
Epidemiology, Diagnosis and Management of Penile Cancer: Results from the Spanish National Registry of Penile Cancer

 ,
,  , , , , , , ,
, , , , , , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Recruitment
2.2. Objective
2.3. Statistical Analysis
3. Results
3.1. Clinics
3.2. Histology and Staging
3.3. Management
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Promotor
References
- Chaux, A.; Netto, G.J.; Rodríguez, I.M.; Barreto, J.E.; Oertell, J.; Ocampos, S.; Boggino, H.; Codas, R.; Bosch, F.X.; de Sanjose, S.; et al. Epidemiologic profile, sexual history, pathologic features, and human papillomavirus status of 103 patients with penile carcinoma. World J. Urol. 2013, 31, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Backes, D.M.; Kurman, R.J.; Pimenta, J.M.; Smith, J.S. Systematic review of human papillomavirus prevalence in invasive penile cancer. Cancer Causes Control. 2009, 20, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Baldur-Felskov, B.; Hannibal, C.G.; Munk, C.; Kjaer, S.K. Increased incidence of penile cancer and high-grade penile intraepithelial neoplasia in Denmark 1978–2008: A nationwide population-based study. Cancer Causes Control. 2012, 23, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Schoffer, O.; Neumann, A.; Stabenow, R.; Schülein, S.; Böhm, W.-D.; Gonsior, A.; Horn, L.-C.; Kriegel, C.; Stolzenburg, J.-U.; Wirth, M.; et al. Penile cancer—Incidence, mortality, and survival in Saxony, Germany. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 295.e1–295.e8. [Google Scholar] [CrossRef]
- Pow-Sang, M.R.; Ferreira, U.; Pow-Sang, J.M.; Nardi, A.C.; Destefano, V. Epidemiology and Natural History of Penile Cancer. Urology 2010, 76, S2–S6. [Google Scholar] [CrossRef]
- Morris, B.J.; Kennedy, S.E.; Wodak, A.D.; Mindel, A.; Golovsky, D.; Schrieber, L.; Lumbers, E.R.; Handelsman, D.J.; Ziegler, J.B. Early infant male circumcision: Systematic review, risk-benefit analysis, and progress in policy. World J. Clin. Pediatr. 2017, 6, 89–102. [Google Scholar] [CrossRef]
- Hakenberg, O.W.; Compérat, E.M.; Minhas, S.; Necchi, A.; Protzel, C.; Watkin, N. EAU guidelines on penile cancer EAU Guidelines Edn. In Proceedings of the EAU Annual Congress, Amsterdam, The Netherlands, 1–4 July 2022. [Google Scholar]
- Douglawi, A.; Masterson, T.A. Penile cancer epidemiology and risk factors. Curr. Opin. Urol. 2019, 29, 145–149. [Google Scholar] [CrossRef]
