
Pretreatment Plasma Circulating Tumor DNA RAS/BRAF Mutational Status in Refractory Metastatic Colorectal Cancer Patients Who Are Candidates for Anti-EGFR Rechallenge Therapy: A Pooled Analysis of the CAVE and VELO Clinical Trials


 , , , , ,
, , , , , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
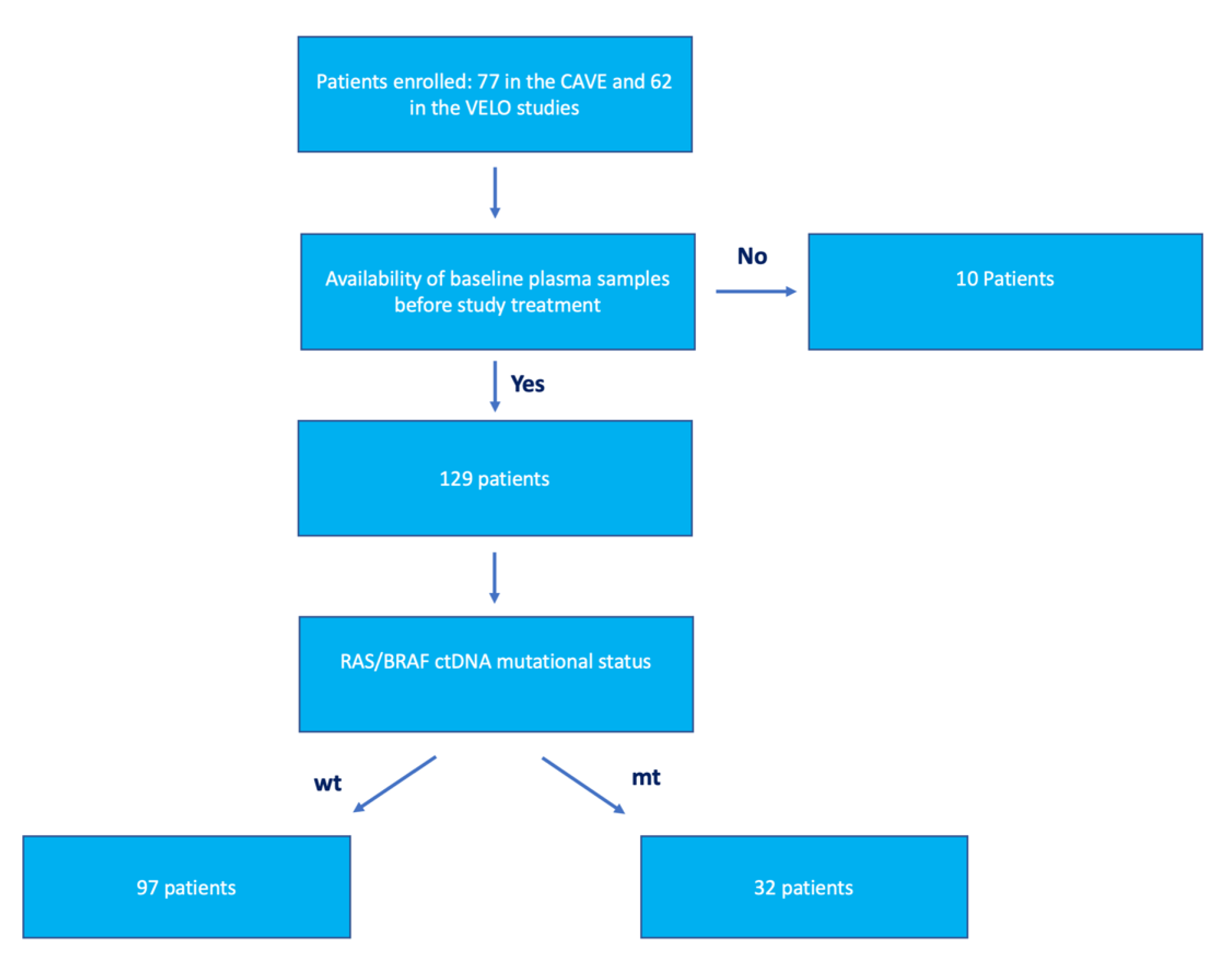
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ciardiello, F.; Ciardiello, D.; Martini, G.; Napolitano, S.; Tabernero, J.; Cervantes, A. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA A Cancer J. Clin. 2022, 72, 372–401. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, E.; Ciardiello, D.; Martini, G.; Troiani, T.; Cardone, C.; Vitiello, P.; Normanno, N.; Rachiglio, A.; Maiello, E.; Latiano, T.; et al. Implementing anti-epidermal growth factor receptor (EGFR) therapy in metastatic colorectal cancer: Challenges and future perspectives. Ann. Oncol. 2020, 31, 30–40. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Lenz, H.-J.; Köhne, C.-H.; Heinemann, V.; Tejpar, S.; Melezínek, I.; Beier, F.; Stroh, C.; Rougier, P.; van Krieken, J.H.; et al. Fluorouracil, Leucovorin, and Irinotecan Plus Cetuximab Treatment and RAS Mutations in Colorectal Cancer. J. Clin. Oncol. 2015, 33, 692–700. [Google Scholar] [CrossRef]
- Douillard, J.-Y.; Oliner, K.S.; Siena, S.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N. Engl. J. Med. 2013, 369, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Granieri, S.; Cotsoglou, C.; Bonomi, A.; Salvatore, L.; Filippi, R.; Nigro, O.; Gelsomino, F.; Zurlo, I.V.; Depetris, I.; Giampieri, R.; et al. Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study. Cancers 2022, 14, 5513. [Google Scholar] [CrossRef] [PubMed]
- Martini, G.; Ciardiello, D.; Vitiello, P.P.; Napolitano, S.; Cardone, C.; Cuomo, A.; Troiani, T.; Ciardiello, F.; Martinelli, E. Resistance to anti-epidermal growth factor receptor in metastatic colorectal cancer: What does still need to be addressed? Cancer Treat. Rev. 2020, 86, 102023. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Tabernero, J.; Lakomy, R.; Prenen, H.; Prausová, J.; Macarulla, T.; Ruff, P.; van Hazel, G.A.; Moiseyenko, V.; Ferry, D.; et al. Addition of Aflibercept to Fluorouracil, Leucovorin, and Irinotecan Improves Survival in a Phase III Randomized Trial in Patients With Metastatic Colorectal Cancer Previously Treated With an Oxaliplatin-Based Regimen. J. Clin. Oncol. 2012, 30, 3499–3506. [Google Scholar] [CrossRef]
