Evaluation of a Balloon Implant for Simultaneous Magnetic Nanoparticle Hyperthermia and High-Dose-Rate Brachytherapy of Brain Tumor Resection Cavities

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Thermobrachytherapy System Components
2.1.1. TBT Balloon Implant
2.1.2. Nanofluid and Magnetic Field Generator
2.1.3. Fiber Optic Thermometry System
2.1.4. HDR Brachytherapy System
2.2. Laboratory Studies of TBT Balloon Implant in Phantom
2.2.1. Human Skull Model and Brain-Tissue-Equivalent Gel Phantom
2.2.2. Thermal Dosimetry Measurements
2.2.3. Radiation Dosimetry Measurements
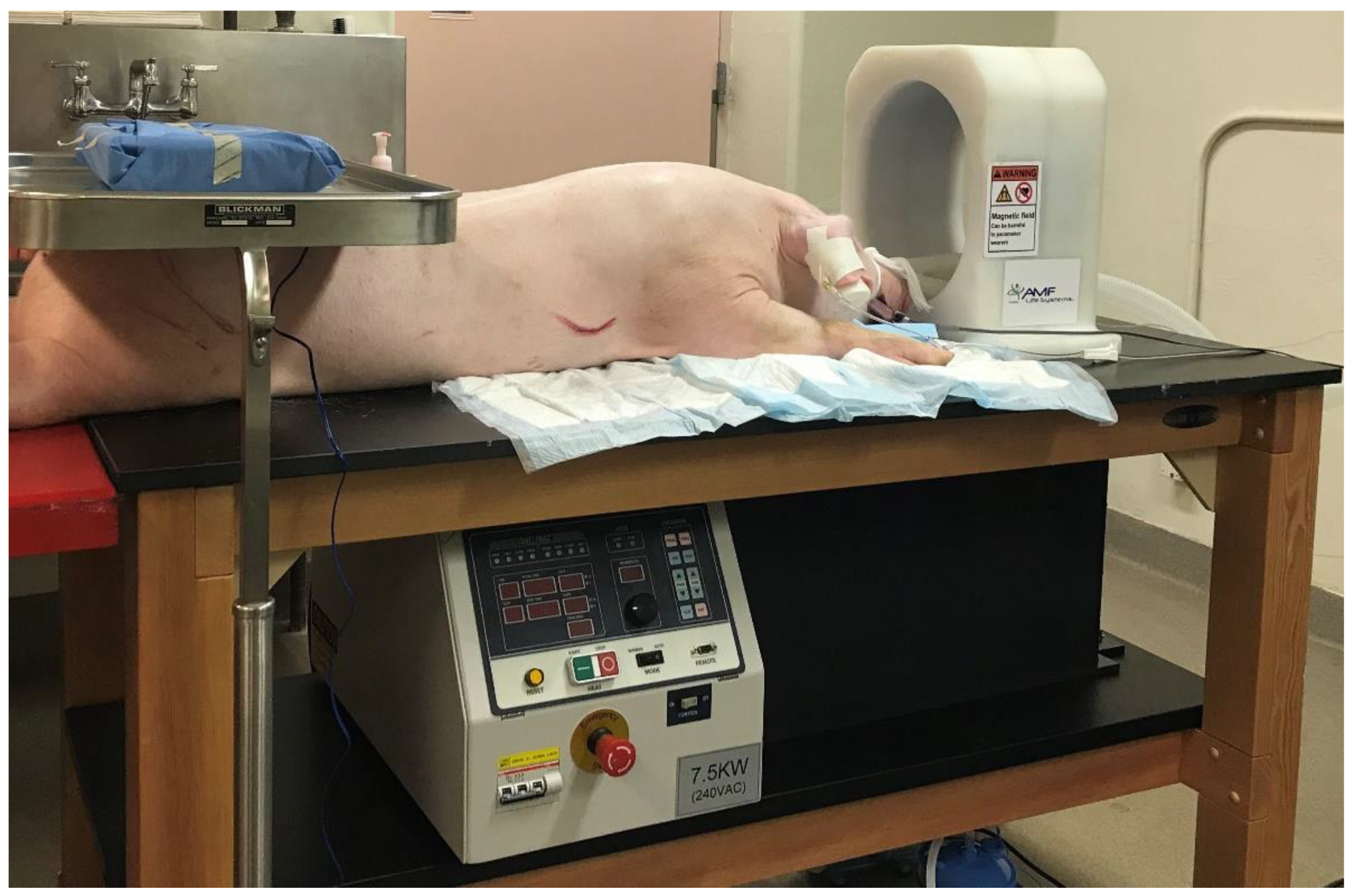
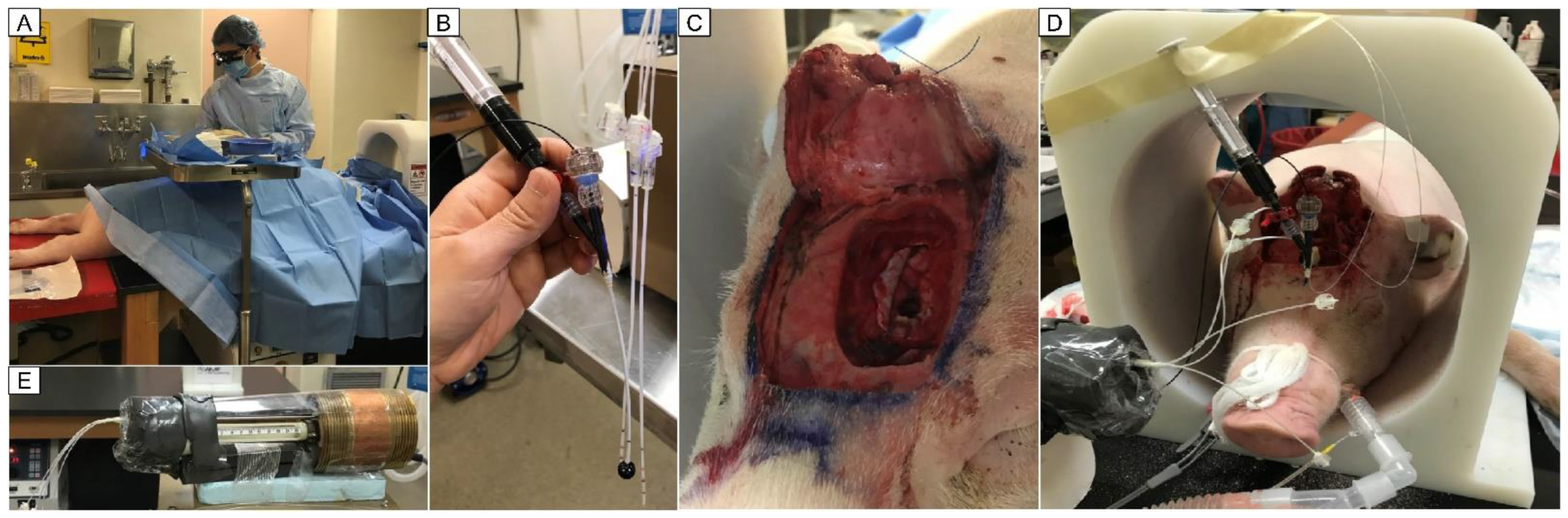
2.3. In Vivo Experiments of TBT Balloon Implant in Pig Brain
3. Results
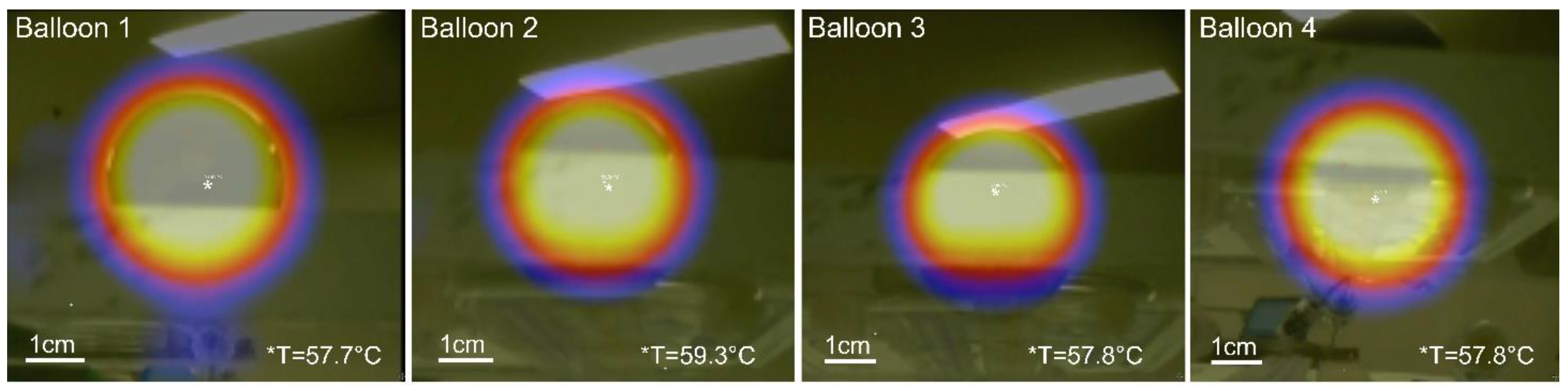
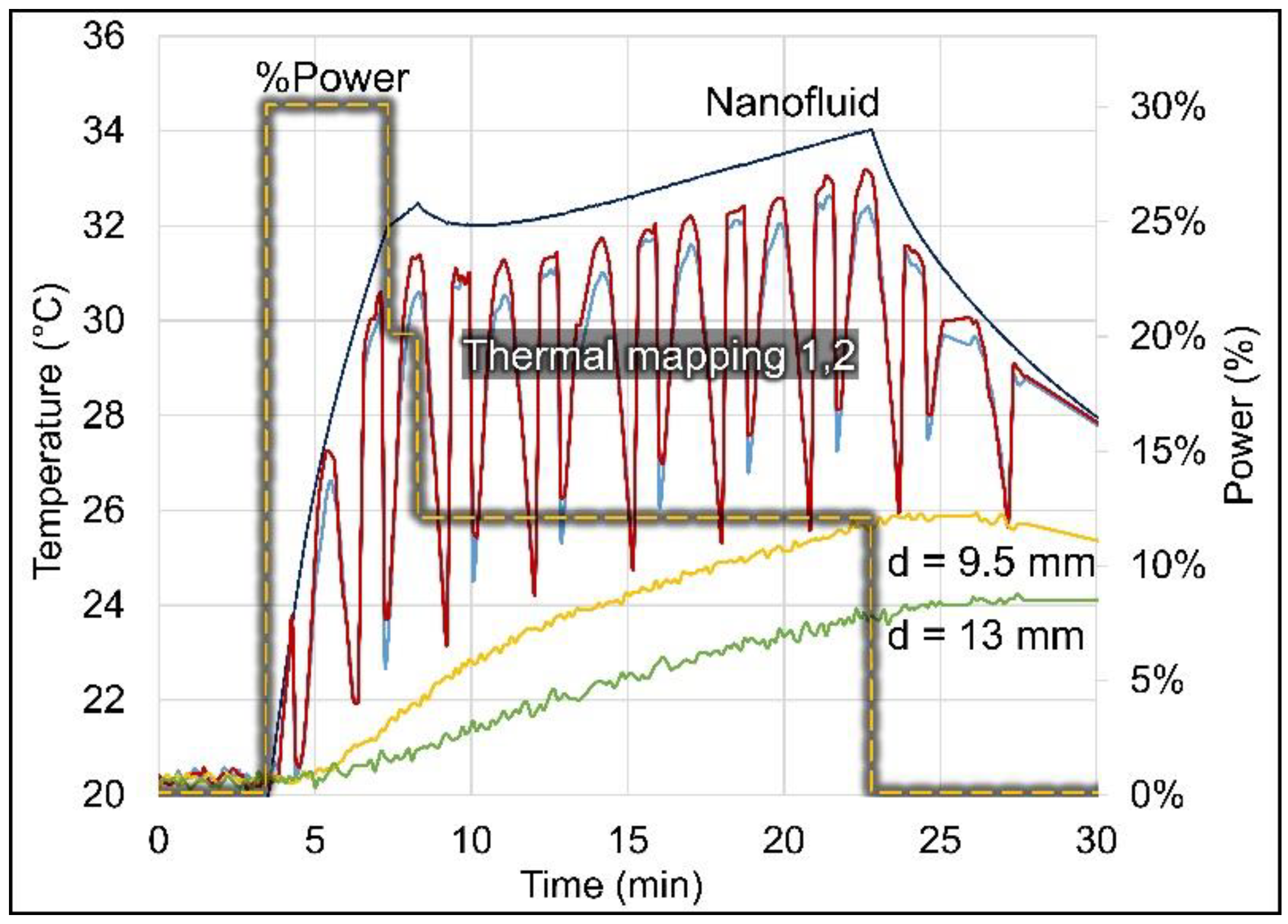
3.1. Thermal Dosimetry in Phantom
3.2. Compatibility of MNP Hyperthermia and HDR Brachytherapy
3.2.1. Effect of Nanofluid on Radiation Dosimetry
3.2.2. Effect of Magnetic Field and Balloon Heating on Radiation Dosimetry
3.3. Thermal Dosimetry in Pig Brain
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petrecca, K.; Guiot, M.-C.; Panet-Raymond, V.; Souhami, L. Failure pattern following complete resection plus radiotherapy and temozolomide is at the resection margin in patients with glioblastoma. J. Neurooncol. 2013, 111, 19–23. [Google Scholar] [CrossRef]
- McDonald, M.W.; Shu, H.K.; Curran, W.J., Jr.; Crocker, I.R. Pattern of failure after limited margin radiotherapy and temozolomide for glioblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Rapp, M.; Baernreuther, J.; Turowski, B.; Steiger, H.J.; Sabel, M.; Kamp, M.A. Recurrence Pattern Analysis of Primary Glioblastoma. World Neurosurg. 2017, 103, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lopez, P.D.; Corrales-Garcia, E.M. Survival in glioblastoma: A review on the impact of treatment modalities. Clin. Transl. Oncol. 2016, 18, 1062–1071. [Google Scholar] [CrossRef]
- Mohile, N.A.; Messersmith, H.; Gatson, N.T.; Hottinger, A.F.; Lassman, A.; Morton, J.; Ney, D.; Nghiemphu, P.L.; Olar, A.; Olson, J.; et al. Therapy for Diffuse Astrocytic and Oligodendroglial Tumors in Adults: ASCO-SNO Guideline. J. Clin. Oncol. 2022, 40, 403–426. [Google Scholar] [CrossRef]
- Overgaard, J. The current and potential role of hyperthermia in radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1989, 16, 535–549. [Google Scholar] [CrossRef]
