
The Role of Branched-Chain Amino Acid Supplementation in Combination with Locoregional Treatments for Hepatocellular Carcinoma: Systematic Review and Meta-Analysis


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search Strategy
2.3. Data Collection and Extraction
2.4. Assessment of Study Quality
2.5. Statistical Analysis
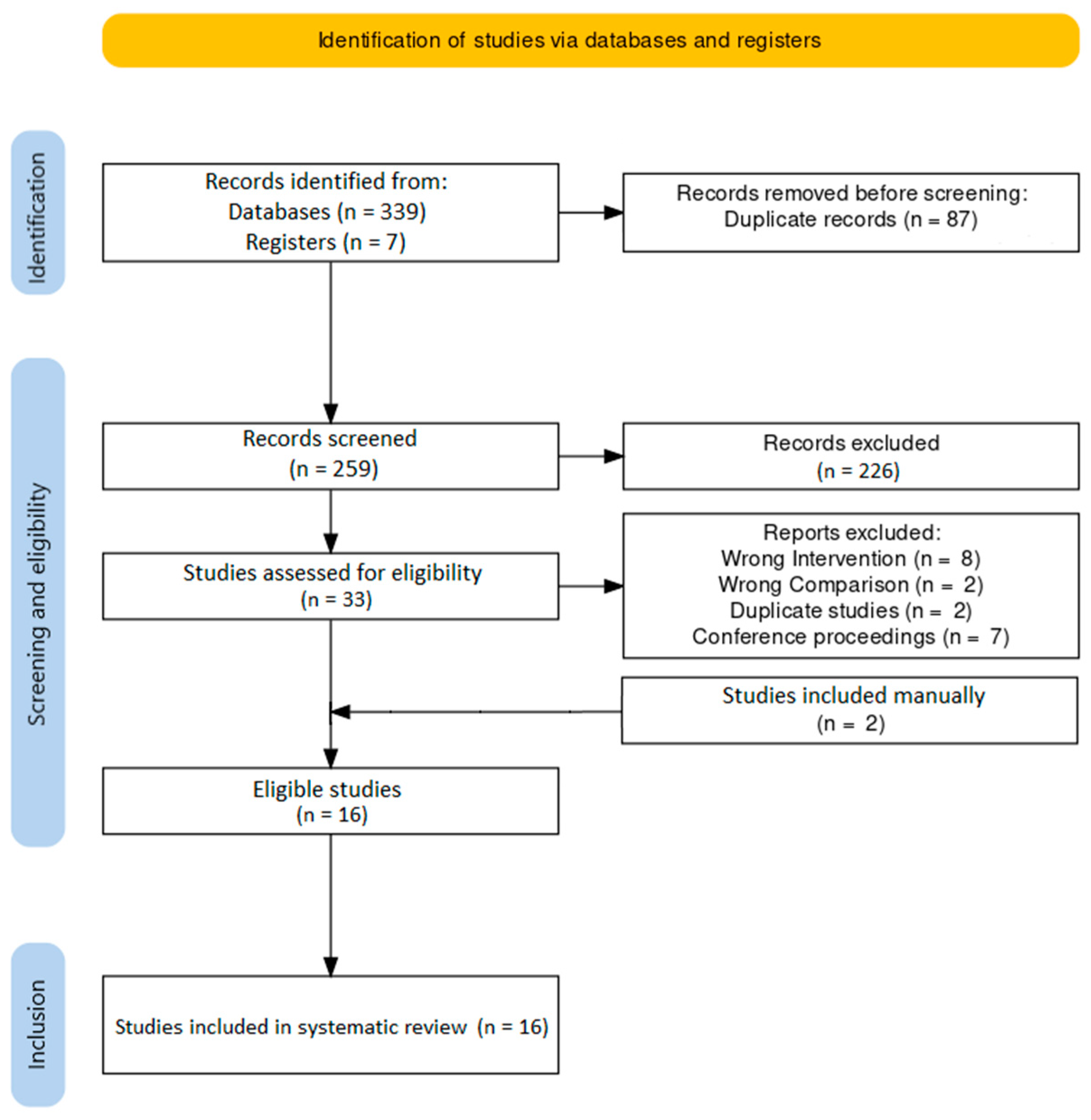
3. Results
3.1. Study Characteristics
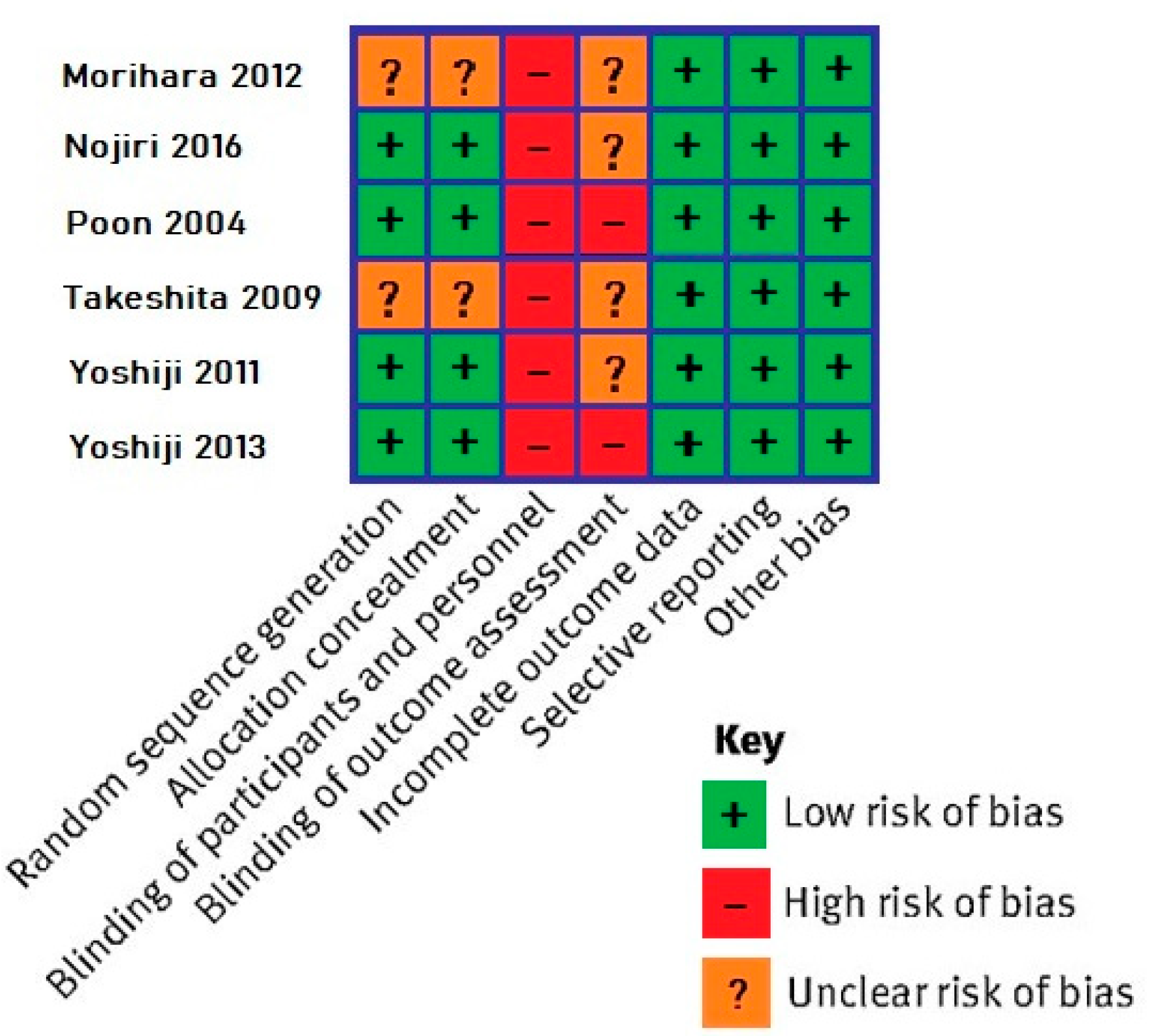
3.2. Quality of Evidence Assessment
3.3. Baseline Patient Characteristics
3.4. Baseline Laboratory Values
3.5. Locoregional Treatments
3.6. BCAA Supplements
3.7. Follow-Up Time
3.8. Overall Survival (OS)
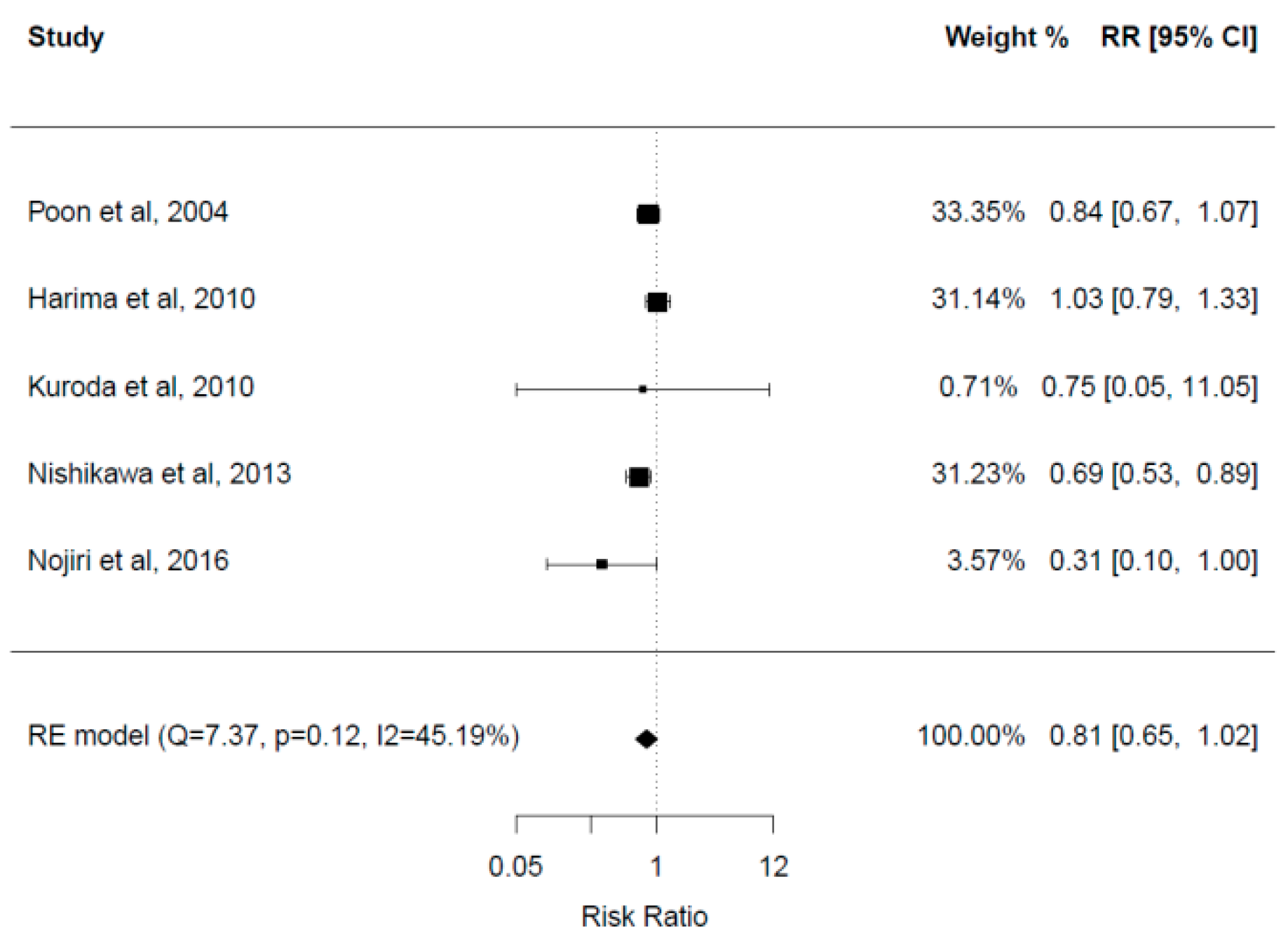
3.9. Mortality Rate
3.10. Recurrence-Free Survival (RFS)
3.11. Recurrence Rate
3.12. Event-Free Survival (EFS)
3.13. Overall Events/Complications
3.14. Child-Pugh Score
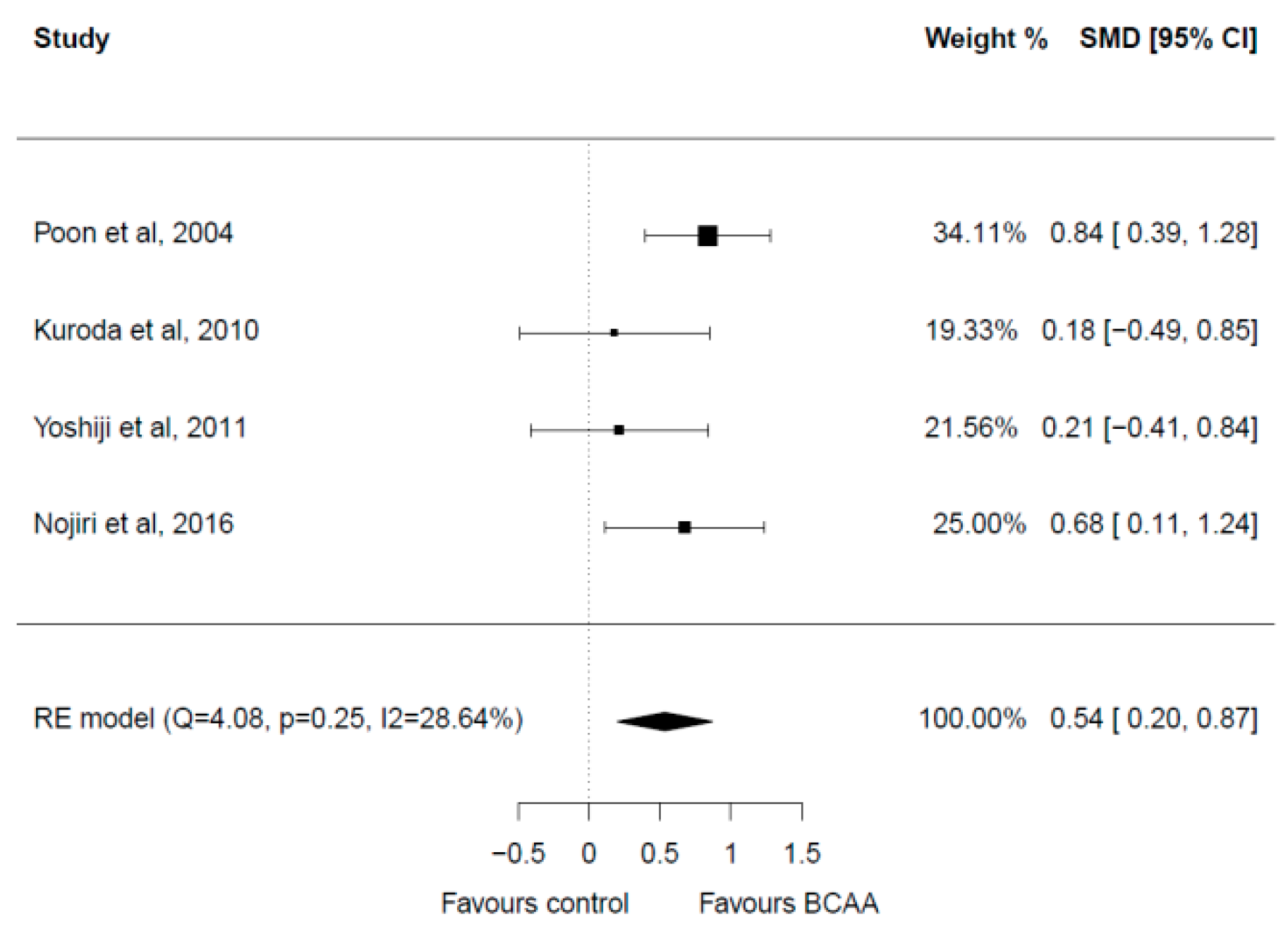
3.15. Albumin
3.16. AST and ALT
3.17. Ammonia
3.18. TBil
3.19. PT
3.20. BTR
3.21. Other Laboratory Values
3.22. Quality of Life and Sarcopenia Indices
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ye, F.; Zhai, M.; Long, J.; Gong, Y.; Ren, C.; Zhang, D.; Lin, X.; Liu, S. The burden of liver cirrhosis in mortality: Results from the global burden of disease study. Front. Public Health 2022, 10, 909455. [Google Scholar] [CrossRef] [PubMed]
- Chronic Liver Disease and Cirrhosis. CDC/National Center for Health Statistics. January 2022. Available online: https://www.cdc.gov/nchs/fastats/liver-disease.htm (accessed on 20 August 2022).
- Cirrhosis Collaborators, G. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef]
- Cheemerla, S.; Balakrishnan, M. Global Epidemiology of Chronic Liver Disease. Clin. Liver Dis. 2021, 17, 365–370. [Google Scholar] [CrossRef]
- Poh, Z.; Goh, B.B.; Chang, P.E.; Tan, C.K. Rates of cirrhosis and hepatocellular carcinoma in chronic hepatitis B and the role of surveillance: A 10-year follow-up of 673 patients. Eur. J. Gastroenterol. Hepatol. 2015, 27, 638–643. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. 1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Izumi, N.; Charlton, M.R.; Sata, M. Branched-chain amino acids as pharmacological nutrients in chronic liver disease. Hepatology 2011, 54, 1063–1070. [Google Scholar] [CrossRef]
- Holeček, M. Branched-chain amino acids in health and disease: Metabolism, alterations in blood plasma, and as supplements. Nutr. Metab. 2018, 15, 33. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Aly, A.; Ronnebaum, S.; Patel, D.; Doleh, Y.; Benavente, F. Epidemiologic, humanistic and economic burden of hepatocellular carcinoma in the USA: A systematic literature review. Hepat. Oncol. 2020, 7, Hep27. [Google Scholar] [CrossRef]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491.e1. [Google Scholar] [CrossRef]
- Song, M.J. Hepatic artery infusion chemotherapy for advanced hepatocellular carcinoma. World J. Gastroenterol. 2015, 21, 3843–3849. [Google Scholar] [CrossRef] [PubMed]
- Kohla, M.A.; Abu Zeid, M.I.; Al-Warraky, M.; Taha, H.; Gish, R.G. Predictors of hepatic decompensation after TACE for hepatocellular carcinoma. BMJ Open Gastroenterol. 2015, 2, e000032. [Google Scholar] [CrossRef] [PubMed]
- Okabayashi, T.; Nishimori, I.; Sugimoto, T.; Iwasaki, S.; Akisawa, N.; Maeda, H.; Ito, S.; Onishi, S.; Ogawa, Y.; Kobayashi, M.; et al. The benefit of the supplementation of perioperative branched-chain amino acids in patients with surgical management for hepatocellular carcinoma: A preliminary study. Dig. Dis. Sci. 2008, 53, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Takeda, H.; Nishikawa, H.; Iguchi, E.; Ohara, Y.; Sakamoto, A.; Saito, S.; Nishijima, N.; Nasu, A.; Komekado, H.; Kita, R.; et al. Effect of treatment with branched-chain amino acids during sorafenib therapy for unresectable hepatocellular carcinoma. Hepatol. Res. 2014, 44, 302–312. [Google Scholar] [CrossRef]
