
Bevacizumab as Single Agent in Children and Teenagers with Optic Pathway Glioma

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
1.1. Pediatric Low-Grade Glioma and Optic Pathway Glioma (OPG)
1.2. Management of OPG
1.3. Angiogenesis and Bevacizumab Rationale in OPG
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Imaging Assessment
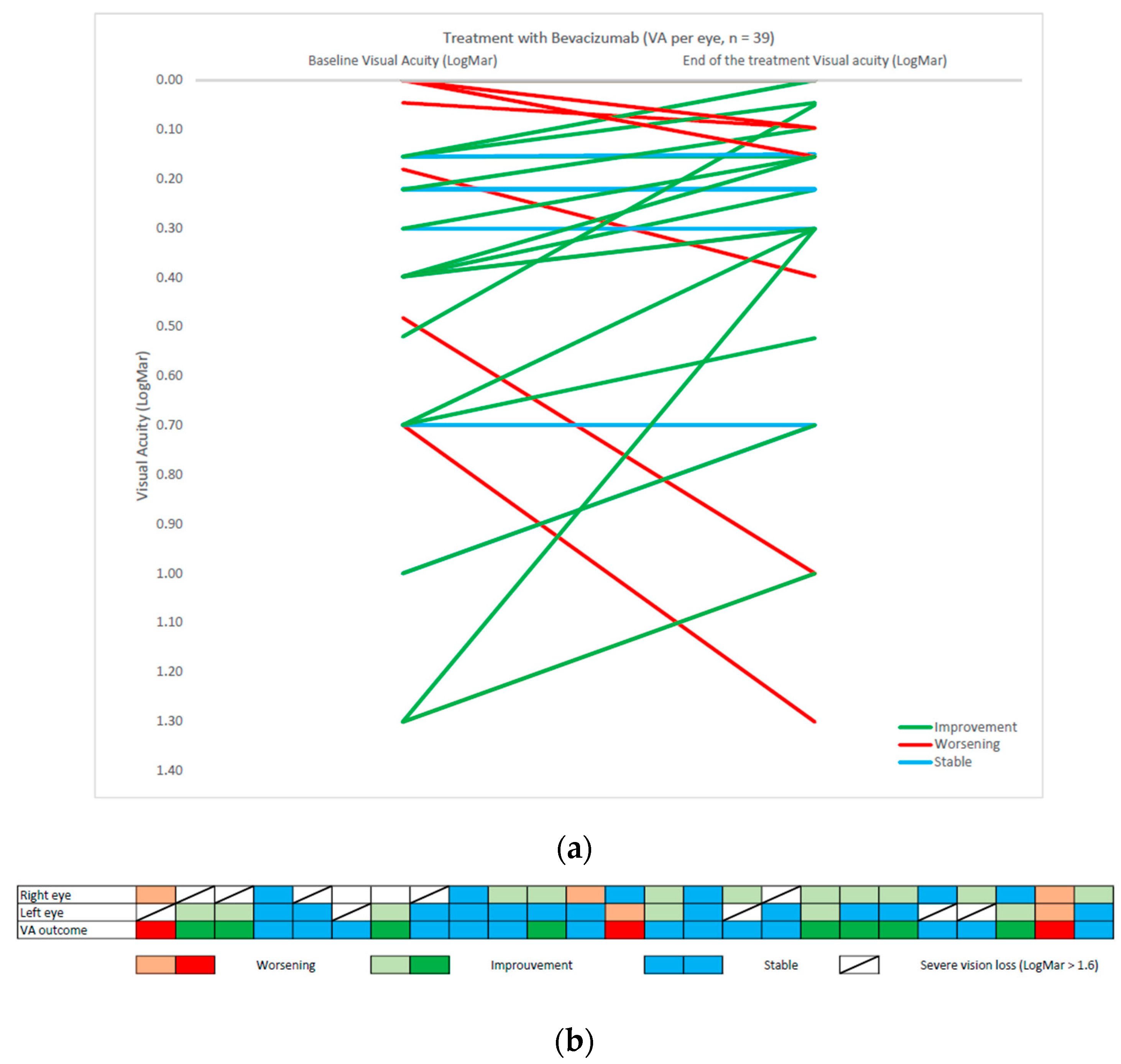
3.2. Visual Assessment
3.3. Correlation between Radiological and Ophtalmological Response and NF1 Patients
3.4. Treatment Tolerance and Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Blank, P.; Bandopadhayay, P.; Haas-Kogan, D.; Fouladi, M.; Fangusaro, J. Management of pediatric low-grade glioma. Curr. Opin. Pediatr. 2019, 31, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.; Weller, R.O. WHO Classification of Tumours of the Central Nervous System. Available online: https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/WHO-Classification-Of-Tumours-Of-The-Central-Nervous-System-2016 (accessed on 30 September 2021).
