
Epidemiology of Neuroendocrine Neoplasms and Results of Their Treatment with [177Lu]Lu-DOTA-TATE or [177Lu]Lu-DOTA-TATE and [90Y]Y-DOTA-TATE—A Six-Year Experience in High-Reference Polish Neuroendocrine Neoplasm Center

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment Protocol
2.2. Statistical Analysis
2.3. Laboratory Evaluation
3. Results
3.1. Gender and Age
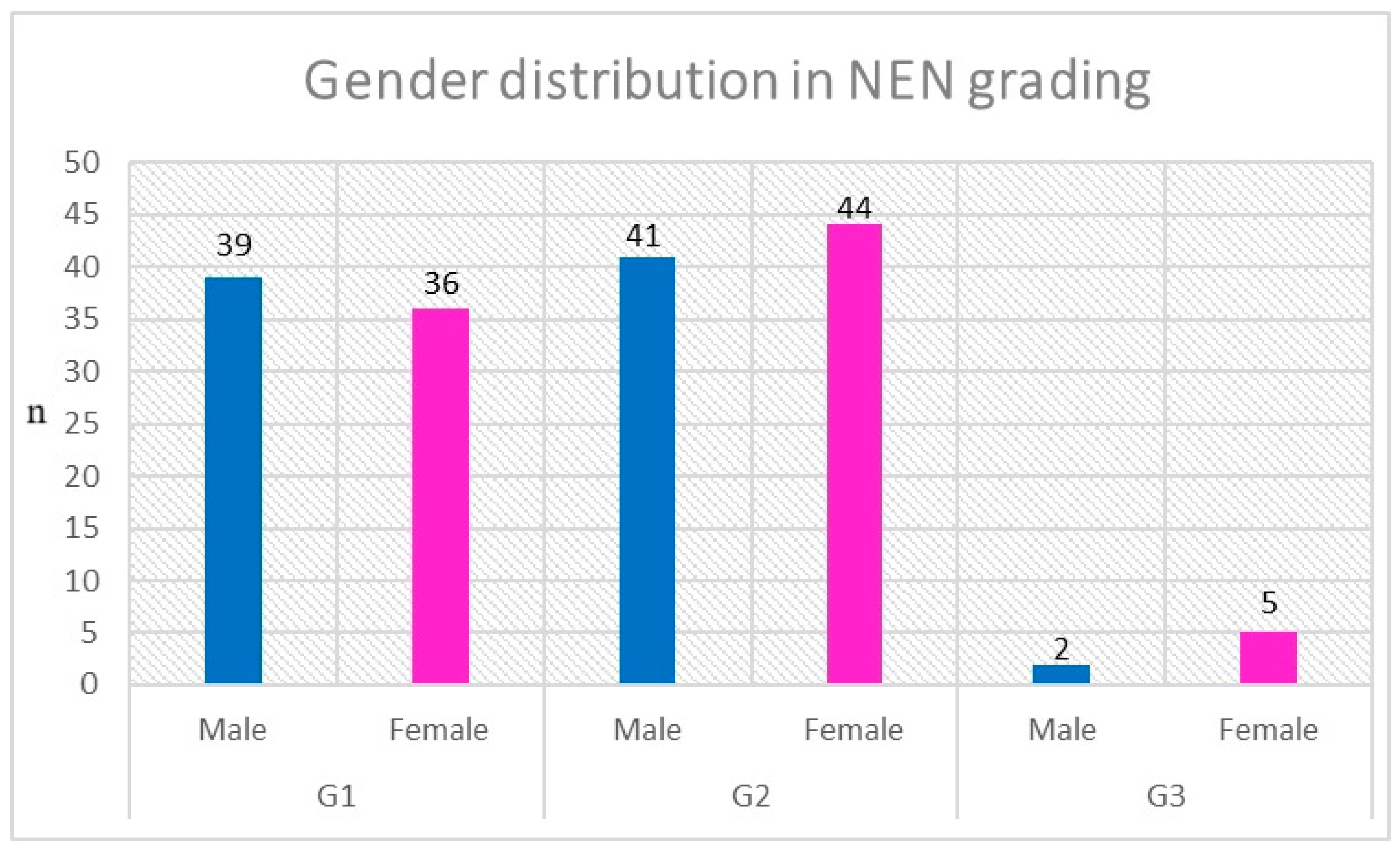
3.2. NEN Grading and Ki-67
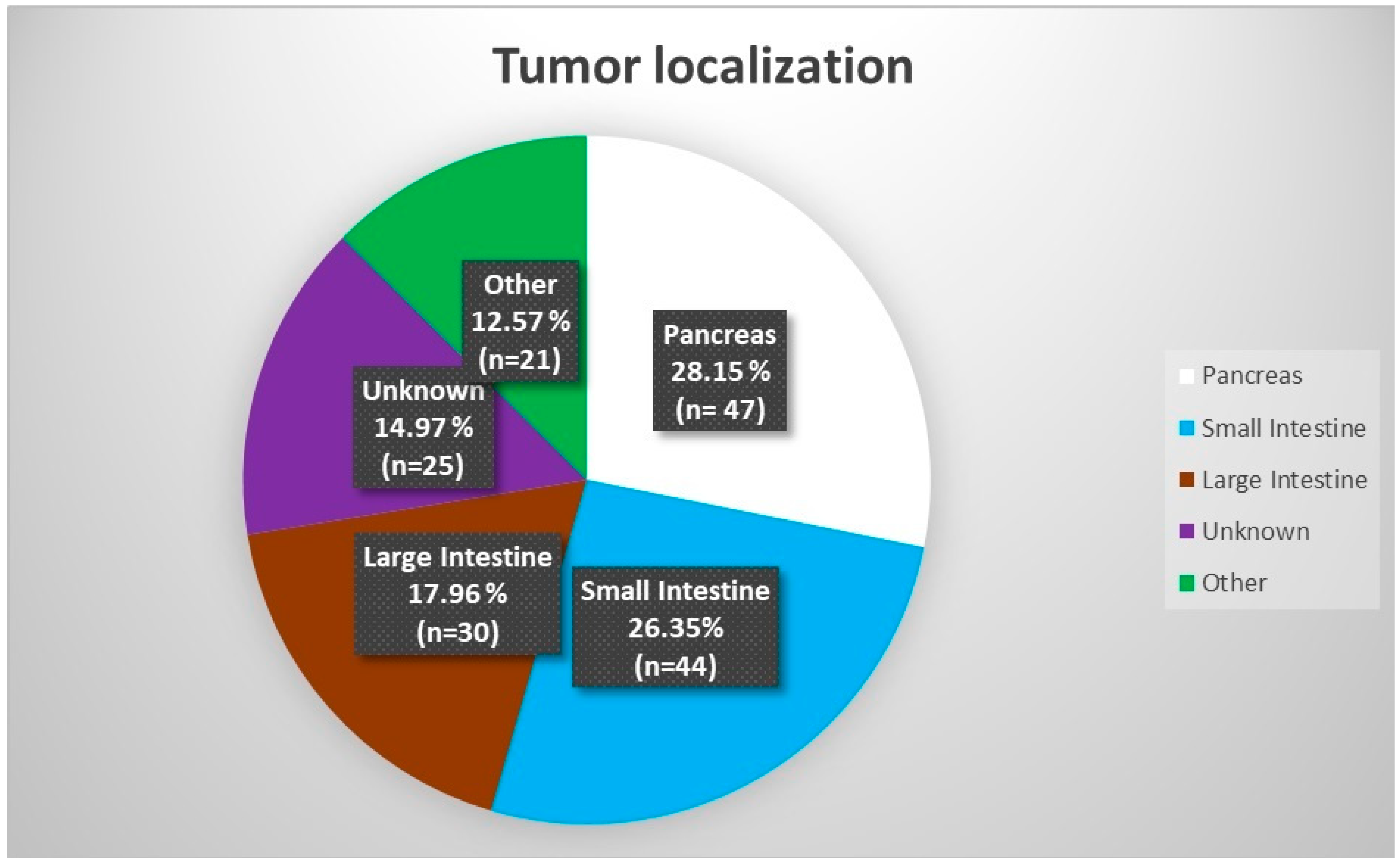