- Imanaka, K.; Ohkawa, K.; Tatsumi, T.; Katayama, K.; Inoue, A.; Imai, Y.; Oshita, M.; Iio, S.; Mita, E.; Fukui, H.; et al. Impact of branched-chain amino acid supplementation on survival in patients with advanced hepatocellular carcinoma treated with sorafenib: A multicenter retrospective cohort study. Hepatol. Res. 2016, 46, 1002–1010. [Google Scholar] [CrossRef]
- Lee, I.J.; Seong, J.; Bae, J.I.; You, S.H.; Rhee, Y.; Lee, J.H. Effect of Oral Supplementation with Branched-chain Amino Acid (BCAA) during Radiotherapy in Patients with Hepatocellular Carcinoma: A Double-Blind Randomized Study. Cancer Res. Treat. 2011, 43, 24–31. [Google Scholar] [CrossRef]
- Chen, L.; Chen, Y.; Wang, X.; Li, H.; Zhang, H.; Gong, J.; Shen, S.; Yin, W.; Hu, H. Efficacy and safety of oral branched-chain amino acid supplementation in patients undergoing interventions for hepatocellular carcinoma: A meta-analysis. Nutr. J. 2015, 14, 67. [Google Scholar] [CrossRef]
- Xue, W.X.; Yang, F.; Duan, J.J.; Sun, J.B.; Peng, H. Effect of oral administration of branched-chain amino acids supplementation on the mortality of patients with hepatocellular carcinoma: A meta-analysis. Zhonghua Yi Xue Za Zhi 2020, 100, 3793–3800. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Harima, Y.; Yamasaki, T.; Hamabe, S.; Saeki, I.; Okita, K.; Terai, S.; Sakaida, I. Effect of a late evening snack using branched-chain amino acid-enriched nutrients in patients undergoing hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma. Hepatol. Res. 2010, 40, 574–584. [Google Scholar] [CrossRef]
- Ishihara, T.; Iwasa, M.; Tanaka, H.; Kaito, M.; Ikoma, J.; Shibata, T.; Takei, Y. Effect of branched-chain amino acids in patients receiving intervention for hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 2673–2680. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Michitaka, I.; Kamimura, H.; Higuchi, K.; Kubota, T.; Seki, K.I.; Ohta, H.; Yoshida, T.; Kamimura, T. Oral branched-chain amino acids administration improves impaired liver dysfunction after radiofrequency ablation therapy for hepatocellular carcinoma. Hepato-Gastroenterol. 2009, 56, 1491–1495. [Google Scholar]
- Iwasa, M.; Sugimoto, R.; Ishihara, T.; Sekoguchi-Fujikawa, N.; Yoshikawa, K.; Mifuji-Moroka, R.; Tanaka, H.; Kobayashi, Y.; Hasegawa, H.; Takei, Y. Usefulness of levocarnitine and/or branched-chain amino acids during invasive treatment for hepatocellular carcinoma. J. Nutr. Sci. Vitaminol. 2015, 61, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Kanekawa, T.; Nagai, H.; Kanayama, M.; Sumino, Y. Importance of branched-chain amino acids in patients with liver cirrhosis and advanced hepatocellular carcinoma receiving hepatic arterial infusion chemotherapy. Cancer Chemother. Pharmacol. 2014, 74, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, H.; Ushio, A.; Miyamoto, Y.; Sawara, K.; Oikawa, K.; Kasai, K.; Endo, R.; Takikawa, Y.; Kato, A.; Suzuki, K. Effects of branched-chain amino acid-enriched nutrient for patients with hepatocellular carcinoma following radiofrequency ablation: A one-year prospective trial. J. Gastroenterol. Hepatol. 2010, 25, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Morihara, D.; Iwata, K.; Hanano, T.; Kunimoto, H.; Kuno, S.; Fukunaga, A.; Yotsumoto, K.; Takata, K.; Tanaka, T.; Sakurai, K.; et al. Late-evening snack with branched-chain amino acids improves liver function after radiofrequency ablation for hepatocellular carcinoma. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2012, 42, 658–667. [Google Scholar] [CrossRef]
