
Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response

 ,
,  , , , ,
, , , ,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Design and Methods
2.1. Study Design and Target Population
2.2. TMA Preparation for the Detection of TME Markers
2.3. Slide-Scanning and Digital Image Analysis
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Clinico-Pathological, Cellular and Genetic Characteristics of the Patient Cohort
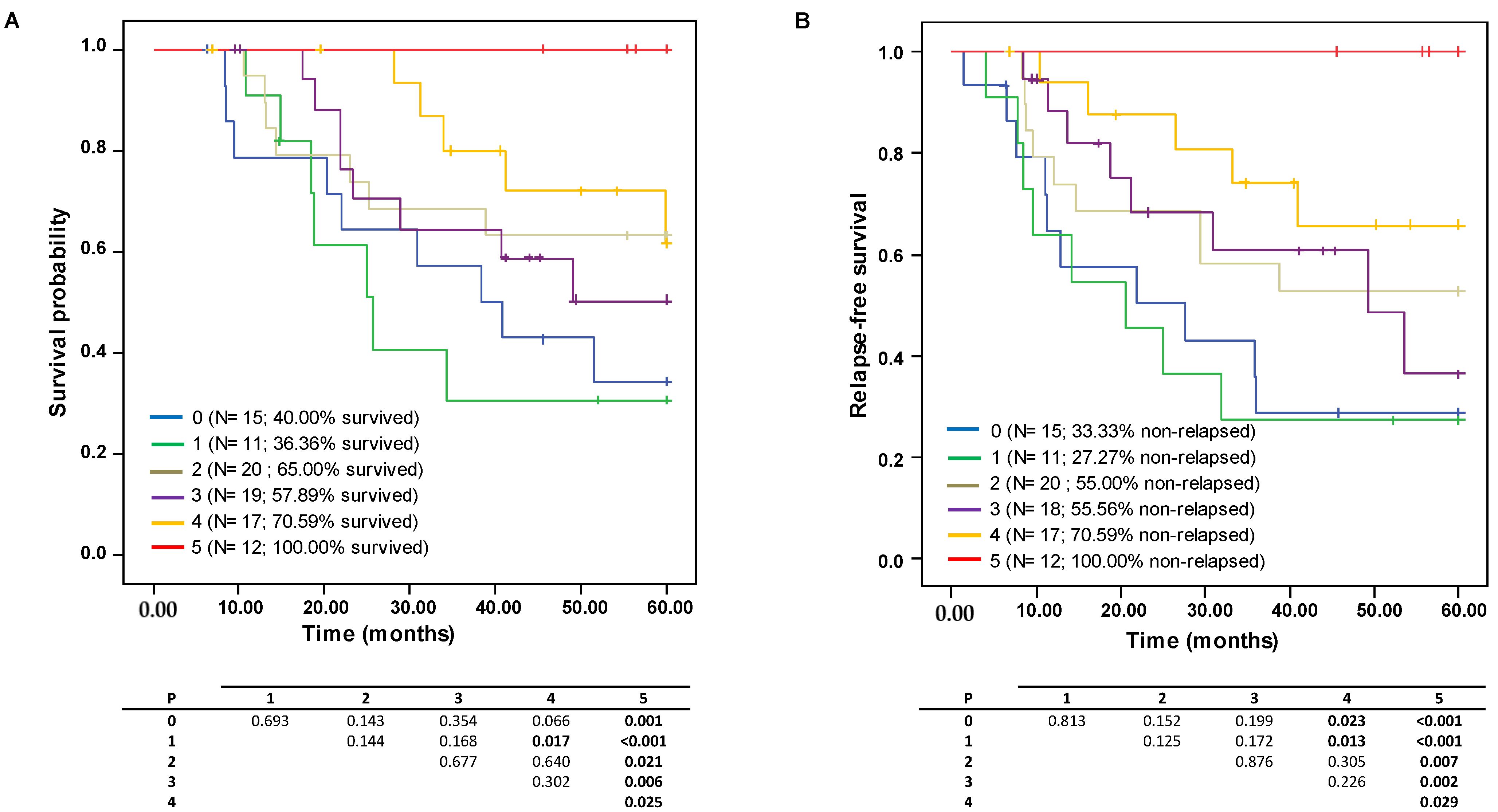
3.2. Survival Curve Analysis According to IHC Markers and mRNA Expression Levels
3.3. Univariate and Multivariate Cox Regression of Markers and Clinico-Pathological Findings in Residual Tumor Post-NAC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-negative breast cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.J.; Tan, P.H.; van de Vijver, M.J. World Health Organization Classification of Tumours of the Breast, 5th ed.; IARC Press: Lyon, France, 2019; ISBN -10: 9283245008. [Google Scholar]
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, M.; Seo, J.H.; Gong, G.; Lee, H.J. Changes in Tumor-infiltrating Lymphocytes after Neoadjuvant Chemotherapy and Clinical Significance in Triple Negative Breast Cancer. Anticancer Res. 2020, 40, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Mustacchi, G.; De Laurentiis, M. The role of taxanes in triple-negative breast cancer: Literature review. Drug Des. Devel. Ther. 2015, 9, 4303–4318. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Pivot, X.; Cortes, J.; Elias, A.; Cesari, R.; Khosravan, R.; Collier, M.; Huang, X.; Cataruozolo, P.E.; Kern, K.A.; et al. Randomized phase II study of sunitinib versus standard of care for patients with previously treated advanced triple-negative breast cancer. Breast 2013, 22, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; Andre, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Curigliano, G.; Criscitiello, C.; Gelao, L.; Goldhirsch, A. Molecular pathways: Human leukocyte antigen G (HLA-G). Clin. Cancer Res. 2013, 19, 5564–5571. [Google Scholar] [CrossRef]
- Yu, K.D.; Zhu, R.; Zhan, M.; Rodriguez, A.A.; Yang, W.; Wong, S.; Makris, A.; Lehmann, B.D.; Chen, X.; Mayer, I.; et al. Identification of prognosis-relevant subgroups in patients with chemoresistant triple-negative breast cancer. Clin. Cancer Res. 2013, 19, 2723–2733. [Google Scholar] [CrossRef]
- Hanahan, D.; Coussens, L.M. Accessories to the crime: Functions of cells recruited to the tumor microenvironment. Cancer Cell 2012, 21, 309–322. [Google Scholar] [CrossRef]
- Vanguri, R.S.; Fenn, K.M.; Kearney, M.R.; Wang, Q.; Guo, H.; Marks, D.K.; Chin, C.; Alcus, C.F.; Thompson, J.B.; Leu, C.S.; et al. Tumor Immune Microenvironment and Response to Neoadjuvant Chemotherapy in Hormone Receptor/HER2+ Early Stage Breast Cancer. Clin. Breast Cancer 2022, 22, 538–546. [Google Scholar] [CrossRef]
- von der Lippe Gythfeldt, H.; Lien, T.; Tekpli, X.; Silwal-Pandit, L.; Borgen, E.; Garred, O.; Skjerven, H.; Schlichting, E.; Lundgren, S.; Wist, E.; et al. Immune phenotype of tumor microenvironment predicts response to bevacizumab in neoadjuvant treatment of ER-positive breast cancer. Int. J. Cancer 2020, 147, 2515–2525. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, L.G.; Sarian, L.O.; Vassallo, J.; de Paiva Silva, G.R.; Ramalho, S.O.B.; Ferracini, A.C.; da Silva Araujo, K.; Jales, R.M.; Figueira, D.E.; Derchain, S. Evaluation of PD-L1 and tumor infiltrating lymphocytes in paired pretreatment biopsies and post neoadjuvant chemotherapy surgical specimens of breast carcinoma. Sci. Rep. 2021, 11, 22478. [Google Scholar] [CrossRef] [PubMed]