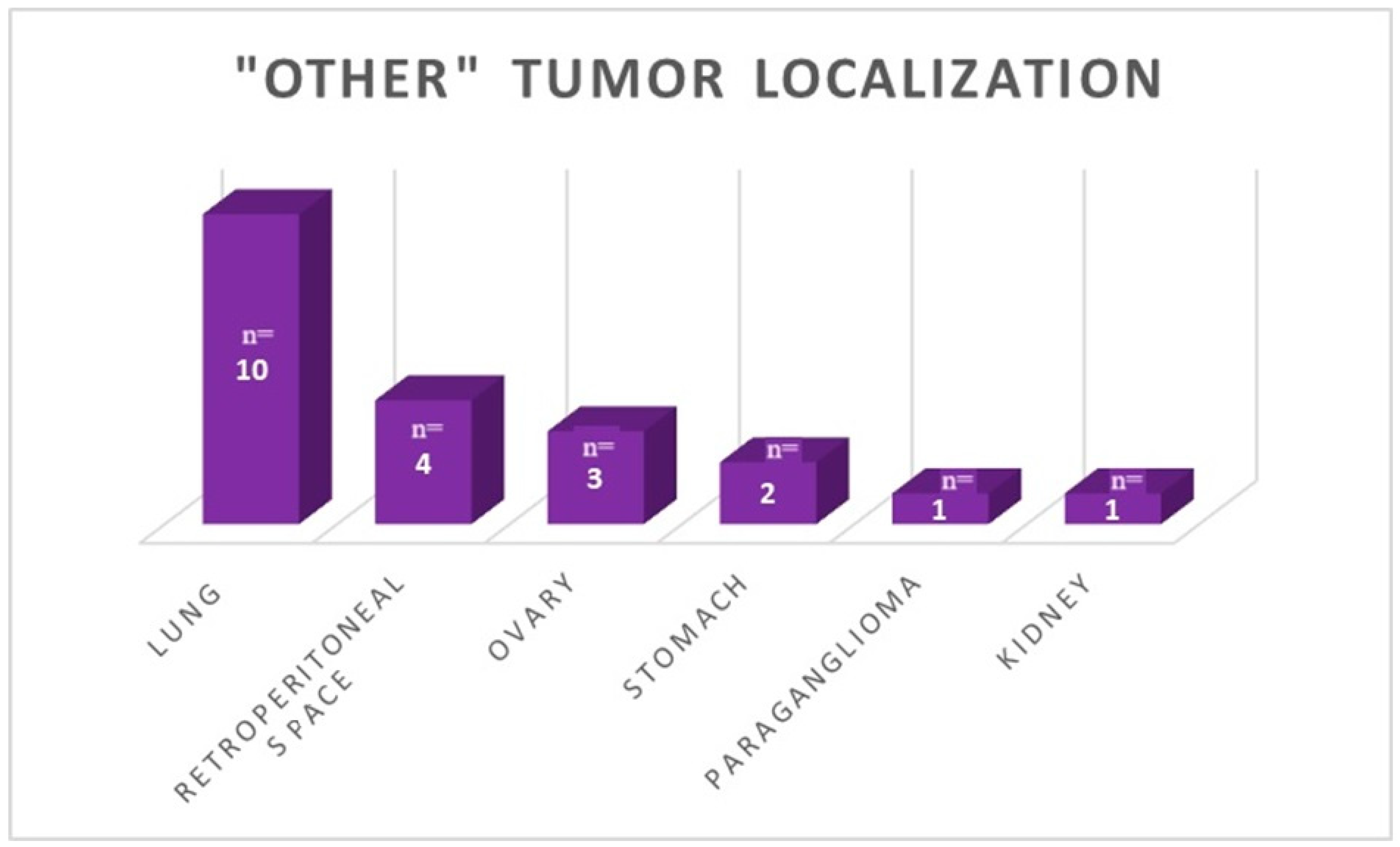
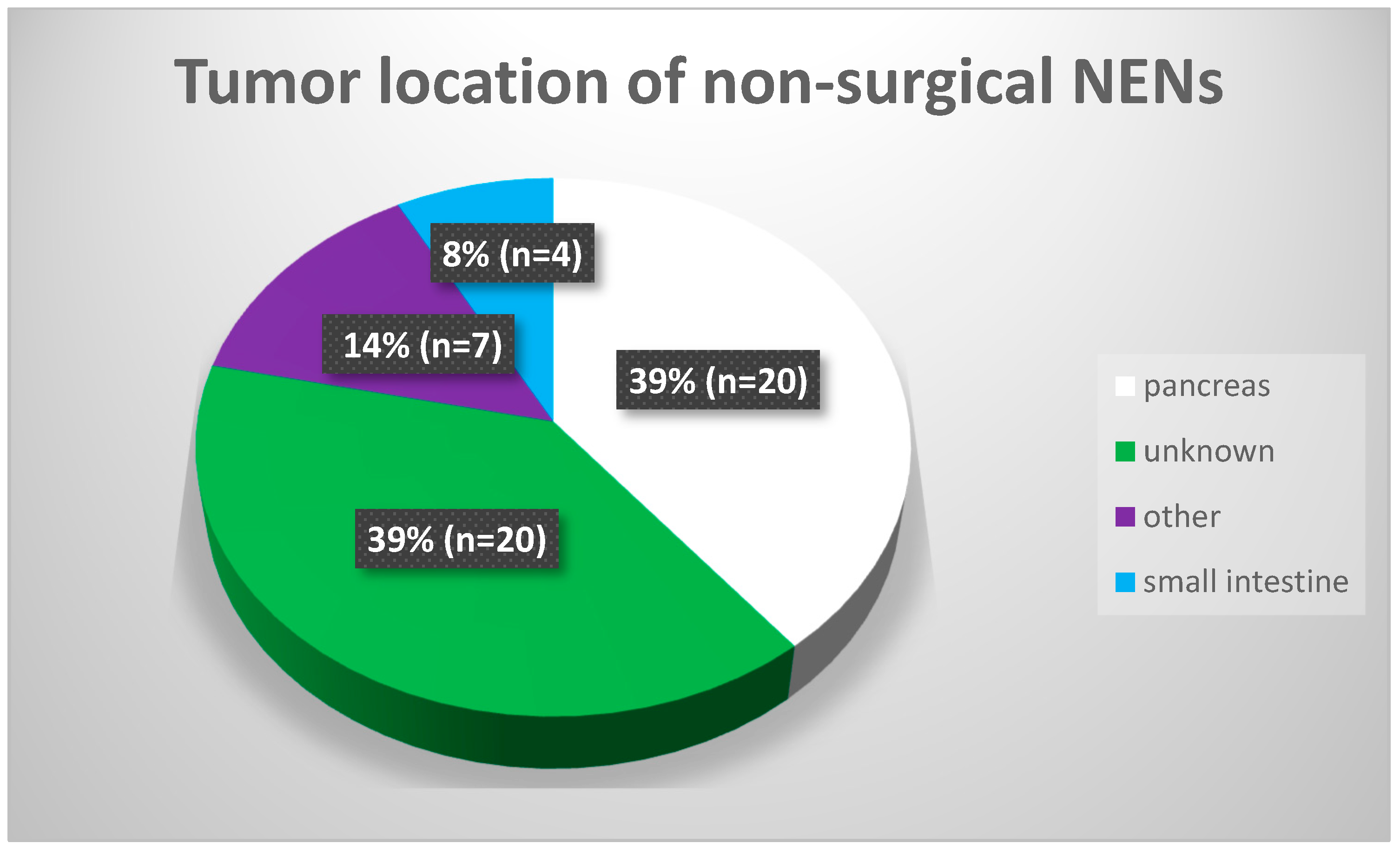
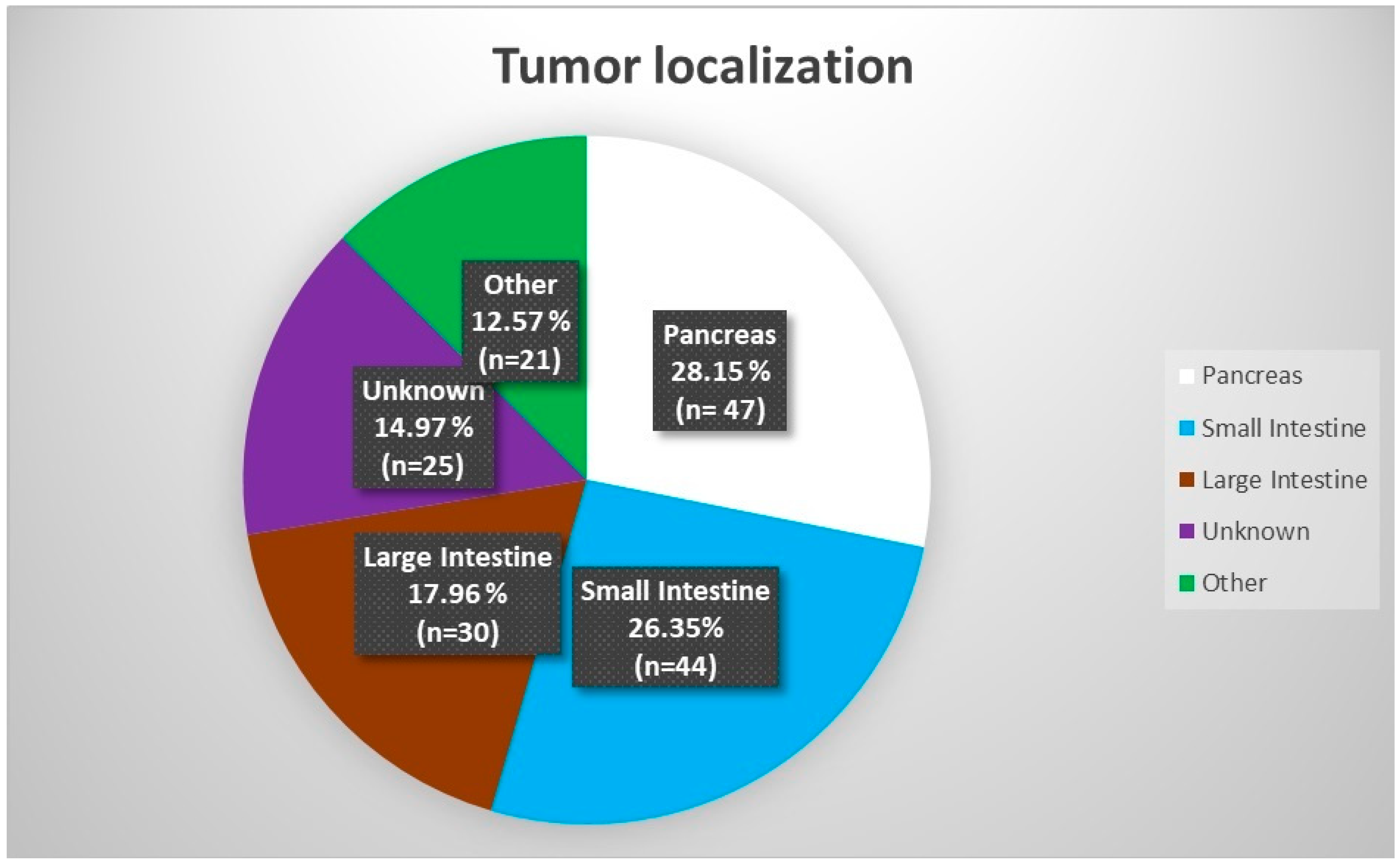
