



Combined Serum ALBUMIN with Neutrophil-to-Lymphocyte Ratio Predicts the Prognosis of Biliary Tract Cancer after Curative Resection

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics and Clinicopathological Data
3.2. Prognostic Factors of Resected Biliary Tract Cancer Patients
3.3. Recurrence-Free Survival and Overall Survival
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Vaquero, J.; Guedj, N.; Claperon, A.; Nguyen Ho-Bouldoires, T.H.; Paradis, V.; Fouassier, L. Epithelial-mesenchymal transition in cholangiocarcinoma: From clinical evidence to regulatory networks. J. Hepatol. 2017, 66, 424–441. [Google Scholar] [CrossRef]
- Hasegawa, S.; Ikai, I.; Fujii, H.; Hatano, E.; Shimahara, Y. Surgical resection of hilar cholangiocarcinoma: Analysis of survival and postoperative complications. World J. Surg. 2007, 31, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.H.; Xie, W.Y.; Zhang, Z.D.; Li, S.; Zhang, D.F.; Liu, Y.J.; Zhu, J.Y.; Leng, X.S. Postoperative Complications and Survival Analysis of Surgical Resection for Hilar Cholangiocarcinoma: A Retrospective Study of Fifty-Nine Consecutive Patients. Chin. Med. Sci. J. 2020, 35, 157–169. [Google Scholar]
- Chen, S.; Zhang, J.; Wang, R.; Luo, X.; Chen, H. The platinum-based treatments for advanced non-small cell lung cancer, is low/negative ERCC1 expression better than high/positive ERCC1 expression? A meta-analysis. Lung Cancer 2010, 70, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Dabholkar, M.; Bostick-Bruton, F.; Weber, C.; Bohr, V.A.; Egwuagu, C.; Reed, E. ERCC1 and ERCC2 expression in malignant tissues from ovarian cancer patients. J. Natl. Cancer Inst. 1992, 84, 1512–1517. [Google Scholar] [CrossRef] [PubMed]
- Park, K.W.; Jung, E.S.; Kim, D.G.; Yoo, Y.K.; Hong, T.H.; Lee, I.S.; Koh, Y.H.; Kim, J.H.; Lee, M.A. ERCC1 Can Be a Prognostic Factor in Hilar Cholangiocarcinoma and Extrahepatic Bile Duct Cancer, But Not in Intrahepatic Cholangiocarcinoma. Cancer Res. Treat. 2013, 45, 63–69. [Google Scholar] [CrossRef]
- Wu, Z.; Miao, X.; Zhang, Y.; Li, D.; Zou, Q.; Yuan, Y.; Liu, R.; Yang, Z. XRCC1 Is a Promising Predictive Biomarker and Facilitates Chemo-Resistance in Gallbladder Cancer. Front. Mol. Biosci. 2020, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C.; Elahi, M.M.; Sattar, N.; Angerson, W.J.; Johnstone, J.; McArdle, C.S. Measurement of the systemic inflammatory response predicts cancer-specific and non-cancer survival in patients with cancer. Nutr. Cancer 2001, 41, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Jansson, H.; Cornillet, M.; Bjorkstrom, N.K.; Sturesson, C.; Sparrelid, E. Prognostic value of preoperative inflammatory markers in resectable biliary tract cancer—Validation and comparison of the Glasgow Prognostic Score and Modified Glasgow Prognostic Score in a Western cohort. Eur. J. Surg. Oncol. 2020, 46, 804–810. [Google Scholar] [CrossRef] [PubMed]