- Upadhya, D.; Hattiangady, B.; Castro, O.W.; Shuai, B.; Kodali, M.; Attaluri, S.; Bates, A.; Dong, Y.; Zhang, S.C.; Prockop, D.J.; et al. Human induced pluripotent stem cell-derived MGE cell grafting after status epilepticus attenuates chronic epilepsy and comorbidities via synaptic integration. Proc. Natl. Acad. Sci. USA 2019, 116, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Giraldo, N.A.; Sanchez-Salas, R.; Peske, J.D.; Vano, Y.; Becht, E.; Petitprez, F.; Validire, P.; Ingels, A.; Cathelineau, X.; Fridman, W.H.; et al. The clinical role of the TME in solid cancer. Br. J. Cancer 2019, 120, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Badr, N.M.; Berditchevski, F.; Shaaban, A.M. The Immune Microenvironment in Breast Carcinoma: Predictive and Prognostic Role in the Neoadjuvant Setting. Pathobiology 2020, 87, 61–74. [Google Scholar] [CrossRef]
- Valenberg, F.; Hiar, A.M.; Wallace, E.; Bridge, J.A.; Mayne, D.J.; Beqaj, S.; Sexton, W.J.; Lotan, Y.; Weizer, A.Z.; Jansz, G.K.; et al. Prospective Validation of an mRNA-based Urine Test for Surveillance of Patients with Bladder Cancer. Eur. Urol. 2019, 75, 853–860. [Google Scholar] [CrossRef]
- Miyashita, M.; Sasano, H.; Tamaki, K.; Hirakawa, H.; Takahashi, Y.; Nakagawa, S.; Watanabe, G.; Tada, H.; Suzuki, A.; Ohuchi, N.; et al. Prognostic significance of tumor-infiltrating CD8+ and FOXP3+ lymphocytes in residual tumors and alterations in these parameters after neoadjuvant chemotherapy in triple-negative breast cancer: A retrospective multicenter study. Breast Cancer Res. 2015, 17, 124. [Google Scholar] [CrossRef]
- Pinard, C.; Debled, M.; Ben Rejeb, H.; Velasco, V.; Tunon de Lara, C.; Hoppe, S.; Richard, E.; Brouste, V.; Bonnefoi, H.; MacGrogan, G. Residual cancer burden index and tumor-infiltrating lymphocyte subtypes in triple-negative breast cancer after neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2020, 179, 11–23. [Google Scholar] [CrossRef]
- Lee, J.S.; Yost, S.E.; Yuan, Y. Neoadjuvant Treatment for Triple Negative Breast Cancer: Recent Progresses and Challenges. Cancers 2020, 12, 1404. [Google Scholar] [CrossRef]
- Dieci, M.V.; Tsvetkova, V.; Griguolo, G.; Miglietta, F.; Tasca, G.; Giorgi, C.A.; Cumerlato, E.; Massa, D.; Lo Mele, M.; Orvieto, E.; et al. Integration of tumour infiltrating lymphocytes, programmed cell-death ligand-1, CD8 and FOXP3 in prognostic models for triple-negative breast cancer: Analysis of 244 stage I-III patients treated with standard therapy. Eur J. Cancer 2020, 136, 7–15. [Google Scholar] [CrossRef]
- Bai, Y.G.; Gao, G.X.; Zhang, H.; Zhang, S.; Liu, Y.H.; Duan, X.N.; Xu, L. Prognostic value of tumor-infiltrating lymphocyte subtypes in residual tumors of patients with triple-negative breast cancer after neoadjuvant chemotherapy. Chin. Med. J. (Engl.) 2020, 133, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martinez, E.; Gil, G.L.; Benito, A.C.; Gonzalez-Billalabeitia, E.; Conesa, M.A.; Garcia Garcia, T.; Garcia-Garre, E.; Vicente, V.; Ayala de la Pena, F. Tumor-infiltrating immune cell profiles and their change after neoadjuvant chemotherapy predict response and prognosis of breast cancer. Breast Cancer Res. 2014, 16, 488. [Google Scholar] [CrossRef] [PubMed]
- Hamy, A.S.; Bonsang-Kitzis, H.; De Croze, D.; Laas, E.; Darrigues, L.; Topciu, L.; Menet, E.; Vincent-Salomon, A.; Lerebours, F.; Pierga, J.Y.; et al. Interaction between Molecular Subtypes and Stromal Immune Infiltration before and after Treatment in Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Clin. Cancer Res. 2019, 25, 6731–6741. [Google Scholar] [CrossRef] [PubMed]
- Cocco, S.; Piezzo, M.; Calabrese, A.; Cianniello, D.; Caputo, R.; Lauro, V.D.; Fusco, G.; Gioia, G.D.; Licenziato, M.; De Laurentiis, M. Biomarkers in Triple-Negative Breast Cancer: State-of-the-Art and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 4579. [Google Scholar] [CrossRef] [PubMed]
