
Association between Iron Deficiency and Survival in Older Patients with Cancer

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
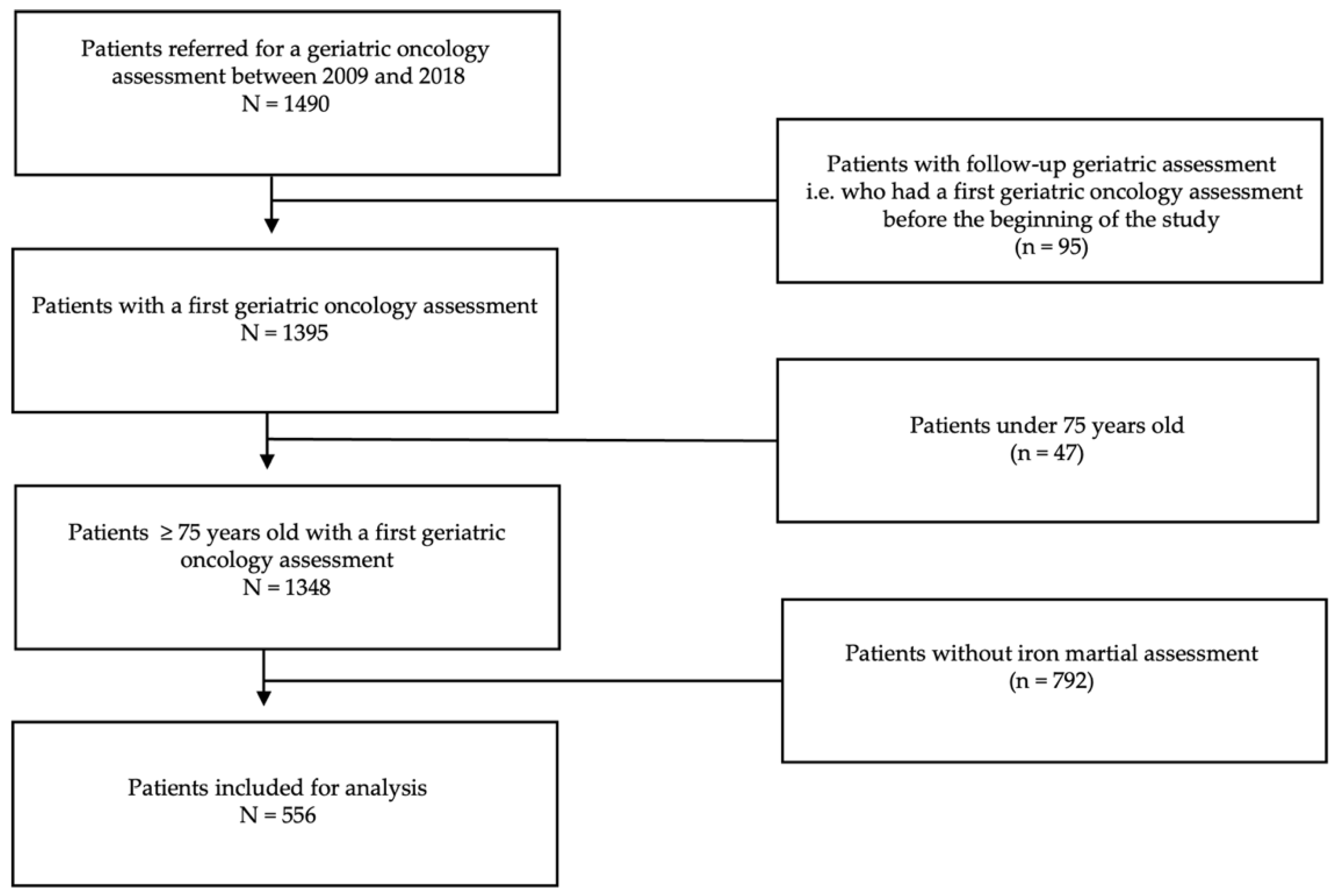
3.1. Patients
3.1.1. Iron Status
3.1.2. Oncological Characteristics
3.2. Survival Analysis
3.2.1. Survival According to General Characteristics
- Univariate analysis
- Multivariate analysis
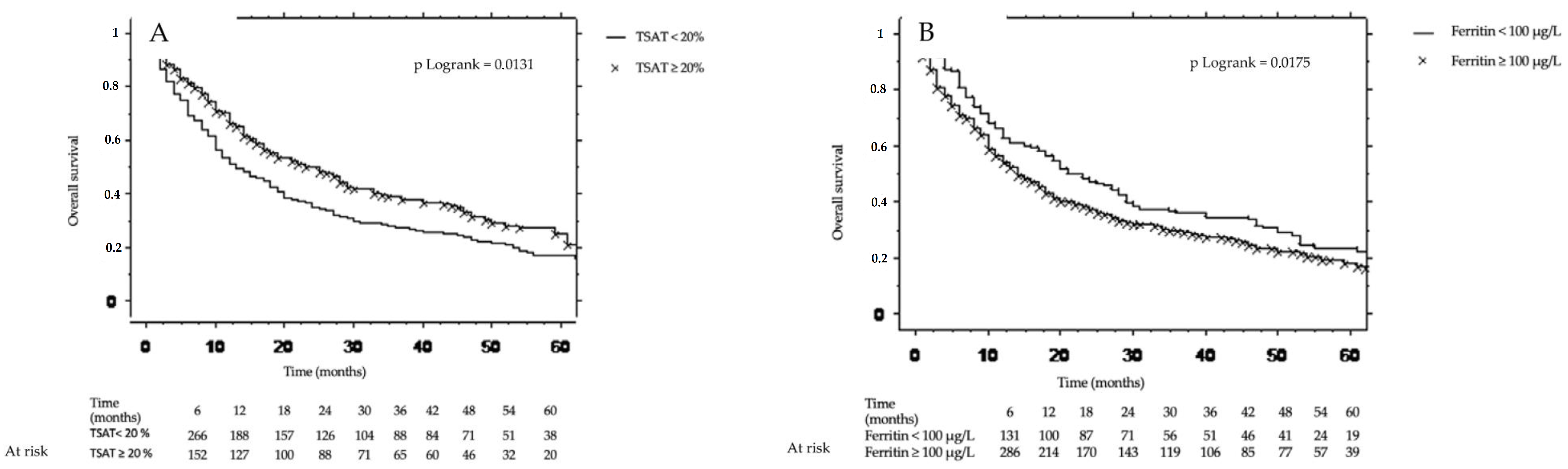
3.2.2. Survival According to Iron Status
- Univariate analysis
- Multivariate analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guralnik, J.M.; Eisenstaedt, R.S.; Ferrucci, L.; Klein, H.G.; Woodman, R.C. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004, 104, 2263–2268. [Google Scholar] [CrossRef] [PubMed]
- Lasocki, S.; Chudeau, N.; Papet, T.; Tartiere, D.; Roquilly, A.; Carlier, L.; Mimoz, O.; Seguin, P.; Malledant, Y.; Asehnoune, K.; et al. Prevalence of iron deficiency on ICU discharge and its relation with fatigue: A multicenter prospective study. Crit. Care 2014, 18, 542. [Google Scholar] [CrossRef] [PubMed]
- Phipps, O.; Brookes, M.J.; Al-Hassi, H.O. Iron deficiency, immunology, and colorectal cancer. Nutr. Rev. 2020, 79, 88–97. [Google Scholar] [CrossRef]
- Beard, J.L.; Connor, J.R.; Jones, B.C. Iron in the Brain. Nutr. Rev. 1993, 51, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Comín-Colet, J.; Enjuanes, C.; González, G.; Torrens, A.; Cladellas, M.; Meroño, O.; Ribas, N.; Ruiz, S.; Gómez, M.; Verdú, J.M.; et al. Iron deficiency is a key determinant of health-related quality of life in patients with chronic heart failure regardless of anaemia status. Eur. J. Heart Fail. 2013, 15, 1164–1172. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Ponikowski, P.; Kirwan, B.-A.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Fabien, V.; Filippatos, G.; Göhring, U.M.; Keren, A.; et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial. Lancet 2020, 396, 1895–1904. [Google Scholar] [CrossRef]