- Farazdaghi, M.K.; Katowitz, W.R.; Avery, R.A. Current treatment of optic nerve gliomas. Curr. Opin. Ophthalmol. 2019, 30, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Listernick, R.; Charrow, J.; Greenwald, M.; Mets, M. Natural history of optic pathway tumors in children with neurofibromatosis type 1: A longitudinal study. J. Pediatr. 1994, 125, 63–66. [Google Scholar] [CrossRef]
- Tenny, R.T.; Laws, E.R.; Younge, B.R.; Rush, J.A. The neurosurgical management of optic glioma. J. Neurosurg. 1982, 57, 452–458. [Google Scholar] [CrossRef]
- Beneš, V.; Julisova, I.; Julis, I. Our treatment philosophy of gliomas of the anterior visual pathways. Child’s Nerv. Syst. 1990, 6, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.A.; Liu, J.; Kieran, M.; Jabado, N.; Picton, S.; Packer, R.; Rose, C.S.; Van Meeteren, A.S.; Carvalho, A.; Van Damme, A.; et al. A multi-disciplinary consensus statement concerning surgical approaches to low-grade, high-grade astrocytomas and diffuse intrinsic pontine gliomas in childhood (CPN Paris 2011) using the Delphi method. Neuro-Oncology 2013, 15, 462–468. [Google Scholar] [CrossRef]
- Robert-Boire, V.; Rosca, L.; Samson, Y.; Ospina, L.H.; Perreault, S. Clinical Presentation and Outcome of Patients with Optic Pathway Glioma. Pediatr. Neurol. 2017, 75, 55–60. [Google Scholar] [CrossRef]
- Fried, I.; Tabori, U.; Tihan, T.; Reginald, A.; Bouffet, E. Optic pathway gliomas: A review. CNS Oncol. 2013, 2, 143–159. [Google Scholar] [CrossRef]
- Wan, M.J.; Ullrich, N.J.; Manley, P.E.; Kieran, M.W.; Goumnerova, L.C.; Heidary, G. Long-term visual outcomes of optic pathway gliomas in pediatric patients without neurofibromatosis type 1. J. Neuro-Oncol. 2016, 129, 173–178. [Google Scholar] [CrossRef]
- Kollias, S.S.; Barkovich, J.; Edwards, M.S. Magnetic Resonance Analysis of Suprasellar Tumors of Childhood. Pediatr. Neurosurg. 1991, 17, 284–303. [Google Scholar] [CrossRef]
- Ryall, S.; Zapotocky, M.; Fukuoka, K.; Nobre, L.; Stucklin, A.G.; Bennett, J.; Siddaway, R.; Li, C.; Pajovic, S.; Arnoldo, A.; et al. Integrated Molecular and Clinical Analysis of 1,000 Pediatric Low-Grade Gliomas. Cancer Cell 2020, 37, 569–583.e5. [Google Scholar] [CrossRef]
- Mueller, S.; Fullerton, H.; Stratton, K.; Leisenring, W.; Weathers, R.E.; Stovall, M.; Armstrong, G.T.; Goldsby, R.E.; Packer, R.J.; Sklar, C.A.; et al. Radiation, Atherosclerotic Risk Factors, and Stroke Risk in Survivors of Pediatric Cancer: A Report from the Childhood Cancer Survivor Study. Int. J. Radiat. Oncol. 2013, 86, 649–655. [Google Scholar] [CrossRef]
- Lassaletta, A.; Scheinemann, K.; Zelcer, S.M.; Hukin, J.; Wilson, B.A.; Jabado, N.; Carret, A.S.; Lafay-Cousin, L.; Larouche, V.; Hawkins, C.E.; et al. Phase II Weekly Vinblastine for Chemotherapy-Naïve Children with Progressive Low-Grade Glioma: A Canadian Pediatric Brain Tumor Consortium Study. J. Clin. Oncol. 2016, 34, 3537–3543. [Google Scholar] [CrossRef] [PubMed]
- Gnekow, A.K.; Walker, D.A.; Kandels, D.; Picton, S.; Perilongo, G.; Grill, J.; Stokland, T.; Sandstrom, P.E.; Warmuth-Metz, M.; Pietsch, T.; et al. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤16 years) low grade glioma—A final report. Eur. J. Cancer 2017, 81, 206–225. [Google Scholar] [CrossRef]
