with Immune Checkpoint Inhibitors. N. Engl. J. Med. 2021, 384, 581–583. [Google Scholar] [CrossRef]
- Ma, V.T.; Lao, C.D.; Fecher, L.A.; Schiopu, E. Successful use of secukinumab in two melanoma patients with immune checkpoint inhibitor-induced inflammatory arthropathy. Immunotherapy 2022, 14, 593–598. [Google Scholar] [CrossRef]
- Johnson, D.; Patel, A.B.; Uemura, M.I.; Trinh, V.A.; Jackson, N.; Zobniw, C.M.; Tetzlaff, M.T.; Hwu, P.; Curry, J.L.; Diab, A. IL17A Blockade Successfully Treated Psoriasiform Dermatologic Toxicity from Immunotherapy. Cancer Immunol. Res. 2019, 7, 860–865. [Google Scholar] [CrossRef]
- Conroy, M.; Naidoo, J. Immune-related adverse events and the balancing act of immunotherapy. Nat. Commun. 2022, 13, 392. [Google Scholar] [CrossRef]
- Schadendorf, D.; Wolchok, J.D.; Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Chesney, J.; et al. Efficacy and Safety Outcomes in Patients With Advanced Melanoma Who Discontinued Treatment With Nivolumab and Ipilimumab Because of Adverse Events: A Pooled Analysis of Randomized Phase II and III Trials. J. Clin. Oncol. 2017, 35, 3807–3814. [Google Scholar] [CrossRef]
- Bai, X.; Hu, J.; Warner, A.B.; Quach, H.T.; Cann, C.G.; Zhang, M.Z.; Si, L.; Tang, B.; Cui, C.; Yang, X.; et al. Early Use of High-Dose Glucocorticoid for the Management of irAE Is Associated with Poorer Survival in Patients with Advanced Melanoma Treated with Anti-PD-1 Monotherapy. Clin. Cancer Res. 2021, 27, 5993–6000. [Google Scholar] [CrossRef]
- Verheijden, R.J.; May, A.M.; Blank, C.U.; Aarts, M.J.; Berkmortel, F.W.V.D.; Eertwegh, A.J.V.D.; de Groot, J.W.B.; Boers-Sonderen, M.J.; van der Hoeven, J.J.; Hospers, G.A.; et al. Association of Anti-TNF with Decreased Survival in Steroid Refractory Ipilimumab and Anti-PD1-Treated Patients in the Dutch Melanoma Treatment Registry. Clin. Cancer Res. 2020, 26, 2268–2274. [Google Scholar] [CrossRef]
- Perez-Ruiz, E.; Minute, L.; Otano, I.; Alvarez, M.; Ochoa, M.C.; Belsue, V.; De Andrea, C.; Rodriguez-Ruiz, M.E.; Perez-Gracia, J.L.; Marquez-Rodas, I.; et al. Prophylactic TNF blockade uncouples efficacy and toxicity in dual CTLA-4 and PD-1 immunotherapy. Nature 2019, 569, 428–432. [Google Scholar] [CrossRef]
- Montfort, A.; Filleron, T.; Virazels, M.; Dufau, C.; Milhès, J.; Pagès, C.; Olivier, P.; Ayyoub, M.; Mounier, M.; Lusque, A.; et al. Combining Nivolumab and Ipilimumab with Infliximab or Certolizumab in Patients with Advanced Melanoma: First Results of a Phase Ib Clinical Trial. Clin. Cancer Res. 2021, 27, 1037–1047. [Google Scholar] [CrossRef]
- Luo, J.; Beattie, J.A.; Fuentes, P.; Rizvi, H.; Egger, J.V.; Kern, J.A.; Leung, D.Y.; Lacouture, M.E.; Kris, M.G.; Gambarin, M.; et al. Beyond Steroids: Immunosuppressants in Steroid-Refractory or Resistant Immune-Related Adverse Events. J. Thorac. Oncol. 2021, 16, 1759–1764. [Google Scholar] [CrossRef]
- Zhang, Q.; Tang, L.; Zhou, Y.; He, W.; Li, W. Immune Checkpoint Inhibitor-Associated Pneumonitis in Non-Small Cell Lung Cancer: Current Understanding in Characteristics, Diagnosis, and Management. Front. Immunol. 2021, 12, 663986. [Google Scholar] [CrossRef]
