
Management and Oncologic Outcomes of Close and Positive Margins after Transoral CO2 Laser Microsurgery for Early Glottic Carcinoma

 ,
,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Remacle, M.; Arens, C.; Eldin, M.B.; Campos, G.; Estomba, C.C.; Dulguerov, P.; Fiz, I.; Hantzakos, A.; Keghian, J.; Mora, F.; et al. Laser-assisted surgery of the upper aero-digestive tract: A clarification of nomenclature. A consensus statement of the European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2018, 275, 657–658, Erratum for: Eur. Arch. Otorhinolaryngol. 2017, 274, 3723–3727. [Google Scholar] [CrossRef]
- Carta, F.; Bandino, F.; Olla, A.M.; Chuchueva, N.; Gerosa, C.; Puxeddu, R. Prognostic value of age, subglottic, and anterior commissure involvement for early glottic carcinoma treated with CO2 laser transoral microsurgery: A retrospective, single-center cohort study of 261 patients. Eur. Arch. Otorhinolaryngol. 2018, 275, 1199–1210. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, E.V. Transoral laser microsurgery in early glottic lesions. Curr. Otorhinolaryngol. Rep. 2017, 5, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Ansarin, M.; Santoro, L.; Cattaneo, A.; Massaro, M.A.; Calabrese, L.; Giugliano, G.; Maffini, F.; Ostuni, A.; Chiesa, F. Laser surgery of early glottic cancer; impact of margin status on local control and organ preservation. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Fiz, I.; Mazzola, F.; Fiz, F.; Marchi, F.; Filauro, M.; Paderno, A.; Parrinello, G.; Piazza, C.; Peretti, G. Impact of close and positive margins in transoral laser microsurgery for Tis-T2 glottic cancer. Front. Oncol. 2017, 7, 245. [Google Scholar] [CrossRef] [PubMed]
- Aluffi Valletti, P.; Taranto, F.; Chiesa, A.; Pia, F.; Valente, G. Impact of resection margin status on oncological outcomes after CO2 laser cordectomy. Acta Otorhinolaryngol. Ital. 2018, 38, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Galli, A.; Giordano, L.; Sarandria, D.; Di Santo, D.; Bussi, M. Oncological and complication assessment of CO2 laser-assisted endoscopic surgery for T1-T2 glottic tumours: Clinical experience. Acta Otorhinolaryngol. Ital. 2016, 36, 167–173. [Google Scholar] [CrossRef]
- Bertolin, A.; Lionello, M.; Salis, G.; Rizzotto, G.; Lucioni, M. Two-stage CO2 -laser-assisted bilateral cordectomy for cT1b glottic carcinoma. Am. J. Otolaryngol. 2017, 38, 183–187. [Google Scholar] [CrossRef]
- Fiz, I.; Koelmel, J.C.; Sittel, C. Nature and role of surgical margins in transoral laser microsurgery for early and intermediate glottic cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 78–83. [Google Scholar] [CrossRef]
