

Epidemiology of Oral Cancer in Taiwan: A Population-Based Cancer Registry Study
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
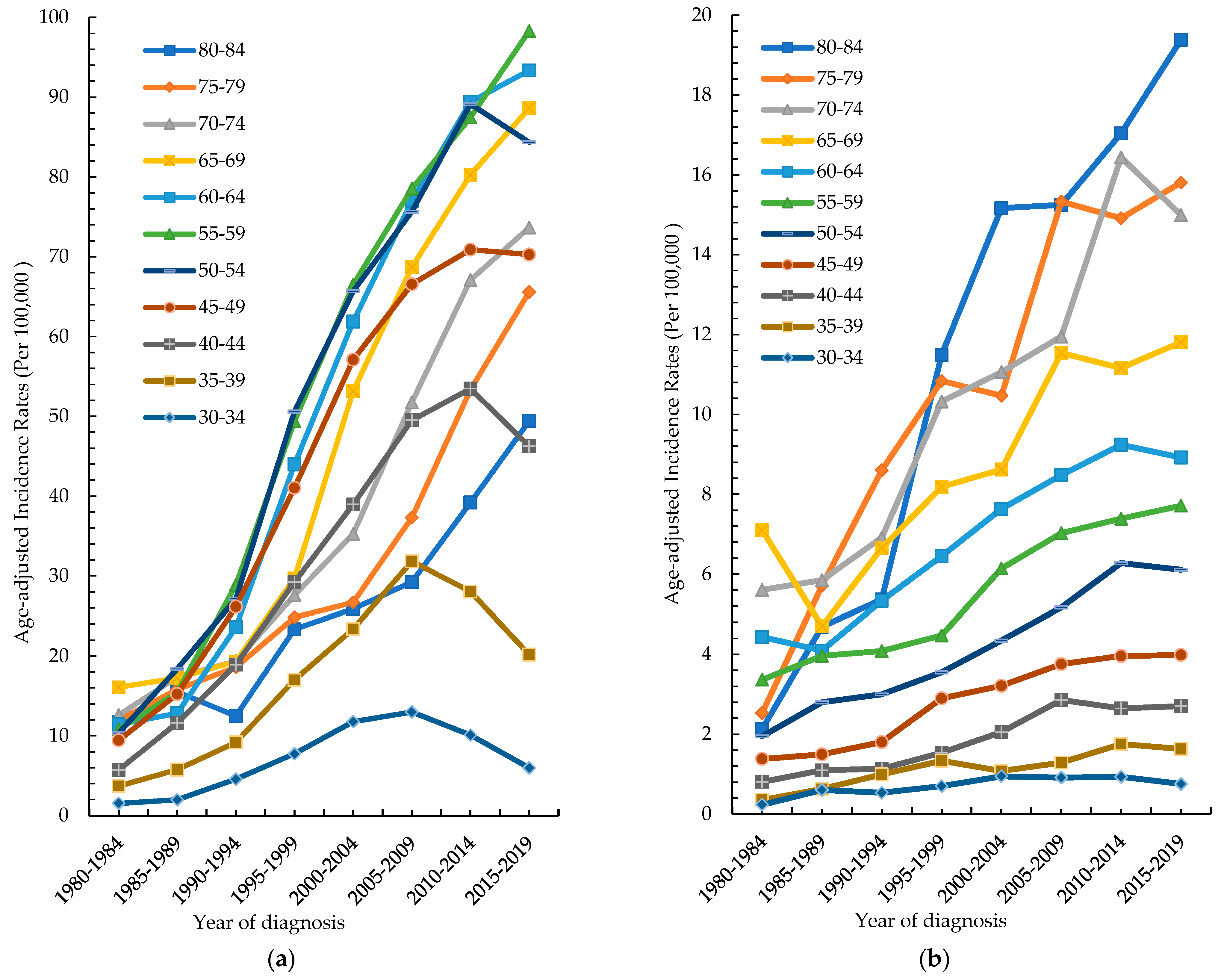
3.1. Trend of Incidence Rate of Oral Cancer
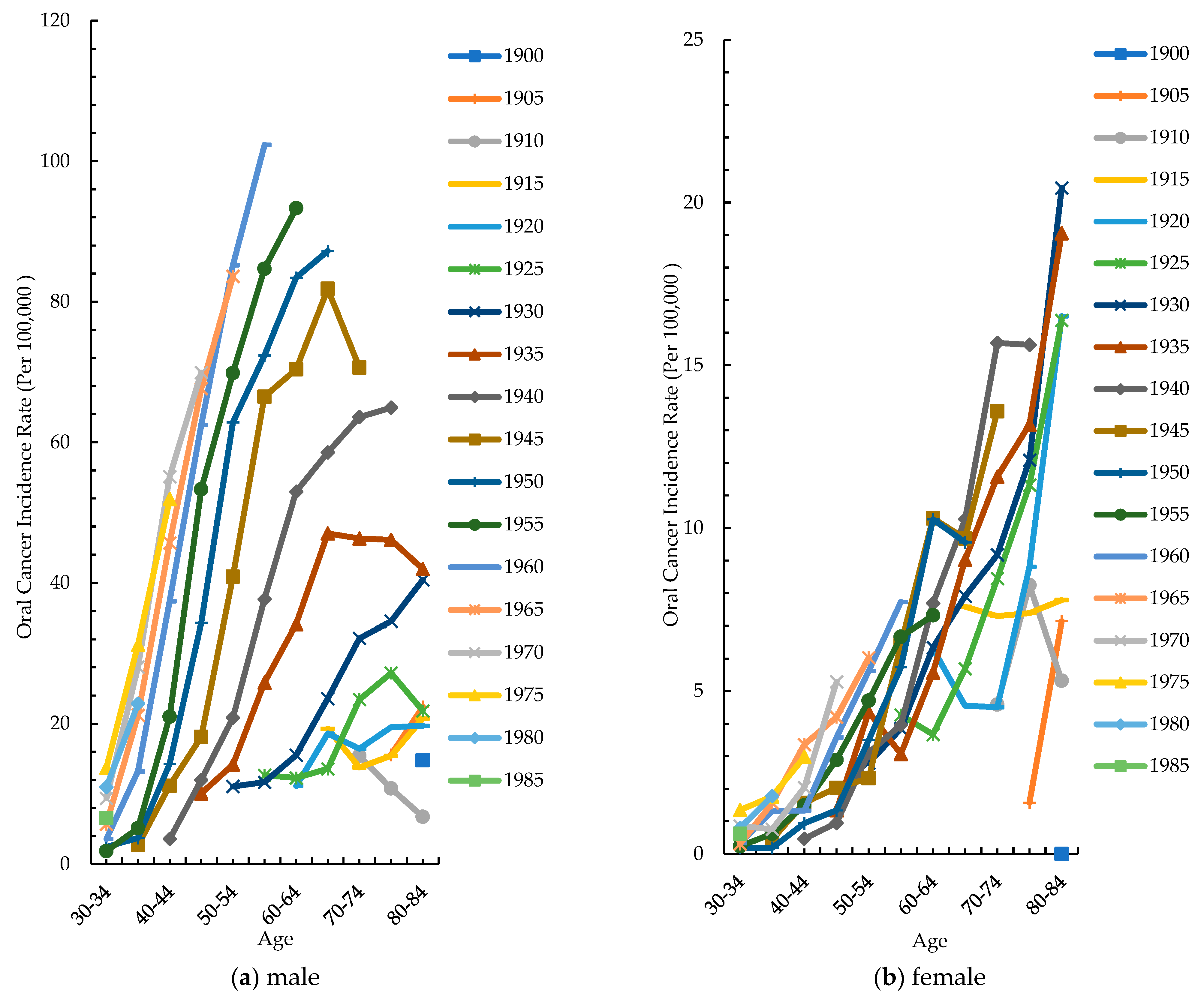
3.2. Age-Specific Incidence Rate by Different Periods
3.3. Cohort-Specific Incidence Rate by Different Age Groups
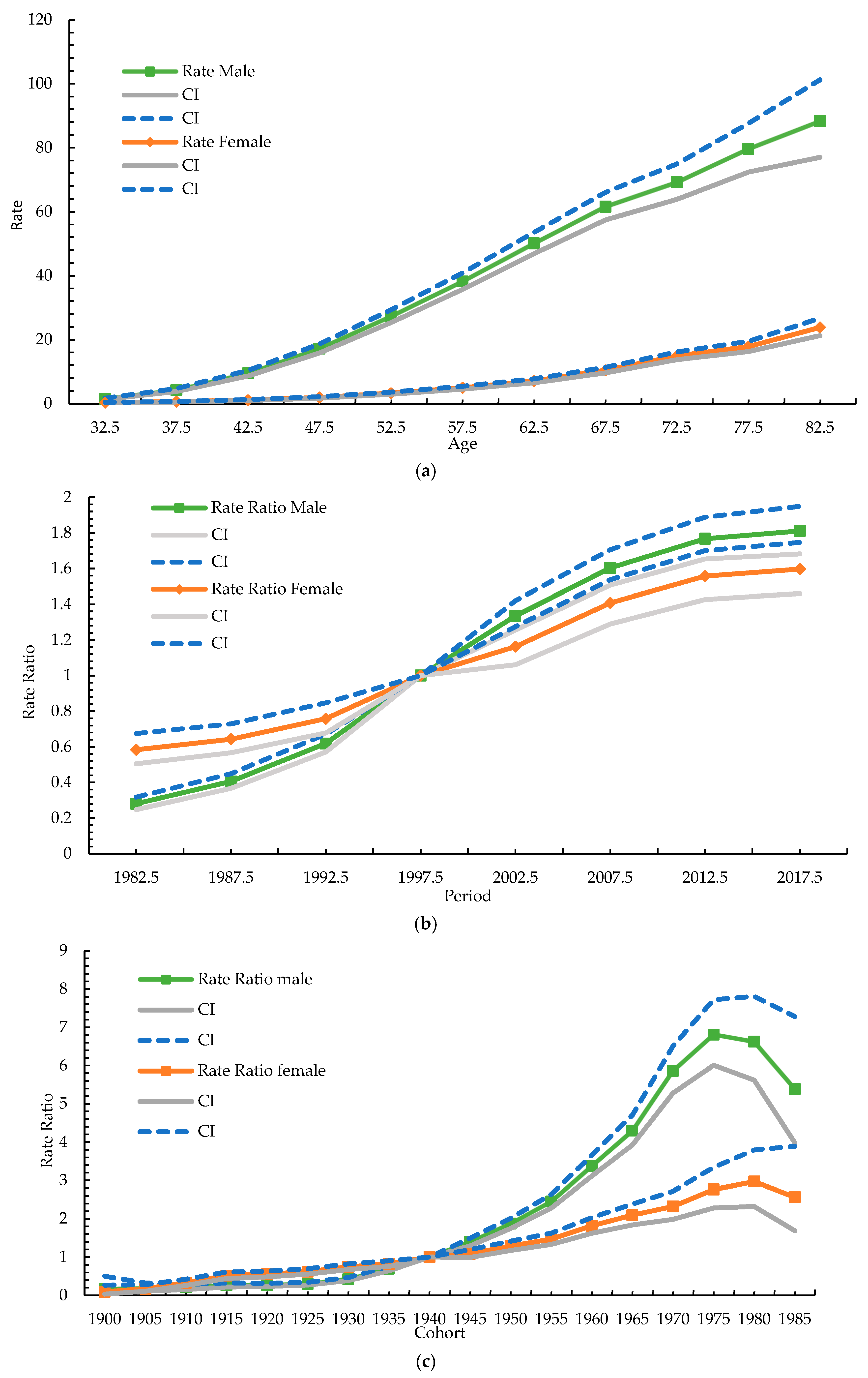
3.4. Age–Period–Cohort Model
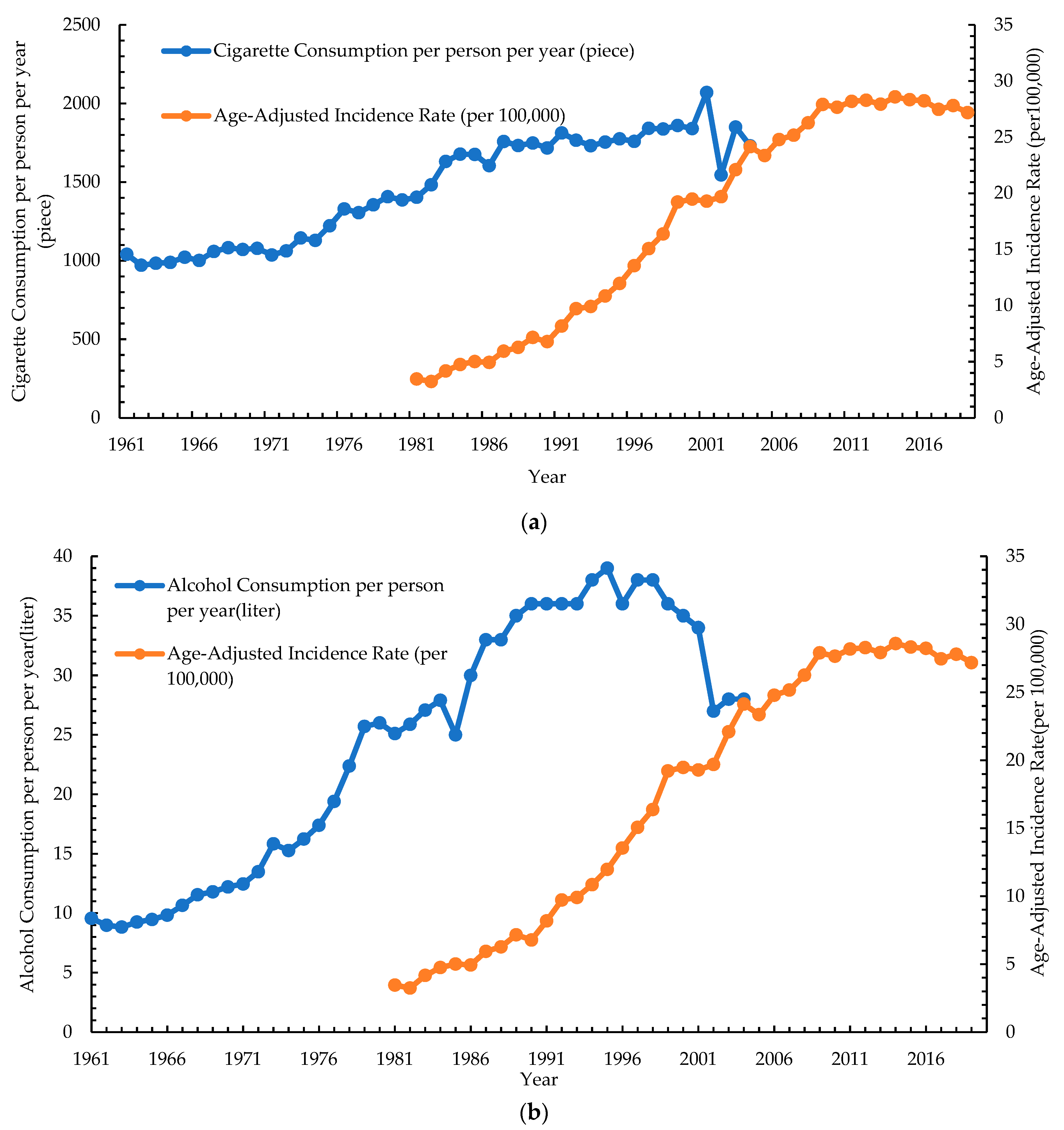
3.5. Correlation of Risk Factors with Age-Standardized Incidence Rate of Oral Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar] [PubMed]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Montero, P.H.; Patel, S.G. Cancer of the oral cavity. Surg. Oncol. Clin. N. Am. 2015, 24, 491–508. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Tsai, M.K.; Chung, W.S.; Hsu, H.L.; Chang, Y.C.; Chan, H.T.; Chiang, P.H.; Cheng, T.Y.; Tsai, S.P. Cancer risks from betel quid chewing beyond oral cancer: A multiple-site carcinogen when acting with smoking. Cancer Causes Control 2010, 21, 1427–1435. [Google Scholar] [CrossRef]
- Ren, Z.H.; Hu, C.Y.; He, H.R.; Li, Y.J.; Lyu, J. Global and regional burdens of oral cancer from 1990 to 2017: Results from the global burden of disease study. Cancer Commun. 2020, 40, 81–92. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Kerr, A.R. Oral Cancer Screening: Past, Present, and Future. J. Dent. Res. 2021, 100, 1313–1320. [Google Scholar] [CrossRef]