- Ater, J.L.; Zhou, T.; Holmes, E.; Mazewski, C.M.; Booth, T.N.; Freyer, D.R.; Lazarus, K.H.; Packer, R.J.; Prados, M.; Sposto, R.; et al. Randomized Study of Two Chemotherapy Regimens for Treatment of Low-Grade Glioma in Young Children: A Report from the Children’s Oncology Group. J. Clin. Oncol. 2012, 30, 2641–2647. [Google Scholar] [CrossRef]
- Falzon, K.; Drimtzias, E.; Picton, S.; Simmons, I. Visual outcomes after chemotherapy for optic pathway glioma in children with and without neurofibromatosis type 1: Results of the International Society of Paediatric Oncology (SIOP) Low-Grade Glioma 2004 trial UK cohort. Br. J. Ophthalmol. 2018, 102, 1367–1371. [Google Scholar] [CrossRef]
- A Azizi, A.; A Walker, D.; Liu, J.-F.; Sehested, A.; Jaspan, T.; Pemp, B.; Simmons, I.; Ferner, R.; Grill, J.; Hargrave, D.; et al. NF1 optic pathway glioma: Analyzing risk factors for visual outcome and indications to treat. Neuro-Oncology 2020, 23, 100–111. [Google Scholar] [CrossRef]
- Packer, R.J.; Pfister, S.; Bouffet, E.; Avery, R.; Bandopadhayay, P.; Bornhorst, M.; Bowers, D.; Ellison, D.; Fangusaro, J.; Foreman, N.; et al. Pediatric low-grade gliomas: Implications of the biologic era. Neuro-Oncology 2016, 19, 750–761. [Google Scholar] [CrossRef]
- Banerjee, A.; Jakacki, R.I.; Onar-Thomas, A.; Wu, S.; Nicolaides, T.; Poussaint, T.Y.; Fangusaro, J.; Phillips, J.; Perry, A.; Turner, D.; et al. A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: A Pediatric Brain Tumor Consortium (PBTC) study. Neuro-Oncology 2017, 19, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Zhukova, N.; Rajagopal, R.; Lam, A.; Coleman, L.; Shipman, P.; Walwyn, T.; Williams, M.; Sullivan, M.; Campbell, M.; Bhatia, K.; et al. Use of bevacizumab as a single agent or in adjunct with traditional chemotherapy regimens in children with unresectable or progressive low-grade glioma. Cancer Med. 2018, 8, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Seyedmirzaei, H.; Shobeiri, P.; Turgut, M.; Hanaei, S.; Rezaei, N. VEGF levels in patients with glioma: A systematic review and meta-analysis. Rev. Neurosci. 2020, 32, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Chen, J.; Ferraro, G.B.; Wu, L.; Datta, M.; Jain, R.K.; Plotkin, S.R.; Stemmer-Rachamimov, A.; Xu, L. Anti-VEGF treatment improves neurological function in tumors of the nervous system. Exp. Neurol. 2017, 299, 326–333. [Google Scholar] [CrossRef]
- Packer, R.J.; Jakacki, R.; Horn, M.; Rood, B.; Vezina, G.; MacDonald, T.; Fisher, M.J.; Cohen, B. Objective response of multiply recurrent low-grade gliomas to bevacizumab and irinotecan. Pediatr. Blood Cancer 2009, 52, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Gururangan, S.; Fangusaro, J.; Poussaint, T.Y.; McLendon, R.E.; Onar-Thomas, A.; Wu, S.; Packer, R.J.; Banerjee, A.; Gilbertson, R.J.; Fahey, F.; et al. Efficacy of bevacizumab plus irinotecan in children with recurrent low-grade gliomas—A Pediatric Brain Tumor Consortium study. Neuro-Oncology 2013, 16, 310–317. [Google Scholar] [CrossRef]
