
A Phase I Dose Escalation and Expansion Study of Epidiolex (Cannabidiol) in Patients with Biochemically Recurrent Prostate Cancer

 , , , , ,
, , , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Study Design
- Complete Biochemical Response: Normalization of PSA (PSA level becomes undetectable) documented by two different measurements taken at least 4 weeks apart.
- Partial Biochemical Response: Reduction in PSA of ≥25% (from baseline) documented by two different measurements taken at least 4 weeks apart.
- Stable Biochemical Disease: An increase in baseline PSA of <25% documented by two different measurements taken at least 4 weeks apart.
- PSA Progression: An increase in baseline PSA of ≥50% documented by two different measurements taken at least 4 weeks apart.
- Clinical Progression: Any positive metastases findings on a bone scan and/or CT scan of the abdomen or pelvis or Axium PET/CT scan or development of symptoms attributable to cancer progression.
2.3. Patient-Reported Outcomes (PROs)
2.4. Statistical Analysis
3. Results
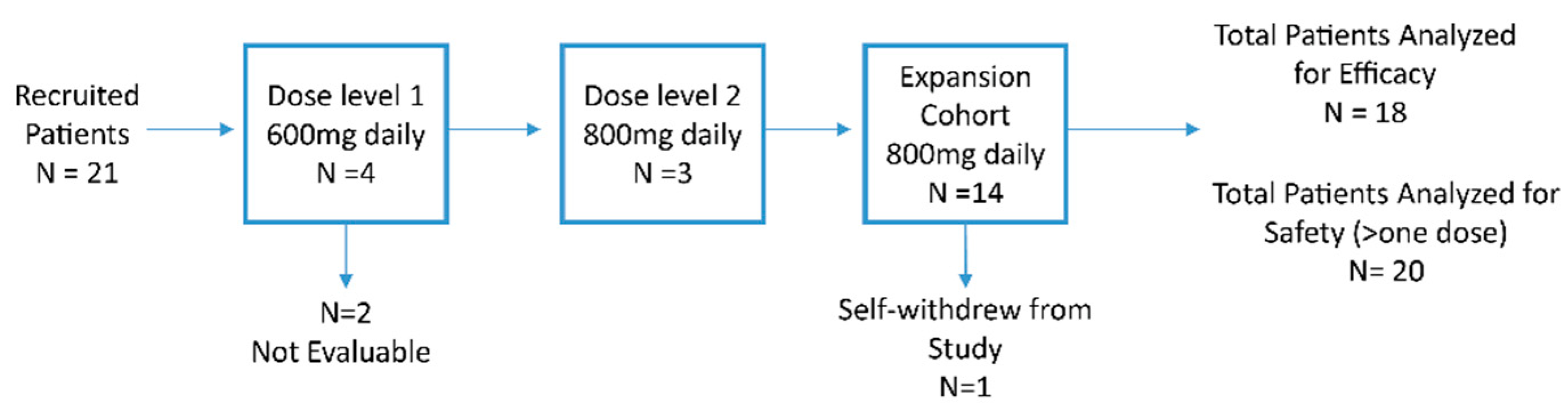
3.1. Phase I Dose Escalation
3.2. Baseline Characteristics
3.3. Treatment-Related Adverse Events
3.4. Preliminary Anti-Tumor Activity
3.5. Preliminary Patient-Reported Outcomes
3.6. Biomarker Assessment CB1 Receptor Expression Level by Immunohistochemistry
3.6.1. Background
3.6.2. Method
3.6.3. Result
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferraro, S.; Bussetti, M.; Bassani, N.; Rossi, R.S.; Incarbone, G.P.; Bianchi, F.; Maggioni, M.; Runza, L.; Ceriotti, F.; Panteghini, M. Definition of Outcome-Based Prostate-Specific Antigen (PSA) Thresholds for Advanced Prostate Cancer Risk Prediction. Cancers 2021, 13, 3381. [Google Scholar] [CrossRef] [PubMed]
- Cookson, M.S.; Aus, G.; Burnett, A.L.; Canby-Hagino, E.D.; D’Amico, A.V.; Dmochowski, R.R.; Eton, D.T.; Forman, J.D.; Goldenberg, S.L.; Hernandez, J.; et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: The American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J. Urol. 2007, 177, 540–545. [Google Scholar] [PubMed]
- Roach, M.; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of prostate cancer specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Pinover, W.H.; Horwitz, E.M.; Hanlon, A.L.; Uzzo, R.G.; Hanks, G.E. Validation of a treatment policy for patients with prostate specific antigen failure after three dimensional conformal prostate radiation therapy. Cancer 2003, 97, 1127–1133. [Google Scholar] [CrossRef]
- Zagars, G.K.; Pollack, A. Kinetics of serum prostate specific antigen after external beam radiation for clinically localized prostate cancer. Radiother. Oncol. 1997, 44, 213–221. [Google Scholar] [CrossRef]