- Schulz, T.U.; Zierold, S.; Sachse, M.M.; Pesch, G.; Tomsitz, D.; Schilbach, K.; Kähler, K.C.; French, L.E.; Heinzerling, L. Persistent immune-related adverse events after cessation of checkpoint inhibitor therapy: Prevalence and impact on patients’ health-related quality of life. Eur. J. Cancer 2022, 176, 88–99. [Google Scholar] [CrossRef]
- Patrinely, J.R., Jr.; Young, A.C.; Quach, H.; Williams, G.R.; Ye, F.; Fan, R.; Horn, L.; Beckermann, K.E.; Gillaspie, E.A.; Sosman, J.A.; et al. Survivorship in immune therapy: Assessing toxicities, body composition and health-related quality of life among long-term survivors treated with antibodies to programmed death-1 receptor and its ligand. Eur. J. Cancer 2020, 135, 211–220. [Google Scholar] [CrossRef]
- Nuñez, N.G.; Berner, F.; Friebel, E.; Unger, S.; Wyss, N.; Gomez, J.M.; Purde, M.-T.; Niederer, R.; Porsch, M.; Lichtensteiger, C.; et al. Immune signatures predict development of autoimmune toxicity in patients with cancer treated with immune checkpoint inhibitors. Med 2023, 4, 113–129.e7. [Google Scholar] [CrossRef]
- Lorentzen, C.L.; Haanen, J.B.; Met, Ö.; Svane, I.M. Clinical advances and ongoing trials on mRNA vaccines for cancer treatment. Lancet Oncol. 2022, 23, e450–e458, Erratum in Lancet Oncol.2022, 23, e492. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Van Not, O.J.; Verheijden, R.J.; van den Eertwegh, A.J.M.; Haanen, J.B.A.G.; Aarts, M.J.B.; Berkmortel, F.W.P.J.V.D.; Blank, C.U.; Boers-Sonderen, M.J.; de Groot, J.-W.B.; Hospers, G.A.P.; et al. Association of Immune-Related Adverse Event Management with Survival in Patients with Advanced Melanoma. JAMA Oncol. 2022, 8, 1794–1801. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients | |
|---|---|
| n = 406 | |
| Age—years | |
| Mean | 64.0 |
| Range | 22–91 |
| Sex—no. (%) | |
| Male | 234 (57.6) |
| Female | 172 (42.4) |
| Tumor type—no. (%) | |
| Cutaneous melanoma | 296 (72.9) |
| Melanoma of unknown primary | 45 (11.1) |
| Mucosal melanoma | 13 (3.2) |
| Conjunctival melanoma | 2 (0.5) |
| Uveal melanoma | 33 (8.1) |
| Cutaneous squamous cell carcinoma | 11 (2.7) |
| Eccrine porocarcinoma | 1 (0.2) |
| Basal cell carcinoma | 2 (0.5) |
| Merkel cell carcinoma | 3 (0.7) |
| Treatment setting—no. (%) | |
| Neoadjuvant | 10 (0.2) |
| Adjuvant | 86 (21.2) |
| Metastatic | 310 (76.4) |
| Treatment—no. (%) | |
| Avelumab | 1 (0.2) |
| Cemiplimab | 13 (3.2) |
| Ipilimumab | 15 (3.7) |
| Nivolumab | 75 (18.5) |
| Pembrolizumab | 129 (31.8) |
| Ipilimumab + nivolumab | 173 (42.6) |
| Occurrence of irAE—no. (%) | |
| No | 225 (55.4) |
| Yes | 181 (44.6) |
| Type of irAE | Highest Grade | Time of Onset after Initiation ICI | Management | Time to First Significant Response of irAEs (If Responsive) | Outcome | |||
|---|---|---|---|---|---|---|---|---|
| Gastrointestinal irAEs | ||||||||
| irHepatitis (n = 44) | 1 | n = 3 | 4.4 months (range: 0.25–48 months) | Continue ICI-therapy (no intervention) | n = 3 | 3.6 days (range: 1–7 days) | Resolved | n = 33 |