- Datta, N.R.; Ordóñez, S.G.; Gaipl, U.S.; Paulides, M.M.; Crezee, H.; Gellermann, J.; Marder, D.; Puric, E.; Bodis, S. Local hyperthermia combined with radiotherapy and-/or chemotherapy: Recent advances and promises for the future. Cancer Treat. Rev. 2015, 41, 742–753. [Google Scholar] [CrossRef]
- Horsman, M.R.; Overgaard, J. Hyperthermia: A potent enhancer of radiotherapy. Clin. Oncol. 2007, 19, 418–426. [Google Scholar] [CrossRef]
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P.M. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef]
- Peeken, J.C.; Vaupel, P.; Combs, S.E. Integrating Hyperthermia into Modern Radiation Oncology: What Evidence Is Necessary? Front. Oncol. 2017, 7, 132. [Google Scholar] [CrossRef]
- Stea, B.; Kittelson, J.; Cassady, J.R.; Hamilton, A.; Guthkelch, N.; Lulu, B.; Obbens, E.; Rossman, K.; Shapiro, W.; Shetter, A.; et al. Treatment of malignant gliomas with interstitial irradiation and hyperthermia. Int. J. Radiat. Oncol. Biol. Phys. 1992, 24, 657–667. [Google Scholar] [CrossRef]
- Stea, B.; Rossman, K.; Kittelson, J.; Shetter, A.; Hamilton, A.; Cassady, J.R. Interstitial irradiation versus interstitial thermoradiotherapy for supratentorial malignant gliomas: A comparative survival analysis. Int. J. Radiat. Oncol. Biol. Phys. 1994, 30, 591–600. [Google Scholar] [CrossRef]
- Maier-Hauff, K.; Rothe, R.; Scholz, R.; Gneveckow, U.; Wust, P.; Thiesen, B.; Feussner, A.; von Deimling, A.; Waldoefner, N.; Felix, R.; et al. Intracranial thermotherapy using magnetic nanoparticles combined with external beam radiotherapy: Results of a feasibility study on patients with glioblastoma multiforme. J. Neurooncol. 2007, 81, 53–60. [Google Scholar] [CrossRef]
- Maier-Hauff, K.; Ulrich, F.; Nestler, D.; Niehoff, H.; Wust, P.; Thiesen, B.; Orawa, H.; Budach, V.; Jordan, A. Efficacy and safety of intratumoral thermotherapy using magnetic iron-oxide nanoparticles combined with external beam radiotherapy on patients with recurrent glioblastoma multiforme. J. Neurooncol. 2011, 103, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Strohbehn, J.W.; Coughlin, C.T.; Ryan, T.P.; Lyons, B.E.; Douple, E.B. Iridium-192 brachytherapy in combination with interstitial microwave-induced hyperthermia for malignant glioma. Appl. Neurophysiol. 1987, 50, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Sneed, P.K.; Stauffer, P.R.; McDermott, M.W.; Diederich, C.J.; Lamborn, K.R.; Prados, M.D.; Chang, S.; Weaver, K.A.; Spry, L.; Malec, M.K.; et al. Survival benefit of hyperthermia in a prospective randomized trial of brachytherapy boost +/− hyperthermia for glioblastoma multiforme. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef]
