
The Prognostic Value of DCE-MRI Findings before Salvage Radiotherapy after Radical Prostatectomy
 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Restaging Work-Up
2.3. Treatment
2.4. Endpoints
2.5. Statistical Analysis
3. Results
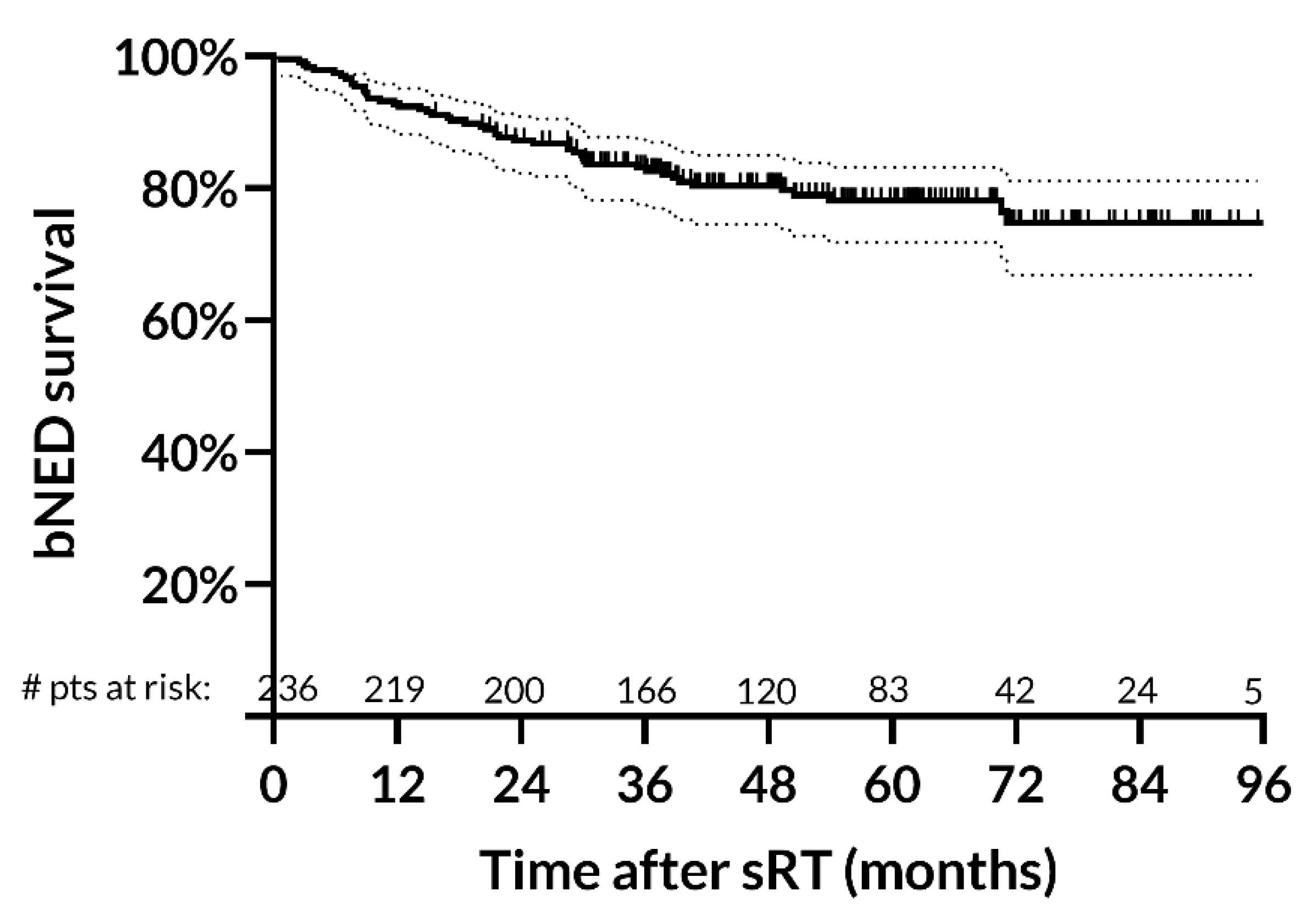
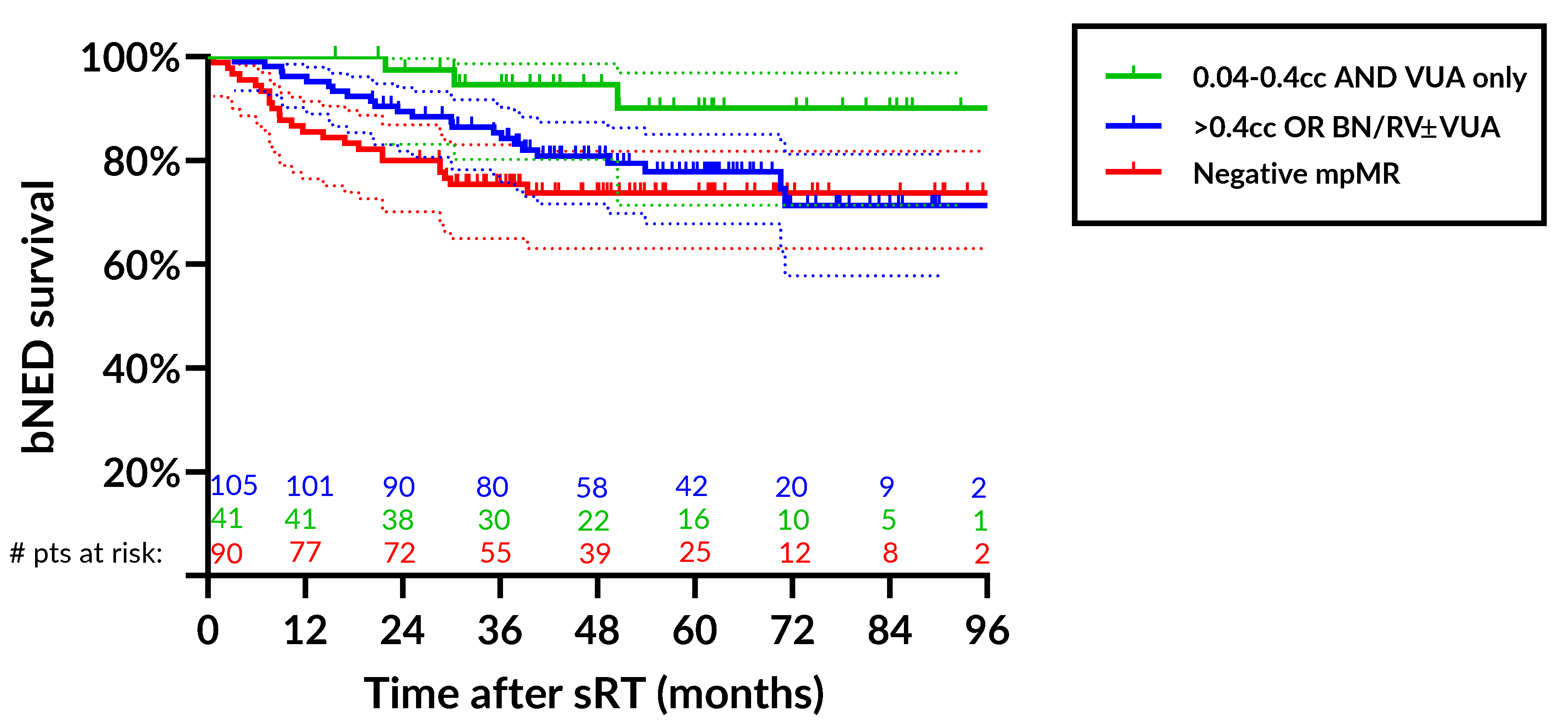
bNED Rates & Predictors of Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomised, controlled phase 3 trial. Lancet 2020, 396, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; Mason, M.D.; et al. EAU Guidelines. In Proceedings of the EAU Annual Congress Milan, Milan, Italy, 19–23 March 2021; ISBN 978-94-92671-13-4. [Google Scholar]
- Emmett, L.; van Leeuwen, P.J.; Nandurkar, R.; Scheltema, M.J.; Cusick, T.; Hruby, G.; Kneebone, A.; Eade, T.; Fogarty, G.; Jagavkar, R.; et al. Treatment Outcomes from (68)Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET. J. Nucl. Med. 2017, 58, 1972–1976. [Google Scholar] [CrossRef] [PubMed]
- Farolfi, A.; Ceci, F.; Castellucci, P.; Graziani, T.; Siepe, G.; Lambertini, A.; Schiavina, R.; Lodi, F.; Morganti, A.G.; Fanti, S. (68)Ga-PSMA-11 PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy and PSA <0.5 ng/mL. Efficacy and impact on treatment strategy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ghadjar, P.; Hayoz, S.; Bernhard, J.; Zwahlen, D.R.; Holscher, T.; Gut, P.; Polat, B.; Hildebrandt, G.; Muller, A.C.; Plasswilm, L.; et al. Dose-intensified Versus Conventional-dose Salvage Radiotherapy for Biochemically Recurrent Prostate Cancer After Prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur. Urol. 2021, 80, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Shimoyachi, N.; Yoshioka, Y.; Sasamura, K.; Yonese, J.; Yamamoto, S.; Yuasa, T.; Soyano, T.; Kozuka, T.; Oguchi, M. Comparison Between Dose-Escalated Intensity Modulated Radiation Therapy and 3-Dimensional Conformal Radiation Therapy for Salvage Radiation Therapy After Prostatectomy. Adv. Radiat. Oncol. 2021, 6, 100753. [Google Scholar] [CrossRef]