3.3. Tumor Location and Functionality
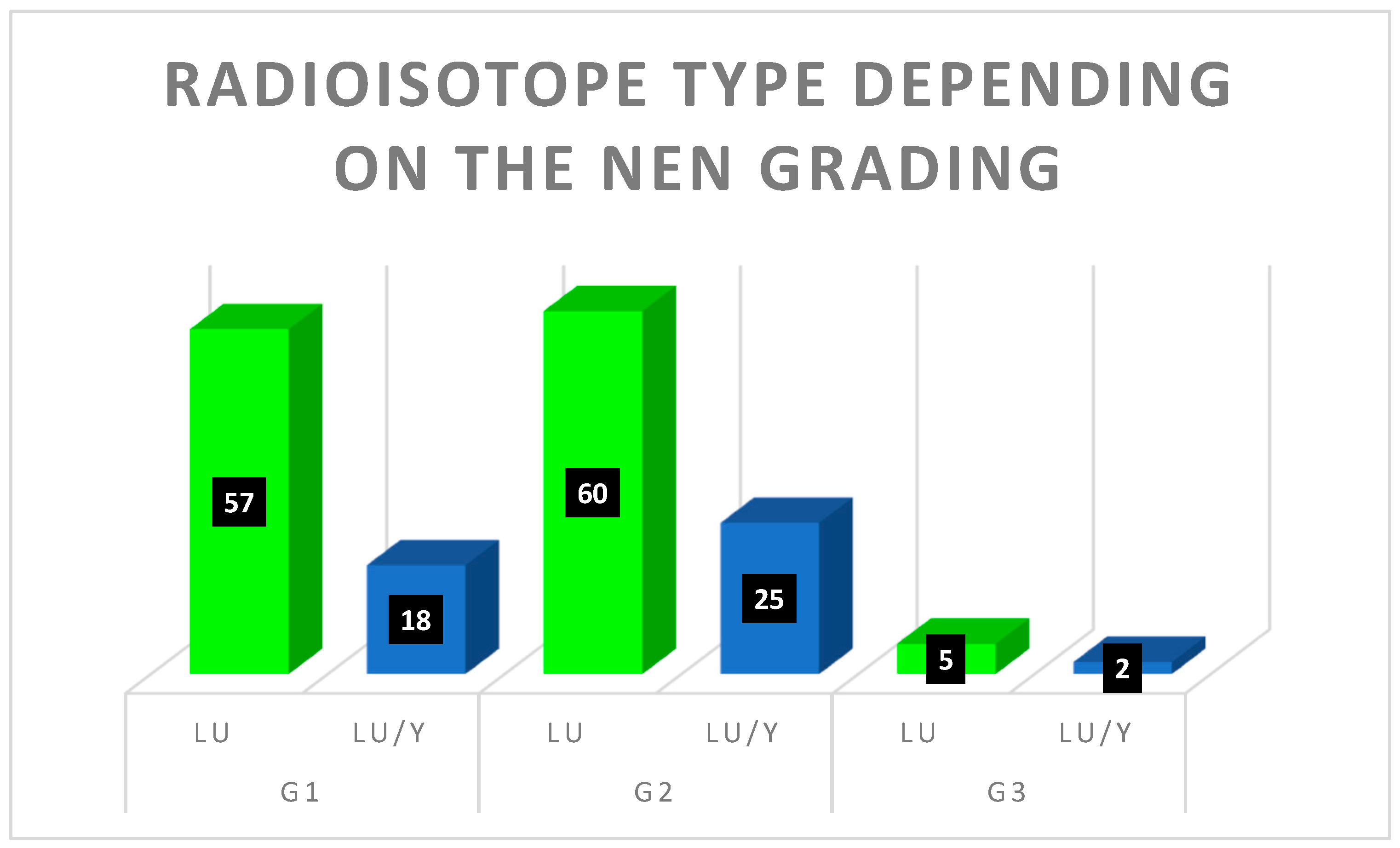
3.4. Advancement and Radioisotope