- Sneed, P.K.; Stauffer, P.R.; Gutin, P.H.; Phillips, T.L.; Suen, S.; Weaver, K.A.; Lamb, S.A.; Ham, B.; Prados, M.D.; Larson, D.A.; et al. Interstitial irradiation and hyperthermia for the treatment of recurrent malignant brain tumors. Neurosurgery 1991, 28, 206–215. [Google Scholar] [CrossRef]
- Hulshof, M.C.; Raaymakers, B.W.; Lagendijk, J.J.; Koot, R.W.; Crezee, H.; Stalpers, L.J.; Gonzalez Gonzalez, D. A feasibility study of interstitial hyperthermia plus external beam radiotherapy in glioblastoma multiforme using the Multi ELectrode Current Source (MECS) system. Int. J. Hyperth. 2004, 20, 451–463. [Google Scholar] [CrossRef]
- Fike, J.R.; Gobbel, G.T.; Satoh, T.; Stauffer, P.R. Normal brain response after interstitial microwave hyperthermia. Int. J. Hyperth. 1991, 7, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Marchosky, J.A.; Welsh, D.M.; Moran, C.J. Hyperthermia treatment of brain tumors. Mo. Med. 1990, 87, 29–33. [Google Scholar] [PubMed]
- De Bree, J.; Lagendijk, J.J.; Raaymakers, B.W.; Bakker, C.J.; Hulshof, M.C.; Koot, R.W.; Hanlo, P.W.; Struikmans, H.; Ramos, L.M.; Battermann, J.J. Treatment planning of brain implants using vascular information and a new template technique. IEEE Trans. Med. Imaging 1998, 17, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Deurloo, I.K.K.; Visser, A.G.; Morawska, M.; van Geel, C.A.J.F.; van Rhoon, G.C.; Levendag, P.C. Application of a capacitive-coupling interstitial hyperthermia system at 27 MHz: Study of different applicator configurations. Phys. Med. Biol. 1991, 36, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Crezee, J.; Kaatee, R.S.; van der Koijk, J.F.; Lagendijk, J.J. Spatial steering with quadruple electrodes in 27 MHz capacitively coupled interstitial hyperthermia. Int. J. Hyperth. 1999, 15, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.P.; Trembly, B.S.; Roberts, D.W.; Strohbehn, J.W.; Coughlin, C.T.; Hoopes, P.J. Brain hyperthermia: I. Interstitial microwave antenna array techniques—The Dartmouth experience. Int. J. Radiat. Oncol. Biol. Phys. 1994, 29, 1065–1078. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Stauffer, P.R.; Fike, J.R. Thermal distribution studies of helical coil microwave antennas for interstitial hyperthermia. Int. J. Radiat. Oncol. Biol. Phys. 1988, 15, 1209–1218. [Google Scholar] [CrossRef]