- Derouane, F.; van Marcke, C.; Berliere, M.; Gerday, A.; Fellah, L.; Leconte, I.; Van Bockstal, M.R.; Galant, C.; Corbet, C.; Duhoux, F.P. Predictive Biomarkers of Response to Neoadjuvant Chemotherapy in Breast Cancer: Current and Future Perspectives for Precision Medicine. Cancers 2022, 14, 3876. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, J.J.; Song, I.H.; Park, I.A.; Kang, J.; Yu, J.H.; Ahn, J.H.; Gong, G. Prognostic and predictive value of NanoString-based immune-related gene signatures in a neoadjuvant setting of triple-negative breast cancer: Relationship to tumor-infiltrating lymphocytes. Breast Cancer Res. Treat. 2015, 151, 619–627. [Google Scholar] [CrossRef]
- Wang, R.X.; Chen, S.; Huang, L.; Shao, Z.M. Predictive and prognostic value of Matrix metalloproteinase (MMP)-9 in neoadjuvant chemotherapy for triple-negative breast cancer patients. BMC Cancer 2018, 18, 909. [Google Scholar] [CrossRef]
- Yu, T.; Di, G. Role of tumor microenvironment in triple-negative breast cancer and its prognostic significance. Chin. J. Cancer Res. 2017, 29, 237–252. [Google Scholar] [CrossRef]
- Blaye, C.; Darbo, E.; Debled, M.; Brouste, V.; Velasco, V.; Pinard, C.; Larmonier, N.; Pellegrin, I.; Tarricone, A.; Arnedos, M.; et al. An immunological signature to predict outcome in patients with triple-negative breast cancer with residual disease after neoadjuvant chemotherapy. ESMO Open 2022, 7, 100502. [Google Scholar] [CrossRef]
- Liu, C.; Li, Y.; Xing, X.; Zhuang, J.; Wang, J.; Wang, C.; Zhang, L.; Liu, L.; Feng, F.; Li, H.; et al. Immunogenomic landscape analyses of immune molecule signature-based risk panel for patients with triple-negative breast cancer. Mol. Nucleic Acids. 2022, 28, 670–684. [Google Scholar] [CrossRef]
- Sun, X.; Zhang, T. Identification of immune-related signature for the prognosis and benefit of immunotherapy in triple-negative breast cancer. Front. Genet. 2022. [Google Scholar] [CrossRef] [PubMed]
- Araujo, J.M.; Gomez, A.C.; Aguilar, A.; Salgado, R.; Balko, J.M.; Bravo, L.; Doimi, F.; Bretel, D.; Morante, Z.; Flores, C.; et al. Effect of CCL5 expression in the recruitment of immune cells in triple negative breast cancer. Sci. Rep. 2018, 8, 4899. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, D.; Bedard, P.L.; Nahleh, Z.; Michiels, S.; Sotiriou, C.; Loi, S.; Sparano, J.A.; Ellis, M.; Hylton, N.; Zujewski, J.A.; et al. A common language in neoadjuvant breast cancer clinical trials: Proposals for standard definitions and endpoints. Lancet Oncol. 2012, 13, e240–e248. [Google Scholar] [CrossRef]
- Steinberg, G.K.; Kondziolka, D.; Wechsler, L.R.; Lunsford, L.D.; Kim, A.S.; Johnson, J.N.; Bates, D.; Poggio, G.; Case, C.; McGrogan, M.; et al. Two-year safety and clinical outcomes in chronic ischemic stroke patients after implantation of modified bone marrow-derived mesenchymal stem cells (SB623): A phase 1/2a study. J. Neurosurg. 2018, 131, 1462–1472. [Google Scholar] [CrossRef]
- Bianchetti, E.; Bates, S.J.; Carroll, S.L.; Siegelin, M.D.; Roth, K.A. Usp9X Regulates Cell Death in Malignant Peripheral Nerve Sheath Tumors. Sci. Rep. 2018, 8, 17390. [Google Scholar] [CrossRef] [PubMed]
- Baxevanis, C.N.; Fortis, S.P.; Perez, S.A. The balance between breast cancer and the immune system: Challenges for prognosis and clinical benefit from immunotherapies. Semin. Cancer Biol. 2019. [Google Scholar] [CrossRef]
- Criscitiello, C.; Bayar, M.A.; Curigliano, G.; Symmans, F.W.; Desmedt, C.; Bonnefoi, H.; Sinn, B.; Pruneri, G.; Vicier, C.; Pierga, J.Y.; et al. A gene signature to predict high tumor-infiltrating lymphocytes after neoadjuvant chemotherapy and outcome in patients with triple-negative breast cancer. Ann. Oncol. 2018, 29, 162–169. [Google Scholar] [CrossRef]
- Hill, B.S.; Sarnella, A.; D’Avino, G.; Zannetti, A. Recruitment of stromal cells into tumour microenvironment promote the metastatic spread of breast cancer. Semin. Cancer Biol. 2020, 60, 202–213. [Google Scholar] [CrossRef]