- Nishikawa, H.; Osaki, Y.; Inuzuka, T.; Takeda, H.; Nakajima, J.; Matsuda, F.; Henmi, S.; Sakamoto, A.; Ishikawa, T.; Saito, S.; et al. Branched-chain amino acid treatment before transcatheter arterial chemoembolization for hepatocellular carcinoma. World J. Gastroenterol. 2012, 18, 1379–1384. [Google Scholar] [CrossRef]
- Nishikawa, H.; Osaki, Y.; Iguchi, E.; Koshikawa, Y.; Ako, S.; Inuzuka, T.; Takeda, H.; Nakajima, J.; Matsuda, F.; Sakamoto, A.; et al. The effect of long-term supplementation with branched-chain amino acid granules in patients with hepatitis C virus-related hepatocellular carcinoma after radiofrequency thermal ablation. J. Clin. Gastroenterol. 2013, 47, 359–366. [Google Scholar] [CrossRef]
- Nojiri, S.; Fujiwara, K.; Shinkai, N.; Iio, E.; Joh, T. Effects of branched-chain amino acid supplementation after radiofrequency ablation for hepatocellular carcinoma: A randomized trial. Nutrition 2017, 33, 20–27. [Google Scholar] [CrossRef]
- Poon, R.T.P.; Yu, W.C.; Fan, S.T.; Wong, J. Long-term oral branched chain amino acids in patients undergoing chemoembolization for hepatocellular carcinoma: A randomized trial. Aliment. Pharmacol. Ther. 2004, 19, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Yano, Y.; Minami, A.; Hirano, H.; Momose, K.; Sugimoto, M.; Yoshida, M.; Azuma, T. Branched-chain amino acid granules improve the non-protein respiratory quotient after radiofrequency ablation. Intern. Med. 2014, 53, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, S.; Ichikawa, T.; Nakao, K.; Miyaaki, H.; Shibata, H.; Matsuzaki, T.; Muraoka, T.; Honda, T.; Otani, M.; Akiyama, M.; et al. A snack enriched with oral branched-chain amino acids prevents a fall in albumin in patients with liver cirrhosis undergoing chemoembolization for hepatocellular carcinoma. Nutr. Res. 2009, 29, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Asahina, Y.; Izumi, N. Long time oral supplementation with branched-chain amino acids improves survival and decreases recurrences in patients with hepatocellular carcinoma. Nihon Shokakibyo Gakkai Zasshi 2008, 105, 808–816. [Google Scholar]
- Yoshiji, H.; Noguchi, R.; Ikenaka, Y.; Kaji, K.; Aihara, Y.; Yamazaki, M.; Yamao, J.; Toyohara, M.; Mitoro, A.; Sawai, M.; et al. Combination of branched-chain amino acids and angiotensin-converting enzyme inhibitor suppresses the cumulative recurrence of hepatocellular carcinoma: A randomized control trial. Oncol. Rep. 2011, 26, 1547–1553. [Google Scholar] [CrossRef]
- Yoshiji, H.; Noguchi, R.; Namisaki, T.; Moriya, K.; Kitade, M.; Aihara, Y.; Douhara, A.; Yamao, J.; Fujimoto, M.; Toyohara, M.; et al. Branched-chain amino acids suppress the cumulative recurrence of hepatocellular carcinoma under conditions of insulin-resistance. Oncol. Rep. 2013, 30, 545–552. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]
- Kudo, M.; Kitano, M.; Sakurai, T.; Nishida, N. General Rules for the Clinical and Pathological Study of Primary Liver Cancer, Nationwide Follow-Up Survey and Clinical Practice Guidelines: The Outstanding Achievements of the Liver Cancer Study Group of Japan. Dig. Dis. 2015, 33, 765–770. [Google Scholar] [CrossRef]
- Nishikawa, H.; Osaki, Y. Clinical significance of therapy using branched-chain amino acid granules in patients with liver cirrhosis and hepatocellular carcinoma. Hepatol. Res. 2014, 44, 149–158. [Google Scholar] [CrossRef]
- Marchesini, G.; Marzocchi, R.; Noia, M.; Bianchi, G. Branched-chain amino acid supplementation in patients with liver diseases. J. Nutr. 2005, 135 (Suppl. 6), 1596S–1601S. [Google Scholar] [CrossRef]
- Ishikawa, T. Early administration of branched-chain amino acid granules. World J. Gastroenterol. 2012, 18, 4486–4490. [Google Scholar] [CrossRef]