- Patel, A.; Dorey, F.; Franklin, J.; de Kernion, J.B. Recurrence patterns after radical retropubic prostatectomy: Clinical usefulness of prostate specific antigen doubling times and log slope prostate specific antigen. J. Urol. 1997, 158, 1441–1445. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Tafuri, A.; Sebben, M.; Amigoni, N.; Processali, T.; Pirozzi, M.; Rizzetto, R.; Shakir, A.; Corsi, P.; Tiso, L.; et al. High surgeon volume and positive surgical margins can predict the risk of biochemical recurrence after robot-assisted radical prostatectomy. Ther. Adv. Urol. 2019, 11, 1756287219878283. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Rafuri, A.; Sebben, M.; Amigoni, N.; Shakir, A.; Corsi, P.; Processali, T.; Pirozzi, M.; Rizzetto, R.; Bernasconi, R.; et al. Linear extent of positive surgical margin impacts biochemical recurrence after robot-assited radical prostatectomy in a high volume center. J. Robot. Surg. 2020, 14, 663–675. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Available online: https://www.nccn.org/ (accessed on 20 December 2021).
- Garcia-Albeniz, X.; Chan, J.M.; Paciorek, A.; Logan, R.W.; Kenfield, S.A.; Cooperberg, M.R.; Carroll, P.R.; Hernan, M.A. Immediate versus deferred initiation of androgen deprivation therapy in prostate cancer patients with PSA-only relapse. An observational follow-up study. Eur. J. Cancer. 2015, 51, 817–824. [Google Scholar] [CrossRef]
- Byar, D.P.; Corle, D.K. Hormone therapy for prostate cancer: Results of the Veterans Administration Cooperative Urological Research Group studies. In NCI Monographs; National Cancer Institute: Bethesda, MA, USA, 1988; pp. 165–170. [Google Scholar]
- McLeod, D.G.; Iversen, P.; See, W.A.; Morris, T.; Armstrong, J.; Wirth, M.P. Casodex Early Prostate Cancer Trialists’ Group. Bicalutamide 150 mg plus standard care vs standard care alone for early prostate cancer. BJU Int. 2006, 97, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Zareba, P.; Duivenvoorden, W.; Leong, D.P.; Pinthus, J.H. Androgen deprivation therapy and cardiovascular disease: What is the linking mechanism? Ther. Adv. Urol. 2016, 8, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Burnell-Nugent, M.; Lossignol, D.; Ganae-Motan, E.D.; Potts, R.; Fallon, M.T. Multicenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain. J. Pain. Symptom Manag. 2010, 39, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Machado Rocha, F.C.; Stefano, S.C.; De Cassia Haiek, R.; Rosa Oliveira, L.M.; Da Silveira, D.X. Therapeutic use of Cannabis sativa on chemotherapy-induced nausea and vomiting among cancer patients: Systematic review and meta-analysis. Eur. J. Cancer Care 2008, 17, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.K.; Ganae-Motan, E.D.; Allende, S.; Yanagihara, R.; Shaiova, L.; Weinstein, S.; McQuade, R.; Wright, S.; Fallon, M.T. Nabiximols for opioid-treated cancer patients with poorly-controlled chronic pain: A randomized, placebo-controlled, graded-dose trial. J. Pain 2012, 13, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Tramer, M.R.; Carroll, D.; Campbell, F.A.; Reynolds, D.J.; Moore, R.A.; McQuay, H.J. Cannabinoids for control of chemotherapy induced nausea and vomiting: Quantitative systematic review. BMJ 2001, 323, 16–21. [Google Scholar] [CrossRef]