- Bennouna, J.; Sastre, J.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 29–37. [Google Scholar] [CrossRef]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized Trial of TAS-102 for Refractory Metastatic Colorectal Cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef]
- Ciardiello, D.; Martini, G.; Famiglietti, V.; Napolitano, S.; De Falco, V.; Troiani, T.; Latiano, T.P.; Ros, J.; Fernandez, E.E.; Vitiello, P.P.; et al. Biomarker-Guided Anti-EGFR Rechallenge Therapy in Metastatic Colorectal Cancer. Cancers 2021, 13, 1941. [Google Scholar] [CrossRef] [PubMed]
- Parseghian, C.; Loree, J.; Morris, V.; Liu, X.; Clifton, K.; Napolitano, S.; Henry, J.; Pereira, A.; Vilar, E.; Johnson, B.; et al. Anti-EGFR-resistant clones decay exponentially after progression: Implications for anti-EGFR re-challenge. Ann. Oncol. 2019, 30, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Sartore-Bianchi, A.; Pietrantonio, F.; Lonardi, S.; Mussolin, B.; Rua, F.; Crisafulli, G.; Bartolini, A.; Fenocchio, E.; Amatu, A.; Manca, P.; et al. Circulating tumor DNA to guide rechallenge with panitumumab in metastatic colorectal cancer: The phase 2 CHRONOS trial. Nat. Med. 2022, 28, 1612–1618. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Rossini, D.; Dell’Aquila, E.; Lonardi, S.; Conca, E.; Del Re, M.; Busico, A.; Pietrantonio, F.; Danesi, R.; Aprile, G.; et al. Rechallenge for Patients With RAS and BRAF Wild-Type Metastatic Colorectal Cancer With Acquired Resistance to First-line Cetuximab and Irinotecan. JAMA Oncol. 2019, 5, 343–350. [Google Scholar] [CrossRef]
- Martinelli, E.; Martini, G.; Famiglietti, V.; Troiani, T.; Napolitano, S.; Pietrantonio, F.; Ciardiello, D.; Terminiello, M.; Borrelli, C.; Vitiello, P.P.; et al. Cetuximab Rechallenge Plus Avelumab in Pretreated Patients With RAS Wild-type Metastatic Colorectal Cancer. JAMA Oncol. 2021, 7, 1529. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, D.; Famiglietti, V.; Napolitano, S.; Esposito, L.; Pietrantonio, F.; Avallone, A.; Maiello, E.; Cremolini, C.; Troiani, T.; Martinelli, E.; et al. Final results of the CAVE trial in RAS wild type metastatic colorectal cancer patients treated with cetuximab plus avelumab as rechallenge therapy: Neutrophil to lymphocyte ratio predicts survival. Clin. Color. Cancer 2022, 21, 141–148. [Google Scholar] [CrossRef]
- Sunakawa, Y.; Nakamura, M.; Ishizaki, M.; Kataoka, M.; Satake, H.; Kitazono, M.; Yanagisawa, H.; Kawamoto, Y.; Kuramochi, H.; Ohori, H.; et al. RAS Mutations in Circulating Tumor DNA and Clinical Outcomes of Rechallenge Treatment With Anti-EGFR Antibodies in Patients With Metastatic Colorectal Cancer. JCO Precis. Oncol. 2020, 4, 898–911. [Google Scholar] [CrossRef]