| 2 | n = 14 | |||||||
| 3 | n = 17 | Systemic cort icosteroids | n = 41 | Improved, but not resolved | n = 4 | |||
| 4 | n = 10 | Second-line treatment required | n = 7 | |||||
| irColitis (n = 50) | 1 | n = 0 | 2.8 months (range: 0.07–26 months) | Continue ICI-therapy (no intervention) | n = 2 | 4.8 days (range: 1–56 days) | Resolved | n = 35 |
| 2 | n = 17 | Systemic steroids | n = 43 | Improved, but not resolved | n = 3 | |||
| 3 | n = 28 | Mesalazin | n = 1 | |||||
| 4 | n = 3 | Unknown | n = 4 | Second-line treatment required | n = 12 | |||
| 5 | n = 0 | |||||||
| Unknown | n = 2 | |||||||
| irPancreatitis (n = 16) | 2 | n = 6 | 6.6 months (range: 0.5–25 months) | Continue ICI-therapy (No intervention) | n = 7 | 8.6 days (range: 1–28 days) | Resolved | n = 10 |
| 3 | n = 8 | |||||||
| Interruption ICI-therapy | n = 2 | Improved, but not resolved | n = 4 | |||||
| 4 | n = 2 | |||||||
| Systemic corticosteroids | n = 7 | Ongoing | n = 2 | |||||
| 5 | n = 0 | |||||||
| irGastritis (n = 3) | 1 | n = 0 | 4.3 months (range: 3–6 months) | Continue ICI-therapy (no intervention) | n = 1 | 3.0 days (range: 3.0–3.0 days) | Resolved | n = 2 |
| 2 | n = 2 | |||||||
| 3 | n = 1 | |||||||
| Systemic steroids | n = 2 | Improved, but not resolved | n = 1 | |||||
| 4 | n = 0 | |||||||
| 5 | n = 0 | |||||||
| irCholecystitis (n = 1) | 2 | n = 0 | 2.0 months (range: 2–2 months) | Systemic corticosteroids | n = 1 | n/a (no improvement) | No improvement | n = 1 |
| 3 | n = 0 | |||||||
| 4 | n = 1 | |||||||
| 5 | n = 0 | |||||||
| Pulmonary irAEs | ||||||||
| irPneumonitis (n = 11) | 1 | n = 1 | 6.4 months (range: 1–24 months) | Continue ICI-therapy (no intervention) | n = 1 | 7.2 days (range: 3 days–28 days) | Resolved | n = 7 |
| 2 | n = 8 | |||||||
| 3 | n = 2 | Systemic steroids | n = 10 | Improved, but not resolved | n = 4 | |||
| 4 | n = 0 | |||||||
| 5 | n = 0 | |||||||
| irSarcoidosis (n = 1) | n/a | n = 1 | 6.0 months (range: 6–6 months) | Inhalative corticosteroids | n = 1 | 7.0 days (range: 7–7 days) | Improved, but not resolved | n = 1 |
| Endocrine irAEs | ||||||||
| irThyroiditis (n = 18) | 1 | n = 4 | 2.8 months (range: 0.25–11 months) | Continue ICI-therapy (no intervention) | n = 1 | 2.4 days (range: 1–28 days) | Resolved | n = 2 |
| 2 | n = 14 | |||||||
| Systemic steroids | n = 1 | |||||||
| 3 | n = 0 | Ongoing insufficiency requiring hormone substitution | n = 16 | |||||
| 4 | n = 0 | Hormone substitution | n = 16 | |||||
| 5 | n = 0 | |||||||
| irHypophysitis (n = 19) | 1 | n = 0 | 4.0 months (range 0.25–21 months) | Permanently discontinuation ICI | n = 1 | 1.9 days (range: 1–14 days) | Resolved | n = 3 |
| 2 | n = 12 | |||||||
| 3 | n = 7 | Hormone substitution | n = 17 | Ongoing insufficiency requiring hormone substitution | n = 16 | |||
| 4 | n = 0 | Unknown | n = 1 | |||||
| 5 | n = 0 | |||||||
| irAdrenalitis (n = 4) | 1 | n = 0 | 2.9 months (range 1.5–4 months) | Hormone substitution | n = 4 | 1.0 day (range: 1–1 day) | Ongoing insufficiency requiring hormone substitution | n = 4 |