- Saraiya, M.; Unger, E.R.; Thompson, T.D.; Lynch, C.F.; Hernandez, B.Y.; Lyu, C.W.; Steinau, M.; Watson, M.; Wilkinson, E.J.; Hopenhayn, C.; et al. US Assessment of HPV Types in Cancers: Implications for Current and 9-Valent HPV Vaccines. Gynecol. Oncol. 2015, 107, djv086. [Google Scholar] [CrossRef]
- Catalfamo, C.J.M.; Brown, H.E.; Dennis, L.K. Evaluating the Strength of Association of Human Papillomavirus Infection with Penile Carcinoma: A Meta-Analysis. Sex. Transm. Dis. 2022, 49, 368–376. [Google Scholar] [CrossRef]
- Faggiano, F.; Partanen, T.; Kogevinas, M.; Boffetta, P. Socioeconomic differences in cancer incidence and mortality. IARC Sci. Publ. 1997, 65–176. [Google Scholar]
- Favorito, L.A.; Nardi, A.C.; Ronalsa, M.; Zequi, S.C.; Sampaio, F.J.B.; Glina, S. Epidemiologic study on penile cancer in Brazil. Int. Braz. J. Urol. 2008, 34, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Bleeker, M.C.G.; Heideman, D.A.M.; Snijders, P.J.F.; Horenblas, S.; Dillner, J.; Meijer, C.J.L.M. Penile cancer: Epidemiology, pathogenesis and prevention. World J. Urol. 2009, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Necchi, A.; Muneer, A.; Tobias-Machado, M.; Tran, A.T.H.; Van Rompuy, A.-S.; Spiess, P.E.; Albersen, M. Penile cancer. Nat. Rev. Dis. Prim. 2021, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Olesen, T.B.; Sand, F.L.; Aalborg, G.L.; Munk, C.; Kjaer, S.K. Incidence of penile intraepithelial neoplasia and incidence and survival of penile cancer in Denmark, 1997 to 2018. Cancer Causes Control. 2022, 33, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Christodoulidou, M.; Sahdev, V.; Houssein, S.; Muneer, A. Epidemiology of penile cancer. Curr. Probl. Cancer 2015, 39, 126–136. [Google Scholar] [CrossRef]
- Arya, M.; Li, R.; Pegler, K.; Sangar, V.; Kelly, J.D.; Minhas, S.; Muneer, A.; Coleman, M.P. Long-term trends in incidence, survival and mortality of primary penile cancer in England. Cancer Causes Control. 2013, 24, 2169–2176. [Google Scholar] [CrossRef]
- Amini, A.P.; Brookes, T.S.; Shah, H.; Bhate, K.; Alnajjar, H.; Muneer, A.; Kravvas, G.; Bunker, C.B. The association between penile cancer and HIV infection: A literature review. Int. J. STD AIDS 2023, 11, 9564624221148622. [Google Scholar] [CrossRef]
- Nuñez, O.; Hernando, V.; Díaz, A. Estimating the number of people living with HIV and the undiagnosed fraction in Spain in 2013. Aids 2018, 32, 2573–2581. [Google Scholar] [CrossRef]
- Douglawi, A.; Masterson, T.A. Updates on the epidemiology and risk factors for penile cancer. Transl. Androl. Urol. 2017, 6, 785–790. [Google Scholar] [CrossRef]