- Gallet, P.; Rumeau, C.; Nguyen, D.T.; Teixeira, P.A.; Baumann, C.; Toussaint, B. “Watchful observation” follow-up scheme after endoscopic CO2 laser treatment for small glottic carcinomas: A retrospective study of 93 cases. Clin. Otolaryngol. 2017, 42, 1193–1199. [Google Scholar] [CrossRef]
- Canis, M.; Ihler, F.; Martin, A.; Matthias, C.; Steiner, W. Transoral laser microsurgery for T1a glottic cancer: Review of 404 cases. Head Neck. 2015, 37, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Jäckel, M.C.; Ambrosch, P.; Martin, A.; Steiner, W. Impact of re-resection for inadequate margins on the prognosis of upper aerodigestive tract cancer treated by laser microsurgery. Laryngoscope 2007, 117, 350–356. [Google Scholar] [CrossRef]
- Peretti, G.; Piazza, C.; Bolzoni, A.; Mensi, M.C.; Rossini, M.; Parrinello, G.; Shapshay, S.M.; Antonelli, A.R. Analysis of recurrences in 322 Tis, T1, or T2 glottic carcinomas treated by carbon dioxide laser. Ann. Otol. Rhinol. Laryngol. 2004, 113, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Puxeddu, R.; Sionis, S.; Gerosa, C.; Carta, F. Enhanced contact endoscopy for the detection of neoangiogenesis in tumors of the larynx and hypopharynx. Laryngoscope 2015, 125, 1600–1606. [Google Scholar] [CrossRef]
- Remacle, M.; Eckel, H.E.; Antonelli, A.; Brasnu, D.; Chevalier, D.; Friedrich, G.; Olofsson, J.; Rudert, H.H.; Thumfart, W.; de Vincentiis, M.; et al. Endoscopic cordectomy. A proposal for a classification by the Working Committee, European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2000, 257, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Remacle, M.; van Haverbeke, C.; Eckel, H.; Bradley, P.; Chevalier, D.; Djukic, V.; de Vicentiis, M.; Friedrich, G.; Olofsson, J.; Peretti, G.; et al. Proposal for revision of the European Laryngological Society classification of endoscopic cordectomies. Eur. Arch. Otorhinolaryngol. 2007, 264, 499–504, Erratum in: Eur. Arch. Otorhinolaryngol. 2007, 264, 709. [Google Scholar] [CrossRef]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers-major changes in the American joint committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Roman, B.R.; Goldenberg, D.; Givi, B. AHNS series-do you know your guidelines? Guideline recommended follow-up and surveillance of head and neck cancer survivors. Head Neck 2016, 38, 168–174. [Google Scholar] [CrossRef]
- Carta, F.; Mariani, C.; Quartu, D.; Gioia, E.; Chuchueva, N.; Puxeddu, R. Single and double mucosal microflap CO2 laser “sliding” technique in the management of iatrogenic glottic web: Anatomical and functional results. Eur. Arch. Otorhinolaryngol. 2019, 276, 3405–3412. [Google Scholar] [CrossRef]