- McNamara, M.G.; Templeton, A.J.; Maganti, M.; Walter, T.; Horgan, A.M.; McKeever, L.; Min, T.; Amir, E.; Knox, J.J. Neutrophil/lymphocyte ratio as a prognostic factor in biliary tract cancer. Eur. J. Cancer. 2014, 50, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.H.; Luo, X.F. Platelet to lymphocyte ratio in biliary tract cancer: Review and meta-analysis. Clin. Chim. Acta 2017, 474, 102–107. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, R.; Fu, J.L.; Zhang, J.; Su, J.B.; Jin, Z.C.; Chen, C.; Zhang, D.; Geng, Z.M. Prognostic value of preoperative peripheral blood neutrophil-to-lymphocyte ratio and gamma-glutamyl transpeptidase-to-platelet ratio index in patients with hepatitis B virus related intrahepatic cholangiocarcinoma after radical resection. Zhonghua Yi Xue Za Zhi 2021, 101, 3134–3140. [Google Scholar]
- Conci, S.; Campagnaro, T.; Danese, E.; Lombardo, E.; Isa, G.; Vitali, A.; Marchitelli, I.; Bagante, F.; Pedrazzani, C.; De Bellis, M.; et al. Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers. Cancers 2021, 13, 3594. [Google Scholar] [CrossRef] [PubMed]
- Kao, H.K.; Lofstrand, J.; Loh, C.Y.; Lao, W.W.; Yi, J.S.; Chang, Y.L.; Chang, K.P. Nomogram based on albumin and neutrophil-to-lymphocyte ratio for predicting the prognosis of patients with oral cavity squamous cell carcinoma. Sci. Rep. 2018, 8, 13081. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Wang, J.; Liu, J.; Chen, S.; Liu, X. Albumin concentrations plus neutrophil lymphocyte ratios for predicting overall survival after curative resection for gastric cancer. OncoTargets Ther. 2016, 9, 4661–4669. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Hsueh, S.W.; Yang, S.H.; Chiu, S.C.; Chiang, N.J.; Chiu, T.J.; Li, C.P.; Bai, L.Y.; Chiu, C.F.; Chuang, S.C.; et al. Predictive value of albumin combined with neutrophil-to-lymphocyte ratio for efficacy and safety profiles in patients with pancreatic ductal adenocarcinoma receiving liposomal irinotecan plus 5-fluorouracil and leucovorin. Am. J. Cancer Res. 2022, 12, 4267–4278. [Google Scholar]
- Omichi, K.; Cloyd, J.M.; Yamashita, S.; Tzeng, C.D.; Conrad, C.; Chun, Y.S.; Aloia, T.A.; Vauthey, J.N. Neutrophil-to-lymphocyte ratio predicts prognosis after neoadjuvant chemotherapy and resection of intrahepatic cholangiocarcinoma. Surgery 2017, 162, 752–765. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, R.; Chen, W.; Xu, X.; Dong, S.; Fan, H.; Liu, C. Prognostic significance of neutrophil to lymphocyte ratio in patients with gallbladder carcinoma. HPB 2016, 18, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.Q.; Ma, C.; Cao, W.Z.; Ning, Z.; Tan, G. Prognostic Significance of NLR, PLR, LMR and Tumor Infiltrating T Lymphocytes in Patients Undergoing Surgical Resection for Hilar Cholangiocarcinoma. Front. Oncol. 2022, 12, 908907. [Google Scholar] [CrossRef] [PubMed]
- Kumamoto, Y.; Kaizu, T.; Tajima, H.; Nishizawa, N.; Ei, S.; Igarashi, K.; Watanabe, M. Neutrophil-to-lymphocyte ratio as a predictor of postoperative morbidity in patients with distal cholangiocarcinoma. Mol. Clin. Oncol. 2018, 9, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Waghray, A.; Sobotka, A.; Marrero, C.R.; Estfan, B.; Aucejo, F.; Narayanan Menon, K.V. Serum albumin predicts survival in patients with hilar cholangiocarcinoma. Gastroenterol. Rep. 2017, 5, 62–66. [Google Scholar] [CrossRef]