- Bandini, M.; Zhu, Y.; Ye, D.-W.; Ornellas, A.A.; Watkin, N.; Ayres, B.; Hakenberg, O.W.; Heidenreich, A.; Raggi, D.; Giannatempo, P.; et al. Contemporary Treatment Patterns and Outcomes for Patients with Penile Squamous Cell Carcinoma: Identifying Management Gaps to Promote Multi-institutional Collaboration. Eur. Urol. Oncol. 2021, 4, 121–123. [Google Scholar] [CrossRef]
- Albersen, M.; Parnham, A.; Joniau, S.; Sahdev, V.; Christodoulidou, M.; Castiglione, F.; Nigam, R.; Malone, P.; Freeman, A.; Jameson, C.; et al. Predictive factors for local recurrence after glansectomy and neoglans reconstruction for penile squamous cell carcinoma. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.H.; Yan, S.; Ottenhof, S.R.; Draeger, D.; Baumgarten, A.; Chipollini, J.; Protzel, C.; Zhu, Y.; Ye, D.-W.; Hakenberg, O.W.; et al. Glansectomy as Primary Management of Penile Squamous Cell Carcinoma: An International Study Collaboration. Urology 2017, 109, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.H.; Muneer, A.; Alnajjar, H.M. Glansectomy and Reconstruction for Penile Cancer: A Systematic Review. Eur. Urol. Focus 2022, 8, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Pohanková, D.; Sirák, I.; Vošmik, M.; Kašaová, L.; Grepl, J.; Paluska, P.; Holub, L.; Špaček, J.; Hodek, M.; Kopeček, M.; et al. High-Dose-Rate Brachytherapy as an Organ-Sparing Treatment for Early Penile Cancer. Cancers 2022, 14, 6248. [Google Scholar] [CrossRef]
- Bandini, M.; Spiess, P.E.; Zhu, Y.; Ornellas, A.A.; Ayres, B.A.; Hakenberg, O.W.; Haidl, F.; Pederzoli, F.; Basile, G.; Briganti, A.; et al. The Relationship of Circumcision with Clinical Tumor Staging of Penile Cancer. Société Int. D’urologie J. 2022, 3, 102–107. [Google Scholar] [CrossRef]
- Mishra, K.; Isali, I.; Sindhani, M.; Prunty, M.; Bell, S.; Mahran, A.; Damiani, G.; Ghannoum, M.; Retuerto, M.; Kutikov, A.; et al. Characterization of Changes in Penile Microbiome Following Pediatric Circumcision. Eur. Urol. Focus 2022. [Google Scholar] [CrossRef]
- Bandini, M.; Ahmed, M.; Basile, G.; Watkin, N.; Master, V.; Zhu, Y.; Prakash, G.; Rodriguez, A.; Ssebakumba, M.K.; Leni, R.; et al. A global approach to improving penile cancer care. Nat. Rev. Urol. 2022, 19, 231–239. [Google Scholar] [CrossRef]
- Daubisse-Marliac, L.; Colonna, M.; Trétarre, B.; Defossez, G.; Molinié, F.; Jéhannin-Ligier, K.; Marrer, E.; Grosclaude, P. Long-term trends in incidence and survival of penile cancer in France. Cancer Epidemiol. 2017, 50, 125–131. [Google Scholar] [CrossRef]