- August, D. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. J. Parenter. Enteral. Nutr. 2002, 26 (Suppl. 1), 1sa–138sa. [Google Scholar]
- Suzuki, K.; Endo, R.; Kohgo, Y.; Ohtake, T.; Ueno, Y.; Kato, A.; Suzuki, K.; Shiraki, R.; Moriwaki, H.; Habu, D.; et al. Guidelines on nutritional management in Japanese patients with liver cirrhosis from the perspective of preventing hepatocellular carcinoma. Hepatol. Res. 2012, 42, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Berzigotti, A.; Zelber-Sagi, S.; Dasarathy, S.; Montagnese, S.; Genton, L.; Plauth, M.; Parés, A. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed]
- Holecek, M. Branched-chain amino acids and ammonia metabolism in liver disease: Therapeutic implications. Nutrition 2013, 29, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, G.; Marzocchi, R.; Agostini, F.; Marchesini, G. Update on branched-chain amino acid supplementation in liver diseases. Curr. Opin. Gastroenterol. 2005, 21, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, G.; Marzocchi, R.; Agostini, F.; Marchesini, G. Update on nutritional supplementation with branched-chain amino acids. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 83–87. [Google Scholar] [CrossRef]
- Ruiz-Margáin, A.; Méndez-Guerrero, O.; Román-Calleja, B.M.; González-Rodríguez, S.; Fernández-Del-Rivero, G.; Rodríguez-Córdova, P.A.; Torre, A.; Macías-Rodríguez, R.U. Dietary management and supplementation with branched-chain amino acids in cirrhosis of the liver. Rev. Gastroenterol. Mex. 2018, 83, 424–433. [Google Scholar] [CrossRef]
- Ooi, P.H.; Gilmour, S.M.; Yap, J.; Mager, D.R. Effects of branched chain amino acid supplementation on patient care outcomes in adults and children with liver cirrhosis: A systematic review. Clin. Nutr. ESPEN 2018, 28, 41–51. [Google Scholar] [CrossRef]
- Holeček, M. Side effects of amino acid supplements. Physiol. Res. 2022, 71, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Koda, M.; Ueki, M.; Maeda, Y.; Mimura, K.I.; Okamoto, K.; Matsunaga, Y.; Kawakami, M.; Hosho, K.; Murawaki, Y. The influence on liver parenchymal function and complications of radiofrequency ablation or the combination with transcatheter arterial embolization for hepatocellular carcinoma. Hepatol. Res. 2004, 29, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Li, J.X.; Wu, H.; Huang, J.W.; Zeng, Y. The influence on liver function after transcatheter arterial chemoembolization combined with percutaneous radiofrequency ablation in patients with hepatocellular carcinoma. J. Formos. Med. Assoc. 2012, 111, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Yatsuhashi, H.; Ohnishi, Y.; Nakayama, S.; Iwase, H.; Nakamura, T.; Imawari, M. Anti-hypoalbuminemic effect of branched-chain amino acid granules in patients with liver cirrhosis is independent of dietary energy and protein intake. Hepatol. Res. 2011, 41, 1027–1035. [Google Scholar] [CrossRef]
- Habu, D.; Nishiguchi, S.; Nakatani, S.; Lee, C.; Enomoto, M.; Tamori, A.; Takeda, T.; Ohfuji, S.; Fukushima, W.; Tanaka, T.; et al. Comparison of the effect of BCAA granules on between decompensated and compensated cirrhosis. Hepatogastroenterology 2009, 56, 1719–1723. [Google Scholar]
- Nishikawa, H.; Kita, R.; Kimura, T.; Ohara, Y.; Takeda, H.; Sakamoto, A.; Saito, S.; Nishijima, N.; Nasu, A.; Komekado, H.; et al. Clinical significance of early interventional therapy of branched-chain amino acid granules in patients with hepatocellular carcinoma: Propensity score matching analysis. Int. J. Oncol. 2014, 45, 1082–1090. [Google Scholar] [CrossRef]
- Konstantis, G.; Pourzitaki, C.; Chourdakis, M.; Kitsikidou, E.; Germanidis, G. Efficacy of branched chain amino acids supplementation in liver cirrhosis: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 1171–1190. [Google Scholar] [CrossRef]