- Cacoub, P.; Choukroun, G.; Cohen-Solal, A.; Luporsi, E.; Peyrin-Biroulet, L.; Peoc’H, K.; Andrieu, V.; Lasocki, S.; Puy, H.; Trochu, J.-N. Iron deficiency screening is a key issue in chronic inflammatory diseases: A call to action. J. Intern. Med. 2022, 292, 542–556. [Google Scholar] [CrossRef]
- Eisenga, M.F.; Nolte, I.M.; van der Meer, P.; Bakker, S.J.L.; Gaillard, C.A.J.M. Association of different iron deficiency cutoffs with adverse outcomes in chronic kidney disease. BMC Nephrol. 2018, 19, 225. [Google Scholar] [CrossRef]
- Guedes, M.; Muenz, D.G.; Zee, J.; Bieber, B.; Stengel, B.; Massy, Z.A.; Mansencal, N.; Wong, M.M.; Charytan, D.M.; Reichel, H.; et al. Serum Biomarkers of Iron Stores Are Associated with Increased Risk of All-Cause Mortality and Cardiovascular Events in Nondialysis CKD Patients, with or without Anemia. J. Am. Soc. Nephrol. 2021, 32, 2020–2030. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, L.; Manning, C.; Chan, S.S.M. Prevalence of gastrointestinal malignancy in iron deficiency without anaemia: A systematic review and meta-analysis. Eur. J. Intern. Med. 2020, 72, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, M.E.; Oosterlaan, F.; van Huis, L.H.; Thielen, N.; Vondeling, A.; van den Bos, F. Nutritional status and interventions for patients with cancer—A systematic review. J. Geriatr. Oncol. 2021, 12, 6–21. [Google Scholar] [CrossRef] [PubMed]
- De Castro, J.; Gascon, P.; Casas, A.; Muñoz-Langa, J.; Alberola, V.; Cucala, M.; Baron, F. Iron deficiency in patients with solid tumours: Prevalence and management in clinical practice. Clin. Transl. Oncol. 2014, 16, 823–828. [Google Scholar] [CrossRef]
- Martens, P.; Minten, L.; Dupont, M.; Mullens, W. Prevalence of underlying gastrointestinal malignancies in iron-deficient heart failure. ESC Heart Fail. 2018, 6, 37–44. [Google Scholar] [CrossRef]
- Busti, F.; Marchi, G.; Ugolini, S.; Castagna, A.; Girelli, D. Anemia and Iron Deficiency in Cancer Patients: Role of Iron Replacement Therapy. Pharmaceuticals 2018, 11, 94. [Google Scholar] [CrossRef]
- Luporsi, E.; Carnot, A.; Massard, V.; Morin, S.; Chauffert, B.; Turpin, A.; Trochu, J.-N.; Cacoub, P. Prevalence of iron deficiency in cancer patients: The French prospective CARENFER study. J. Clin. Oncol. 2020, 38, e15617. [Google Scholar] [CrossRef]