- Marino, F.Z.; Sabetta, R.; Pagliuca, F.; Brunelli, M.; Aquino, G.; Perdonà, S.; Botti, G.; Facchini, G.; Fiorentino, F.; Di Lauro, G.; et al. Discrepancy of p16 immunohistochemical expression and HPV RNA in penile cancer. A multiplex in situ hybridization/immunohistochemistry approach study. Infect. Agents Cancer 2021, 16, 22. [Google Scholar] [CrossRef]
- Medeiros-Fonseca, B.; Cubilla, A.; Brito, H.; Martins, T.; Medeiros, R.; Oliveira, P.; Gil da Costa, R. Experimental Models for Studying HPV-Positive and HPV-Negative Penile Cancer: New Tools for An Old Disease. Cancers 2021, 13, 460. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Median (IQR) or Number (%) | |
|---|---|
| Age, years | 72 (62–81) |
| Prior circumcision | 70 (30.7) |
| Prior HPV exposure | |
| Yes | 2 (0.9) |
| No | 28 (12.3) |
| Unknown | 198 (86.8) |
| Local hygiene | |
| Correct | 62 (27.2) |
| Poor | 48 (21.1) |
| Unknown | 188 (51.7) |
| Smoking habits | |
| Never | 73 (32) |
| Current | 63 (27.6) |
| Unknown | 92 (40.4) |
| Promiscuous sexual habits | |
| Yes | 10 (4.4) |
| No | 47 (20.6) |
| Unknown | 171 (75) |
| Prior penile lesion | |
| Yes | 62 (27.2) |
| No | 97 (42.5) |
| Unknown | 69 (30.3) |
| Referral to a urologist | |
| Specialist | 104 (45.6) |
| General practitioner | 75 (32.9) |
| Entourage | 10 (4.4) |
| Unknown | 39 (17.1) |
| Symptoms | |
| Visually assessed penile lesion | 138 (60.5) |
| Suppuration | 27 (11.8) |
| Pain | 13 (5.7) |
| Itching | 14 (6.1) |
| Unknown | 36 (15.9) |
| Phimosis at clinical presentation | 103 (45.2) |
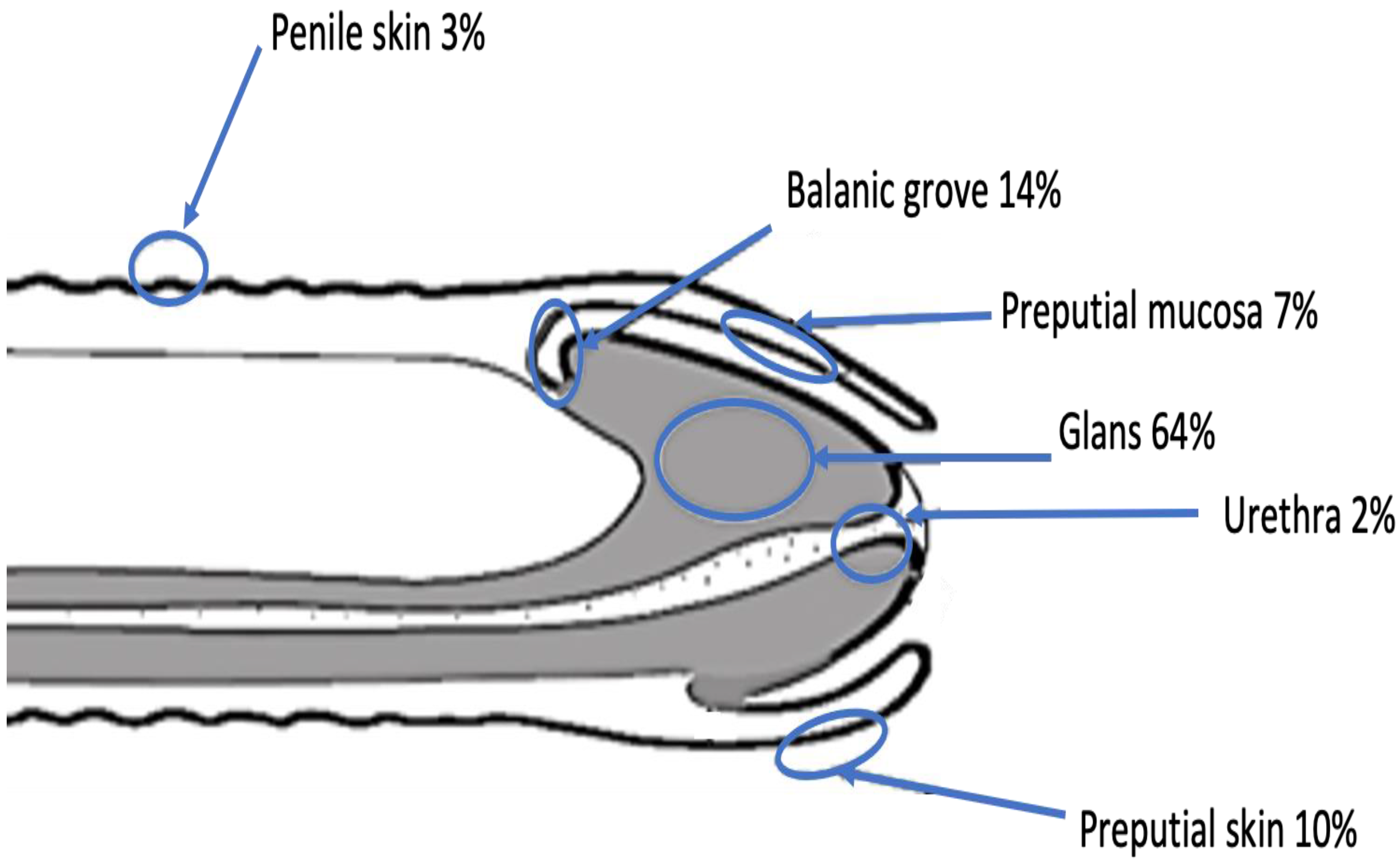
| Tumor location | |
| Glans | 145 (63.6) |
| Balanic groove | 17 (7.5) |
| Preputial skin | 22 (9.7) |
| Preputial mucosa | 32 (14) |
| Penile skin | 6 (2.6) |
| Urethra | 5 (2.2) |
| Unknown | 1 (0.4) |
| Median (IQR) or Number (%) | |
|---|---|
| Histology | |
| Squamous cell carcinoma (SCC) | 217 (95.2) |
| Undetermined carcinoma | 1 (0.4) |
| Melanoma | 1 (0.4) |
| Unknown | 9 (4) |
| SqCC subtype | |
| Common carcinoma | 143 (62.7) |
| Basaloid carcinoma | 5 (2.2) |
| Warty carcinoma | 9 (4) |
| Papillary carcinoma | 2 (0.9) |
| Verrucous carcinoma | 28 (12.3) |
| Sarcomatoid carcinoma | 1 (0.4) |
| Mixed carcinoma | 4 (1.7) |
| Adenosquamous carcinoma | 2 (0.9) |
| Unknown | 34 (14.9) |
| Clinical T stage | |
| cTx | 23 (10.1) |
| cT0 | 5 (2.2) |
| cTis | 22 (9.6) |
| cTa | 7 (3.1) |
| cT1a | 51 (22.4) |
| cT1b | 17 (7.5) |
| cT2 (corpus spongiosum) | 45 (19.7) |
| cT2 (corpus cavernosum) | 21 (9.2) |
| cT3 | 28 (12.3) |
| cT4 | 9 (3.9) |
| Clinical N stage | |
| Nx | 55 (24.1) |
| N0 | 132 (57.9) |