- Chuang, S.L.; Su, W.W.; Chen, S.L.; Yen, A.M.; Wang, C.P.; Fann, J.C.; Chiu, S.Y.; Lee, Y.C.; Chiu, H.M.; Chang, D.C.; et al. Population-based screening program for reducing oral cancer mortality in 2,334,299 Taiwanese cigarette smokers and/or betel quid chewers. Cancer 2017, 123, 1597–1609. [Google Scholar] [CrossRef]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef]
- Health Promotion Administration Taiwan Cancer Registry Database. Available online: https://cris.hpa.gov.tw/pagepub/Home.aspx (accessed on 11 November 2022).
- Chiang, C.J.; Wang, Y.W.; Lee, W.C. Taiwan’s Nationwide Cancer Registry System of 40 years: Past, present, and future. J. Formos. Med. Assoc. 2019, 118, 856–858. [Google Scholar] [CrossRef]
- Taiwan Tobacco and Liquor Corporation Taiwan Tobacco and Wine Statistical Yearbook. Available online: https://www.ttl.com.tw/ (accessed on 11 November 2022).
- Finance, M.O. Yearbook of Financial Statistics. Available online: https://www.mof.gov.tw/ (accessed on 11 November 2022).
- Council of Agriculture. Agricultural Statistics Yearbook. Available online: https://www.coa.gov.tw/ (accessed on 11 November 2022).
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age standardization of rates: A new WHO standard. Geneva World Health Organ. 2001, 9, 1–14. [Google Scholar]