| 2 | n = 1 | |||||||
| 3 | n = 3 | |||||||
| 4 | n = 0 | |||||||
| 5 | n = 0 | |||||||
| irDiabetes (n = 1) | n/a | n = 1 | 3 months (range 3–3 months) | Hormone substitution | n = 1 | 1.0 day (range 1–1 day) | Ongoing insufficiency requiring hormone substitution | n = 1 |
| Renal irAEs | ||||||||
| irNephritis (n = 6) | 3 | n = 5 | 2.7 months (range 0.25–4 months) | Systemic corticosteroids | n = 6 | 5.5 days (range 3–14 days) | Resolved | n = 5 |
| 4 | n = 1 | |||||||
| improved, but not resolved | n = 1 | |||||||
| 5 | n = 0 | |||||||
| Cardiac irAEs | ||||||||
| irMyocarditis (n = 7) | 2 | n = 4 | 4.3 months (range 0.5–22 months) | Interruption of ICI therapy | n = 1 | 8.7 days (range 3–14 days) | Resolved | n = 6 |
| 3 | n = 3 | |||||||
| 4 | n = 0 | Systemic corticosteroids | n = 6 | Second-line treatment required | n = 1 | |||
| 5 | n = 0 | |||||||
| Cutaneous irAEs | ||||||||
| irDermatitis (n = 22) (maculopapular rash n = 15, lichenoid rash n = 4, bullous pemphigoid n = 2, alopecia n = 1) | 1 | n = 16 | 4.2 months (range 0.1–21 months) | Continue ICI-therapy (no intervention) | n = 1 | 9.5 days (range 1–28 days) | Resolved | n = 12 |
| 2 | n = 4 | |||||||
| Improved, but not resolved | n = 5 | |||||||
| Topical corticosteroids | n = 17 | |||||||
| 3 | n = 1 | Not improved | n = 2 | |||||
| n/a | n = 1 | Systemic corticosteroids | n = 4 | |||||
| Second-line treatment required | n = 3 | |||||||
| Rheumatoid irAEs | ||||||||
| irArthritis (n = 10) | 1 | n = 0 | 3.3 months (range 0.03–11 months) | NSAIDs | n = 1 | 5.5 days (range 1–21 days) | Resolved | n = 3 |
| 2 | n = 10 | Systemic corticosteroids | n = 7 | Improved, but not resolved | n = 5 | |||
| 3 | n = 0 | Systemic + intralesional corticosteroids | n = 2 | Second-line treatment required | n = 2 | |||
| Ophthalmic irAEs | ||||||||
| Ophthalmic irAEs (n = 3) (uveitis n = 1, conjunctivitis n = 1, papillitis n = 1) | 1 | n = 0 | 9.6 months (range 9–11 months) | Intravitreal corticosteroids | n = 1 | 8.0 days (range 3–14 days) | Resolved | n = 3 |
| 2 | n = 2 | |||||||
| Topical corticosteroids | n = 1 | |||||||
| 3 | n = 0 | |||||||
| 4 | n = 0 | Interruption of ICI-therapy (no intervention) | n = 1 | |||||
| n/a | n = 1 | |||||||
| Neurologic irAEs | ||||||||
| Neurologic irAEs (n = 11) (myositis n = 1, myasthenia gravis n = 1, myalgia n = 1, CPK increased n = 1, polyneuritis n = 1, vocal cord paresis n = 1, bilateral vestibulopathy n = 2, limbic encephalitis n = 1, peripheral sensory polyneuropathy n = 2) | 1 | n = 1 | 2.1 months (range 1.5–5 months) | Continue ICI-therapy (no intervention) | n = 2 | 7.0 days (range1–14 days) | Resolved | n = 9 |
| 2 | n = 4 | Discontinuation ICI therapy (no intervention) | n = 2 | |||||
| Systemic corticosteroids | n = 4 | |||||||
| 3 | n = 3 | Systemic corticosteroids + intralesional corticosteroids | n = 1 | Improved, but not resolved | n = 2 | |||
| 4 | n = 0 | |||||||
| systemic corticosteroids (high dose) | n = 2 | |||||||