- Napolitano, S.; De Falco, V.; Martini, G.; Esposito, L.; Famiglietti, V.; Martinelli, E.; Ciardiello, D.; Marrone, F.; Avallone, A.; Cardone, C.; et al. Panitumumab plus trifluridine/tipiracil as anti-Epidermal Growth Factor Receptor rechallenge therapy in chemo-refractory RAS wild-type metastatic colorectal cancer: The randomized phase 2 VELO trial. J. Clin. Oncol. 2023, 41, 129. [Google Scholar] [CrossRef]
- Vitiello, P.P.; De Falco, V.; Giunta, E.F.; Ciardiello, D.; Cardone, C.; Vitale, P.; Zanaletti, N.; Borrelli, C.; Poliero, L.; Terminiello, M.; et al. Clinical Practice Use of Liquid Biopsy to Identify RAS/BRAF Mutations in Patients with Metastatic Colorectal Cancer (mCRC): A Single Institution Experience. Cancers 2019, 11, 1504. [Google Scholar] [CrossRef]
- Misale, S.; Di Nicolantonio, F.; Sartore-Bianchi, A.; Siena, S.; Bardelli, A. Resistance to Anti-EGFR Therapy in Colorectal Cancer: From Heterogeneity to Convergent Evolution. Cancer Discov. 2014, 4, 1269–1280. [Google Scholar] [CrossRef]
- Parseghian, C.M.; Napolitano, S.; Loree, J.M.; Kopetz, S. Mechanisms of Innate and Acquired Resistance to Anti-EGFR Therapy: A Review of Current Knowledge with a Focus on Rechallenge Therapies. Clin. Cancer Res. 2019, 25, 6899–6908. [Google Scholar] [CrossRef]
- Yaeger, R.; Kotani, D.; Mondaca, S.; Parikh, A.R.; Bando, H.; Van Seventer, E.E.; Taniguchi, H.; Zhao, H.; Thant, C.N.; de Stanchina, E.; et al. Response to Anti-EGFR Therapy in Patients with BRAF non-V600–Mutant Metastatic Colorectal Cancer. Clin. Cancer Res. 2019, 25, 7089–7097. [Google Scholar] [CrossRef]
- Bertotti, A.; Migliardi, G.; Galimi, F.; Sassi, F.; Torti, D.; Isella, C.; Corà, D.; Di Nicolantonio, F.; Buscarino, M.; Petti, C.; et al. A Molecularly Annotated Platform of Patient-Derived Xenografts (“Xenopatients”) Identifies HER2 as an Effective Therapeutic Target in Cetuximab-Resistant Colorectal Cancer. Cancer Discov. 2011, 1, 508–523. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, A.; Corso, S.; Bertotti, A.; Hobor, S.; Valtorta, E.; Siravegna, G.; Sartore-Bianchi, A.; Scala, E.; Cassingena, A.; Zecchin, D.; et al. Amplification of the MET Receptor Drives Resistance to Anti-EGFR Therapies in Colorectal Cancer. Cancer Discov. 2013, 3, 658–673. [Google Scholar] [CrossRef] [PubMed]
- Cardone, C.; Blauensteiner, B.; Moreno-Viedma, V.; Martini, G.; Simeon, V.; Vitiello, P.P.; Ciardiello, D.; Belli, V.; Matrone, N.; Troiani, T.; et al. AXL is a predictor of poor survival and of resistance to anti-EGFR therapy in RAS wild-type metastatic colorectal cancer. Eur. J. Cancer 2020, 138, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Siravegna, G.; Mussolin, B.; Buscarino, M.; Corti, G.; Cassingena, A.; Crisafulli, G.; Ponzetti, A.; Cremolini, C.; Amatu, A.; Lauricella, C.; et al. Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat. Med. 2015, 21, 795–801. [Google Scholar] [CrossRef]