3.5. Previous Surgery and Chemotherapy
3.6. Somatostatin Analogues
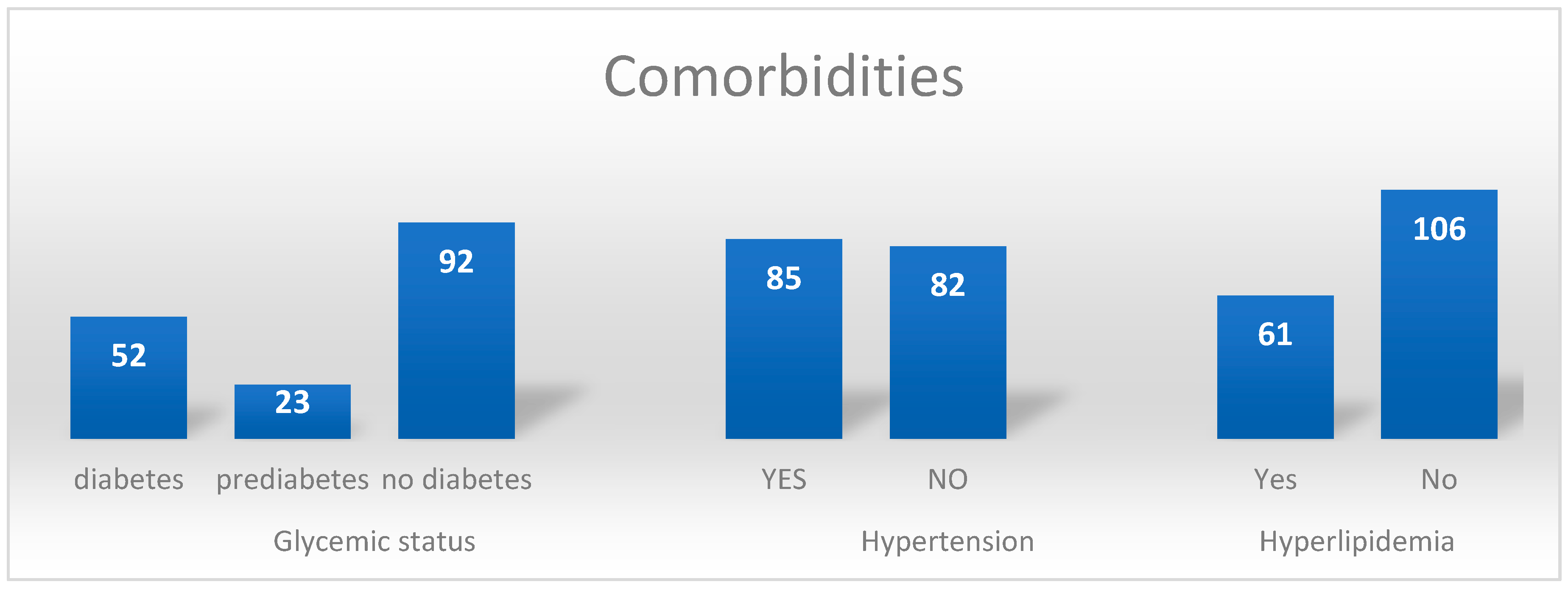