- Shen, J.; Wen, T.; Li, C.; Yan, L.; Li, B.; Yang, J. The Prognostic Prediction Role of Preoperative Serum Albumin Level in Patients with Intahepatic Cholangiocarcinoma Following Hepatectomy. Dig. Dis. 2018, 36, 306–313. [Google Scholar] [CrossRef]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Salati, M.; Caputo, F.; Cunningham, D.; Marcheselli, L.; Spallanzani, A.; Rimini, M.; Gelsomino, F.; Reggiani-Bonetti, L.; Andrikou, K.; Rovinelli, F.; et al. The A.L.A.N. score identifies prognostic classes in advanced biliary cancer patients receiving first-line chemotherapy. Eur. J. Cancer 2019, 117, 84–90. [Google Scholar] [CrossRef]
- Muller, L.; Mahringer-Kunz, A.; Jungmann, F.; Tanyildizi, Y.; Bartsch, F.; Czauderna, C.; Duber, C.; Galle, P.R.; Weinmann, A.; Kloeckner, R.; et al. Risk Stratification in Advanced Biliary Tract Cancer: Validation of the A.L.A.N. Score. J. Oncol. 2020, 2020, 6180613. [Google Scholar] [CrossRef]
- Yang, F.; Huang, Q.; Guan, Z.; Diao, Q. Prognostic significance of pretreatment neutrophil-to-lymphocyte ratio in patients with laryngeal cancer: A systematic review and meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 417–425. [Google Scholar] [CrossRef]
- Kang, M.H.; Go, S.I.; Song, H.N.; Lee, A.; Kim, S.H.; Kang, J.H.; Jeong, B.K.; Kang, K.M.; Ling, H.; Lee, G.W. The prognostic impact of the neutrophil-to-lymphocyte ratio in patients with small-cell lung cancer. Br. J. Cancer 2014, 111, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Fu, S.J.; Shen, S.L.; Li, S.Q.; Hua, Y.P.; Hu, W.J.; Liang, L.J.; Peng, B.G. Prognostic value of preoperative peripheral neutrophil-to-lymphocyte ratio in patients with HBV-associated hepatocellular carcinoma after radical hepatectomy. Med. Oncol. 2013, 30, 721. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, W.; Feng, L.J. Prognostic significance of neutrophil lymphocyte ratio in patients with gastric cancer: A meta-analysis. PLoS ONE 2014, 9, e111906. [Google Scholar] [CrossRef] [PubMed]
- Nozawa, H.; Chiu, C.; Hanahan, D. Infiltrating neutrophils mediate the initial angiogenic switch in a mouse model of multistage carcinogenesis. Proc. Natl. Acad. Sci. USA 2006, 103, 12493–12498. [Google Scholar] [CrossRef]
- Croker, B.A.; Lewis, R.S.; Babon, J.J.; Mintern, J.D.; Jenne, D.E.; Metcalf, D.; Zhang, J.G.; Cengia, L.H.; O’Donnell, J.A.; Roberts, A.W. Neutrophils require SHP1 to regulate IL-1beta production and prevent inflammatory skin disease. J. Immunol. 2011, 186, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.; Shi, M.; Zeng, Z.; Qi, R.Z.; Liu, Z.W.; Zhang, J.Y.; Yang, Y.P.; Tien, P.; Wang, F.S. PD-1 and PD-L1 upregulation promotes CD8+ T-cell apoptosis and postoperative recurrence in hepatocellular carcinoma patients. Int. J. Cancer 2011, 128, 887–896. [Google Scholar] [CrossRef]