- Bridgeman, M.B.; Abazia, D.T. Medicinal Cannabis: History, Pharmacology, And Implications for the Acute Care Setting. Pharm. Ther. 2017, 42, 180–188. [Google Scholar]
- Kolodny, R.C.; Masters, W.H.; Kolodner, R.M.; Toro, G. Depression of plasma testosterone levels after chronic intensive marihuana use. N. Engl. J. Med. 1974, 290, 872–874. [Google Scholar] [CrossRef]
- Sarfaraz, S.; Afaq, F.; Adhami, V.M.; Mukhtar, H. Cannabinoid receptor as a novel target for the treatment of prostate cancer. Cancer Res. 2005, 65, 1635–1641. [Google Scholar] [CrossRef]
- Sarfaraz, S.; Afaq, F.; Adhami, V.M.; Malik, A.; Mukhtar, H. Cannabinoid receptor agonist-induced apoptosis of human prostate cancer cells LNCaP proceeds through sustained activation of ERK1/2 leading to G1 cell cycle arrest. J. Biol. Chem. 2006, 281, 39480–39491. [Google Scholar] [CrossRef]
- De Petrocellis, L.; Ligresti, A.; Schiano Moriello, A.; Lappelli, M.; Verde, R.; Stott, C.G.; Cristino, L.; Orlando, P.; Marzo, V.D. Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: Pro-apoptotic effects and underlying mechanisms. Br. J. Pharmacol. 2013, 168, 79–102. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Cross, J.H.; Laux, L.; Marsh, E.; Miller, I.; Nabbout, R.; Scheffer, I.E.; Thiele, E.A.; Wright, S. Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome. N. Engl. J. Med. 2017, 376, 2011–2020. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210365lbl.pdf (accessed on 20 December 2021).
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- van Andel, G.; Bottomley, A.; Fossa, S.D.; Efficace, F.; Coens, C.; Guerif, S.; Kynaston, H.; Gontero, P.; Thalmann, G.; Akdas, A.; et al. An international field study of the EORTC QLQ-PR25: A questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur. J. Cancer 2008, 44, 2418–2424. [Google Scholar] [CrossRef]
- Marchalant, Y.; Brownjohn, P.W.; Bonnet, A.; Kleffmann, T.; Ashton, J.C. Validating Antibodies to the Cannabinoid CB2 Receptor: Antibody Sensitivity Is Not Evidence of Antibody Specificity. J. Histochem. Cytochem. 2014, 62, 395–404. [Google Scholar] [CrossRef]
- Daniels, K.E.; Luginbuhl, A.J.; Mardekian, S.K.; Cognetti, D.M.; Curry, J.M.; South, A.P. Assessment of quality and consistency of monoclonal antibodies for CB1 and CB2 in head and neck squamous cell carcinoma. Head Neck 2019, 41, 3105–3113. [Google Scholar] [CrossRef]