- Ploug, M.; Kroijer, R.; Qvist, N.; Lindahl, C.H.; Knudsen, T. Iron deficiency in colorectal cancer patients: A cohort study on prevalence and associations. Color. Dis. 2021, 23, 853–859. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef]
- Balducci, L.; Beghe, C. The application of the principles of geriatrics to the management of the older person with cancer. Crit. Rev. Oncol. Hematol. 2000, 35, 147–154. [Google Scholar] [CrossRef]
- Angelini, D.E.; Radivoyevitch, T.; McCrae, K.R.; Khorana, A.A. Bleeding incidence and risk factors among cancer patients treated with anticoagulation. Am. J. Hematol. 2019, 94, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Fantony, J.J.; Inman, B. Thromboembolism and bleeding in bladder cancer. Oncology 2014, 28, 847–854. [Google Scholar] [PubMed]
- Terret, C.; Castel-Kremer, E.; Albrand, G.; Droz, J.P. Effects of comorbidity on screening and early diagnosis of cancer in elderly people. Lancet Oncol. 2009, 10, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Aapro, M.; Beguin, Y.; Bokemeyer, C.; Dicato, M.; Gascón, P.; Glaspy, J.; Hofmann, A.; Link, H.; Littlewood, T.; Ludwig, H.; et al. Management of anaemia and iron deficiency in patients with cancer: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv96–iv110. [Google Scholar] [CrossRef] [PubMed]
- Caillet, P.; Laurent, M.; Bastuji-Garin, S.; Liuu, E.; Culine, S.; Lagrange, J.-L.; Canoui-Poitrine, F.; Paillaud, E. Optimal management of elderly cancer patients: Usefulness of the Comprehensive Geriatric Assessment. Clin. Interv. Aging 2014, 9, 1645–1660. [Google Scholar] [CrossRef] [PubMed]
- Mast, A.E.; Blinder, M.A.; Gronowski, A.M.; Chumley, C.; Scott, M.G. Clinical utility of the soluble transferrin receptor and comparison with serum ferritin in several populations. Clin. Chem. 1998, 44, 45–51. [Google Scholar] [CrossRef]
- INCA—Les Cancers En France. Available online: https://www.e-cancer.fr/ressources/cancers_en_france/ (accessed on 24 February 2022).