- Denkert, C.; von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.D.; et al. Tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy with or without carboplatin in human epidermal growth factor receptor 2-positive and triple-negative primary breast cancers. J. Clin. Oncol. 2015, 33, 983–991. [Google Scholar] [CrossRef]
- Mooney-Somers, J.; Lau, A.; Bateson, D.; Richters, J.; Stewart, M.; Black, K.; Nothnagle, M. Enhancing use of emergency contraceptive pills: A systematic review of women’s attitudes, beliefs, knowledge, and experiences in Australia. Health Care Women Int. 2019, 40, 174–195. [Google Scholar] [CrossRef]
- Liu, T.; Larionova, I.; Litviakov, N.; Riabov, V.; Zavyalova, M.; Tsyganov, M.; Buldakov, M.; Song, B.; Moganti, K.; Kazantseva, P.; et al. Tumor-associated macrophages in human breast cancer produce new monocyte attracting and pro-angiogenic factor YKL-39 indicative for increased metastasis after neoadjuvant chemotherapy. Oncoimmunology 2018, 7, e1436922. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, A.; Carpi, A. Immune manipulation of advanced breast cancer: An interpretative model of the relationship between immune system and tumor cell biology. Med. Res. Rev. 2009, 29, 436–471. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.A.; Hassan, H.; Vilardo, L.; Kumar, S.K.; Kumar, A.V.; Kelsch, R.; Schneider, C.; Kiesel, L.; Eich, H.T.; Zucchi, I.; et al. Syndecan-1 (CD138) modulates triple-negative breast cancer stem cell properties via regulation of LRP-6 and IL-6-mediated STAT3 signaling. PLoS ONE 2013, 8, e85737. [Google Scholar] [CrossRef] [PubMed]
- Pinder, S.E.; Brown, J.P.; Gillett, C.; Purdie, C.A.; Speirs, V.; Thompson, A.M.; Shaaban, A.M. The manufacture and assessment of tissue microarrays: Suggestions and criteria for analysis, with breast cancer as an example. J. Clin. Pathol. 2013, 66, 169–177. [Google Scholar] [CrossRef]
- Pelekanou, V.; Villarroel-Espindola, F.; Schalper, K.A.; Pusztai, L.; Rimm, D.L. CD68, CD163, and matrix metalloproteinase 9 (MMP-9) co-localization in breast tumor microenvironment predicts survival differently in ER-positive and -negative cancers. Breast Cancer Res. 2018, 20, 154. [Google Scholar] [CrossRef]
- Herlin, P.; Signolle, N. Method for Determining the Position of Tissue Sampler Chips on a Blade of Transparent Material. 2005, FR2860319B1. Available online: https://patents.google.com/patent/FR2860319B1/en/ (accessed on 5 December 2022).
- Lejeune, M.; Plancoulaine, B.; Elie, N.; Bosch, R.; Fontoura, L.; de Villasante, I.; Korzynska, A.; Navarro, A.G.; Colon, E.S.; Lopez, C. How the variability between computer-assisted analysis procedures evaluating immune markers can influence patients’ outcome prediction. Histochem Cell Biol. 2021, 156, 461–478. [Google Scholar] [CrossRef]
- Lopez, C.; Callau, C.; Bosch, R.; Korzynska, A.; Jaen, J.; Garcia-Rojo, M.; Bueno, G.; Salvado, M.T.; Alvaro, T.; Onos, M. Development of automated quantification methodologies of immunohistochemical markers to determine patterns of immune response in breast cancer: A retrospective cohort study. BMJ Open 2014, 4, e005643. [Google Scholar] [CrossRef]
- Callau, C.; Lejeune, M.; Korzynska, A.; Garcia, M.; Bueno, G.; Bosch, R.; Jaen, J.; Orero, G.; Salvado, T.; Lopez, C. Evaluation of cytokeratin-19 in breast cancer tissue samples: A comparison of automatic and manual evaluations of scanned tissue microarray cylinders. Biomed. Eng. Online 2015, 14 (Suppl. 2), S2. [Google Scholar] [CrossRef]
- Dieci, M.V.; Miglietta, F.; Guarneri, V. Immune Infiltrates in Breast Cancer: Recent Updates and Clinical Implications. Cells 2021, 10, 223. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA; National Institutes of Health (US): Bethesda, MD, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326791/ (accessed on 5 December 2022).