- Piazza, C.; Paderno, A.; Grazioli, P.; Del Bon, F.; Montalto, N.; Perotti, P.; Morello, R.; Filauro, M.; Nicolai, P.; Peretti, G. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery. Laryngoscope 2017, 128, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Bertino, G.; Degiorgi, G.; Tinelli, C.; Cacciola, S.; Occhini, A.; Benazzo, M. CO2 laser cordectomy for T1-T2 glottic cancer: Oncological and functional long-term results. Eur. Arch. Otorhinolaryngol. 2015, 272, 2389–2395. [Google Scholar] [CrossRef] [PubMed]
- Charbonnier, Q.; Thisse, A.S.; Sleghem, L.; Mouawad, F.; Chevalier, D.; Page, C.; Mortuaire, G. Oncologic outcomes of patients with positive margins after laser cordectomy for T1 and T2 glottic squamous cell carcinoma. Head Neck 2016, 38, 1804–1809. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Chun, B.G.; Kim, S.W.; Kim, S.T.; Oh, J.H.; Hong, J.C.; Lee, K.D. Transoral laser microsurgery for early glottic cancer as one-stage single-modality therapy. Laryngoscope 2013, 123, 2670–2674. [Google Scholar] [CrossRef]
- Hartl, D.M.; de Monès, E.; Hans, S.; Janot, F.; Brasnu, D. Treatment of early-stage glottic cancer by transoral laser resection. Ann. Otol. Rhinol. Laryngol. 2007, 116, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Karatzanis, A.D.; Waldfahrer, F.; Psychogios, G.; Hornung, J.; Zenk, J.; Velegrakis, G.A.; Iro, H. Resection margins and other prognostic factors regarding surgically treated glottic carcinomas. J. Surg. Oncol. 2010, 101, 131–136. [Google Scholar] [CrossRef]
- Jumaily, M.; Faraji, F.; Osazuwa-Peters, N.; Walker, R.J.; Ward, G.M. Prognostic significance of surgical margins after transoral laser microsurgery for early-stage glottic squamous cell carcinoma. Oral Oncol. 2019, 97, 105–111. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Lu, Z.M.; Luo, X.N.; Chen, L.S.; Ge, P.J.; Song, X.H.; Chen, S.H.; Wu, Y.L. Retrospective analysis of prognostic factors in 205 patients with laryngeal squamous cell carcinoma who underwent surgical treatment. PLoS ONE 2013, 8, e60157. [Google Scholar] [CrossRef]
- Garofolo, S.; Piazza, C.; Del Bon, F.; Mangili, S.; Guastini, L.; Mora, F.; Nicolai, P.; Peretti, G. Intraoperative narrow band imaging better delineates superficial resection margins during transoral laser microsurgery for early glottic cancer. Ann. Otol. Rhinol. Laryngol. 2015, 124, 294–298. [Google Scholar] [CrossRef]
- Meulemans, J.; Hauben, E.; Peeperkorn, S.; Nuyts, S.; Delaere, P.; Poorten, V.V. Transoral laser microsurgery (TLM) for glottic cancer: Prospective assessment of a new pathology workup protocol. Front. Surg. 2020, 7, 56. [Google Scholar] [CrossRef]