- Roderburg, C.; Loosen, S.H.; Jahn, J.K.; Gänsbacher, J.; Luedde, T.; Kostev, K.; Luedde, M. Heart failure is associated with an increased incidence of cancer diagnoses. ESC Heart Fail. 2021, 8, 3628–3633. [Google Scholar] [CrossRef]
- Calabrich, A.; Katz, A. Management of anemia in cancer patients. Futur. Oncol. 2011, 7, 507–517. [Google Scholar] [CrossRef]
- Knight, K.; Wade, S.; Balducci, L. Prevalence and outcomes of anemia in cancer: A systematic review of the literature. Am. J. Med. 2004, 116, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yu, L.; Ding, J.; Chen, Y. Iron Metabolism in Cancer. Int. J. Mol. Sci. 2018, 20, 95. [Google Scholar] [CrossRef]
- Huang, X. Iron overload and its association with cancer risk in humans: Evidence for iron as a carcinogenic metal. Mutat. Res. Mol. Mech. Mutagen. 2003, 533, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Yalovenko, T.M.; Todor, I.M.; Lukianova, N.Y.; Chekhun, V.F. Hepcidin as a possible marker in determination of malignancy degree and sensitivity of breast cancer cells to cytostatic drugs. Exp. Oncol. 2016, 38, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Hamaï, A.; Cañeque, T.; Müller, S.; Mai, T.T.; Hienzsch, A.; Ginestier, C.; Charafe-Jauffret, E.; Codogno, P.; Mehrpour, M.; Rodriguez, R. An iron hand over cancer stem cells. Autophagy 2017, 13, 1465–1466. [Google Scholar] [CrossRef] [PubMed]
- Torti, S.V.; Torti, F.M. Iron and Cancer: 2020 Vision. Cancer Res. 2020, 80, 5435–5448. [Google Scholar] [CrossRef] [PubMed]
- Aksan, A.; Farrag, K.; Aksan, S.; Schroeder, O.; Stein, J. Flipside of the Coin: Iron Deficiency and Colorectal Cancer. Front. Immunol. 2021, 12, 635899. [Google Scholar] [CrossRef] [PubMed]
- Lachaier, E.; Louandre, C.; Godin, C.; Saidak, Z.; Baert, M.; Diouf, M.; Chauffert, B.; Galmiche, A. Sorafenib induces ferroptosis in human cancer cell lines originating from different solid tumors. Anticancer Res. 2014, 34, 6417–6422. [Google Scholar]
- Lei, G.; Zhuang, L.; Gan, B. Targeting ferroptosis as a vulnerability in cancer. Nat. Rev. Cancer 2022, 22, 381–396. [Google Scholar] [CrossRef]
- Panieri, E.; Santoro, M.M. ROS homeostasis and metabolism: A dangerous liason in cancer cells. Cell Death Dis. 2016, 7, e2253. [Google Scholar] [CrossRef]
- Migdal, C.; Serres, M. Reactive oxygen species and oxidative stress. Med. Sci. 2011, 27, 405–412. [Google Scholar] [CrossRef]
- Manz, D.H.; Blanchette, N.L.; Paul, B.T.; Torti, F.M.; Torti, S.V. Iron and cancer: Recent insights. Ann. N. Y. Acad. Sci. 2016, 1368, 149–161. [Google Scholar] [CrossRef]
- Zhang, X.; Edwards, B.J. Malnutrition in Older Adults with Cancer. Curr. Oncol. Rep. 2019, 21, 80. [Google Scholar] [CrossRef]
- Poisson, J.; Martinez-Tapia, C.; Heitz, D.; Geiss, R.; Albrand, G.; Falandry, C.; Gisselbrecht, M.; Couderc, A.; Boulahssass, R.; Liuu, E.; et al. Prevalence and prognostic impact of cachexia among older patients with cancer: A nationwide cross-sectional survey (NutriAgeCancer). J. Cachex. Sarcopenia Muscle 2021, 12, 1477–1488. [Google Scholar] [CrossRef]