- Fridlender, Z.G.; Sun, J.; Kim, S.; Kapoor, V.; Cheng, G.; Ling, L.; Worthen, G.S.; Albelda, S.M. Polarization of tumor-associated neutrophil phenotype by TGF-beta: “N1” versus “N2” TAN. Cancer Cell 2009, 16, 183–194. [Google Scholar] [CrossRef]
- Liu, F.; Hu, H.J.; Ma, W.J.; Yang, Q.; Wang, J.K.; Li, F.Y. Prognostic significance of neutrophil-lymphocyte ratio and carbohydrate antigen 19-9 in patients with gallbladder carcinoma. Medicine 2019, 98, e14550. [Google Scholar] [CrossRef]
- Horwich, T.B.; Kalantar-Zadeh, K.; MacLellan, R.W.; Fonarow, G.C. Albumin levels predict survival in patients with systolic heart failure. Am. Heart J. 2008, 155, 883–889. [Google Scholar] [CrossRef]
- Menon, V.; Greene, T.; Wang, X.; Pereira, A.A.; Marcovina, S.M.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005, 68, 766–772. [Google Scholar] [CrossRef]
- Pacelli, F.; Doglietto, G.B.; Alfieri, S.; Piccioni, E.; Sgadari, A.; Gui, D.; Crucitti, F. Prognosis in intra-abdominal infections. Multivariate analysis on 604 patients. Arch. Surg. 1996, 131, 641–645. [Google Scholar] [CrossRef]
- Gatta, A.; Verardo, A.; Bolognesi, M. Hypoalbuminemia. Intern. Emerg. Med. 2012, 7 (Suppl. 3), 193–199. [Google Scholar] [CrossRef]
- Fleck, A.; Raines, G.; Hawker, F.; Trotter, J.; Wallace, P.I.; Ledingham, I.M.; Calman, K.C. Increased vascular permeability: A major cause of hypoalbuminaemia in disease and injury. Lancet 1985, 1, 781–784. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef]
- Al-Shaiba, R.; McMillan, D.C.; Angerson, W.J.; Leen, E.; McArdle, C.S.; Horgan, P. The relationship between hypoalbuminaemia, tumour volume and the systemic inflammatory response in patients with colorectal liver metastases. Br. J. Cancer 2004, 91, 205–207. [Google Scholar] [CrossRef]
- Seebacher, V.; Grimm, C.; Reinthaller, A.; Heinze, G.; Tempfer, C.; Hefler, L.; Polterauer, S. The value of serum albumin as a novel independent marker for prognosis in patients with endometrial cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 101–106. [Google Scholar] [CrossRef]
- Sharma, R.; Hook, J.; Kumar, M.; Gabra, H. Evaluation of an inflammation-based prognostic score in patients with advanced ovarian cancer. Eur. J. Cancer 2008, 44, 251–256. [Google Scholar] [CrossRef]
- Bekos, C.; Polterauer, S.; Seebacher, V.; Bartl, T.; Joura, E.; Reinthaller, A.; Sturdza, A.; Horvat, R.; Schwameis, R.; Grimm, C. Pre-operative hypoalbuminemia is associated with complication rate and overall survival in patients with vulvar cancer undergoing surgery. Arch. Gynecol. Obstet. 2019, 300, 1015–1022. [Google Scholar] [CrossRef]
- Golse, N.; Nunez, J.; Mazzotta, A.; Cano, L.; Bergeat, D.; Sulpice, L.; Jeddou, H.; Abdelrafee, A.; Sa Cunha, A.; Cherqui, D.; et al. Personalized Preoperative Nomograms Predicting Postoperative Risks after Resection of Perihilar Cholangiocarcinoma. World J. Surg. 2020, 44, 3449–3460. [Google Scholar] [CrossRef]