- Kalra, M.; Heath, J.A.; Kellie, S.J.; Pozza, L.D.; Stevens, M.M.; Swamy, S.; McCowage, G.B. Confirmation of Bevacizumab Activity, and Maintenance of Efficacy in Retreatment After Subsequent Relapse, in Pediatric Low-grade Glioma. J. Pediatr. Hematol. 2015, 37, e341–e346. [Google Scholar] [CrossRef]
- Vredenburgh, J.J.; Desjardins, A.; Reardon, D.A.; Friedman, H.S. Experience with irinotecan for the treatment of malignant glioma. Neuro-Oncology 2009, 11, 80–91. [Google Scholar] [CrossRef]
- Hwang, E.I.; Jakacki, R.I.; Fisher, M.J.; Kilburn, L.B.; Horn, M.; Vezina, G.; Rood, B.R.; Packer, R.J. Long-term efficacy and toxicity of bevacizumab-based therapy in children with recurrent low-grade gliomas. Pediatr. Blood Cancer 2012, 60, 776–782. [Google Scholar] [CrossRef]
- Fangusaro, J.; Witt, O.; Driever, P.H.; Bag, A.K.; de Blank, P.; Kadom, N.; Kilburn, L.; Lober, R.M.; Robison, N.J.; Fisher, M.J.; et al. Response assessment in paediatric low-grade glioma: Recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) working group. Lancet Oncol. 2020, 21, e305–e316. [Google Scholar] [CrossRef]
- Chukwueke, U.N.; Wen, P.Y. Use of the Response Assessment in Neuro-Oncology (RANO) criteria in clinical trials and clinical practice. CNS Oncol. 2019, 8, CNS28. [Google Scholar] [CrossRef]
- Daiber, H.F.; Gnugnoli, D.M. Visual Acuity. In Treasure Island; StatPearls Publishing: Tampa/St. Petersburg, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/NBK563298/ (accessed on 5 November 2022).
- Fisher, M.J.; Avery, R.A.; Allen, J.C.; Ardern-Holmes, S.L.; Bilaniuk, L.T.; Ferner, R.E.; Gutmann, D.H.; Listernick, R.; Martin, S.; Ullrich, N.J.; et al. Functional outcome measures for NF1-associated optic pathway glioma clinical trials. Neurology 2013, 81, S15–S24. [Google Scholar] [CrossRef] [PubMed]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. CTCAE versión 5.0. Evaluación de la gravedad de los eventos adversos dermatológicos de las terapias antineoplásicas. Actas Dermo-Sifiliográficas 2020, 112, 90–92. [Google Scholar] [CrossRef]
- Levenbaum, E.; Ellika, S.; Korones, D.N. Bevacizumab in treating the cystic components of pediatric low-grade gliomas: A report of four patients. Pediatr. Blood Cancer 2019, 66, e27917. [Google Scholar] [CrossRef]
- Avery, R.A.; Hwang, E.I.; Jakacki, R.I.; Packer, R.J. Marked Recovery of Vision in Children with Optic Pathway Gliomas Treated With Bevacizumab. JAMA Ophthalmol. 2014, 132, 111–114. [Google Scholar] [CrossRef]
- de Marcellus, C.; Tauziède-Espariat, A.; Cuinet, A.; Pasqualini, C.; Robert, M.P.; Beccaria, K.; Puget, S.; Boddaert, N.; Figarella-Branger, D.; De Carli, E.; et al. The role of irinotecan-bevacizumab as rescue regimen in children with low-grade gliomas: A retrospective nationwide study in 72 patients. J. Neuro-Oncol. 2022, 157, 355–364. [Google Scholar] [CrossRef]
- Heng, M.A.; Padovani, L.; Dory-Lautrec, P.; Gentet, J.C.; Verschuur, A.; Pasquier, E.; Figarella-Branger, D.; Scavarda, D.; André, N. Can metronomic maintenance with weekly vinblastine prevent early relapse/progression after bevacizumab–irinotecan in children with low-grade glioma? Cancer Med. 2016, 5, 1542–1545. [Google Scholar] [CrossRef]