- Lui, G.Y.; Kovacevic, Z.; Richardson, V.; Merlot, A.M.; Kalinowski, D.S.; Richardson, D.R. Targeting cancer by binding iron: Dissecting cellular signaling pathways. Oncotarget 2015, 6, 18748–18779. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.L.; Lee, D.-H.; Na, Y.J.; Kim, B.R.; Jeong, Y.A.; Lee, S.I.; Kang, S.; Joung, S.Y.; Lee, S.-Y.; Oh, S.C.; et al. Iron chelator-induced apoptosis via the ER stress pathway in gastric cancer cells. Tumour Biol. 2016, 37, 9709–9719. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.Y.; Mina, E.; Roetto, A.; Porporato, P.E. Iron: An Essential Element of Cancer Metabolism. Cells 2020, 9, 2591. [Google Scholar] [CrossRef] [PubMed]
- Crielaard, B.J.; Lammers, T.; Rivella, S. Targeting iron metabolism in drug discovery and delivery. Nat. Rev. Drug Discov. 2017, 16, 400–423. [Google Scholar] [CrossRef] [PubMed]
- Făgărășan, V.; Andraș, D.; Amarinei, G.; Seicean, R.I.; Bințințan, V.V.; Dindelegan, G.C.; Căinap, C.I. Absolute and Functional Iron Deficiency in Colon Cancer: A Cohort Study. Medicina 2022, 58, 1202. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.V.; Agar, M.R.; Soo, W.-K.; To, T.; Phillips, J.L. Screening Tools for Identifying Older Adults with Cancer Who May Benefit from a Geriatric Assessment: A Systematic Review. JAMA Oncol. 2021, 7, 616–627. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Rodriguez, R.A.; Humphreys, M.H. Association between serum ferritin and measures of inflammation, nutrition and iron in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 141–149. [Google Scholar] [CrossRef]
- National Kidney Foundation Anemia Working Group. NKF-K/DOQI Clinical Practice Guidelines for Anemia of Chronic Kidney Disease: Update 2000. Am. J. Kidney Dis. 2001, 37, S182–S238. [Google Scholar] [CrossRef]
- Patterson, C.; Turpie, I.D.; Benger, A.M. Assessment of Iron Stores in Anemic Geriatric Patients. J. Am. Geriatr. Soc. 1985, 33, 764–767. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | N, (%) |
|---|---|
| Gender, n = 556 (female) | 245 (44) |
| Age, n = 556 (years), mean (S.D) | 82 (±4.6) |
| Duration follow-up, n = 556, days (median) [interquartiles] | 484 [190–1377] |
| Geriatric assessment | |
| ADL, n = 555, mean (S.D) | 5 (±1) |
| IADL, n = 342, mean (S.D) | 5 (±3.5) |
| Place of living, n = 539 | |
| Community | 472 (88) |
| Nursing home | 40 (7) |
| Residential care home | 10 (2) |
| Service home | 2 (0.4) |
| Long-term care unit | 1 (0.2) |
| CIRS-G, n = 556, mean (S.D) | 8 (±5) |
| MNA, n = 553, mean (S.D) | 21 (±6) |
| GDS 15, n = 425, mean (S.D) | 4 (±3) |
| MMSE, n = 536, mean (S.D) | 26 (±5) |
| Timed up and go, n = 533 (pathological) | 151 (28) |
| Chair stand test, n = 459 (pathological) | 170 (37) |