- Parseghian, C.M.; Sun, R.; Woods, M.; Napolitano, S.; Lee, H.M.; Alshenaifi, J.; Willis, J.; Nunez, S.; Raghav, K.P.; Morris, V.K.; et al. Resistance Mechanisms to Anti–Epidermal Growth Factor Receptor Therapy in RAS/RAF Wild-Type Colorectal Cancer Vary by Regimen and Line of Therapy. J. Clin. Oncol. 2023, 41, 460–471. [Google Scholar] [CrossRef]
- Vivancos, A.; Aranda, E.; Benavides, M.; Élez, E.; Gómez-España, M.A.; Toledano, M.; Alvarez, M.; Parrado, M.R.C.; García-Barberán, V.; Diaz-Rubio, E. Comparison of the Clinical Sensitivity of the Idylla Platform and the OncoBEAM RAS CRC Assay for KRAS Mutation Detection in Liquid Biopsy Samples. Sci. Rep. 2019, 9, 8976. [Google Scholar] [CrossRef]
- Vidal, J.; Bellosillo, B.; Vivas, C.S.; García-Alfonso, P.; Carrato, A.; Cano, M.; García-Carbonero, R.; Élez, E.; Losa, F.; Massutí, B.; et al. Ultra-selection of metastatic colorectal cancer patients using next-generation sequencing to improve clinical efficacy of anti-EGFR therapy. Ann. Oncol. 2019, 30, 439–446. [Google Scholar] [CrossRef]
- Germani, M.; Rossini, D.; Vetere, G.; Giordano, M.; Capone, I.; Manca, P.; Bergamo, F.; Conca, V.; Borelli, B.; Boccaccino, A.; et al. 367P Prospective evaluation of emergent RAS and BRAF mutations in pre-treated metastatic colorectal cancer patients candidate to anti-EGFR re-treatment: Preliminary findings from the PARERE study. Ann. Oncol. 2022, 33, S704. [Google Scholar] [CrossRef]
- Napolitano, S.; Martini, G.; Ciardiello, D.; Di Maio, M.; Normanno, N.; Avallone, A.; Martinelli, E.; Maiello, E.; Troiani, T.; Ciardiello, F. CAVE-2 (Cetuximab-AVElumab) mCRC: A Phase II Randomized Clinical Study of the Combination of Avelumab Plus Cetuximab as a Rechallenge Strategy in Pre-Treated RAS/BRAF Wild-Type mCRC Patients. Front. Oncol. 2022, 12, 940523. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 129 |
|---|---|
| Age | |
| Years (median) | 63 (30–88) |
| Sex | |
| F | 56 (43.4%) |
| M | 73 (56.6%) |
| Performance status | |
| 0 | 86 (66.7%) |
| 1 | 43 (33.3%) |
| Tumor location | |
| Left colon and rectum | 118 (91.5%) |
| Right colon | 11 (8.5%) |
| Primary tumor resection | |
| Yes | 92 (71.3%) |
| No | 37 (28.7%) |
| Number of metastatic sites | |
| <3 | 82 (63.6%) |
| ≥3 | 47 (36.4%) |
| Liver metastasis | |
| Yes | 67 (51.9%) |