- Zilli, T.; Jorcano, S.; Peguret, N.; Caparrotti, F.; Hidalgo, A.; Khan, H.G.; Vees, H.; Weber, D.C.; Miralbell, R. Dose-adapted salvage radiotherapy after radical prostatectomy based on an erMRI target definition model: Toxicity analysis. Acta Oncol. 2014, 53, 96–102. [Google Scholar] [CrossRef]
- Breen, W.G.; Stish, B.J.; Harmsen, W.S.; Froemming, A.T.; Mynderse, L.A.; Choo, C.R.; Davis, B.J.; Pisansky, T.M. The prognostic value, sensitivity, and specificity of multiparametric magnetic resonance imaging before salvage radiotherapy for prostate cancer. Radiother. Oncol. 2021, 161, 9–15. [Google Scholar] [CrossRef]
- Sharma, V.; Nehra, A.; Colicchia, M.; Westerman, M.E.; Kawashima, A.; Froemming, A.T.; Kwon, E.D.; Mynderse, L.A.; Karnes, R.J. Multiparametric Magnetic Resonance Imaging Is an Independent Predictor of Salvage Radiotherapy Outcomes After Radical Prostatectomy. Eur. Urol. 2018, 73, 879–887. [Google Scholar] [CrossRef]
- Song, W.; Jeon, H.G.; Sung, H.H.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Choi, H.Y.; Lee, H.M. Prognostic factors after salvage radiotherapy alone in patients with biochemical recurrence after radical prostatectomy. Int. J. Urol. 2016, 23, 56–61. [Google Scholar] [CrossRef]
- Faiella, A.; Sciuto, R.; Giannarelli, D.; Bottero, M.; Farneti, A.; Bertini, L.; Rea, S.; Landoni, V.; Vici, P.; Ferriero, M.C.; et al. A Prospective Study Assessing the Post-Prostatectomy Detection Rate of a Presumed Local Failure at mpMR with Either (64)CuCl2 or (64)CuPSMA PET/CT. Cancers 2021, 13, 5564. [Google Scholar] [CrossRef]