- Satoh, T.; Seilhan, T.M.; Stauffer, P.R.; Sneed, P.K.; Fike, J.R. Interstitial helical coil microwave antenna for experimental brain hyperthermia. Neurosurgery 1988, 23, 564–569. [Google Scholar] [CrossRef]
- Sneed, P.K.; Matsumoto, K.; Stauffer, P.R.; Fike, J.R.; Smith, V.; Gutin, P.H. Interstitial microwave hyperthermia in a canine brain model. Int. J. Radiat. Oncol. Biol. Phys. 1986, 12, 1887–1897. [Google Scholar] [CrossRef]
- Marchosky, J.A.; Moran, C.J.; Fearnot, N.E.; Babbs, C.F. Hyperthermia catheter implantation and therapy in the brain. J. Neurosurg. 1990, 72, 975–979. [Google Scholar] [CrossRef]
- DeFord, J.A.; Babbs, C.F.; Patel, U.H.; Fearnot, N.E.; Marchosky, J.A.; Moran, C.J. Accuracy and precision of computer-simulated tissue temperatures in individual human intracranial tumours treated with interstitial hyperthermia. Int. J. Hyperth. 1990, 6, 755–769. [Google Scholar] [CrossRef]
- Stea, B.; Cetas, T.C.; Cassady, J.R.; Guthkelch, A.N.; Iacono, R.; Lulu, B.; Lutz, W.; Obbens, E.; Rossman, K.; Seeger, J.; et al. Interstitial thermoradiotherapy of brain tumors: Preliminary results of a phase I clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 1990, 19, 1463–1471. [Google Scholar] [CrossRef]
- Stauffer, P.R.; Cetas, T.C.; Fletcher, A.M.; DeYoung, D.W.; Dewhirst, M.W.; Oleson, J.R.; Roemer, R.B. Observations on the use of ferromagnetic implants for inducing hyperthermia. IEEE Trans. Biomed. Eng. 1984, 31, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.; Maier-Hauff, K. Magnetic nanoparticles for intracranial thermotherapy. J. Nanosci. Nanotechnol. 2007, 7, 4604–4606. [Google Scholar] [CrossRef] [PubMed]
- Thiesen, B.; Jordan, A. Clinical applications of magnetic nanoparticles for hyperthermia. Int. J. Hyperth. 2008, 24, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.; Belmonte-Reche, E.; Gallo, J.; Baltazar, F.; Banobre-Lopez, M. Magnetic Solid Nanoparticles and Their Counterparts: Recent Advances towards Cancer Theranostics. Pharmaceutics 2022, 14, 506. [Google Scholar] [CrossRef] [PubMed]
- Soares, G.A.; Pereira, G.M.; Romualdo, G.R.; Biasotti, G.G.A.; Stoppa, E.G.; Bakuzis, A.F.; Baffa, O.; Barbisan, L.F.; Miranda, J.R.A. Biodistribution Profile of Magnetic Nanoparticles in Cirrhosis-Associated Hepatocarcinogenesis in Rats by AC Biosusceptometry. Pharmaceutics 2022, 14, 1907. [Google Scholar] [CrossRef]