- Brown, J.D.; Winterstein, A.G. Potential Adverse Drug Events and Drug-Drug Interactions with Medical and Consumer Cannabidiol (CBD) Use. J. Clin. Med. 2019, 8, 989. [Google Scholar] [CrossRef]
- van Ours, J.C.; Williams, J.; Fergusson, D.; Horwood, L.J. Cannabis use and suicidal ideation. J. Health Econ. 2013, 32, 524–537. [Google Scholar] [CrossRef]
- Lima, I.V.A.; Bellozi, P.M.Q.; Batista, E.M.; Vilela, L.R.; Brandao, I.L.; Ribeiro, F.M.; Dutra Moraes, M.F.; Moreira, F.A.; de Oliveira, A.C.P. Cannabidiol anticonvulsant effect is mediated by the PI3Kgamma pathway. Neuropharmacology 2020, 176, 108156. [Google Scholar] [CrossRef]
- Carracedo, A.; Gironella, M.; Lorente, M.; Garcia, S.; Guzman, M.; Velasco, G.; Lovanna, J.L. Cannabinoids induce apoptosis of pancreatic tumor cells via endoplasmic reticulum stress-related genes. Cancer Res. 2006, 66, 6748–6755. [Google Scholar] [CrossRef]
- Velasco, G.; Sanchez, C.; Guzman, M. Endocannabinoids and Cancer. Handb. Exp. Pharmacol. 2015, 231, 449–472. [Google Scholar] [CrossRef]
- Demuth, D.G.; Molleman, A. Cannabinoid signalling. Life Sci. 2006, 78, 549–563. [Google Scholar] [CrossRef] [PubMed]
- Velasco, G.; Sanchez, C.; Guzman, M. Anticancer mechanisms of cannabinoids. Curr. Oncol. 2016, 23, S23–S32. [Google Scholar] [CrossRef] [PubMed]
- Caffarel, M.M.; Andradas, C.; Perez-Gomez, E.; Guzman, M.; Sanchez, C. Cannabinoids: A new hope for breast cancer therapy? Cancer Treat. Rev. 2012, 38, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Daris, B.; Tancer Verboten, M.; Knez, Z.; Ferk, P. Cannabinoids in cancer treatment: Therapeutic potential and legislation. Bosn. J. Basic. Med. Sci. 2019, 19, 14–23. [Google Scholar] [CrossRef]
- Turcotte, C.; Blanchet, M.R.; Laviolette, M.; Flamand, N. The CB2 receptor and its role as a regulator of inflammation. Cell. Mol. Life Sci. 2016, 73, 4449–4470. [Google Scholar] [CrossRef]
- Caffarel, M.M.; Sarrio, D.; Palacios, J.; Guzman, M.; Sanchez, C. Delta9-tetrahydrocannabinol inhibits cell cycle progression in human breast cancer cells through Cdc2 regulation. Cancer Res. 2006, 66, 6615–6621. [Google Scholar] [CrossRef]
- Fraguas-Sanchez, A.I.; Martin-Sabroso, C.; Torres-Suarez, A.I. Insights into the effects of the endocannabinoid system in cancer: A review. Br. J. Pharmacol. 2018, 175, 2566–2580. [Google Scholar] [CrossRef]
- Perez-Gomez, E.; Andradas, C.; Blasco-Benito, S.; Caffarel, M.M.; Garcia-Taboada, E.; Villa-Morales, M.; Moreno, E.; Hamann, S.; Martin-Villar, E.; Flores, J.M.; et al. Role of cannabinoid receptor CB2 in HER2 pro-oncogenic signaling in breast cancer. J. Natl. Cancer Inst. 2015, 107, djv077. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Median (Range) |
|---|---|
| Age (years) | 69 (47–85) |
| PSA (ng/mL) | 1.25 (0.24–16.3) |
| Testosterone, total (ng/dL) | 325 (7–1166) |
| Time from diagnosis to study entry (months) | 93 (5–204) |