- da Silva, J.L.; Cardoso Nunes, N.C.; Izetti, P.; de Mesquita, G.G.; de Melo, A.C. Triple negative breast cancer: A thorough review of biomarkers. Crit Rev. Oncol. Hematol. 2020, 145, 102855. [Google Scholar] [CrossRef]
- Wang, X.X.; Jiang, Y.Z.; Li, J.J.; Song, C.G.; Shao, Z.M. Effect of nodal status on clinical outcomes of triple-negative breast cancer: A population-based study using the SEER 18 database. Oncotarget 2016, 7, 46636–46645. [Google Scholar] [CrossRef]
- Yin, L.; Shuang, H.; Sheng, C.; Liang, H.; Sun, X.J.; Yang, W.T.; Shao, Z.M. The Prognostic Value of Nodal Staging in Triple-Negative Breast Cancer—A Cohort from China. Sci. Rep. 2018, 8, 9007. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.; Gibert-Ramos, A.; Bosch, R.; Korzynska, A.; Garcia-Rojo, M.; Bueno, G.; Garcia-Fontgivell, J.F.; Martinez Gonzalez, S.; Fontoura, L.; Gras Navarro, A.; et al. Differences in the Immune Response of the Nonmetastatic Axillary Lymph Nodes between Triple-Negative and Luminal A Breast Cancer Surrogate Subtypes. Am. J. Pathol. 2021, 191, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Volm, M.D.; Shapiro, R.L.; Yee, H.T.; Oratz, R.; Formenti, S.C.; Muggia, F.; Symmans, W.F. Development of tumor-infiltrating lymphocytes in breast cancer after neoadjuvant paclitaxel chemotherapy. Clin. Cancer Res. 2001, 7, 3025–3030. [Google Scholar]
- da Silva, J.L.; de Albuquerque, L.Z.; Rodrigues, F.R.; de Mesquita, G.G.; Fernandes, P.V.; Thuler, L.C.S.; de Melo, A.C. Prognostic Influence of Residual Tumor-Infiltrating Lymphocyte Subtype After Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer. Front. Oncol. 2021, 11, 636716. [Google Scholar] [CrossRef]
- Gao, G.; Wang, Z.; Qu, X.; Zhang, Z. Prognostic value of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer: A systematic review and meta-analysis. BMC Cancer 2020, 20, 179. [Google Scholar] [CrossRef]
- Kaewkangsadan, V.; Verma, C.; Eremin, J.M.; Cowley, G.; Ilyas, M.; Eremin, O. Crucial Contributions by T Lymphocytes (Effector, Regulatory, and Checkpoint Inhibitor) and Cytokines (TH1, TH2, and TH17) to a Pathological Complete Response Induced by Neoadjuvant Chemotherapy in Women with Breast Cancer. J. Immunol. Res. 2016, 2016, 4757405. [Google Scholar] [CrossRef]
- Abdelrahman, A.E.; Rashed, H.E.; Toam, M.; Omar, A.; Abdelhamid, M.I.; Matar, I. Clinicopathological significance of the immunologic signature (PDL1, FOXP3+ Tregs, TILs) in early stage triple-negative breast cancer treated with neoadjuvant chemotherapy. Ann. Diagn Pathol. 2021, 51, 151676. [Google Scholar] [CrossRef]
- Bates, G.J.; Fox, S.B.; Han, C.; Leek, R.D.; Garcia, J.F.; Harris, A.L.; Banham, A.H. Quantification of regulatory T cells enables the identification of high-risk breast cancer patients and those at risk of late relapse. J. Clin. Oncol. 2006, 24, 5373–5380. [Google Scholar] [CrossRef]
- Aptsiauri, N.; Ruiz-Cabello, F.; Garrido, F. The transition from HLA-I positive to HLA-I negative primary tumors: The road to escape from T-cell responses. Curr. Opin. Immunol. 2018, 51, 123–132. [Google Scholar] [CrossRef]