- Kok, H.P.; Cressman, E.N.K.; Ceelen, W.; Brace, C.L.; Ivkov, R.; Grull, H.; Ter Haar, G.; Wust, P.; Crezee, J. Heating technology for malignant tumors: A review. Int. J. Hyperth. 2020, 37, 711–741. [Google Scholar] [CrossRef]
- Stauffer, P.R. Evolving technology for thermal therapy of cancer. Int. J. Hyperthermia 2005, 21, 731–744. [Google Scholar] [CrossRef]
- Stauffer, P.R.; Diederich, C.J.; Seegenschmiedt, M.H. Interstitial heating technologies, In Thermoradiotherapy and Thermochemotherapy: Biology, Physiology, Physics, 2nd ed.; Seegenschmiedt, M.H., Fessenden, P., Vernon, C.C., Eds.; Springer: Berlin/Heidelberg, Germany, 1995; Volume 1, pp. 279–320. [Google Scholar]
- Overgaard, J. Simultaneous and sequential hyperthermia and radiation treatment of an experimental tumor and its surrounding normal tissue in vivo. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 1507–1517. [Google Scholar] [CrossRef]
- Stauffer, P.R.; Rodrigues, D.B.; Goldstein, R.; Nguyen, T.; Yu, Y.; Wan, S.; Woodward, R.; Gibbs, M.; Vasilchenko, I.L.; Osintsev, A.M.; et al. Feasibility of removable balloon implant for simultaneous magnetic nanoparticle heating and HDR brachytherapy of brain tumor resection cavities. Int. J. Hyperth. 2020, 37, 1189–1201. [Google Scholar] [CrossRef]
- Goldstein, R. Induction Coil for Low Radiofrequency Applications in a Human Head. US Patent US 10,286,223 B2, 14 May 2019. [Google Scholar]
- Sapareto, S.A.; Dewey, W.C. Thermal dose determination in cancer therapy. Int. J. Radiat. Oncol. Biol. Phys. 1984, 10, 787–800. [Google Scholar] [CrossRef]
- Stauffer, P.R.; Cetas, T.C.; Jones, R.C. Magnetic induction heating of ferromagnetic implants for inducing localized hyperthermia in deep-seated tumors. IEEE Trans. Biomed. Eng. 1984, 31, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.B.; Maccarini, P.F.; Salahi, S.; Oliveira, T.R.; Pereira, P.J.S.; Limao-Vieira, P.; Snow, B.W.; Reudink, D.; Stauffer, P.R. Design and optimization of an ultra wideband and compact microwave antenna for radiometric monitoring of brain temperature. IEEE Trans. Biomed. Eng. 2014, 61, 2154–2160. [Google Scholar] [CrossRef]
- Williamson, J.F.; Brenner, D.J. Physics and Biology of Brachytherapy. In Perez and Brady’s Principles and Practice of Radiation Oncology, 7th ed.; Halperin, E.C., Wazer, D.E., Perez, C.A., Brady, L.W., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2001; Volume 1, pp. 530–581. [Google Scholar]
- Yamamoto, S.; Matsuda, I. Measurement of the Resonant Magneto-Optical Kerr Effect Using a Free Electron Laser. Appl. Sci. 2017, 7, 662. [Google Scholar] [CrossRef]