- Campo, F.; D’Aguanno, V.; Greco, A.; Ralli, M.; De Vincentiis, M. The prognostic value of adding narrow-band imaging in transoral laser microsurgery for early glottic cancer: A review. Lasers Surg. Med. 2020, 52, 301–306. [Google Scholar] [CrossRef]
- Blanch, J.L.; Vilaseca, I.; Bernal-Sprekelsen, M.; Grau, J.J.; Moragas, M.; Traserra-Coderch, J.; Caballero, M.; Sabater, F.; Guilemany, J.M.; Alos, L. Prognostic significance of surgical margins in transoral CO2 laser microsurgery for T1–T4 pharyngo- laryngeal cancers. Eur. Arch. Otorhinolaryngol. 2007, 264, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Hendriksma, M.; Montagne, M.W.; Langeveld, T.P.M.; Veselic, M.; van Benthem, P.P.G.; Sjögren, E.V. Evaluation of surgical margin status in patients with early glottic cancer (Tis-T2) treated with transoral CO2 laser microsurgery, on local control. Eur. Arch. Otorhinolaryngol. 2018, 275, 2333–2340. [Google Scholar] [CrossRef] [PubMed]
- Verro, B.; Greco, G.; Chianetta, E.; Saraniti, C. Management of Early Glottic Cancer Treated by CO2 Laser According to Surgical-Margin Status: A Systematic Review of the Literature. Int. Arch. Otorhinolaryngol. 2021, 25, e301–e308. [Google Scholar] [CrossRef]
- Mariani, C.; Carta, F.; Tatti, M.; Marrosu, V.; Gerosa, C.; Puxeddu, R. Shrinkage of specimens after CO2 laser cordectomy: An objective intraoperative evaluation. Eur. Arch. Otorhinolaryngol. 2021, 278, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.; Fakhry, N.; Duflo, S.; Lagier, A.; Mancini, J.; Dessi, P.; Giovanni, A. Prognostic value of the status of resection margins after endoscopic laser cordectomy for T1a glottic carcinoma. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 297–300. [Google Scholar] [CrossRef]
- Ansarin, M.; Cattaneo, A.; de Benedetto, L.; Zorzi, S.; Lombardi, F.; Alterio, D.; Rocca, M.C.; Scelsi, D.; Preda, L.; Chiesa, F.; et al. Retrospective analysis of factors influencing oncologic outcome in 590 patients with early-intermediate glottic cancer treated by transoral laser microsurgery. Head Neck 2017, 39, 71–81. [Google Scholar] [CrossRef]
- Poorten, V.V.; Meulemans, J.; Van Lierde, C.; Nuyts, S.; Delaere, P. Current indications for adjuvant treatment following transoral laser microsurgery of early and intermediate laryngeal cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 79–85. [Google Scholar] [CrossRef]
- Meulemans, J.; Bijnens, J.; Delaere, P.; Poorten, V.V. Up-front and salvage transoral laser microsurgery for early glottic squamous cell carcinoma: A single centre retrospective case series. Front. Oncol. 2018, 8, 186. [Google Scholar] [CrossRef]