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.P.; Shin, H.I.; Choi, S.Y.; et al. Oral cancer: A multicenter study. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e23–e29. [Google Scholar] [CrossRef] [PubMed]
- Neville, B.W.; Day, T.A. Oral cancer and precancerous lesions. CA Cancer J. Clin. 2002, 52, 195–215. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.L.; Khammissa, R.R.; Kramer, B.B.; Lemmer, J.J. Oral squamous cell carcinoma in relation to field precancerisation: Pathobiology. Cancer Cell Int. 2013, 13, 31. [Google Scholar] [CrossRef]
- Kumar, M.; Nanavati, R.; Modi, T.G.; Dobariya, C. Oral cancer: Etiology and risk factors: A review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef]
- Yang, C.H.; Lin, Y.D.; Yen, C.Y.; Chuang, L.Y.; Chang, H.W. A systematic gene-gene and gene-environment interaction analysis of DNA repair genes XRCC1, XRCC2, XRCC3, XRCC4, and oral cancer risk. Omics 2015, 19, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Dissanayaka, W.L.; Pitiyage, G.; Kumarasiri, P.V.; Liyanage, R.L.; Dias, K.D.; Tilakaratne, W.M. Clinical and histopathologic parameters in survival of oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Koontongkaew, S. The tumor microenvironment contribution to development, growth, invasion and metastasis of head and neck squamous cell carcinomas. J. Cancer 2013, 4, 66–83. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2008, 122, 155–164. [Google Scholar] [CrossRef]