- Shinohara, K.; Ebata, T.; Shimoyama, Y.; Mizuno, T.; Yokoyama, Y.; Yamaguchi, J.; Onoe, S.; Watanabe, N.; Nagino, M. A Study on Radial Margin Status in Resected Perihilar Cholangiocarcinoma. Ann. Surg. 2021, 273, 572–578. [Google Scholar] [CrossRef]
- Spolverato, G.; Yakoob, M.Y.; Kim, Y.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; et al. The Impact of Surgical Margin Status on Long-Term Outcome After Resection for Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2015, 22, 4020–4028. [Google Scholar] [CrossRef]
- Burt, A.D.; Alves, V.; Bedossa, P.; Clouston, A.; Guido, M.; Hubscher, S.; Kakar, S.; Ng, I.; Park, Y.N.; Reeves, H.; et al. Data set for the reporting of intrahepatic cholangiocarcinoma, perihilar cholangiocarcinoma and hepatocellular carcinoma: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Histopathology 2018, 73, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.W.; Cheung, T.T.; She, W.H.; Chok, K.S.H.; Chan, A.C.Y.; Ng, I.O.L.; Chan, S.C.; Lo, C.M. The effect of wide resection margin in patients with intrahepatic cholangiocarcinoma: A single-center experience. Medicine 2016, 95, e4133. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Lu, W.; Li, B.; Meng, X.; Dong, J. Influence of surgical margins on overall survival after resection of intrahepatic cholangiocarcinoma: A meta-analysis. Medicine 2016, 95, e4621. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wang, L.; Wang, M.; He, X.; Xu, W.; Zhu, W.; Zhao, Y.; Wang, L. Prognostic value of resection margin length after surgical resection for intrahepatic cholangiocarcinoma. Am. J. Surg. 2021, 222, 383–389. [Google Scholar] [CrossRef]
- Kim, B.J.; Newhook, T.E.; Tzeng, C.D.; Ikoma, N.; Chiang, Y.J.; Chun, Y.S.; Vauthey, J.N.; Tran Cao, H.S. Lymphadenectomy and margin-negative resection for biliary tract cancer surgery in the United States-Differential technical performance by approach. J. Surg. Oncol. 2022, 126, 658–666. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Numbers | Percentage (%) | |
|---|---|---|
| Gender | ||
| Male | 167 | 58.2 |
| Female | 120 | 41.8 |
| Age (Median: 61.5± 10.93 years old) | ||
| <62 | 136 | 47.4 |
| ≧62 | 151 | 52.6 |
| Performance status (ECOG) | ||
| 0 | 175 | 61.0 |
| 1 | 78 | 27.2 |
| 2 | 34 | 11.8 |
| Tumor site | ||
| Intrahepatic | 177 | 61.7 |
| Gall bladder | 37 | 12.9 |
| Common bile duct | 51 | 17.8 |
| Perihilar | 22 | 7.7 |
| Tumor size | ||
| T1 | 81 | 28.2 |
| T2 | 111 | 38.7 |
| T3 | 51 | 17.8 |
| T4 | 44 | 15.3 |
| Lymph nodes | ||
| N0 | 102 | 35.5 |
| N1 | 47 | 16.4 |
| N2 | 3 | 1 |
| No dissection | 135 | 47.0 |
| TMN stage | ||
| I | 83 | 28.9 |
| II | 124 | 43.2 |
| III | 39 | 13.6 |
| IV | 41 | 14.3 |
| Hepatitis B | ||
| Yes | 99 | 34.5 |
| No | 188 | 65.5 |
| Hepatitis C | ||
| Yes | 48 | 16.7 |
| No | 239 | 83.3 |
| CA199 before surgery | ||
| <350 | 227 | 79.1 |
| ≧350 | 60 | 20.9 |
| Vascular invasion | ||
| No | 133 | 46.3 |
| Yes | 134 | 46.7 |
| Portal invasion | 20 | 7.0 |
| Surgical margin | ||
| R0 | 217 | 75.6 |
| R1 | 37 | 12.9 |
| Close margin (1 mm) | 33 | 11.5 |
| Adjuvant treatment | ||
| No | 214 | 74.6 |