| Age Group | Number (%) |
| 40–49 | 1 (4.7%) |
| 50–59 | 1 (4.7%) |
| 60–69 | 9 (42.8%) |
| 70–79 | 7 (33%) |
| 80–89 | 3 (14.2%) |
| Total | 21 (100%) |
| Race | Number (%) |
| White | 17 (85.7%) |
| African American | 2 (9.5%) |
| Asian | 1 (4.7%) |
| Unknown | 1(4.7%) |
| Total | 21 (100%) |
| Prior Treatment | Number (%) |
| Prostatectomy Alone | 4 (19.1%) |
| Radiation Alone | 5 (23.8%) |
| Prostatectomy and salvage radiation | 12 (57.1%) |
| Untreated | 0 (0%) |
| Total | 21 (100%) |
| Gleason grade at diagnosis | Number (%) |
| 3 + 3 = 6 | 1 (4.7%) |
| 3 + 4 = 7 | 6 (28.5%) |
| 4 + 3 = 7 | 8 (38%) |
| ≥8 | 5 (23.8%) |
| Unknown | 1 (4.7%) |
| Total | 21 (100%) |
| Staging groups for prostatectomy patients | Number (%) |
| T1N0 | 2 (13.3%) |
| T2N0 | 6 (40%) |
| T3aN0 | 5 (33.3%) |
| T3bN1 | 1 (6.6%) |
| Unknown | 1 (6.6%) |
| Total | 15 (100%) |
| PSA doubling time | Number (%) |
| Less than 6 months | 3 (14.3%) |
| 6 to 12 months | 6 (28.6%) |
| >12 months | 11 (52.4%) |
| Body System | Symptom | All AEs N (%) | CTCAE Toxicity Grade | Acute Onset (within 30 Days) N (%) | CTCAE Toxicity Grade | Chronic Onset (within 90 Days) | CTCAE Toxicity Grade | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |||||
| Gastrointestinal | Diarrhea | 11 (55%) | 10 | 1 | 0 | 0 | 0 | 8 (40%) | 7 | 1 | 0 | 0 | 0 | 10 (50%) | 9 | 1 | 0 | 0 | 0 |
| Nausea | 5 (25%) | 5 | 0 | 0 | 0 | 0 | 3 (15%) | 3 | 0 | 0 | 0 | 0 | 4 (20%) | 4 | 0 | 0 | 0 | 0 | |
| Bloating | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | ||||||
| Stomach pain | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | ||||||
| Abnormal LFTs | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 0 | ||||||
| General | Fatigue | 4 (20%) | 3 | 1 | 0 | 0 | 0 | 2 (10%) | 2 | 0 | 0 | 0 | 0 | 4 (20%) | 3 | 1 | 0 | 0 | 0 |
| Malaise | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | |
| Nervous system | Headache | 2 (10%) | 2 | 0 | 0 | 0 | 0 | 2 (10%) | 2 | 0 | 0 | 0 | 0 | 2 (10%) | 2 | 0 | 0 | 0 | 0 |
| Insomnia | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 0 | ||||||
| Skin | Rash | 1 (5%) | 1 | 0 | 0 | 0 | 0 | 0 | 1 (5%) | 1 | 0 | 0 | 0 | 0 | |||||
| Baseline | 12-Week Post-Baseline | Mean Change | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean | Std | N | Mean | Std | Lower Bound | Upper Bound | p-Value | ||
| Global health status/QoL | 17 | 78.4 | 15.0 | 12 | 81.3 | 13.4 | 2.9 | −8.0 | 13.8 | 0.60 |
| Physical functioning | 17 | 92.9 | 11.9 | 12 | 90.0 | 14.4 | −2.9 | −13.3 | 7.5 | 0.56 |
| Role functioning | 17 | 97.1 | 8.8 | 12 | 93.1 | 13.2 | −4 | −13.0 | 5.0 | 0.34 |
| Emotional functioning | 17 | 94.1 | 9.2 | 12 | 96.5 | 5.6 | 2.4 | −3.3 | 8.1 | 0.43 |
| Cognitive functioning | 17 | 93.1 | 10.3 | 12 | 91.7 | 11.2 | −1.4 | −9.8 | 7.0 | 0.73 |
| Social functioning | 17 | 97.1 | 8.8 | 12 | 95.8 | 10.4 | −1.3 | −8.9 | 6.3 | 0.72 |