- Marron, M.; Boffetta, P.; Zhang, Z.F.; Zaridze, D.; Wünsch-Filho, V.; Winn, D.M.; Wei, Q.; Talamini, R.; Szeszenia-Dabrowska, N.; Sturgis, E.M.; et al. Cessation of alcohol drinking, tobacco smoking and the reversal of head and neck cancer risk. Int. J. Epidemiol. 2010, 39, 182–196. [Google Scholar] [CrossRef]
- Choudhari, S.K.; Chaudhary, M.; Gadbail, A.R.; Sharma, A.; Tekade, S. Oxidative and antioxidative mechanisms in oral cancer and precancer: A review. Oral Oncol. 2014, 50, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Tsai, S.P.; Chen, C.J.; Cheng, T.Y.; Tsai, M.C.; Levy, D.T. Smoking attributable mortality for Taiwan and its projection to 2020 under different smoking scenarios. Tob. Control 2005, 14, i76–i80. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.P.; Levy, D.T.; Cheng, T.Y.; Hsu, C.C.; Tsai, S.P. Smoking behaviour in Taiwan, 2001. Tob. Control 2005, 14, i51–i55. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.; Sansgiry, S.; Peters, R.; Yang, M.; Abughosh, S. Cigarette smoking among Taiwanese adults. Epidemiology 2011, 1, 107. [Google Scholar]