| Chemotherapy | 53 | 18.5 |
| CCRT | 13 | 4.5 |
| Radiotherapy | 7 | 2.4 |
| ERCC1 | ||
| Negative | 247 | 86.1 |
| Positive | 40 | 13.9 |
| XRCC1 | ||
| Negative | 251 | 87.5 |
| Positive | 36 | 12.5 |
| Albumin | ||
| <3.5 | 88 | 30.7 |
| ≧3.5 | 199 | 69.3 |
| NLR | ||
| <2.28 | 119 | 41.5 |
| ≧2.28 | 166 | 58.5 |
| Clinical and Pathological Characteristics | Albumin | NLR | ANS | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| <3.5 | ≧3.5 | p-Value | <2.28 | ≧2.28 | p-Value | 0 | 1 | 2 | p-Value | |
| N = 88 | N = 199 | N = 119 | N = 168 | N = 96 | N = 126 | N = 65 | ||||
| Age | ||||||||||
| <62 | 39 | 97 | 0.489 | 63 | 73 | 0.113 | 52 | 56 | 28 | 0.260 |
| ≧62 | 49 | 102 | 56 | 95 | 44 | 70 | 37 | |||
| Sex | ||||||||||
| Male | 52 | 115 | 0.837 | 69 | 98 | 0.953 | 56 | 72 | 39 | 0.930 |
| Female | 36 | 84 | 50 | 70 | 40 | 54 | 26 | |||
| Tumor location | ||||||||||
| Intrahepatic | 46 | 131 | 0.132 | 85 | 92 | 0.012 | 70 | 76 | 31 | 0.037 |
| Gall bladder | 12 | 25 | 15 | 22 | 12 | 16 | 9 | |||
| Common bile duct | 21 | 30 | 14 | 37 | 10 | 24 | 17 | |||
| Hilar | 9 | 13 | 5 | 17 | 4 | 10 | 8 | |||
| p-T Status | ||||||||||
| 1–2 | 46 | 146 | 0.001 | 99 | 93 | 0.001 | 83 | 79 | 30 | 0.001 |
| 3–4 | 42 | 53 | 20 | 75 | 13 | 47 | 35 | |||
| p-N status | ||||||||||
| Negative | 29 | 73 | 0.001 | 37 | 65 | 0.001 | 32 | 46 | 24 | 0.001 |
| Positive | 26 | 24 | 12 | 38 | 7 | 22 | 21 | |||
| No dissection | 33 | 102 | 70 | 65 | 57 | 58 | 20 | |||
| AJCC pathological stage | ||||||||||
| I-II | 53 | 154 | 0.003 | 98 | 109 | 0.001 | 82 | 88 | 37 | 0.001 |
| III-IV | 35 | 45 | 21 | 59 | 14 | 38 | 28 | |||
| Vascular invasion | ||||||||||
| No | 29 | 104 | 0.002 | 62 | 71 | 0.100 | 55 | 56 | 22 | 0.012 |
| Yes | 59 | 95 | 57 | 97 | 41 | 70 | 43 | |||
| Surgical margin | ||||||||||
| R0 | 55 | 162 | 0.003 | 99 | 118 | 0.033 | 81 | 99 | 37 | 0.002 |
| Close margin (1 mm) | 16 | 17 | 8 | 25 | 7 | 11 | 15 | |||
| R1 | 17 | 20 | 12 | 25 | 8 | 16 | 13 | |||
| DM. | ||||||||||
| No | 64 | 143 | 0.88 | 94 | 113 | 0.029 | 76 | 85 | 46 | 0.150 |
| Yes | 24 | 56 | 25 | 55 | 20 | 41 | 19 | |||
| HBV | ||||||||||
| No | 68 | 120 | 0.005 | 63 | 125 | 0.001 | 50 | 83 | 55 | 0.001 |
| Yes | 20 | 79 | 56 | 43 | 46 | 43 | 10 | |||
| HCV | ||||||||||
| No | 76 | 163 | 0.351 | 92 | 147 | 0.023 | 75 | 105 | 59 | 0.108 |
| Yes | 12 | 36 | 27 | 21 | 21 | 21 | 6 | |||
| CA19-9 | ||||||||||
| <350 | 58 | 169 | 0.001 | 104 | 123 | 0.004 | 87 | 99 | 41 | 0.001 |
| ≧350 | 30 | 30 | 15 | 45 | 9 | 27 | 24 | |||
| Performance status (ECOG) | ||||||||||
| 0 | 40 | 135 | 0.002 | 83 | 92 | 0.026 | 73 | 72 | 30 | 0.001 |
| 1 | 33 | 45 | 23 | 55 | 13 | 42 | 23 | |||
| 2 | 15 | 19 | 13 | 21 | 10 | 12 | 12 | |||
| Recurrence | ||||||||||
| Yes | 60 | 81 | 0.001 | 49 | 92 | 0.023 | 33 | 64 | 44 | 0.001 |
| No | 28 | 118 | 70 | 76 | 63 | 62 | 21 | |||
| ERCC1 | ||||||||||
| Negative | 81 | 166 | 0.064 | 98 | 149 | 0.166 | 77 | 110 | 60 | 0.078 |
| Positive | 7 | 33 | 21 | 19 | 19 | 16 | 5 | |||
| XRCC1 | ||||||||||