- Kitajima, K.; Murphy, R.C.; Nathan, M.A.; Froemming, A.T.; Hagen, C.E.; Takahashi, N.; Kawashima, A. Detection of recurrent prostate cancer after radical prostatectomy: Comparison of 11C-choline PET/CT with pelvic multiparametric MR imaging with Endorectal coil. J. Nucl. Med. 2014, 55, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Valicenti, R.K.; Thompson, I., Jr.; Albertsen, P.; Davis, B.J.; Goldenberg, S.L.; Wolf, J.S.; Sartor, O.; Klein, E.; Hahn, C.; Michalski, J.; et al. Adjuvant and salvage radiation therapy after prostatectomy: American Society for Radiation Oncology/American Urological Association guidelines. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 822–828. [Google Scholar] [CrossRef]
- Sanguineti, G.; Bertini, L.; Faiella, A.; Ferriero, M.C.; Marzi, S.; Farneti, A.; Landoni, V. Response on DCE-MRI predicts outcome of salvage radiotherapy for local recurrence after radical prostatectomy. Tumori 2021, 107, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Bottero, M.; Faiella, A.; Giannarelli, D.; Farneti, A.; D’Urso, P.; Bertini, L.; Landoni, V.; Vici, P.; Sanguineti, G. A prospective study assessing the pattern of response of local disease at DCE-MRI after salvage radiotherapy for prostate cancer. Clin. Transl. Radiat. Oncol. 2022, 35, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Connolly, J.A.; Shinohara, K.; Presti, J.C., Jr.; Carroll, P.R. Local recurrence after radical prostatectomy: Characteristics in size, location, and relationship to prostate-specific antigen and surgical margins. Urology 1996, 47, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Masi, M.; Landoni, V.; Faiella, A.; Farneti, A.; Marzi, S.; Guerrisi, M.; Sanguineti, G. Comparison of rigid and deformable coregistration between mpMRI and CT images in radiotherapy of prostate bed cancer recurrence. Phys. Med. 2021, 92, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Renard-Penna, R.; Zhang-Yin, J.; Montagne, S.; Aupin, L.; Bruguiere, E.; Labidi, M.; Latorzeff, I.; Hennequin, C. Targeting Local Recurrence After Surgery With MRI Imaging for Prostate Cancer in the Setting of Salvage Radiation Therapy. Front. Oncol. 