- Perez-Pena, J.; Tibor Fekete, J.; Paez, R.; Baliu-Pique, M.; Garcia-Saenz, J.A.; Garcia-Barberan, V.; Manzano, A.; Perez-Segura, P.; Esparis-Ogando, A.; Pandiella, A.; et al. A Transcriptomic Immunologic Signature Predicts Favorable Outcome in Neoadjuvant Chemotherapy Treated Triple Negative Breast Tumors. Front. Immunol. 2019, 10, 2802. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Ishigami, S.; Kijima, Y.; Funasako, Y.; Hirata, M.; Okumura, H.; Shinchi, H.; Koriyama, C.; Ueno, S.; Yoshinaka, H.; et al. Clinical implication of HLA class I expression in breast cancer. BMC Cancer 2011, 11, 454. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.B.; Kim, Y.A.; Seo, J.H.; Lee, H.J.; Gong, G.; Park, S.H. Prediction of prognostic signatures in triple-negative breast cancer based on the differential expression analysis via NanoString nCounter immune panel. BMC Cancer 2020, 20, 1052. [Google Scholar] [CrossRef] [PubMed]
- Szpor, J.; Streb, J.; Glajcar, A.; Fraczek, P.; Winiarska, A.; Tyrak, K.E.; Basta, P.; Okon, K.; Jach, R.; Hodorowicz-Zaniewska, D. Dendritic Cells Are Associated with Prognosis and Survival in Breast Cancer. Diagnostics 2021, 11, 702. [Google Scholar] [CrossRef]
- Liu, Y.; Teng, L.; Fu, S.; Wang, G.; Li, Z.; Ding, C.; Wang, H.; Bi, L. Highly heterogeneous-related genes of triple-negative breast cancer: Potential diagnostic and prognostic biomarkers. BMC Cancer 2021, 21, 644. [Google Scholar] [CrossRef]
- Goode, G.; Gunda, V.; Chaika, N.V.; Purohit, V.; Yu, F.; Singh, P.K. MUC1 facilitates metabolomic reprogramming in triple-negative breast cancer. PLoS ONE 2017, 12, e0176820. [Google Scholar]
- Maeda, T.; Hiraki, M.; Jin, C.; Rajabi, H.; Tagde, A.; Alam, M.; Bouillez, A.; Hu, X.; Suzuki, Y.; Miyo, M.; et al. MUC1-C Induces PD-L1 and Immune Evasion in Triple-Negative Breast Cancer. Cancer Res. 2018, 78, 205–215. [Google Scholar] [CrossRef]
- Atta Manu, E.; Bedu-Addo, K.; Titiloye, N.A.; Ameh-Mensah, C.; Opoku, F.; Duduyemi, B.M. Expression of Tumour-Associated MUC1 Is a Poor Prognostic Marker in Breast Cancer in Kumasi, Ghana. J. Oncol. 2020, 2020, 9752952. [Google Scholar] [CrossRef]
- Jing, X.; Liang, H.; Hao, C.; Yang, X.; Cui, X. Overexpression of MUC1 predicts poor prognosis in patients with breast cancer. Oncol. Rep. 2019, 41, 801–810. [Google Scholar] [CrossRef]
- Schmidt, M.; Weyer-Elberich, V.; Hengstler, J.G.; Heimes, A.S.; Almstedt, K.; Gerhold-Ay, A.; Lebrecht, A.; Battista, M.J.; Hasenburg, A.; Sahin, U.; et al. Prognostic impact of CD4-positive T cell subsets in early breast cancer: A study based on the FinHer trial patient population. Breast Cancer Res. 2018, 20, 15. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 96) | Non-Relapsed (n = 54) | Relapsed (n = 41) | p | Alive (n = 59) | Dead (n = 37) | p | |
|---|---|---|---|---|---|---|---|
| Age Years, median (IQR) | 51 (26) | 51 (26) | 52 (28) | 0.473* | 51 (26) | 55 (28) | 0.660 * |
| Menopausal status Pre-menopausal Menopausal | 35 (44.9%) 43 (55.1%) | 20 (45.5%) 24 (54.5%) | 15 (45.5%) 18 (54.5%) | 1.000 Ɨ | 21 (44.7%) 26 (55.3%) | 14 (45.2%) 17 (54.8%) | 1.000 Ɨ |
| Histological grade <3 =3 | 17 (18.5%) 75 (81.5%) | 9 (17.6%) 42 (82.4%) | 8 (20.0%) 32 (80.0%) | 0.988 Ɨ | 13 (23.2%) 43 (76.8%) | 4 (11.1%) 32 (88.9%) | 0.236 Ɨ |
| Tumor diameter mm, median (IQR) | 25.00 (22.00) | 22.00 (25.00) | 30.00 (25.00) | 0.011 * | 22.00 (23.00) | 30.00 (20.00) | 0.021 * |
| Nodal status Negative Positive | 41 (43.6%) 53 (56.4%) | 29 (55.8%) 23 (44.2%) | 12 (29.3%) 29 (70.7%) | 0.019 Ɨ | 32 (56.1%) 25 (43.9%) | 9 (24.3%) 28 (75.7%) | 0.005 Ɨ |
| Ki67 degree ≤30% >30% | 24 (27.9%) 62 (72.1%) | 10 (20.0%) 40 (80.0%) | 14 (40.0%) 21 (60.0%) | 0.077 Ɨ | 14 (26.4%) 39 (73.6%) | 10 (30.3%) 23 (69.7%) | 0.886 Ɨ |
| Pathological response Partial response Without response | 63 (65.6%) 33 (34.4%) | 40 (74.1%) 14 (25.9%) | 23 (56.1%) 18 (43.9%) | 0.106 Ɨ | 42 (71.2%) 17 (28.8%) | 21 (56.8%) 16 (43.2%) | 0.219 Ɨ |