| Negative | 78 | 173 | 0.835 | 100 | 151 | 0.196 | 80 | 133 | 58 | 0.339 |
| Positive | 10 | 26 | 19 | 17 | 16 | 13 | 7 | |||
| Variables | Category | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|
| HR. | 95% CI | p-Value | HR. | 95% CI | p-Value | ||
| Age | <62 vs. ≧62 | 0.937 | 0.67–1.31 | 0.699 | 0.762 | 0.53–1.09 | 0.141 |
| Gender | Female vs. male | 0.772 | 0.55–1.09 | 0.139 | 0.762 | 0.86–1.81 | 0.245 |
| ECOG performance | 0 | Reference | |||||
| 1 | 1.56 | 1.08–2.28 | 0.020 | 1.159 | 0.78–1.73 | 0.473 | |
| 2 | 2.198 | 1.37–3.54 | 0.001 | 1.409 | 0.85–2.34 | 0.183 | |
| Tumor location | Intrahepatic | Reference | |||||
| Gall bladder | 0.728 | 0.41–1.31 | 0.288 | 0.541 | 0.29–1.02 | 0.057 | |
| Common bile duct | 1.40 | 0.92–2.13 | 0.114 | 1.285 | 0.75–2.20 | 0.359 | |
| Hilar | 1.52 | 0.86–2.68 | 0.148 | 0.476 | 0.25–0.92 | 0.026 | |
| p-T status | 3–4 vs. 1–2 | 2.42 | 1.73–3.38 | <0.001 | |||
| p-N status | Negative | Reference | |||||
| Positive | 2.35 | 1.54–3.61 | <0.001 | ||||
| No lymph node dissection | 1.089 | 0.74–1.61 | 0.667 | ||||
| AJCC pathological stage | III–IV vs. I–II | 2.525 | 1.80–3.55 | <0.001 | 2.285 | 1.47–3.55 | <0.001 |
| Vascular invasion | Yes vs. No | 2.048 | 1.45–2.90 | <0.001 | 1.998 | 1.37–2.92 | <0.001 |
| Surgical margin | R0 | Reference | |||||
| Margin 1 mm | 1.424 | 0.86–2.36 | 0.169 | 1.104 | 0.65–1.87 | 0.715 | |
| R1 | 2.443 | 1.57–3.81 | <0.001 | 1.510 | 0.92–2.47 | 0.101 | |
| Adjuvant Treatment | Yes vs. No | 1.46 | 1.03–2.08 | 0.035 | 0.630 | 0.41–0.96 | 0.032 |
| DM | Yes vs. No | 0.902 | 0.62–1.30 | 0.580 | 0.853 | 0.58–1.26 | 0.426 |
| HBV | Yes vs. No | 0.620 | 0.43–0.90 | 0.011 | 0.669 | 0.44–1.03 | 0.067 |
| HCV | Yes vs. No | 0.819 | 0.52–1.30 | 0.399 | 1.121 | 0.68–1.85 | 0.654 |
| CA19-9 | ≧350 vs. <350 | 3.373 | 2.36–4.82 | <0.001 | 3.271 | 2.17–4.93 | <0.001 |
| ERCC1 | Positive vs. negative | 1.244 | 0.74–2.09 | 0.412 | 0.837 | 0.51–1.38 | 0.484 |
| XRCC1 | Positive vs. negative | 1.16 | 0.71–1.90 | 0.566 | 1.27 | 0.75–2.15 | 0.372 |
| Albumin | ≧3.5 vs. <3.5 | 0.386 | 0.28–0.54 | <0.001 | |||
| NLR | <2.28 vs.≧2.28 | 1.615 | 1.14–2.29 | 0.007 | |||
| ANS | 2 | Reference | |||||
| 0 | 0.290 | 0.18–0.46 | <0.001 | 0.497 | 0.30–0.82 | 0.007 | |
| 1 | 0.494 | 0.34–0.73 | <0.001 | 0.638 | 0.42–0.96 | 0.031 | |
| Variates | Category | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age | <62 vs. ≧62 | 0.761 | 0.53–1.09 | 0.134 | 1.005 | 0.69–1.47 | 0.980 |
| Gender | Female vs. male | 0.904 | 0.63–1.30 | 0.587 | 1.071 | 0.72–1.59 | 0.732 |
| ECOG performance | 0 | Reference | |||||
| 1 | 2.151 | 1.45–3.19 | <0.001 | 1.502 | 0.98–2.30 | 0.062 | |
| 2 | 2.714 | 1.64–4.49 | <0.001 | 1.623 | 0.94–2.79 | 0.080 | |
| Tumor location | Intrahepatic | Reference | |||||
| Gall bladder | 0.968 | 0.52–1.79 | 0.866 | 0.541 | 0.45–1.66 | 0.665 | |
| Common bile duct | 1.640 | 1.06–2.53 | 0.026 | 1.466 | 0.84–2.57 | 0.183 | |
| Hilar | 1.928 | 1.06–3.50 | 0.031 | 0.819 | 0.42–1.61 | 0.561 | |
| p-T status | 3–4 vs. 1–2 | 2.551 | 1.79–3.65 | <0.001 | |||