- Gluud, L.L.; Dam, G.; Les, I.; Córdoba, J.; Marchesini, G.; Borre, M.; Aagaard, N.K.; Vilstrup, H. Branched-chain amino acids for people with hepatic encephalopathy. Cochrane Database Syst. Rev. 2015, 9, Cd001939. [Google Scholar] [CrossRef]
- Nishikawa, H.; Fukunishi, S.; Asai, A.; Nishiguchi, S.; Higuchi, K. Sarcopenia and Frailty in Liver Cirrhosis. Life 2021, 11, 399. [Google Scholar] [CrossRef]
- Dhaliwal, A.; Armstrong, M.J. Sarcopenia in cirrhosis: A practical overview. Clin. Med. 2020, 20, 489–492. [Google Scholar] [CrossRef]
- Marasco, G.; Serenari, M.; Renzulli, M.; Alemanni, L.V.; Rossini, B.; Pettinari, I.; Dajti, E.; Ravaioli, F.; Golfieri, R.; Cescon, M.; et al. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J. Gastroenterol. 2020, 55, 927–943. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Montano-Loza, A.J.; Lai, J.C.; Dasarathy, S.; Merli, M. Sarcopenia and frailty in decompensated cirrhosis. J. Hepatol. 2021, 75 (Suppl. 1), S147–S162. [Google Scholar] [CrossRef] [PubMed]
- Begini, P.; Gigante, E.; Antonelli, G.; Carbonetti, F.; Iannicelli, E.; Anania, G.; Imperatrice, B.; Pellicelli, A.M.; Fave, G.D.; Marignani, M. Sarcopenia predicts reduced survival in patients with hepatocellular carcinoma at first diagnosis. Ann. Hepatol. 2017, 16, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Chen, J.D.; Wu, W.T.; Huang, K.C.; Hsu, C.T.; Han, D.S. Association between Loss of Skeletal Muscle Mass and Mortality and Tumor Recurrence in Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Liver Cancer 2018, 7, 90–103. [Google Scholar] [CrossRef]
- Dodson, R.M.; Firoozmand, A.; Hyder, O.; Tacher, V.; Cosgrove, D.P.; Bhagat, N.; Herman, J.M.; Wolfgang, C.L.; Geschwind, J.F.H.; Kamel, I.R.; et al. Impact of Sarcopenia on Outcomes Following Intra-arterial Therapy of Hepatic Malignancies. J. Gastrointest. Surg. 2013, 17, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Guichet, P.L.; Taslakian, B.; Zhan, C.; Aaltonen, E.; Farquharson, S.; Hickey, R.; Horn, C.J.; Gross, J.S. MRI-Derived Sarcopenia Associated with Increased Mortality Following Yttrium-90 Radioembolization of Hepatocellular Carcinoma. Cardiovasc. Interv. Radiol. 2021, 44, 1561–1569. [Google Scholar] [CrossRef]
- Salman, A.; Salman, M.; Moustafa, A.; El-Din Shaaban, H.; El-Mikkawy, A.; Labib, S.; Youssef, A.; Gouda Omar, M.; Matter, M.; Elkassar, H. Impact of sarcopenia on two-year mortality in patients with hcv-associated hepatocellular carcinoma after radiofrequency ablation. J. Hepatocell. Carcinoma 2021, 8, 313–320. [Google Scholar] [CrossRef]
- Dimou, A.; Tsimihodimos, V.; Bairaktari, E. The Critical Role of the Branched Chain Amino Acids (BCAAs) Catabolism-Regulating Enzymes, Branched-Chain Aminotransferase (BCAT) and Branched-Chain α-Keto Acid Dehydrogenase (BCKD), in Human Pathophysiology. Int. J. Mol. Sci. 2022, 23, 4022. [Google Scholar] [CrossRef]
- van den Berg, E.H.; Flores-Guerrero, J.L.; Gruppen, E.G.; de Borst, M.H.; Wolak-Dinsmore, J.; Connelly, M.A.; Bakker, S.J.L.; Dullaart, R.P.F. Non-Alcoholic Fatty Liver Disease and Risk of Incident Type 2 Diabetes: Role of Circulating Branched-Chain Amino Acids. Nutrients 2019, 11, 705. [Google Scholar] [CrossRef]
- Galarregui, C.; Cantero, I.; Marin-Alejandre, B.A.; Monreal, J.I.; Elorz, M.; Benito-Boillos, A.; Herrero, J.I.; de la, O.V.; Ruiz-Canela, M.; Hermsdorff, H.H.M.; et al. Dietary intake of specific amino acids and liver status in subjects with nonalcoholic fatty liver disease: Fatty liver in obesity (FLiO) study. Eur. J. Nutr. 2021, 60, 1769–1780. [Google Scholar] [CrossRef]