- Winkler, R.; Ciria, M.; Ahmad, M.; Plank, H.; Marcuello, C. A Review of the Current State of Magnetic Force Microscopy to Unravel the Magnetic Properties of Nanomaterials Applied in Biological Systems and Future Directions for Quantum Technologies. Nanomaterials 2023, 13, 2585. [Google Scholar] [CrossRef]
- Tsien, C.I.; Pugh, S.L.; Dicker, A.P.; Raizer, J.J.; Matuszak, M.M.; Lallana, E.C.; Huang, J.; Algan, O.; Deb, N.; Portelance, L.; et al. NRG Oncology/RTOG1205: A Randomized Phase II Trial of Concurrent Bevacizumab and Reirradiation Versus Bevacizumab Alone as Treatment for Recurrent Glioblastoma. J. Clin. Oncol. 2023, 41, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.J.; Giaccia, A.J. Time, Dose, and Fractionation in Radiotherapy. In Radiobiology for the Radiologist, 7th ed.; Hall, E.J., Giaccia, A.J., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; Volume 1, pp. 391–411. [Google Scholar]
- Pedicini, P.; Fiorentino, A.; Simeon, V.; Tini, P.; Chiumento, C.; Pirtoli, L.; Salvatore, M.; Storto, G. Clinical radiobiology of glioblastoma multiforme: Estimation of tumor control probability from various radiotherapy fractionation schemes. Strahlenther. Onkol. 2014, 190, 925–932. [Google Scholar] [CrossRef]
- Dharnipragada, R.; Ferreira, C.; Shah, R.; Reynolds, M.; Dusenbery, K.; Chen, C.C. GammaTile®(GT) as a brachytherapy platform for rapidly growing brain metastasis. Neurooncol. Adv. 2023, 5, vdad062. [Google Scholar]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Tu, Z.; Xiong, H.; Qiu, Y.; Li, G.; Wang, L.; Peng, S. Limited recurrence distance of glioblastoma under modern radiotherapy era. BMC Cancer 2021, 21, 720. [Google Scholar] [CrossRef]
- Stauffer, P.; Bar-Ad, V.; Hurwitz, M.; Luginbuhl, A.; Marcolongo, M.; Rodrigues, D.; Cogneti, D.; Curry, J.; Prudnikova, K. Tumor Bed Implant for Multimodality Treatment of at Risk Tissue Surrounding a Resection Cavity. US Patent Application No. 16/086,733, 20 September 2018. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanofluid | Saturation Magnetization (mT) | Viscosity at 27 °C (mPa·s) | Density at 25 °C (kg/m3) | Magnetite (Fe3O4) Particle Concentration (v/v) | Water Soluble Dispersant | Deionized Water |
|---|---|---|---|---|---|---|
| EMG 304 | 27.5 | <10 | 1220 | 4.5% | 1.5% | 94.0% |
| EMG 308 | 6.6 | <10 | 1050 | 1.2% | 0.5% | 98.3% |
| Job # | Relative Power P% (Duration) | H 1 (kA/m) | Application |