| Single-leg stance test, n = 492 (pathological) | 256 (52) |
| Comorbidities | |
| Chronic heart failure, n = 556 | 159 (29) |
| Chronic renal disease, n = 528 | 323 (61) |
| Anemia, n = 545 | 302 (55) |
| Iron measurements | |
| Ferritin (µg/L), n = 545, mean (S.D) | 381 (±366) |
| TSAT, n = 545 | 18 (±13) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | [95% CI] | p * | HR | [95% CI] | p * | |
| Gender, female | 0.83 | [0.69–1.01] | 0.0683 | - | - | - |
| Age, years | 1.02 | [1.00–1.04] | 0.0306 | 1.03 | [1.00–1.06] | 0.0404 |
| ADL (+1 point) | 0.80 | [0.74–0.86] | <0.0001 | 0.89 | [0.75–1.06] | 0.1969 |
| IADL (+1 point) | 0.90 | [0.86–0.95] | <0.0001 | 0.97 | [0.90–1.05] | 0.5211 |
| CIRS-G (+1 point) | 1.02 | [1.00–1.05] | 0.0154 | 1.01 | [0.98–1.05] | 0.2798 |
| MNA (+1 point) | 0.89 | [0.88–0.91] | <0.0001 | 0.92 | [0.89–0.96] | <0.0001 |
| GDS 15 (+1 point) | 1.04 | [1.00–1.07] | 0.0318 | 1.01 | [0.97–1.07] | 0.4479 |
| MMSE (+1 point) | 0.97 | [0.95–0.99] | 0.0349 | 1.02 | [0.99–1.06] | 0.1404 |
| Chronic renal failure | 1.35 | [1.11–1.65] | 0.0027 | 1.04 | [0.76–1.42] | 0.7936 |
| Chronic heart failure | 1.24 | [1.02–1.52] | 0.0314 | 1.35 | [1.00–1.84] | 0.0496 |
| Timed up and Go, pathological | 1.42 | [1.15–1.75] | 0.0009 | 1.05 | [0.64–1.73] | 0.8323 |
| Chair stand test, pathological | 1.50 | [1.21–1.86] | 0.0002 | 0.95 | [0.58–1.53] | 0.8385 |
| Single-leg stance test, pathological | 1.31 | [1.07–1.60] | 0.0075 | 1.23 | [0.88–1.70] | 0.2112 |
| Cancers at risk of bleeding ** | 1.26 | [1.04–1.52] | 0.0150 | 1.28 | [0.95–1.72] | 0.1038 |
| Metastases | 1.86 | [1.54–2.25] | <0.0001 | 2.22 | [1.65–2.98] | <0.0001 |
| Anemia | 1.71 | [1.41–2.08] | <0.0001 | 1.41 | [1.05–1.90] | 0.0209 |
| Univariate Analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Independently of Anemia | Without Anemia | With Anemia | ||||||
| HR | [95% CI] | p * | HR | [95% CI] | p * | HR | [95% CI] | p * | |
| Severe ID | 0.66 | [0.45–0.96] | 0.0305 | 0.70 | [0.40–1.22] | 0.2107 | 0.65 | [0.40–1.07] | 0.938 |
| ID | 1.29 | [1.06–1.58] | 0.0106 | 0.70 | [0.56–0.88] | 0.0024 | 1.69 | [1.40–2.05] | <0.0001 |
| AID | 0.77 | [0.63–0.96] | 0.0200 | 0.72 | [0.53–0.98] | 0.0393 | 0.87 | [0.67–1.13] | 0.3126 |
| FID | 1.44 | [1.19–1.74] | 0.0001 | 0.73 | [0.56–0.96] | 0.0244 | 2.07 | [1.96–2.55] | <0.0001 |
| Multivariate Analysis | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Without Anemia | With Anemia | |||||||||
| HR | [95% CI] | p * | HR | [95% CI] | p * | HR | [95% CI] | p * | |||
| FID | 0.65 | [0.43–0.99] | 0.0495 | ID | 1.51 | [1.12–2.05] | 0.0065 | FID | 1.73 | [1.26–2.38] | 0.0007 |
| Age | 1.03 | [0.99–1.06] | 0.0588 | Age | 1.03 | [0.57–1.51] | 0.0495 | Age | 1.03 | [0.99–1.06] | 0.0759 |
| ADL | 0.89 | [0.75–1.06] | 0.2132 | ADL | 0.90 | [0.76–1.07] | 0.2714 | ADL | 0.92 | [0.77–1.09] | 0.3457 |