| Symptom Scales | ||||||||||
| Fatigue | 17 | 12.4 | 13.0 | 12 | 16.7 | 18.7 | 4.3 | −8.5 | 17.1 | 0.47 |
| Nausea/Vomiting | 17 | 1.0 | 4.0 | 12 | 1.4 | 4.8 | 0.4 | −3.1 | 3.9 | 0.81 |
| Pain | 17 | 15.7 | 21.6 | 12 | 13.9 | 17.2 | −1.8 | −16.6 | 13.0 | 0.81 |
| Dyspnea | 17 | 7.8 | 14.6 | 12 | 13.9 | 22.3 | 6.1 | −9.0 | 21.2 | 0.38 |
| Insomnia | 17 | 13.7 | 16.9 | 12 | 8.3 | 20.7 | −5.4 | −20.3 | 9.5 | 0.45 |
| Appetite loss | 17 | 0.0 | 0.0 | 12 | 0.0 | 0.0 | N/A | N/A | N/A | N/A |
| Constipation | 17 | 3.9 | 11.1 | 12 | 13.9 | 17.2 | 10 | −1.6 | 21.6 | 0.07 |
| Diarrhea | 17 | 7.8 | 14.6 | 12 | 8.3 | 15.1 | 0.5 | −11.0 | 12.0 | 0.93 |
| Financial problems | 17 | 7.8 | 14.6 | 12 | 11.1 | 16.4 | 3.3 | −8.8 | 15.4 | 0.57 |
| Prostate−Specific | ||||||||||
| Urinary symptoms | 17 | 17.9 | 12.7 | 12 | 17.5 | 11.2 | −0.4 | −9.6 | 8.8 | 0.93 |
| Incontinence aid | 7 | 9.5 | 16.3 | 3 | 22.2 | 19.2 | 12.7 | −13.3 | 38.7 | 0.29 |
| Bowel symptoms | 17 | 6.4 | 8.1 | 12 | 7.6 | 8.3 | 1.2 | −5.2 | 7.6 | 0.70 |
| Hormonal treatment−related symptoms | 17 | 5.9 | 6.0 | 12 | 9.0 | 10.2 | 3.1 | −3.6 | 9.8 | 0.31 |
| Sexual activity | 17 | 67.6 | 22.3 | 12 | 63.9 | 21.1 | −3.7 | −20.4 | 13.0 | 0.66 |
| Sexual functioning | 8 | 56.9 | 26.8 | 2 | 77.8 | 0.0 | 20.9 | 1.5 | 40.3 | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myint, Z.W.; St. Clair, W.H.; Strup, S.E.; Yan, D.; Li, N.; Allison, D.B.; McLouth, L.E.; Ellis, C.S.; Wang, P.; James, A.C.; et al. A Phase I Dose Escalation and Expansion Study of Epidiolex (Cannabidiol) in Patients with Biochemically Recurrent Prostate Cancer. Cancers 2023, 15, 2505. https://doi.org/10.3390/cancers15092505
Myint ZW, St. Clair WH, Strup SE, Yan D, Li N, Allison DB, McLouth LE, Ellis CS, Wang P, James AC, et al. A Phase I Dose Escalation and Expansion Study of Epidiolex (Cannabidiol) in Patients with Biochemically Recurrent Prostate Cancer. Cancers. 2023; 15(9):2505. https://doi.org/10.3390/cancers15092505
Chicago/Turabian StyleMyint, Zin W., William H. St. Clair, Stephen E. Strup, Donglin Yan, Ning Li, Derek B. Allison, Laurie E. McLouth, Carleton S. Ellis, Peng Wang, Andrew C. James, and et al. 2023. "A Phase I Dose Escalation and Expansion Study of Epidiolex (Cannabidiol) in Patients with Biochemically Recurrent Prostate Cancer" Cancers 15, no. 9: 2505. https://doi.org/10.3390/cancers15092505
APA StyleMyint, Z. W., St. Clair, W. H., Strup, S. E., Yan, D., Li, N., Allison, D. B., McLouth, L. E., Ellis, C. S., Wang, P., James, A. C., Hensley, P. J., Otto, D. E., Arnold, S. M., DiPaola, R. S., & Kolesar, J. M. (2023). A Phase I Dose Escalation and Expansion Study of Epidiolex (Cannabidiol) in Patients with Biochemically Recurrent Prostate Cancer. Cancers, 15(9), 2505. https://doi.org/10.3390/cancers15092505