|---|---|---|---|
| 1 | 30% (240 s), 20% (60 s), 12% (900 s) | 5.6, 4.6, 3.5 | Thermal mapping in phantom |
| 2 | 15% (50 s), 35% (330 s), 10% (720 s) | 4.0, 6.0, 3.2 | In-air experiments |
| 3 | 15% (50 s), 35% (200 s), 7% (720 s) | 4.0, 6.0, 2.7 | In-air experiments |
| 4 | 15% (50 s), 55% (200 s), 20% (720 s) | 4.0, 7.6, 4.6 | In-phantom experiments |
| 5 | 10% (30 s), 47% (60 s), 27% (720 s) | 3.2, 7.0, 5.3 | Thermal mapping in pig brain |
| Balloon #2 in Air | DI Water (cGy) | DI Water + Nanofluid (cGy) | Difference (%) | |
|---|---|---|---|---|
| OSLD locations | distal | 453 | 454 | +0.2% |
| above | 532 | 451 | −15.2% | |
| underneath | 533 | 500 | −6.2% | |
| left | 538 | 453 | −15.8% | |
| right | 445 | 421 | −5.4% | |
| Average | 500 | 456 | −8.9% | |
| In air | 7 January 2021 | 8 January 2021 | |||||
|---|---|---|---|---|---|---|---|
| HDR (cGy) | HDR + HT (cGy) | Difference (%) | HDR (cGy) | HDR + HT (cGy) | Difference (%) | ||
| Balloon #2 | DA = 30 mm × DL = 34 mm, Tmax = 77 °C | DA = 29 mm × DL = 34 mm, Tmax = 55 °C | |||||
| OSLD locations | Distal | 438 | 380 | −13.2% | 430 | 408 | −5.1% |
| Top | 455 | 480 | +5.5% | 440 | 469 | +6.6% | |
| Bottom | 515 | 481 | −6.6% | 495 | 498 | +0.6% | |
| Left | 481 | 467 | −2.9% | 482 | 435 | −9.8% | |
| Right | 380 | 384 | 1.1% | 397 | 379 | −4.5% | |
| Average | 454 | 438 | −3.4% | 449 | 438 | −2.5% | |
| OSLD underneath balloon | HDR (cGy) | HDR + HT (cGy) | Difference (%) | HDR (cGy) | HDR + HT (cGy) | Difference (%) | |
| Balloon #1 | DA = 29 mm × DL = 34 mm, Tmax = 66 °C | DA = 30.0 mm × DL = 33.6 mm, Tmax = 52.2 °C | |||||
| Dose (cGy) | 607 | 536 | −11.7% | 527 | 449 | −14.8% | |
| Balloon #3 | DA = 30.8 mm × DL = 29.4 mm, Tmax = 64.5 °C | DA = 28.0 mm × DL = 30.3 mm, Tmax = N/A | |||||
| Dose (cGy) | 512 | 487 | −4.9% | N/A due to leaking from injection site | |||
| Balloon #4 | DA = 28.5 mm × DL = 33 mm, Tmax = 64.2 °C | DA = 28.5 mm × DL = 33.5 mm, Tmax = 53.4 °C | |||||
| Dose (cGy) | 498 | 459 | −7.8% | 430 | 481 | +11.9% | |
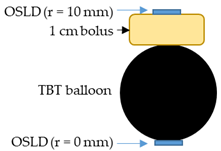 | Balloon #3 in air, DA = 30.7 mm × DL = 30.5 mm, Tmax = 52 °C | |||
| Radial distance from the balloon surface | HDR (cGy) | HDR + HT (cGy) | Difference (%) | |
| r = 0 mm (directly underneath the balloon) | 506 | 521 | +3.0% | |
| r = 10 mm (converted from 0 mm distance) | 186 | 191 | +3.0% | |
| r = 10 mm (on top of 1 cm bolus) | 182 * | 179 | −1.6% | |