| IADL | 0.96 | [0.89–1.04] | 0.3834 | IADL | 0.96 | [0.89–1.03] | 0.3147 | IADL | 0.95 | [0.88–1.03] | 0.2533 |
| CIRS-G | 1.01 | [0.98–1.05] | 0.3033 | CIRS-G | 1.02 | [0.98–1.05] | 0.2311 | CIRS-G | 1.02 | [0.99–1.06] | 0.1281 |
| MNA | 0.92 | [0.88–0.95] | <0.0001 | MNA | 0.93 | [0.89–0.96] | 0.0004 | MNA | 0.93 | [0.89–0.97] | 0.0006 |
| GDS 15 | 1.02 | [0.97–1.08] | 0.3042 | GDS 15 | 1.02 | [0.97–1.07] | 0.3756 | GDS 15 | 1.02 | [0.97–1.07] | 0.3631 |
| MMSE | 1.03 | [0.99–1.06] | 0.0864 | MMSE | 1.02 | [0.99–1.06] | 0.1194 | MMSE | 1.02 | [0.99–1.06] | 0.1532 |
| Timed up and go | 1.07 | [0.65–1.77] | 0.7665 | Timed Up and Go | 1.06 | [0.64–1.76] | 0.8072 | Timed Up and Go | 1.01 | [0.61–1.67] | 0.9582 |
| Chair stand test | 0.93 | [0.58–1.51] | 0.7970 | Chair stand test | 0.93 | [0.57–1.51] | 0.7865 | Chair stand test | 1.00 | [0.62–1.62] | 0.9769 |
| Single-leg stance test | 1.23 | [0.88–1.71] | 0.2147 | Single-leg stance test | 1.22 | [0.79–1.69] | 0.2348 | Single-leg stance test | 1.21 | [0.87–1.68] | 0.2528 |
| Chronic renal failure | 1.13 | [0.83–1.53] | 0.4231 | Chronic renal failure | 1.08 | [0.79–1.46] | 0.6083 | Chronic renal failure | 1.08 | [0.80–1.47] | 0.5995 |
| Chronic heart failure | 1.44 | [1.07–1.95] | 0.0162 | Chronic heart failure | 1.33 | [0.98–1.81] | 0.0664 | Chronic heart failure | 1.41 | [1.04–1.90] | 0.0243 |
| Cancers at risk of bleeding ** | 1.34 | [0.99–1.80] | 0.0515 | Cancers at risk of bleeding ** | 1.21 | [0.89–1.64] | 0.2245 | Cancers at risk of bleeding ** | 1.29 | [0.96–1.74] | 0.0877 |
| Metastases | 2.25 | [1.67–3.02] | <0.0001 | Metastases | 2.16 | [1.61–2.91] | <0.0001 | Metastases | 2.12 | [1.58–2.85] | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tisserand, J.; Randrian, V.; Paccalin, M.; Saulnier, P.-J.; Arviset, M.; Fourmy, A.; Arriudarré, V.; Jamet, A.; Moreno, Y.; Valéro, S.; et al. Association between Iron Deficiency and Survival in Older Patients with Cancer. Cancers 2023, 15, 1533. https://doi.org/10.3390/cancers15051533
Tisserand J, Randrian V, Paccalin M, Saulnier P-J, Arviset M, Fourmy A, Arriudarré V, Jamet A, Moreno Y, Valéro S, et al. Association between Iron Deficiency and Survival in Older Patients with Cancer. Cancers. 2023; 15(5):1533. https://doi.org/10.3390/cancers15051533
Chicago/Turabian StyleTisserand, Julie, Violaine Randrian, Marc Paccalin, Pierre-Jean Saulnier, Marine Arviset, Arthur Fourmy, Victor Arriudarré, Amélie Jamet, Yvan Moreno, Simon Valéro, and et al. 2023. "Association between Iron Deficiency and Survival in Older Patients with Cancer" Cancers 15, no. 5: 1533. https://doi.org/10.3390/cancers15051533
APA StyleTisserand, J., Randrian, V., Paccalin, M., Saulnier, P.-J., Arviset, M., Fourmy, A., Arriudarré, V., Jamet, A., Moreno, Y., Valéro, S., & Liuu, E. (2023). Association between Iron Deficiency and Survival in Older Patients with Cancer. Cancers, 15(5), 1533. https://doi.org/10.3390/cancers15051533