- Tramacere, I.; Negri, E.; Bagnardi, V.; Garavello, W.; Rota, M.; Scotti, L.; Islami, F.; Corrao, G.; Boffetta, P.; La Vecchia, C. A meta-analysis of alcohol drinking and oral and pharyngeal cancers. Part 1: Overall results and dose-risk relation. Oral Oncol. 2010, 46, 497–503. [Google Scholar] [CrossRef]
- Reidy, J.; McHugh, E.; Stassen, L.F. A review of the relationship between alcohol and oral cancer. Surgeon 2011, 9, 278–283. [Google Scholar] [CrossRef]
- Seitz, H.K.; Stickel, F. Molecular mechanisms of alcohol-mediated carcinogenesis. Nat. Rev. Cancer 2007, 7, 599–612. [Google Scholar] [CrossRef]
- Wang, L.J.; Lin, C.L.; Chen, Y.C.; Lin, C.; Shyu, Y.C.; Chen, C.K. Sex Differences in the Relationship between Excessive Alcohol Consumption and Metabolic Abnormalities: A Community-Based Study in Taiwan. Nutrients 2022, 14, 2957. [Google Scholar] [CrossRef]
- Huang, Y.C.; Wu, S.C.; Hsiao, P.C.; Chen, L.Y.; Ting, T.T.; Chen, C.Y.; Kuan, C.C.; Tu, Y.K.; Huang, J.H.; Yen, C.F.; et al. Men’s decrease and women’s increase in harmful alcohol use from the 2014 to 2018 national surveys in Taiwan: A harbinger for an emerging national trend in East Asia? Int. J. Drug Policy 2022, 99, 103441. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Trivedy, C.; Peters, T.J. Areca nut use: An independent risk factor for oral cancer. BMJ 2002, 324, 799–800. [Google Scholar] [CrossRef]