| In Phantom | Balloon #1 | Balloon #2 | Balloon #3 | Balloon #4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dimensions | DA = 30.2 mm DL = 33.5 mm | DA = 29.3 mm DL = 33.6 mm | DA = 30.7 mm DL = 30.5 mm | DA = 30.5 mm DL = 33.5 mm | ||||||||
| Tmax | 43 °C | 49 °C | 48 °C | 49.5 °C | ||||||||
| OSLD locations | HDR (cGy) | HDR + HT (cGy) | Difference (%) | HDR (cGy) | HDR + HT (cGy) | Difference (%) | HDR (cGy) | HDR + HT (cGy) | Difference (%) | HDR (cGy) | HDR + HT (cGy) | Difference (%) |
| Top | 537 | 535 | −0.4% | 496 | 480 | −3.2% | 514 | 420 | −18.3% | 401 | 424 | +5.7% |
| Bottom | 496 | 506 | +2.0% | 557 | 513 | −7.9% | 462 | 433 | −6.3% | 517 | 462 | −10.6% |
| Left | 401 | 516 | +28.7% | 563 | 497 | −11.7% | 487 | 477 | −2.1% | 441 | 425 | −3.6% |
| Right | 429 | 410 | −4.4% | 466 | 458 | −1.7% | 466 | 457 | −1.9% | 437 | 458 | +4.8% |
| Average | 466 | 492 | +5.6% | 520 | 487 | −6.4% | 482 | 447 | −7.4% | 449 | 442 | −1.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wan, S.; Rodrigues, D.B.; Kwiatkowski, J.; Khanna, O.; Judy, K.D.; Goldstein, R.C.; Overbeek Bloem, M.; Yu, Y.; Rooks, S.E.; Shi, W.; et al. Evaluation of a Balloon Implant for Simultaneous Magnetic Nanoparticle Hyperthermia and High-Dose-Rate Brachytherapy of Brain Tumor Resection Cavities. Cancers 2023, 15, 5683. https://doi.org/10.3390/cancers15235683
Wan S, Rodrigues DB, Kwiatkowski J, Khanna O, Judy KD, Goldstein RC, Overbeek Bloem M, Yu Y, Rooks SE, Shi W, et al. Evaluation of a Balloon Implant for Simultaneous Magnetic Nanoparticle Hyperthermia and High-Dose-Rate Brachytherapy of Brain Tumor Resection Cavities. Cancers. 2023; 15(23):5683. https://doi.org/10.3390/cancers15235683
Chicago/Turabian StyleWan, Shuying, Dario B. Rodrigues, Janet Kwiatkowski, Omaditya Khanna, Kevin D. Judy, Robert C. Goldstein, Marty Overbeek Bloem, Yan Yu, Sophia E. Rooks, Wenyin Shi, and et al. 2023. "Evaluation of a Balloon Implant for Simultaneous Magnetic Nanoparticle Hyperthermia and High-Dose-Rate Brachytherapy of Brain Tumor Resection Cavities" Cancers 15, no. 23: 5683. https://doi.org/10.3390/cancers15235683
APA StyleWan, S., Rodrigues, D. B., Kwiatkowski, J., Khanna, O., Judy, K. D., Goldstein, R. C., Overbeek Bloem, M., Yu, Y., Rooks, S. E., Shi, W., Hurwitz, M. D., & Stauffer, P. R. (2023). Evaluation of a Balloon Implant for Simultaneous Magnetic Nanoparticle Hyperthermia and High-Dose-Rate Brachytherapy of Brain Tumor Resection Cavities. Cancers, 15(23), 5683. https://doi.org/10.3390/cancers15235683