- Djukic, V.; Milovanović, J.; Jotić, A.D.; Vukasinovic, M.; Folic, M.M.; Ivanov, S.Y.; Satueva, D.B. Laser transoral microsurgery in treatment of early laryngeal carcinoma. Eur. Arch. Otorhinolaryngol. 2019, 276, 1747–1755. [Google Scholar] [CrossRef]
- Grant, D.G.; Bradley, P.T.; Parmar, A.; Toll, E.C.; Baldwin, D.L.; Porter, G.C.; Tierney, P.A. Implications of positive margins or incomplete excision in laryngeal cancer treated by transoral laser microsurgery: How we do it. Clin. Otolaryngol. 2009, 34, 485–489. [Google Scholar] [CrossRef]
- Peretti, G.; Piazza, C.; Mensi, M.C.; Magnoni, L.; Bolzoni, A. Endoscopic treatment of cT2 glottic carcinoma: Prognostic impact of different pT subcategories. Ann. Otol. Rhinol. Laryngol. 2005, 114, 579–586. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | No. of Patients |
|---|---|
| All | 351 |
| Age | 65.6 (range 29–90 years) |
| Male/female | 328/23 |
| Type of surgical cordectomies | 34 type I cordectomy 94 type II cordectomy 77 type III cordectomy 21 type IV cordectomy 122 type V cordectomy (61 a, 7 ab, 4 abc, 11 abcd, 2 abd, 10 ac, 8 acd, 7 ad, 7 b, 3 bc, 2 c) 3 type VI cordectomy |
| Clinical N classification | 351 cN0 |
| Pathological T classification | 34 pTis 193 pT1a 61 pT1b 63 pT2 |
| Margin status | 286 NEG 8 CS 15 CD 16 SS 9 MS 17 DEEP |
| Patient/Sex/Age (Years) | Type of Cordectomy | pT | Margin Status after Primary Treatment | CO2 Laser Enlargement | Site of Relapse/Time of Relapse (Years) | Salvage Treatment | Outcome/Time of Last Follow-Up (Years) |
|---|---|---|---|---|---|---|---|
| DG/M/76.3 | Va | 1b | NEG | - | Larynx/1.7 | CO2 TOLMS and radiotherapy | DOC/2.5 |
| FE/M/68.5 | IV | 1b | NEG | - | Larynx/0.3 | CO2 TOLMS | NED/7 |
| MG/M/70.1 | II | 1a | NEG | - | Larynx/0.6 | Type II horizontal laryngectomy and radiotherapy | NED/5 |
| VA/M/61.9 | II | 1a | NEG | - | Larynx/2.4 | CO2 TOLMS | DOC/11.1 |
| RB/M/82.7 | Vabc | 2 | DEEP | Yes (no residual tumor at histology) | Larynx/2.4 | Refused treatment | DOD/2.5 |
| DE/M/72.8 | II | 1a | NEG | - | Larynx/0.7 | CO2 TOLMS | DOC/4.9 |
| LS/M/76.6 | Va | 2 | NEG | - | Larynx/1.7 | CO2 TOLMS | DOC/4.3 |
| FG/M/64.1 | Vacd | 2 | NEG | - | Larynx/1.3 | Type II horizontal laryngectomy | NED/11 |
| MS/M/53.5 | IV | 1a | NEG | - | Larynx/3 | Total laryngectomy | NED/7.8 |
| SC/M/61.4 | III | 1a | NEG | - | Larynx/0.8 | CO2 TOLMS | NED/6.6 |
| CS/M/60.9 | II | 1a | NEG | - | Larynx/1.8 | CO2 TOLMS | NED/2.1 |
| ZF/M/71.5 | Vabcd | 2 | NEG | - | Larynx/0.2 | Total laryngectomy | DOC/0.5 |
| PB/M/64.1 | Vac | 2 | DEEP | Yes (no residual tumor at histology) | Larynx/1.2 | Total laryngectomy | NED/5.2 |
| RM/M/73.8 | I | 1a | NEG | - | Larynx/1.2 | Radiotherapy | NED/5.7 |
| DS/F/62.8 | Vabcd | 2 | NEG | - | Larynx/0.5 | Total laryngectomy and radiotherapy | NED/5.1 |