2022, 12, 775387. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Shariat, S.F.; Zelefsky, M.J.; Kattan, M.W.; Butler, E.B.; Teh, B.S.; Klein, E.A.; Kupelian, P.A.; Roehrborn, C.G.; Pistenmaa, D.A.; et al. Salvage radiotherapy for recurrent prostate cancer after radical prostatectomy. JAMA 2004, 291, 1325–1332. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Schmidt Hegemann, N.S.; Rogowski, P.; Eze, C.; Schafer, C.; Stief, C.; Lang, S.; Spohn, S.; Steffens, R.; Li, M.; Gratzke, C.; et al. Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis. Cancers 2020, 12, 3395. [Google Scholar] [CrossRef]
- Calais, J.; Ceci, F.; Eiber, M.; Hope, T.A.; Hofman, M.S.; Rischpler, C.; Bach-Gansmo, T.; Nanni, C.; Savir-Baruch, B.; Elashoff, D.; et al. (18)F-fluciclovine PET-CT and (68)Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol. 2019, 20, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Giovacchini, G.; Picchio, M.; Garcia-Parra, R.; Briganti, A.; Abdollah, F.; Gianolli, L.; Schindler, C.; Montorsi, F.; Messa, C.; Fazio, F. 11C-choline PET/CT predicts prostate cancer-specific survival in patients with biochemical failure during androgen-deprivation therapy. J. Nucl. Med. 2014, 55, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Emmett, L.; Hruby, G. Clinical impact of PET imaging in prostate cancer management. Curr. Opin. Urol. 2020, 30, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Dundee, P.; Furrer, M.A.; Corcoran, N.M.; Peters, J.; Pan, H.; Ballok, Z.; Ryan, A.; Guerrieri, M.; Costello, A.J. Defining Prostatic Vascular Pedicle Recurrence and the Anatomy of Local Recurrence of Prostate Cancer on Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography. Eur. Urol. Open Sci. 2022, 41, 116–122. [Google Scholar] [CrossRef]