| Surgery Tumorectomy Mastectomy No lymphadenectomy Lymphadenectomy | 36 (38.3%) 58 (61.7%) 20 (21.3%) 74 (78.7%) | 21 (40.4%) 31 (59.6%) 13 (25.0%) 39 (75.0%) | 14 (34.1%) 27 (65.9%) 7 (17.1%) 34 (82.9%) | 0.688 Ɨ 0.503 Ɨ | 25 (43.9%) 32 (56.1%) 14 (24.6%) 43 (75.4%) | 11 (29.7%) 26 (70.3%) 6 (16.2%) 31 (83.8%) | 0.246 Ɨ 0.479 Ɨ |
| Adjuvant chemotherapy No Yes | 77 (82.8%) 16 (17.2%) | 42 (80.8%) 10 (19.2%) | 35 (87.5%) 5 (12.5%) | 0.561 Ɨ | 47 (82.5%) 10 (17.5%) | 30 (83.3%) 6 (16.7%) | 1.000 Ɨ |
| Adjuvant radiotherapy No Yes | 4 (4.5%) 84 (95.5%) | 3 (6.0%) 47 (94.0%) | 1 (2.6%) 37 (97.4%) | 0.631 Ɨ | 3 (5.5%) 52 (94.5%) | 1 (3.0%) 32 (97.0%) | 1.000 Ɨ |
| Relapse No Yes | 54 (56.8%) 41 (43.2%) | - | - | - | 52 (88.1%) 7 (11.9%) | 2 (5.6%) 34 (94.4%) | <0.001 Ɨ |
| Overall survival Months, median (IQR) | 47.32 (38.10) | 60.00 (14.60) | 25.07 (25.65) | <0.001 * | - | - | - |
| Relapse-free survival Months, median (IQR) | 40.67 (46.89) | - | - | - | 60.00 (16.13) | 13.73 (14.88) | <0.001 * |
| Survival status Alive Dead | 59 (61.5%) 37 (38.5%) | 52 (96.3%) 2 (3.7%) | 7 (17.1%) 34 (82.9%) | <0.001 Ɨ | - | - | - |
| Non-Relapsed (n = 54) | Relapsed (n = 41) | p | Alive (n = 59) | Death (n = 37) | p | |
|---|---|---|---|---|---|---|
| CD4+ T lymphocytes | 0.85 (2.29) | 0.28 (0.97) | 0.004 * | 0.86 (2.33) | 0.30 (0.74) | 0.004 * |
| CD8+ T lymphocytes | 0.81 (2.08) | 0.37 (0.89) | 0.051 * | 0.79 (1.95) | 0.37 (0.80) | 0.055 * |
| FOXP3+ regulatory T cells | 0.06 (0.19) | 0.03 (0.06) | 0.004 * | 0.06 (0.19) | 0.03 (0.06) | 0.020 * |
| CD57+ NK cells | 0.02 (0.06) | 0.05 (0.39) | 0.093 * | 0.03 (0.09) | 0.03 (0.32) | 0.698 * |
| CD68+ macrophages | 1.72 (2.53) | 1.42 (2.55) | 0.604 * | 1.91 (3.48) | 1.39 (2.35) | 0.418 * |
| CD1a+ dendritic cells | 0.12 (0.43) | 0.07 (0.18) | 0.032 * | 0.12 (0.41) | 0.07 (0.18) | 0.053 * |
| CD21+ dendritic cells | 0.001 (0.009) | 0.000 (0.002) | 0.002 * | 0.001 (0.007) | 0.000 (0.002) | 0.013 * |
| CD83+ dendritic cells | 0.07 (0.18) | 0.03 (0.11) | 0.103 * | 0.06 (0.17) | 0.03 (0.11) | 0.201 * |
| CD15+ granulocytes | 1.05 (4.60) | 2.27 (5.28) | 0.523 * | 1.17 (4.74) | 1.51 (4.53) | 0.836 * |
| HLA-DR+ APC | 14.94 (28.17) | 9.63 (12.32) | 0.101 * | 14.86 (28.64) | 9.63 (11.35) | 0.156 * |
| CD31+ endothelial cells | 1.35 (2.81) | 1.18 (1.90) | 0.173 * | 1.37 (2.81) | 1.15 (1.73) | 0.114 * |
| CD34+ endothelial cells | 1.88 (1.69) | 1.90 (1.61) | 0.921 * | 2.11 (1.87) | 1.86 (1.16) | 0.407 * |
| CD138+ cells | 26.25 (34.49) | 25.76 (37.63) | 0.940 * | 23.84 (35.42) | 27.49 (38.88) | 0.454 * |
| CXCL13 Absence Presence | 20 (40.8%) 29 (59.2%) | 25 (64.1%) 14 (35.9%) | 0.050 Ɨ | 24 (44.4%) 30 (55.6%) | 22 (62.9%) 13 (37.1%) | 0.139 Ɨ |
| IL6 Absence Presence | 16 (33.3%) 32 (66.7%) | 14 (36.8%) 24 (63.2%) | 0.911 Ɨ | 18 (34.0%) 35 (66.0%) | 12 (35.3%) 22 (64.7%) | 1.000 Ɨ |
| IL10 Absence Presence | 42 (85.7%) 7 (14.3%) | 35 (89.7%) 4 (10.3%) | 0.748 Ɨ | 46 (85.2%) 8 (14.8%) | 32 (91.4%) 3 (8.6%) | 0.516 Ɨ |
| IL15 Absence Presence | 22 (46.8%) 25 (53.2%) | 22 (57.9%) 16 (42.1%) | 0.424 Ɨ | 25 (48.1%) 27 (51.9%) | 19 (55.9%) 15 (44.1%) | 0.626 Ɨ |
| MMP1 Absence Presence | 29 (59.2%) 20 (40.8%) | 27 (71.1%) 11 (28.9%) | 0.357 Ɨ | 35 (64.8%) 19 (35.2%) | 22 (64.7%) 12 (35.3%) | 1.000 Ɨ |
| MMP9 Absence Presence | 14 (29.2%) 34 (70.8%) | 15 (39.5%) 23 (60.5%) | 0.439 Ɨ | 17 (32.1%) 36 (67.9%) | 12 (35.3%) 22 (64.7%) | 0.938 Ɨ |