| BM/M/51.7 | Vb | 1a | NEG | - | Larynx/2.1 | Type III horizontal laryngectomy | NED/3.2 |
| SG/M/68.3 | Vac | 1b | NEG | - | Neck node/0.9 | Neck dissection and radiotherapy | NED/1.5 |
| MI/M/48.1 | II | 1a | DEEP | Yes (no residual tumor at histology) | Larynx/1.2 | CO2 TOLMS | NED/4.8 |
| LM/M/68.7 | II | 1b | CD | No | Larynx/0.5 | CO2 TOLMS | NED/5 |
| PA/M/74.1 | Va | 1b | NEG | - | Larynx/0.8 | CO2 TOLMS | NED/5 |
| CA/M/70.3 | III | 1b | NEG | - | Larynx/0.6 | CO2 TOLMS | DOC/2.2 |
| MV/M/65.7 | II | 1b | CD | No | Larynx/1.3 | CO2 TOLMS | NED/1.6 |
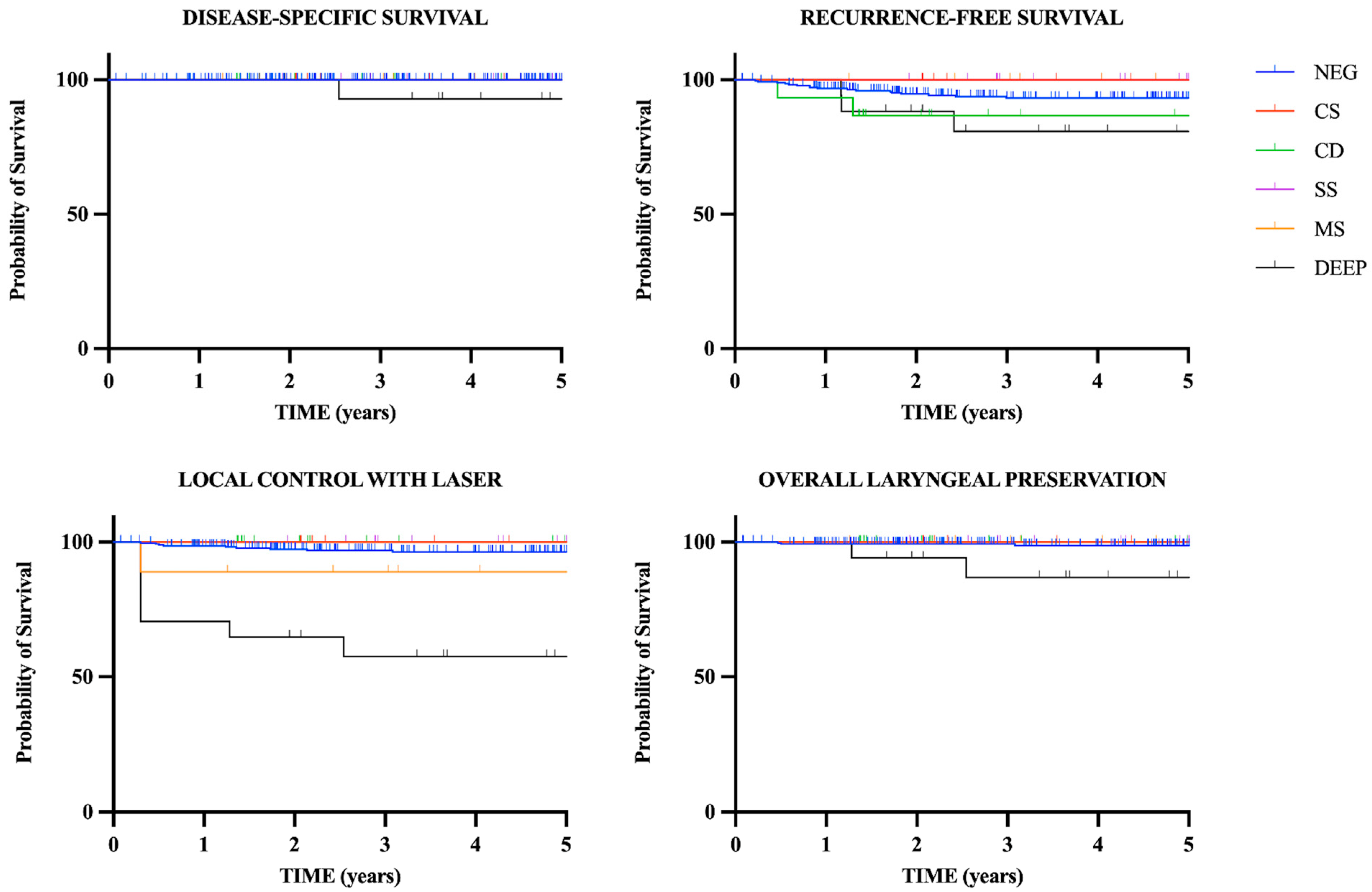
| DSS 5 Years | RFS 5 Years | LCL 5 Years | OLP 5 Years | |
|---|---|---|---|---|
| All patients (n = 351) | 99.6% | 92.9% | 94.6% | 98.2% |
| NEG margins (n = 286) | 100% | 93.2% | 96.4% | 98.7% |
| CS margin (n = 8) | 100% | 100% | 100% | 100% |
| CD margin (n = 15) | 100% | 86.7% | 100% | 100% |
| SS margin (n = 16) | 100% | 100% | 100% | 100% |
| MS margins (n = 9) | 100% | 100% | 88.9% | 100% |
| DEEP margin (n = 17) | 92.9% | 80.9% | 57.5% | 86.9% |
| Recurrence | 5-Year RFS | Hazard Ratio (95% CI) | p | |
|---|---|---|---|---|
| NEG margins (n = 286) | 17 (5.9%) | 93.2% | 1 (Reference) | NA |
| CD margin (n = 15) | 2 (13.3%) | 86.7% | 2.537 (0.2854–22.55) | =0.2 |
| DEEP margin (n = 17) | 3 (17.6%) | 80.9% | 2.863 (0.4395–18.66) | =0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mariani, C.; Carta, F.; Bontempi, M.; Marrosu, V.; Tatti, M.; Pinto, V.; Gerosa, C.; Puxeddu, R. Management and Oncologic Outcomes of Close and Positive Margins after Transoral CO2 Laser Microsurgery for Early Glottic Carcinoma. Cancers 2023, 15, 1490. https://doi.org/10.3390/cancers15051490
Mariani C, Carta F, Bontempi M, Marrosu V, Tatti M, Pinto V, Gerosa C, Puxeddu R. Management and Oncologic Outcomes of Close and Positive Margins after Transoral CO2 Laser Microsurgery for Early Glottic Carcinoma. Cancers. 2023; 15(5):1490. https://doi.org/10.3390/cancers15051490
Chicago/Turabian StyleMariani, Cinzia, Filippo Carta, Mauro Bontempi, Valeria Marrosu, Melania Tatti, Valeria Pinto, Clara Gerosa, and Roberto Puxeddu. 2023. "Management and Oncologic Outcomes of Close and Positive Margins after Transoral CO2 Laser Microsurgery for Early Glottic Carcinoma" Cancers 15, no. 5: 1490. https://doi.org/10.3390/cancers15051490
APA StyleMariani, C., Carta, F., Bontempi, M., Marrosu, V., Tatti, M., Pinto, V., Gerosa, C., & Puxeddu, R. (2023). Management and Oncologic Outcomes of Close and Positive Margins after Transoral CO2 Laser Microsurgery for Early Glottic Carcinoma. Cancers, 15(5), 1490. https://doi.org/10.3390/cancers15051490