- Ceci, F.; Bianchi, L.; Borghesi, M.; Polverari, G.; Farolfi, A.; Briganti, A.; Schiavina, R.; Brunocilla, E.; Castellucci, P.; Fanti, S. Prediction nomogram for (68)Ga-PSMA-11 PET/CT in different clinical settings of PSA failure after radical treatment for prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 136–146. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Stratification | Median/# | IQR/% |
|---|---|---|---|
| Age | Continuum | 69.4 | 66–75 |
| pT stage at RP | 2 | 135 | 57.2 |
| 3a | 84 | 35.6 | |
| 3b | 17 | 7.2 | |
| pN stage at RP | pN0 | 136 | 57.6 |
| pNx | 100 | 42.4 | |
| Surgical margins at RP | 0 | 117 | 49.6 |
| 1 | 115 | 48.7 | |
| Missing | 4 | 1.7 | |
| ISUP category at RP | 1 | 20 | 8.5 |
| 2 | 115 | 48.7 | |
| 3 | 71 | 30.1 | |
| 4 | 16 | 6.8 | |
| 5 | 14 | 5.9 | |
| Detectable PSA after RP | No | 214 | 90.7% |
| Yes | 22 | 9.3% | |
| Time from RP to sRT (mths) | Continuum | 44.9 | 19.9–84.1 |
| PSA at RP (ng/mL) | Continuum | 7.2 | 5.3–10.0 |
| Pre sRT PSA (ng/mL) | Continuum | 0.51 | 0.35–0.96 |
| PSADT (mths) | Continuum | 10.8 | 4.5–20.1 |
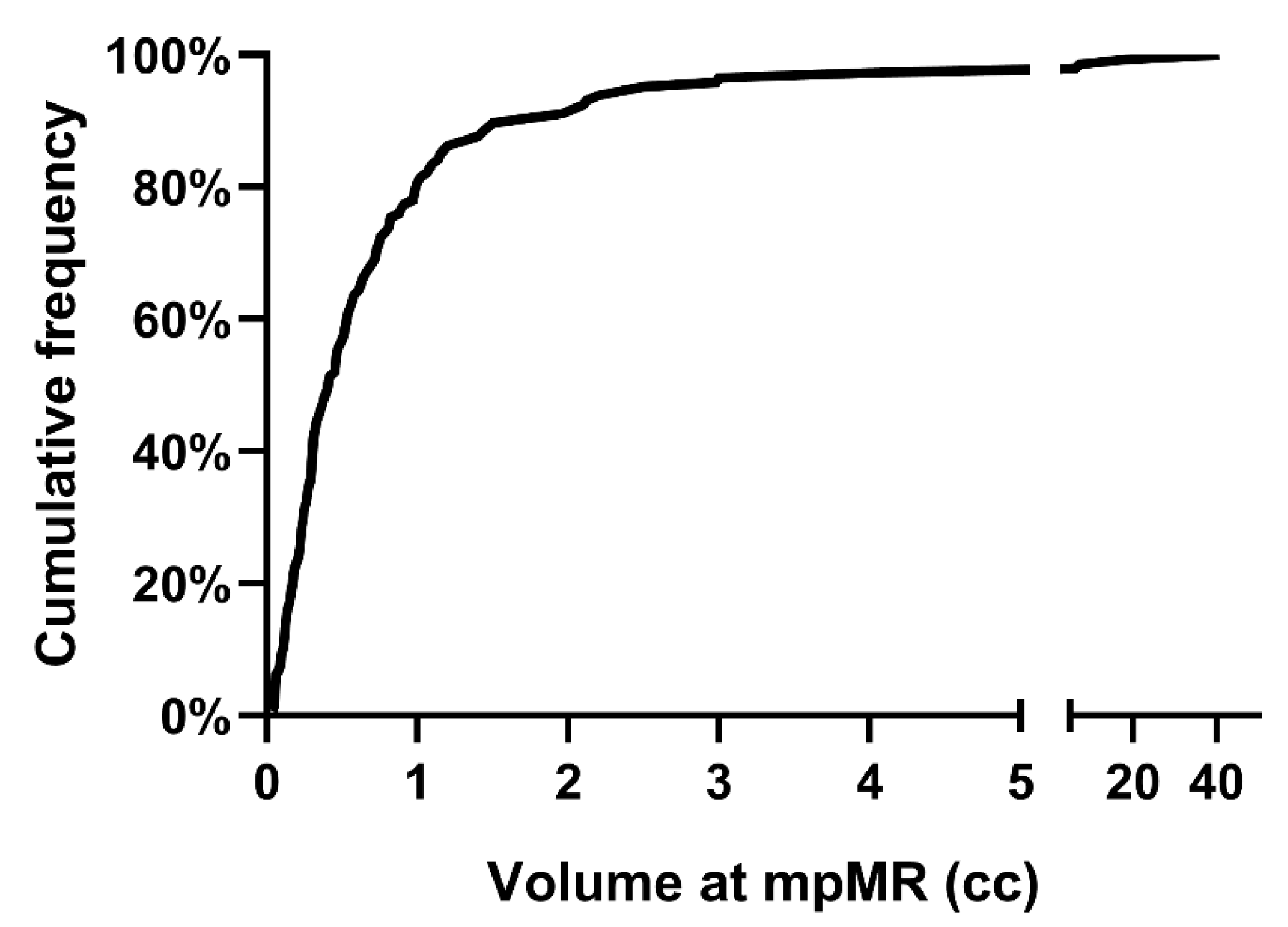
| Macro tumor load (cc) per pt | Continuum | 0.41 | 0.22–0.83 |
| # Lesions | 0 | 90 | 38.1 |
| 1 | 125 | 53.0 | |
| 2 | 20 | 8.5 | |
| 3 | 1 | 0.4 | |
| Involved subsites @ DCE-MRI | VUA | 85 | 36% |
| BN | 39 | 16.5% | |
| RV | 34 | 14.4% | |
| DCE-MRI findings | Negative | 90 | 38.1% |
| Positive | 146 | 61.9% | |
| DCE-MRI | In-house | 191 | 80.9% |
| Outside Institution | 45 | 19.1% | |
| PET/CT | Choline only | 144 | 61.0% |
| Cu/PSMA ± Choline | 92 | 39.0% | |
| WPRT | No | 86 | 36.4% |
| Yes | 150 | 63.6% | |
| EAU risk | Low | 88 | 37.3% |
| High | 144 | 61.0% | |
| Androgen Deprivation | None | 211 | 89.4% |
| Any | 25 | 10.6% | |
| Dose to the prostatic fossa | 66 Gy | 40 | 16.9% |
| 69 Gy | 196 | 83.1% |
| Positive vs. Negative DCE-MRI | Disease Location at DCE-MRI | ||||||