| p-N status | Negative | Reference | |||||
| Positive | 2.686 | 1.63–4.29 | <0.001 | ||||
| No lymph node dissection | 1.126 | 0.74–1.73 | 0.586 | ||||
| AJCC pathological stage | III–IV vs. I–II | 2.441 | 1.70–3.51 | <0.001 | 2.140 | 1.36–3.38 | 0.001 |
| Vascular invasion | Yes vs. no | 2.303 | 1.57–3.37 | <0.001 | 1.998 | 1.33–3.01 | 0.001 |
| Surgical margin | R0 | Reference | |||||
| Margin 1 mm | 1.591 | 0.93–2.73 | 0.092 | 1.148 | 0.63–2.03 | 0.635 | |
| R1 | 3.623 | 2.37–5.55 | <0.001 | 2.240 | 1.40–3.57 | 0.001 | |
| Adjuvant Treatments | Yes vs. No | 1.419 | 0.97–2.07 | 0.070 | 0.622 | 0.40–0.97 | 0.034 |
| DM | Yes vs. No | 1.436 | 0.99–2.09 | 0.060 | 1.106 | 0.74–1.65 | 0.624 |
| HBV | Yes vs. No | 0.516 | 0.34–0.78 | 0.002 | 0.675 | 0.42–1.08 | 0.103 |
| HCV | Yes vs. No | 0.760 | 0.46–1.27 | 0.294 | 1.017 | 0.59–1.76 | 0.951 |
| CA19-9 | ≧350 vs. <350 | 2.875 | 1.98–4.19 | <0.001 | 2.333 | 1.54–3.54 | <0.001 |
| ERCC1 | Positive vs. negative | 0.972 | 0.58–1.62 | 0.913 | 0.861 | 0.51–1.45 | 0.573 |
| XRCC1 | Positive vs. negative | 0.74 | 0.45–1.22 | 0.24 | 0.652 | 0.39–1.08 | 0.097 |
| Albumin | <3.5 vs. ≧3.5 | 0.385 | 0.27–0.55 | <0.001 | |||
| NLR | ≧2.28 vs. <2.28 | 1.751 | 1.20–2.56 | 0.004 | |||
| ANS | 2 | Reference | |||||
| 0 | 0.261 | 0.16–0.43 | <0.001 | 0.532 | 0.31–0.93 | 0.027 | |
| 1 | 0.482 | 0.32–0.73 | <0.001 | 0.626 | 0.41–0.97 | 0.034 | |
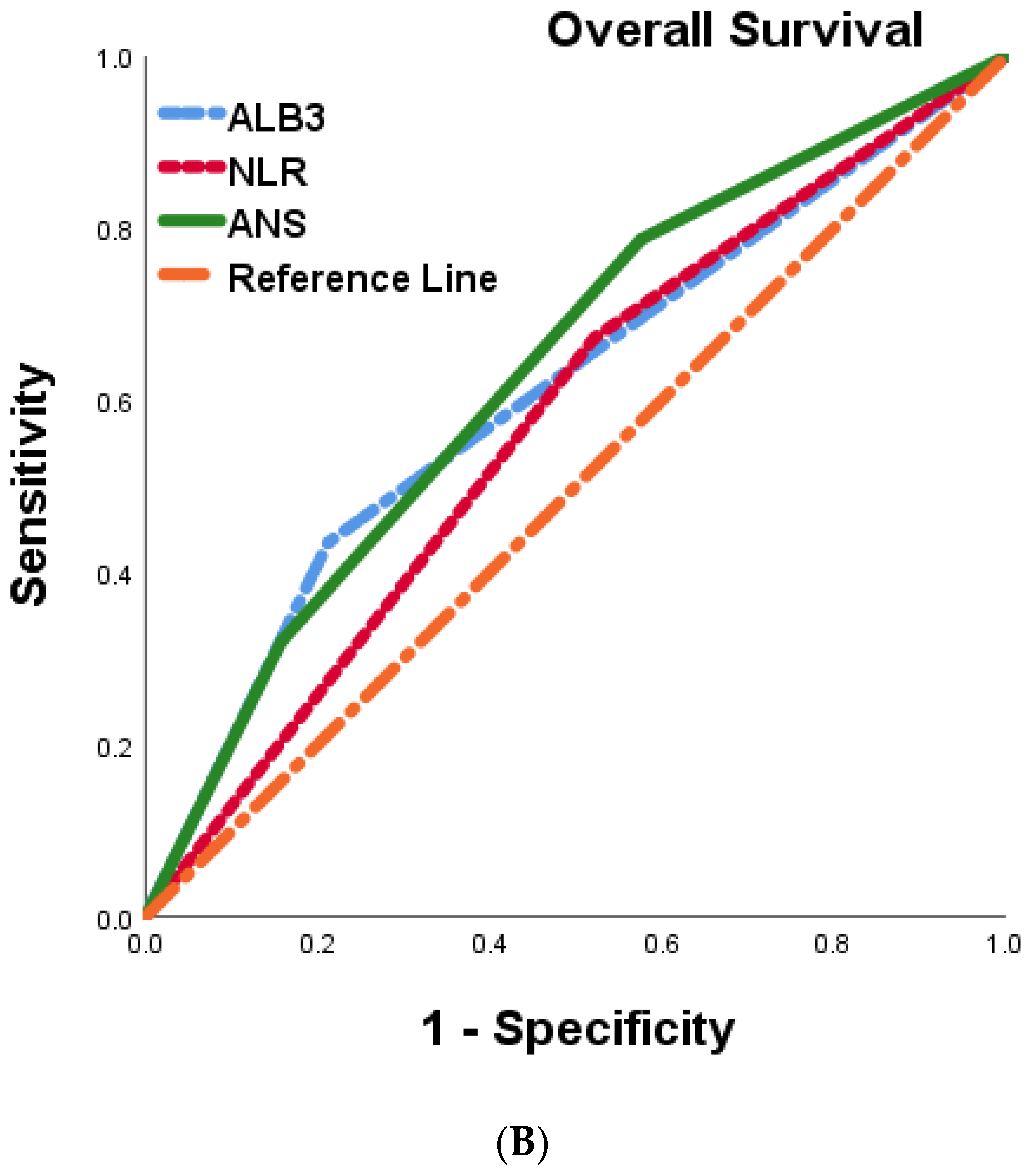
| Recurrent Free Survival | Overall Survival | |||
|---|---|---|---|---|
| Variates | Area under the ROC Curve (95% CI) | p-Value | Area under the ROC Curve (95% CI) | p-Value |
| ANC | 0.627 (0.563–0.691) | <0.001 | 0.636 (0.571–0.0700) | <0.001 |
| Albumin | 0.612 (0.547–0.677) | 0.001 | 0.611 (0.544–0.678) | 0.001 |
| NLR | 0.536 (0.497–0.629) | 0.065 | 0.575 (0.509–0.642) | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, T.-J.; Liu, Y.-W.; Yong, C.-C.; Yin, S.-M.; Yeh, C.-H.; Chen, Y.-Y. Combined Serum ALBUMIN with Neutrophil-to-Lymphocyte Ratio Predicts the Prognosis of Biliary Tract Cancer after Curative Resection. Cancers 2023, 15, 5474. https://doi.org/10.3390/cancers15225474
Chiu T-J, Liu Y-W, Yong C-C, Yin S-M, Yeh C-H, Chen Y-Y. Combined Serum ALBUMIN with Neutrophil-to-Lymphocyte Ratio Predicts the Prognosis of Biliary Tract Cancer after Curative Resection. Cancers. 2023; 15(22):5474. https://doi.org/10.3390/cancers15225474
Chicago/Turabian StyleChiu, Tai-Jan, Yueh-Wei Liu, Chee-Chien Yong, Shih-Min Yin, Cheng-His Yeh, and Yen-Yang Chen. 2023. "Combined Serum ALBUMIN with Neutrophil-to-Lymphocyte Ratio Predicts the Prognosis of Biliary Tract Cancer after Curative Resection" Cancers 15, no. 22: 5474. https://doi.org/10.3390/cancers15225474
APA StyleChiu, T.-J., Liu, Y.-W., Yong, C.-C., Yin, S.-M., Yeh, C.-H., & Chen, Y.-Y. (2023). Combined Serum ALBUMIN with Neutrophil-to-Lymphocyte Ratio Predicts the Prognosis of Biliary Tract Cancer after Curative Resection. Cancers, 15(22), 5474. https://doi.org/10.3390/cancers15225474