| No | 62 (48.1%) |
| Number of previous lines of treatment | |
| 2 | 113 (87.6%) |
| 3 | 8 (6.2%) |
| 4 | 4 (3.1%) |
| 5 | 2 (1.6%) |
| 6 | 2 (1.6%) |
| Baseline ctDNA | |
| RAS/BRAF wt | 97(75.2%) |
| RAS/BRAF mt | 32 (24.8%) |
| Type of RAS/BRAF Mutation | Number of Patients (32) |
|---|---|
| BRAF V600E | 1 |
| KRAS A146P | 2 |
| KRAS A146PT | 1 |
| KRAS A146PV | 1 |
| KRAS G12A | 3 |
| KRAS G12C | 2 |
| KRAS G12D | 5 |
| KRAS G12S | 2 |
| KRAS G12V | 2 |
| KRAS G13D | 3 |
| KRAS Q61H | 6 |
| KRAS Q61H and BRAF V600E | 1 |
| KRAS Q61R | 1 |
| NRAS G13D | 1 |
| KRAS Q61L | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciardiello, D.; Napolitano, S.; Famiglietti, V.; Esposito, L.; De Falco, V.; Di Liello, A.; Avallone, A.; Maiello, E.; Pietrantonio, F.; Cremolini, C.; et al. Pretreatment Plasma Circulating Tumor DNA RAS/BRAF Mutational Status in Refractory Metastatic Colorectal Cancer Patients Who Are Candidates for Anti-EGFR Rechallenge Therapy: A Pooled Analysis of the CAVE and VELO Clinical Trials. Cancers 2023, 15, 2117. https://doi.org/10.3390/cancers15072117
Ciardiello D, Napolitano S, Famiglietti V, Esposito L, De Falco V, Di Liello A, Avallone A, Maiello E, Pietrantonio F, Cremolini C, et al. Pretreatment Plasma Circulating Tumor DNA RAS/BRAF Mutational Status in Refractory Metastatic Colorectal Cancer Patients Who Are Candidates for Anti-EGFR Rechallenge Therapy: A Pooled Analysis of the CAVE and VELO Clinical Trials. Cancers. 2023; 15(7):2117. https://doi.org/10.3390/cancers15072117
Chicago/Turabian StyleCiardiello, Davide, Stefania Napolitano, Vincenzo Famiglietti, Lucia Esposito, Vincenzo De Falco, Alessandra Di Liello, Antonio Avallone, Evaristo Maiello, Filippo Pietrantonio, Chiara Cremolini, and et al. 2023. "Pretreatment Plasma Circulating Tumor DNA RAS/BRAF Mutational Status in Refractory Metastatic Colorectal Cancer Patients Who Are Candidates for Anti-EGFR Rechallenge Therapy: A Pooled Analysis of the CAVE and VELO Clinical Trials" Cancers 15, no. 7: 2117. https://doi.org/10.3390/cancers15072117
APA StyleCiardiello, D., Napolitano, S., Famiglietti, V., Esposito, L., De Falco, V., Di Liello, A., Avallone, A., Maiello, E., Pietrantonio, F., Cremolini, C., Zampino, M. G., Fazio, N., Troiani, T., Martinelli, E., Ciardiello, F., & Martini, G. (2023). Pretreatment Plasma Circulating Tumor DNA RAS/BRAF Mutational Status in Refractory Metastatic Colorectal Cancer Patients Who Are Candidates for Anti-EGFR Rechallenge Therapy: A Pooled Analysis of the CAVE and VELO Clinical Trials. Cancers, 15(7), 2117. https://doi.org/10.3390/cancers15072117