- Guha, N.; Warnakulasuriya, S.; Vlaanderen, J.; Straif, K. Betel quid chewing and the risk of oral and oropharyngeal cancers: A meta-analysis with implications for cancer control. Int. J. Cancer 2014, 135, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Ho, Y.S.; Lee, P.H.; Chan, C.P.; Lee, J.J.; Hahn, L.J.; Wang, Y.J.; Jeng, J.H. Areca nut extract and arecoline induced the cell cycle arrest but not apoptosis of cultured oral KB epithelial cells: Association of glutathione, reactive oxygen species and mitochondrial membrane potential. Carcinogenesis 2001, 22, 1527–1535. [Google Scholar] [CrossRef]
- Tsai, Y.S.; Lee, K.W.; Huang, J.L.; Liu, Y.S.; Juo, S.H.; Kuo, W.R.; Chang, J.G.; Lin, C.S.; Jong, Y.J. Arecoline, a major alkaloid of areca nut, inhibits p53, represses DNA repair, and triggers DNA damage response in human epithelial cells. Toxicology 2008, 249, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.J.; Chang, M.L.; Chiang, C.P.; Hahn, L.J.; Hsieh, L.L.; Chen, C.J. Interaction of collagen-related genes and susceptibility to betel quid-induced oral submucous fibrosis. Cancer Epidemiol. Biomark. Prev. 2002, 11, 646–653. [Google Scholar]
- Chiba, I. Prevention of Betel Quid Chewers’ Oral Cancer in the Asian-Pacific Area. Asian Pac. J. Cancer Prev. 2001, 2, 263–269. [Google Scholar] [PubMed]
- Betel-quid and areca-nut chewing. IARC Monogr. Eval. Carcinog. Risk Chem. Hum. 1985, 37, 137–202.