| 5 | n = 0 | |||||||
| n/a | n = 3 | |||||||
| Other irAEs | ||||||||
| CD4 + -count-decreased n = 1, polyserositis n = 1 | 1 | n = 0 | 4.5 months (range 3–6 months) | permanent interruption of ICI therapy | n = 1 | 7 days (range 7–7 days) | resolved | n = 1 |
| 2 | n = 0 | |||||||
| 3 | n = 1 | |||||||
| 4 | n = 1 | systemic corticosteroids | n = 1 | no improvement | n = 1 | |||
| Type of irAE | Total Number of irAEs | irAEs Treated with Systemic Steroids | sr/sd-irAEs | Percentage of sr/sd-irAEs (%) |
|---|---|---|---|---|
| irHepatitis | 44 | 41 | 11 | 26.8 |
| irColitis | 50 | 43 | 15 | 34.9 |
| irPancreatitis | 16 | 7 | 1 | 14.3 |
| irGastritis | 3 | 2 | 0 | 0 |
| irPneumonitis | 11 | 10 | 4 | 40.0 |
| irNephritis | 6 | 6 | 1 | 16.7 |
| irMyocarditis | 7 | 6 | 1 | 16.7 |
| irDermatitis | 22 | 4 | 3 | 75.0 |
| irArthritis | 10 | 9 | 7 | 77.8 |
| Neurologic irAEs | 11 | 7 | 2 | 25.6 |
| irAE | Second-Line Treatment | Mean Time to First Response of irAE | Outcome |
|---|---|---|---|
| irColitis (n = 12) | Infliximab 5 mg/kg 1 dose (n = 6) 2 doses (n = 6) | 1.3 days (0 days–7 days) | Complete resolution (n = 9) Improvement, but not resolution (n = 1) Third-line therapy (n = 2) |
| irHepatitis (n = 7) | Mycophenolate-mofetil 1g/day (n = 2) 2g/day (n = 5) | 2.8 days (2 days–7 days) | Complete resolution (n = 5) Improvement, but no resolution (n = 1) Third-line therapy (n = 1) |
| irDermatitis (lichenoid rash n = 2, bullous drug reaction n = 1) | Acitretin 10 mg xtracorporeal photopheresis IVIG 2g/kg | 4 weeks 6 weeks 3 weeks | Improvement, but no resolution (n = 3) |
| irArthritis (n = 2) | Methotrexate 15 mg/week s.c. | 6 weeks–3 months | Improvement, but no resolution (n = 2) |
| irMyocarditis (n = 1) | IVIG 2g/kg | 2 weeks | Resolved |
| Type of irAE | ASCO Guidelines | NCCN Guidelines | ESMO Guidelines | Patient Cohort | |
|---|---|---|---|---|---|
| Skin Toxicities | Maculopapular rash | Infliximab, tocilizumab | |||
| Bullous dermatoses | Rituximab | IVIG (1/1) | |||
| Other cutaneous adverse reactions | IVIG/cyclosporine | ||||
| irLichen ruber | Acitretin (1/2), ECP (1/2) | ||||
| Gastrointestinal Toxicities | irColitis | Infliximab/TNF-α blocker, Vedolizumab if refractory to TNF-α blocker | Infliximab, vedolizumab | Infliximab, if not responsive, higher-dose infliximab, ustekinumab, tofacitinib, extracorporeal photopheresis, fecal microbiota transplantation | Infliximab (12/12) |
| irHepatitis | Grade 3: mycophenolate mofetil/azathioprine Grade 4: mycophenolate mofetil (avoid infliximab) | Mycophenolate mofetil (infliximab not recommended) | Mycophenolate mofetil, tocilizumab, tacrolimus, azathioprine, cyclosporine, antithymocyte globulin | Mycophenolate mofetil (7/7) | |
| irPancreatitis | |||||
| Lung Toxicity | irPneumonitis | Infliximab/mycophenolate mofetil/IVIG/cyclophosphamide | Infliximab, mycophenolate mofetil, IVIG | Tocilizumab, infliximab, IVIG, mycophenolate mofetil, cyclophosphamide | |