- Lo, E.K.K.; Xu, J.H.; Zhan, Q.; Zeng, Z.; El-Nezami, H. The Emerging Role of Branched-Chain Amino Acids in Liver Diseases. Biomedicines 2022, 10, 1444. [Google Scholar] [CrossRef] [PubMed]
- Ericksen, R.E.; Lim, S.L.; McDonnell, E.; Shuen, W.H.; Vadiveloo, M.; White, P.J.; Ding, Z.; Kwok, R.; Lee, P.; Radda, G.K.; et al. Loss of BCAA Catabolism during Carcinogenesis Enhances mTORC1 Activity and Promotes Tumor Development and Progression. Cell Metab. 2019, 29, 1151–1165.e6. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Type of Study | Study Period | Group | N | Age (Years) | M/F | HBV/HCV/Other | Stage I/II/III/IV | Child–Pugh A/B/C | Max Tumor Size (cm) | Mean Tumor Number |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Harima et al. 2010 [23] | Cohort r | 12/2007–2/2009 | Control | 10 | 66.4 ± 12.8 | 8/2 | 1/8/1 | 1/2/6/1 | 6/4/0 | NR | NR |
| BCAA | 13 | 64.5 ± 9.5 | 11/2 | 5/7/1 | 1/3/3/6 | 6/7/0 | NR | NR | |||
| Ishihara et al. 2014 [24] | Cohort r | 4/2004–4/2012 | Control | 86 | 72.2 ± 8.6 | 57/29 | 13/49/24 | 21/49/11/10 | 74/11/1 | 2.9 ± 2.6 | NR |
| BCAA | 76 | 71.7 ± 7.2 | 46/30 | 9/64/3 | 13/14/21/28 | 35/36/5 | 2.9 ± 3.2 | NR | |||
| Control | 68 | 71.9 ± 6.5 | 47/21 | 7/47/14 | 21/40/6/2 | 59/9/0 | 2.1 ± 0.8 | NR | |||
| BCAA | 40 | 73.0 ± 6.0 | 13/27 | 0/34/6 | 16/16/7/1 | 23/16/1 | 2.0 ± 0.8 | NR | |||
| Ishikawa et al. 2009 [25] | Cohort r | 5/2002–11/2006 | Control | 17 | 71.6 ± 8.3 | 7/10 | NR | NR | 0/15/2 | 2.2 ± 0.7 | 1 |
| BCAA | 11 | 68.5 ± 7.4 | 4/7 | NR | NR | 0/5/6 | 2.3 ± 0.6 | 1 | |||
| Iwasa et al. 2015 [26] | Cohort p | 1/2013–12/2013 & 9/2014–11/2014 | Control | 84 | 74.0 ± 8.0 | 65/18 | 16/44/22 | 16/30/21/16 | 71/12/0 | NR | NR |
| BCAA | 36 | 70.0 ± 7.0 | 23/13 | 6/23/5 | 10/15/6/5 | 20/15/1 | NR | NR | |||
| Kanekawa et al. 2014 [27] | Cohort r | 1/2000–12/2011 | Control | 43 | 68.0 ± 7.0 | 34/9 | 6/30/7 | 0/0/14/29 | 30/13/0 | NR | NR |
| BCAA | 49 | 66.3 ± 7.0 | 43/6 | 8/30/11 | 0/0/8/41 | 23/26/0 | NR | NR | |||
| Kuroda et al. 2010 [28] | Cohort p | 10/2005–10/2006 | Control | 15 | 66.0 ± 8.1 | 9/6 | NR | 5/8/2/0 | 6/8/1 | 2.0 ± 0.4 | 1.9 ± 0.6 |
| BCAA | 20 | 65.6 ± 7.0 | 13/7 | NR | 6/11/3/0 | 8/11/1 | 2.0 ± 0.6 | 1.9 ± 0.5 | |||
| Morihara et al. 2012 [29] | RCT (pilot) | 4/2005–6/2006 | Control | 10 | 69.3 ± 8.9 | 7/3 | 0/10/0 | NR | 7/3/0 | 2.4 ± 0.8 | 1.9 ± 1.2 |
| BCAA (a.m.) | 10 | 66.9 ± 9.7 | 8/2 | 0/9/1 | NR | 7/3/0 | 2.4 ± 0.8 | 1.7 ± 0.9 | |||
| BCAA (p.m.) | 10 | 73.5 ± 8.5 | 8/2 | 0/9/1 | NR | 9/1/0 | 2.0 ± 1.1 | 1.6 ± 0.8 | |||
| Nishikawa et al. 2012 [30] | Cohort r | 1/2004–1/2010 | Control | 59 | 73.2 ± 10.1 | 32/27 | 8/43/10 | 1/11/35/12 | 39/10/1 | 3.6 ± 1.5 | NR |
| BCAA | 40 | 69.9 ± 8.8 | 27/13 | 2/28/10 | 0/12/23/5 | 22/15/3 | 3.3 ± 1.7 | NR | |||
| Nishikawa et al. 2013 [31] | Cohort r | 1/2004–10/2011 | Control | 141 | 70.9 ± 7.8 | 83/58 | 0/141/0 | 60/60/21/0 | 88/52/1 | 2.0 ± 0.7 | 1.1 ± 0.4 |
| BCAA | 115 | 69.3 ± 9.4 | 64/51 | 115/0/0 | 41/58/16/0 | 83/30/2 | 2.0 ± 0.6 | 1.1 ± 0.4 | |||
| Nojiri et al. 2016 [32] | RCT | 8/2009–4/2012 | Control | 26 | 69.1 ± 11.0 | 15/11 | 22/2/2 | 14/9/3/0 | 23/3/0 | 1.8 ± 0.6 | 1.5 ± 0.5 |
| BCAA | 25 | 69.7 ± 9.0 | 15/10 | 22/1/2 | 15/8/2/0 | 21/4/0 | 1.8 ± 0.6 | 1.4 ± 0.5 | |||
| Poon et al. 2004 [33] | RCT | 7/1998–12/2000 | Control | 43 | 57.9 ± 12.1 | 39/4 | NR | NR | NR | 7.1 ± 3.6 | NR |
| BCAA | 41 | 58.0 ± 13.9 | 39/2 | NR | NR | NR | 7.4 ± 3.4 | NR | |||
| Saito et al. 2014 [34] | Cohort p | 8/2009–12/2012 | Control | 27 | 70.0 ± 1.9 | 16/11 | 5/18/4 | 14/10/3/0 | NR | NR | NR |
| BCAA | 13 | 73.4 ± 2.2 | 8/5 | 0/11/2 | 4/7/1/1 | NR | NR | NR | |||
| Takeshita et al. 2009 [35] | RCT | 1/2004–12/2005 | Control | 28 | 70.6 ± 9.8 | 21/7 | NR | NR | NR | NR | NR |