| MMP12 Absence Presence | 36 (78.3%) 10 (21.7%) | 34 (89.5%) 4 (10.5%) | 0.281 Ɨ | 41 (80.4%) 10 (19.6%) | 30 (88.2%) 4 (11.8%) | 0.511 Ɨ |
| MUC1 Absence Presence | 23 (46.9%) 26 (53.1%) | 13 (34.2%) 25 (65.8%) | 0.329 Ɨ | 27 (50.0%) 27 (50.0%) | 9 (26.5%) 25 (73.5%) | 0.050 Ɨ |
| TNF-α Absence Presence | 30 (57.7%) 22 (42.3%) | 22 (57.9%) 16 (42.1%) | 1.000 Ɨ | 33 (57.9%) 24 (42.1%) | 19 (55.9%) 15 (44.1%) | 1.000 Ɨ |
| Univariate Analysis | Multivariate Analysis | Multivariate Analysis after Bootstraping | ||||
|---|---|---|---|---|---|---|
| Variables Associated with OS | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p |
| Tumor diameter | 1.018 (1.004–1.032) | 0.009 | - | - | - | - |
| Nodal status at baseline Positive Negative | 3.154 (1.485–6.699) 1.0 | 0.003 | 4.061 (1.653–9.973) 1.0 | 0.002 | 2.869 (1.335–6.168) 1.0 | 0.007 |
| CD4 | 0.746 (0.566–0.983) | 0.038 | 0.642 (0.435–0.950) | 0.027 | 0.773 (0.601–0.994) | 0.083 |
| CD8 | 0.816 (0.651–1.024) | 0.079 | - | - | - | - |
| FOXP3 | 0.012 (0.000–0.583) | 0.026 | - | - | - | - |
| HLA-DR | 0.981 (0.962–1.000) | 0.049 | - | - | - | - |
| CD31 | 0.793 (0.631–0.997) | 0.047 | - | - | - | - |
| MUC1 Presence Absence | 2.472 (1.153–5.301) 1.0 | 0.020 | 2.296 (1.049–5.026) 1.0 | 0.038 | 2.655 (1.237–5.697) 1.0 | 0.006 |
| Variables associated with RFS | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p |
| Tumor diameter | 1.018 (1.006–1.031) | 0.004 | 1.014 (1.001–1.028) | 0.036 | 1.014 (1.001–1.028) | 0.036 |
| Nodal status at baseline Positive Negative | 2.509 (1.276–4.933) 1.0 | 0.008 | 2.749 (1.270–5.954) 1.0 | 0.010 | 2.749 (1.270–5.954) 1.0 | 0.008 |
| Response Partial Without | 1.766 (0.951–3.279) 1.0 | 0.072 | - | - | - | - |
| CD4 | 0.792 (0.633–0.992) | 0.042 | - | - | - | - |
| CD8 | 0.815 (0.660–1.007) | 0.058 | - | - | - | - |
| FOXP3 | 0.007 (0.000–0.334) | 0.012 | - | - | - | - |
| CD83 | 0.120 (0.010–1.437) | 0.094 | - | - | - | - |
| CD15 | 1.042 (0.993–1.094) | 0.097 | - | - | - | - |
| HLA-DR | 0.982 (0.965–0.999) | 0.043 | - | - | - | - |
| CD31 | 0.820 (0.673–0.999) | 0.049 | - | - | - | - |
| CXCL13 Presence Absence | 0.510 (0.265–0.982) 1.0 | 0.044 | 0.453 (0.220–0.933) 1.0 | 0.032 | 0.453 (0.220–0.933) 1.0 | 0.028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lejeune, M.; Reverté, L.; Sauras, E.; Gallardo, N.; Bosch, R.; Roso, A.; Petit, A.; Peg, V.; Riu, F.; García-Fontgivell, J.; et al. Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response. Cancers 2023, 15, 597. https://doi.org/10.3390/cancers15030597
Lejeune M, Reverté L, Sauras E, Gallardo N, Bosch R, Roso A, Petit A, Peg V, Riu F, García-Fontgivell J, et al. Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response. Cancers. 2023; 15(3):597. https://doi.org/10.3390/cancers15030597
Chicago/Turabian StyleLejeune, Marylène, Laia Reverté, Esther Sauras, Noèlia Gallardo, Ramon Bosch, Albert Roso, Anna Petit, Vicente Peg, Francisco Riu, Joan García-Fontgivell, and et al. 2023. "Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response" Cancers 15, no. 3: 597. https://doi.org/10.3390/cancers15030597
APA StyleLejeune, M., Reverté, L., Sauras, E., Gallardo, N., Bosch, R., Roso, A., Petit, A., Peg, V., Riu, F., García-Fontgivell, J., Ibáñez, J., Relea, F., Vieites, B., Bor, C., de la Cruz-Merino, L., Arenas, M., Rodriguez, V., Galera, J., Korzynska, A., ... López, C. (2023). Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response. Cancers, 15(3), 597. https://doi.org/10.3390/cancers15030597