- Lu, V.M.; Welby, J.P.; Nesvick, C.L.; Daniels, D.J. Efficacy and safety of bevacizumab in progressive pediatric low-grade glioma: A systematic review and meta-analysis of outcome rates. Neuro-Oncol. Pr. 2020, 7, 359–368. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Characteristics | No. of Patients |
|---|---|
| Total number of patients | 31 |
| Median age at diagnosis (range) | 3.8 years (0.3–19.0 y) |
| Median age at first bevacizumab dose (range) | 4.9 years (0.3–19.0 y) |
| No. of patients with NF1 | 11 (35%) |
| Histology | 17 patients (57%) |
| Pilocytic astrocytoma | 16 (52%) |
| Ganglioglioma | 1 (3%) |
| Prior chemotherapy | 11/31 (35%) |
| Weekly vinblastine | 4 (36%) |
| SIOP LGG 2004(vincristine—carboplatine) | 3 (28%) |
| Both chemotherapy protocols | 4 (36%) |
| Radiological Response | 3-Month Evaluation | Best Anytime Response |
|---|---|---|
| Complete response | 0 (0%) | 0 (0%) |
| Major response | 1 (3%) | 1 (3%) |
| Partial response | 3 (10%) | 6 (21%) |
| Stable disease | 18 (62%) | 14 (48%) |
| Minor response | 6 (21%) | 7 (24%) |
| Progressive disease | 1 (3%) | 1 (3%) |
| Clinical Characteristics at Start of Treatment | No |
|---|---|
| Visual acuity evaluable (n = patients) | 25 |
| Monolateral blindness (n = eye) | 10 |
| Median (LogMar) | 0.26 (−0.08–1.30) |
| Optic disk atrophy at fundoscopy (n = patients) | 11 |
| Clinical characteristics after bevacizumab treatment | No |
| visual acuity evaluable (n = patients) | 25 |
| Monolateral blindness (n = eye) | 9 |
| Median (LogMar) at the end of treatment | 0.22 (−0.08–1.30) |
| Median (LogMar) at best moment | 0.15 (−0.08–1.30) |
| Optic disk atrophy at fundoscopy (n = patients) | 11 |
| Change in Visual Acuity (VA) | No of patients (Percentage) |
| Significant improvement (>0.2 LogMAR) | 8 (32%) |
| Steady state (change within 0.2 LogMAR) | 14 (56%) |
| Significant worsening (<0.2 LogMAR) | 3 (14%) |
| Change in Visual Field (VF) | No of patients (Percentage) |
| Improvement | 3 (25%) |
| Steady state | 7 (59%) |
| Worsening | 2 (17%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calò, P.; Pianton, N.; Basle, A.; Vasiljevic, A.; Barritault, M.; Beuriat, P.A.; Faure-Conter, C.; Leblond, P. Bevacizumab as Single Agent in Children and Teenagers with Optic Pathway Glioma. Cancers 2023, 15, 1036. https://doi.org/10.3390/cancers15041036
Calò P, Pianton N, Basle A, Vasiljevic A, Barritault M, Beuriat PA, Faure-Conter C, Leblond P. Bevacizumab as Single Agent in Children and Teenagers with Optic Pathway Glioma. Cancers. 2023; 15(4):1036. https://doi.org/10.3390/cancers15041036
Chicago/Turabian StyleCalò, Pierluigi, Nicolas Pianton, Alexandre Basle, Alexandre Vasiljevic, Marc Barritault, Pierre Aurélien Beuriat, Cécile Faure-Conter, and Pierre Leblond. 2023. "Bevacizumab as Single Agent in Children and Teenagers with Optic Pathway Glioma" Cancers 15, no. 4: 1036. https://doi.org/10.3390/cancers15041036
APA StyleCalò, P., Pianton, N., Basle, A., Vasiljevic, A., Barritault, M., Beuriat, P. A., Faure-Conter, C., & Leblond, P. (2023). Bevacizumab as Single Agent in Children and Teenagers with Optic Pathway Glioma. Cancers, 15(4), 1036. https://doi.org/10.3390/cancers15041036