| N1 | 11 (4.8) |
| N2 | 16 (7) |
| N3 | 14 (3.1) |
| Clinical M stage | |
| Mx | 35 (15.3) |
| M0 | 181 (79.4) |
| M1 | 12 (5.3) |
| Grade at biopsy | |
| Gx | 78 (34.2) |
| G1 | 60 (26.3) |
| G2 | 57 (25) |
| G3–G4 | 33 (14.5) |
| Pathological T stage | |
| pTx | 7 (3.1) |
| pT0 | 3 (1.3) |
| pTis | 23 (10.1) |
| pTa | 7 (3.1) |
| pT1a | 54 (23.7) |
| pT1b | 17 (7.5) |
| pT2 (corpus spongiosum) | 50 (21.9) |
| pT2 (corpus cavernosum) | 22 (9.6) |
| pT3 | 37 (16.2) |
| pT4 | 8 (3.5) |
| Pathological N stage | |
| pNx | 98 (43) |
| pN0 | 91 (39.9) |
| pN1 | 12 (5.3) |
| pN2 | 10 (4.4) |
| pN3 | 17 (7.4) |
| Grade in the final specimen | |
| Gx | 57 (25) |
| G1 | 72 (31.5) |
| G2 | 64 (28.1) |
| G3–G4 | 35 (15.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borque-Fernando, Á.; Gaya, J.M.; Esteban-Escaño, L.M.; Gómez-Rivas, J.; García-Baquero, R.; Agreda-Castañeda, F.; Gallioli, A.; Verri, P.; Ortiz-Vico, F.J.; Amir-Nicolau, B.F.; et al. Epidemiology, Diagnosis and Management of Penile Cancer: Results from the Spanish National Registry of Penile Cancer. Cancers 2023, 15, 616. https://doi.org/10.3390/cancers15030616
Borque-Fernando Á, Gaya JM, Esteban-Escaño LM, Gómez-Rivas J, García-Baquero R, Agreda-Castañeda F, Gallioli A, Verri P, Ortiz-Vico FJ, Amir-Nicolau BF, et al. Epidemiology, Diagnosis and Management of Penile Cancer: Results from the Spanish National Registry of Penile Cancer. Cancers. 2023; 15(3):616. https://doi.org/10.3390/cancers15030616
Chicago/Turabian StyleBorque-Fernando, Ángel, Josep Maria Gaya, Luis Mariano Esteban-Escaño, Juan Gómez-Rivas, Rodrigo García-Baquero, Fernando Agreda-Castañeda, Andrea Gallioli, Paolo Verri, Francisco Javier Ortiz-Vico, Balig Fawwaz Amir-Nicolau, and et al. 2023. "Epidemiology, Diagnosis and Management of Penile Cancer: Results from the Spanish National Registry of Penile Cancer" Cancers 15, no. 3: 616. https://doi.org/10.3390/cancers15030616
APA StyleBorque-Fernando, Á., Gaya, J. M., Esteban-Escaño, L. M., Gómez-Rivas, J., García-Baquero, R., Agreda-Castañeda, F., Gallioli, A., Verri, P., Ortiz-Vico, F. J., Amir-Nicolau, B. F., Osman-Garcia, I., Gil-Martínez, P., Arrabal-Martín, M., Gómez-Ferrer Lozano, Á., Campos-Juanatey, F., Guerrero-Ramos, F., Rubio-Briones, J., & on behalf of Grupo Cooperativo de Registro Nacional Cáncer Pene (PIEM/AEU/2014/0002). (2023). Epidemiology, Diagnosis and Management of Penile Cancer: Results from the Spanish National Registry of Penile Cancer. Cancers, 15(3), 616. https://doi.org/10.3390/cancers15030616