| BCAA | 28 | 69.1 ± 8.2 | 19/9 | NR | NR | NR | NR | NR | |||
| Tsuchiya et al. 2008 [36] | Cohort r | 4/1999–9/2004 | Control | 190 | 67.2 ± 9.0 | 127/63 | NR | 44/113/33/0 | NR | 2.4 ± 0.9 | NR |
| BCAA | 85 | 67.8 ± 6.9 | 41/44 | NR | 20/41/24/0 | NR | 2.3 ± 0.9 | NR | |||
| Yoshiji et al. 2011 [37] | RCT | 5/2004–7/2006 | Control | 26 | 62.5 ± 11.5 | 16/10 | 18/6/8 | 18/7/1/0 | 21/5/0 | 2.1 ± 0.9 | NR |
| BCAA | 16 | 63.7 ± 10.8 | 10/6 | 10/5/5 | 10/5/1/0 | 12/4/0 | 1.8 ± 0.9 | NR | |||
| Yoshiji et al. 2013 [38] | RCT | NR | Control | 42 | 62.2 ± 14.8 | 25/17 | 6/32/13 | 25/16/1/0 | 33/9/0 | 2.2 ± 0.9 | 1.7 ± 1.2 |
| BCAA | 51 | 63.6 ± 15.3 | 32/19 | 9/36/15 | 29/20/2/0 | 41/10/0 | 2.2 ± 0.9 | 1.8 ± 1.0 |
| Laboratory Value | Controls | BCAA | Significance Level | Studies |
|---|---|---|---|---|
| Albumin (mg/dL) | 3.6 ± 0.2 | 3.4 ± 0.2 | p > 0.05 | [23,24,26,27,28,29,30,31,32,33,34,35,37,38] |
| PT (%) | 86.2 ± 5.9 | 82.3 ± 5.1 | p > 0.05 | [23,24,27,28,29,30,31,32,34] |
| TBil (g/dL) | 1.0 ± 0.1 | 1.1 ± 0.2 | p > 0.05 | [23,24,27,28,29,30,31,32,34,35] |
| AFP (ng/mL) | 3713.3 ± 10,982.3 | 1872.3 ± 4481.1 | p > 0.05 | [24,26,27,29,30,31,32,34,37,38] |
| AST (IU/L) | 61.3 ± 6.4 | 64.7 ± 10.4 | p > 0.05 | [28,29,30,31,32,33,34,35] |
| ALT (IU/L) | 56.3 ± 10.0 | 54.5 ± 12.0 | p > 0.05 | [23,27,29,30,31,32,34,35,37,38] |
| Ammonia (ug/dL) | 52.3 ± 5.3 | 77.0 ± 20.2 | p > 0.05 | [23,26,27,35] |
| PLT (×104/mm3) | 11.7 ± 2.6 | 10.0 ± 1.2 | p > 0.05 | [27,28,29,30,31,34,35] |
| BTR | 4.2 ± 0.8 | 3.7 ± 0.3 | p > 0.05 | [23,28,29,32,35] |
| Author | Group | N | RFA | TACE | TACE + RFA | HAIC | BCAA Type | BCAA Dose | BCAA Initiation * | Follow-Up Time | Endpoints for Labs |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Harima et al. 2010 [23] | Control | 10 | 10 | >12 months | 5 weeks | ||||||
| BCAA | 13 | 13 | Aminoleban EN | 50 g qd (10 p.m.) | NR | ||||||
| Ishihara et al. 2014 [24] | Control | 86 | 86 | 10 days | 2, 5, 10 days | ||||||
| BCAA | 76 | 76 | LIVACT granules | 4.15 g tid | ≥2 weeks prior | ||||||
| Control | 68 | 68 | 10 days | 2, 5, 10 days | |||||||
| BCAA | 40 | 40 | LIVACT granules | 4.15 g tid | ≥2 weeks prior | ||||||
| Ishikawa et al. 2009 [25] | Control | 17 | 17 | 12 months | 1, 6, 12 months | ||||||
| BCAA | 11 | 11 | Aminoleban EN | NR | NR | ||||||
| Iwasa et al. 2015 [26] | Control | 84 | 22 | 43 | 17 | 2 | 17 ± 8 days | Time of discharge (17 ± 8 days) | |||
| BCAA | 36 | 12 | 14 | 8 | 2 | LIVACT granules or Aminoleban EN | 4.15 g tid or 50 g bid respectively | ≥4 weeks prior | 21 ± 15 days | Time of discharge (21 ± 15 days) | |
| Kanekawa et al. 2014 [27] | Control | 43 | 43 | >2 years | At every chemo session (every 5 days × 4 weeks) | ||||||
| BCAA | 49 | 49 | LIVACT granules or Aminoleban EN | 4.15 g tid or 50 g bid respectively | Immediately after | ||||||
| Kuroda et al. 2010 [28] | Control | 15 | 15 | 12 months | 3, 6, 9, 12 months | ||||||
| BCAA | 20 | 20 | Aminoleban EN | 50 g bid | NR | ||||||
| Morihara et al. 2012 [29] | Control | 10 | 10 | 12 weeks | 1, 4, 12 weeks | ||||||
| BCAA (a.m.) | 10 | 10 | Aminoleban EN | 50 g qd (7–10 a.m.) | NR | ||||||
| BCAA (p.m.) | 10 | 10 | 50 g qd (10 p.m.) | ||||||||
| Nishikawa et al. 2012 [30] | Control | 59 | 59 | 6 months | 1, 3, 6 months | ||||||
| BCAA | 40 | 40 | LIVACT granules | 4.15 g tid | NR | ||||||
| Nishikawa et al. 2013 [31] | Control | 141 | 141 | 2.5 ± 1,3 years | NA | ||||||
| BCAA | 115 | 115 | LIVACT granules | 4.15 g tid | NR | 2.7 ± 1.5 years | |||||
| Nojiri et al. 2016 [32] | Control | 26 | 26 | 60 months | 12 months | ||||||
| BCAA | 25 | 25 | Aminoleban EN | 50 g bid | 2 weeks prior | ||||||
| Poon et al. 2004 [33] | Control | 43 | 43 | 30.1 ± 5.7 months | 3, 6, 9, 12 months | ||||||