|---|---|---|---|---|---|---|---|
| Covariate | Stratification | HR | 95%CI | p Value | HR | 95%CI | p Value |
| SVI at RP | No | 1 | 1 | ||||
| Yes | 2.84 | 1.18–6.84 | 0.020 | 2.44 | 0.99–5.96 | 0.051 | |
| DCE-MRI status | Negative | 1 | |||||
| Positive | 0.52 | 0.29–0.95 | 0.035 | ||||
| Location at DCE-MRI | None | 1 | |||||
| VUA only | 0.34 | 0.15–0.77 | 0.010 | ||||
| BN/RV ± VUA | 0.73 | 0.37–1.42 | 0.319 | ||||
| Total Volume (cc) | Continuum | 1.06 | 1.02–1.11 | 0.006 | 1.07 | 1.02–1.12 | 0.003 |
| EAU risk | Low | 1 | 1 | ||||
| High | 2.03 | 0.99–4.16 | 0.052 | 2.06 | 1.01–4.21 | 0.048 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farneti, A.; Bottero, M.; Faiella, A.; Giannarelli, D.; Bertini, L.; Landoni, V.; Vici, P.; D’Urso, P.; Sanguineti, G. The Prognostic Value of DCE-MRI Findings before Salvage Radiotherapy after Radical Prostatectomy. Cancers 2023, 15, 1246. https://doi.org/10.3390/cancers15041246
Farneti A, Bottero M, Faiella A, Giannarelli D, Bertini L, Landoni V, Vici P, D’Urso P, Sanguineti G. The Prognostic Value of DCE-MRI Findings before Salvage Radiotherapy after Radical Prostatectomy. Cancers. 2023; 15(4):1246. https://doi.org/10.3390/cancers15041246
Chicago/Turabian StyleFarneti, Alessia, Marta Bottero, Adriana Faiella, Diana Giannarelli, Luca Bertini, Valeria Landoni, Patrizia Vici, Pasqualina D’Urso, and Giuseppe Sanguineti. 2023. "The Prognostic Value of DCE-MRI Findings before Salvage Radiotherapy after Radical Prostatectomy" Cancers 15, no. 4: 1246. https://doi.org/10.3390/cancers15041246
APA StyleFarneti, A., Bottero, M., Faiella, A., Giannarelli, D., Bertini, L., Landoni, V., Vici, P., D’Urso, P., & Sanguineti, G. (2023). The Prognostic Value of DCE-MRI Findings before Salvage Radiotherapy after Radical Prostatectomy. Cancers, 15(4), 1246. https://doi.org/10.3390/cancers15041246