| Musculoskeletal Toxicities | irArthritis | Methotrexate, leflunomide, TNF-α inhibitor, IL-6 receptor inhibitor (not to be used in patients with colitis) | Infliximab, methotrexate, tocilizumab, sulfasalazine, azathioprine, leflunomide, IVIG | Methotrexate, azathioprine, mycophenolate mofetil, tacrolimus, | Methotrexate (2/2) |
| irMyositis | Plasmapheresis, IVIG, methotrexate, azathioprine, mycophenolate mofetil | Tocilizumab, TNF-α inhibitor | |||
| Polymyalgia-like syndrome | Methotrexate, IL-6 receptor inhibition (not to be used in patients with colitis) | ||||
| Renal Toxicities | irNephritis | Mycophenolate mofetil | Azathioprine, cyclophosphamide, infliximab, mycophenolate mofetil | ||
| Nervous System Toxicities | irMyasthenia gravis | IVIG/plasmapheresis | Abatacept, tacrolimus, cyclophosphamide, rituximab, infliximab, tocilizumab, azathioprine, mycophenolate mofetil | ||
| irGuillain–Barré syndrome | IVIG/plasmapheresis | IVIG, plasmapheresis | Plasmapheresis, IVIG | ||
| Peripheral neuropathy | According to Guillain-Barré syndrome management | According to Guillain–Barré syndrome management | IVIG | ||
| Aseptic meningitis | |||||
| Encephalitis | IVIG/rituximab/plasmapheresis | IVIG, rituximab | |||
| Transverse myelitis | IVIG | IVIG, plasmapheresis | Plasmapheresis | ||
| Hematologic Toxicities | irHemolytic anemia | Rituximab, IVIG, cyclosporine A, mycophenolate mofetil | |||
| irThromocytopenic purpura | Plasmapheresis, rituximab | ||||
| irAplastic anemia | Horse antithymocyte globulin + cyclosporine A, if no response, rabbit antithymocyte globulin + cyclosporine/cyclophosphamide | ||||
| irThromocytopenia | IVIG, rituximab | IVIG, eltrombopag | |||
| irHemophilia | Rituximab/cyclophosphamide, cyclosporine, immunoadsorption | ||||
| irAgranuloytosis | |||||
| irHematophagocytic lymphohistiocytosis | Tocilizumab | ||||
| Cardiovascular Toxicities | irMyocarditis, irPericarditis | Mycophenolate mofetil, infliximab, antithymocyte globulin | Antithymocyte globulin, infliximab, IVIG, mycophenolate mofetil | Tocilizumab, mycophenolate mofetil, antithymocyte globulin, alemtuzumab, abatacept | IVIG (1/1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomsitz, D.; Ruf, T.; Zierold, S.; French, L.E.; Heinzerling, L. Steroid-Refractory Immune-Related Adverse Events Induced by Checkpoint Inhibitors. Cancers 2023, 15, 2538. https://doi.org/10.3390/cancers15092538
Tomsitz D, Ruf T, Zierold S, French LE, Heinzerling L. Steroid-Refractory Immune-Related Adverse Events Induced by Checkpoint Inhibitors. Cancers. 2023; 15(9):2538. https://doi.org/10.3390/cancers15092538
Chicago/Turabian StyleTomsitz, Dirk, Theresa Ruf, Sarah Zierold, Lars E. French, and Lucie Heinzerling. 2023. "Steroid-Refractory Immune-Related Adverse Events Induced by Checkpoint Inhibitors" Cancers 15, no. 9: 2538. https://doi.org/10.3390/cancers15092538
APA StyleTomsitz, D., Ruf, T., Zierold, S., French, L. E., & Heinzerling, L. (2023). Steroid-Refractory Immune-Related Adverse Events Induced by Checkpoint Inhibitors. Cancers, 15(9), 2538. https://doi.org/10.3390/cancers15092538