| BCAA | 41 | 41 | Aminoleban EN | 50 g bid | 1 week prior | 29.4 ± 6.0 months | |||||
| Saito et al. 2014 [34] | Control | 27 | 27 | 3 months | 7 days, 3 months | ||||||
| BCAA | 13 | 13 | LIVACT granules | 4.15 g tid | ≥12 weeks prior | ||||||
| Takeshita et al. 2009 [35] | Control | 28 | 28 | 2.7 years | 2 weeks | ||||||
| BCAA | 28 | 28 | Aminoleban EN | 50 g qd (10 p.m.) | 1 day prior | 2.9 years | |||||
| Tsuchiya et al. 2008 [36] | Control | 190 | 190 | >2 years | NA | ||||||
| BCAA | 85 | 85 | LIVACT granules | 4.15 g tid | NR | ||||||
| Yoshiji et al. 2011 [37] | Control | 26 | 26 | 48 months | 12 months | ||||||
| BCAA | 16 | 16 | LIVACT granules | 4.15 g tid | NR | ||||||
| Yoshiji et al. 2013 [38] | Control | 42 | 42 | 60 months | NA | ||||||
| BCAA | 51 | 51 | LIVACT granules | 4.15 g tid | NR |
| Outcome | Total # of Studies | BCAA > Controls | Controls > BCAA | No Difference |
|---|---|---|---|---|
| OS | 6 | 2 studies [31,32] + 3 studies * [23,27,36] | 1 study [35] | |
| Mortality Rate | 5 | 2 studies [30,32] | 3 studies [23,28,33] | |
| RFS | 2 | 1 study [31] | 1 study [30,32] | |
| Recurrence Rate | 6 | 3 studies [31,32,38] | 3 studies [28,36,37] | |
| EFS | 2 | 1 study [32] | 1 study [28] | |
| Overall Events, ascites | 3 | 2 studies [32,33] | 1 study [28] | |
| Readmission rates, peripheral edema | 1 | 1 study [33] | ||
| Variceal rupture | 3 | 3 studies [28,32,33] | ||
| HE, liver abscess | 2 | 2 studies for each ** | ||
| Liver failure, jaundice, tumor rupture, biloma, intra-abdominal bleeding, renal failure, pneumothorax/hemothorax | 1 | 1 study for each ** | ||
| Child–Pugh score | 5 | 3 studies [27,29,30] | 2 studies [32,34] | |
| Albumin | 13 | 11 studies [23,27,28,29,30,32,33,34] | 2 studies [25,37] | |
| AST/ALT | 9 | 1 study [23] | 8 studies [24,27,28,32,33,34,35,37] | |
| Ammonia | 2 | 1 study [35] + 1 study * [26] | ||
| TBil | 6 | 2 studies [29,33] | 4 studies [27,28,34,35] | |
| PT | 6 | 1 study [34] | 5 studies [27,28,29,32,33] | |
| BTR | 6 | 2 studies [23,32] | 4 studies [24,26,28,35] | |
| FPG | 5 | 5 studies [23,28,32,35,37] | ||
| ChE | 3 | 2 studies [23,35] | 1 study [34] | |
| BMI | 3 | 3 studies [23,33,35] | ||
| npRQ | 3 | 3 studies [23,28,34] | ||
| Quality of life | 3 | 2 studies (SF-8) [28,32] + 1 study (FACT-G) [33] | ||
| GGT, LDH, HOMA-IR, IRI | 2 | 2 studies for each ** | ||
| CRP, TProt, TChol, LYMPH, RBC, VEGF, TG | 1 | 1 study for each ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sideris, G.A.; Tsaramanidis, S.; Vyllioti, A.T.; Njuguna, N. The Role of Branched-Chain Amino Acid Supplementation in Combination with Locoregional Treatments for Hepatocellular Carcinoma: Systematic Review and Meta-Analysis. Cancers 2023, 15, 926. https://doi.org/10.3390/cancers15030926
Sideris GA, Tsaramanidis S, Vyllioti AT, Njuguna N. The Role of Branched-Chain Amino Acid Supplementation in Combination with Locoregional Treatments for Hepatocellular Carcinoma: Systematic Review and Meta-Analysis. Cancers. 2023; 15(3):926. https://doi.org/10.3390/cancers15030926
Chicago/Turabian StyleSideris, Georgios A., Savvas Tsaramanidis, Aikaterini T. Vyllioti, and Njogu Njuguna. 2023. "The Role of Branched-Chain Amino Acid Supplementation in Combination with Locoregional Treatments for Hepatocellular Carcinoma: Systematic Review and Meta-Analysis" Cancers 15, no. 3: 926. https://doi.org/10.3390/cancers15030926
APA StyleSideris, G. A., Tsaramanidis, S., Vyllioti, A. T., & Njuguna, N. (2023). The Role of Branched-Chain Amino Acid Supplementation in Combination with Locoregional Treatments for Hepatocellular Carcinoma: Systematic Review and Meta-Analysis. Cancers, 15(3), 926. https://doi.org/10.3390/cancers15030926