- Gupta, B.; Johnson, N.W. Systematic review and meta-analysis of association of smokeless tobacco and of betel quid without tobacco with incidence of oral cancer in South Asia and the Pacific. PLoS ONE 2014, 9, e113385. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.S.; Jen, Y.M.; Wang, B.B.; Lee, J.C.; Kang, B.H. Epidemiology of oral cavity cancer in taiwan with emphasis on the role of betel nut chewing. ORL J. Oto-Rhino-Laryngol. Relat. Spec. 2005, 67, 230–236. [Google Scholar] [CrossRef]
- Hsu, W.-L.; Yu, K.; Chiang, C.-J.; Chen, T.-C.; Wang, C.-P. Head and Neck Cancer Incidence Trends in Taiwan, 1980~2014. Int. J. Head Neck Sci. 2017, 1, 180–189. [Google Scholar]
- Lee, Y.A.; Li, S.; Chen, Y.; Li, Q.; Chen, C.J.; Hsu, W.L.; Lou, P.J.; Zhu, C.; Pan, J.; Shen, H.; et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck 2019, 41, 92–102. [Google Scholar] [CrossRef]
- Su, S.Y. Evaluation of Nationwide Oral Mucosal Screening Program for Oral Cancer Mortality among Men in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 14329. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare Tobacco Hazards Prevention Act. Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=L0070021 (accessed on 22 March 2022).
- Ministry of Finance Tobacco and Alcohol Tax Act. Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=G0330010 (accessed on 22 March 2022).
- Tham, J.; Sem, G.; Sit, E.; Tai, M.C. The ethics of betel nut consumption in Taiwan. J. Med. Ethics 2017, 43, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.Y.; Ho, L.M.; Lee, J.M.; Hwang, J.Y. The possible impact of an alcohol welfare surcharge on consumption of alcoholic beverages in Taiwan. BMC Public Health 2013, 13, 810. [Google Scholar] [CrossRef]
- Huang, C.C.; Ou, C.Y.; Lee, W.T.; Hsiao, J.R.; Tsai, S.T.; Wang, J.D. Life expectancy and expected years of life lost to oral cancer in Taiwan: A nation-wide analysis of 22,024 cases followed for 10 years. Oral Oncol. 2015, 51, 349–354. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, C.-W.; Lin, C.-R.; Chung, Y.-T.; Tang, C.-S. Epidemiology of Oral Cancer in Taiwan: A Population-Based Cancer Registry Study. Cancers 2023, 15, 2175. https://doi.org/10.3390/cancers15072175
Chou C-W, Lin C-R, Chung Y-T, Tang C-S. Epidemiology of Oral Cancer in Taiwan: A Population-Based Cancer Registry Study. Cancers. 2023; 15(7):2175. https://doi.org/10.3390/cancers15072175
Chicago/Turabian StyleChou, Chao-Wei, Chun-Ru Lin, Yi-Ting Chung, and Chin-Sheng Tang. 2023. "Epidemiology of Oral Cancer in Taiwan: A Population-Based Cancer Registry Study" Cancers 15, no. 7: 2175. https://doi.org/10.3390/cancers15072175
APA StyleChou, C.-W., Lin, C.-R., Chung, Y.-T., & Tang, C.-S. (2023). Epidemiology of Oral Cancer in Taiwan: A Population-Based Cancer Registry Study. Cancers, 15(7), 2175. https://doi.org/10.3390/cancers15072175