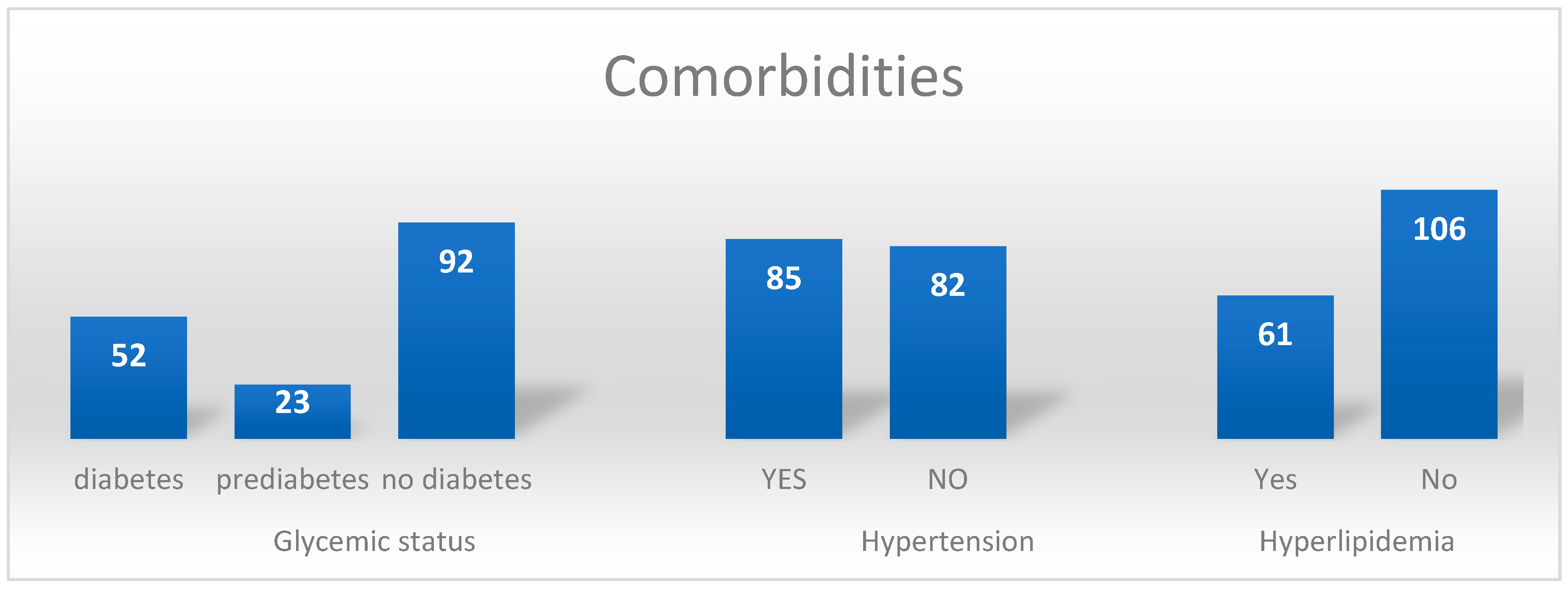
3.7. Comorbidities
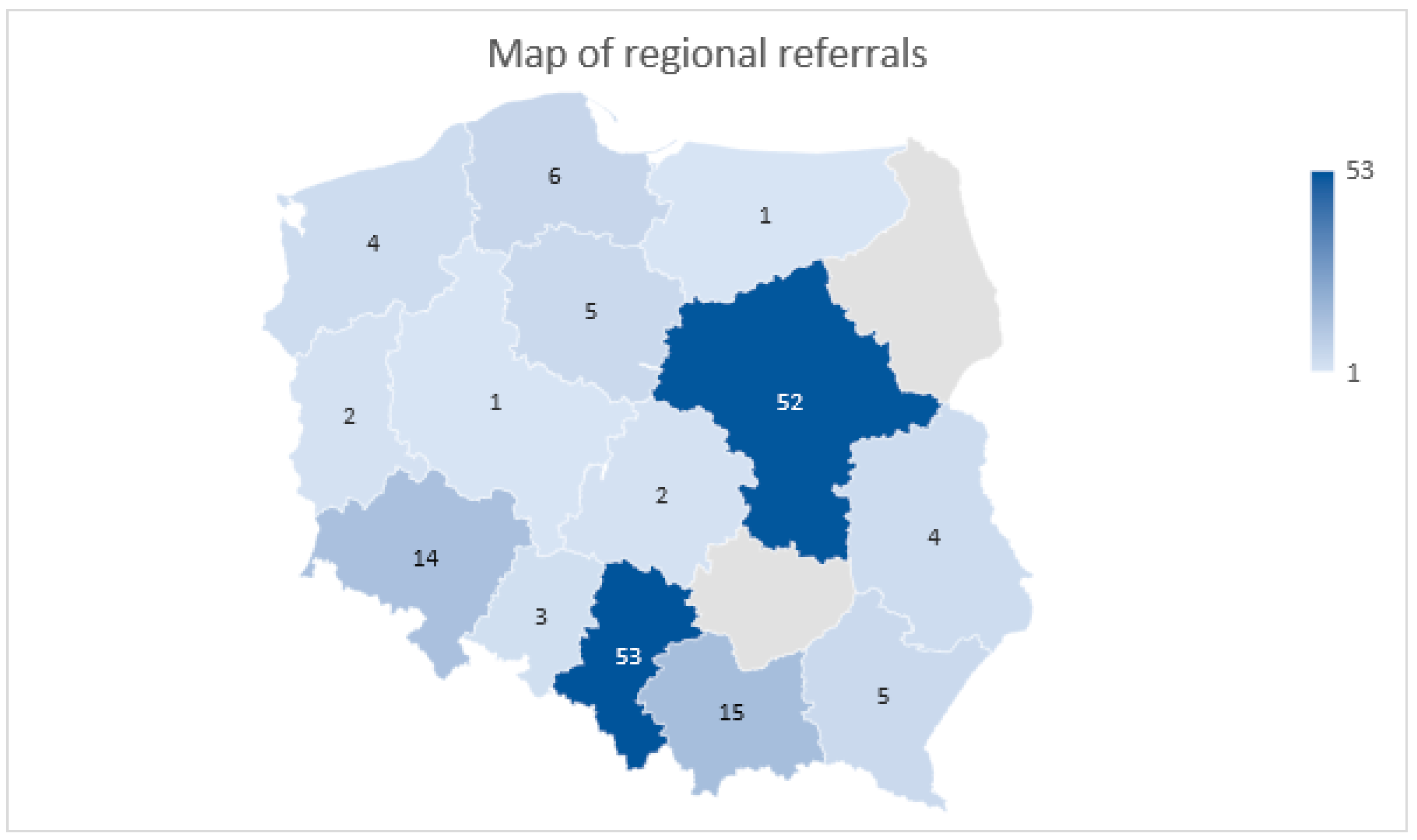
3.8. Regions of Referral
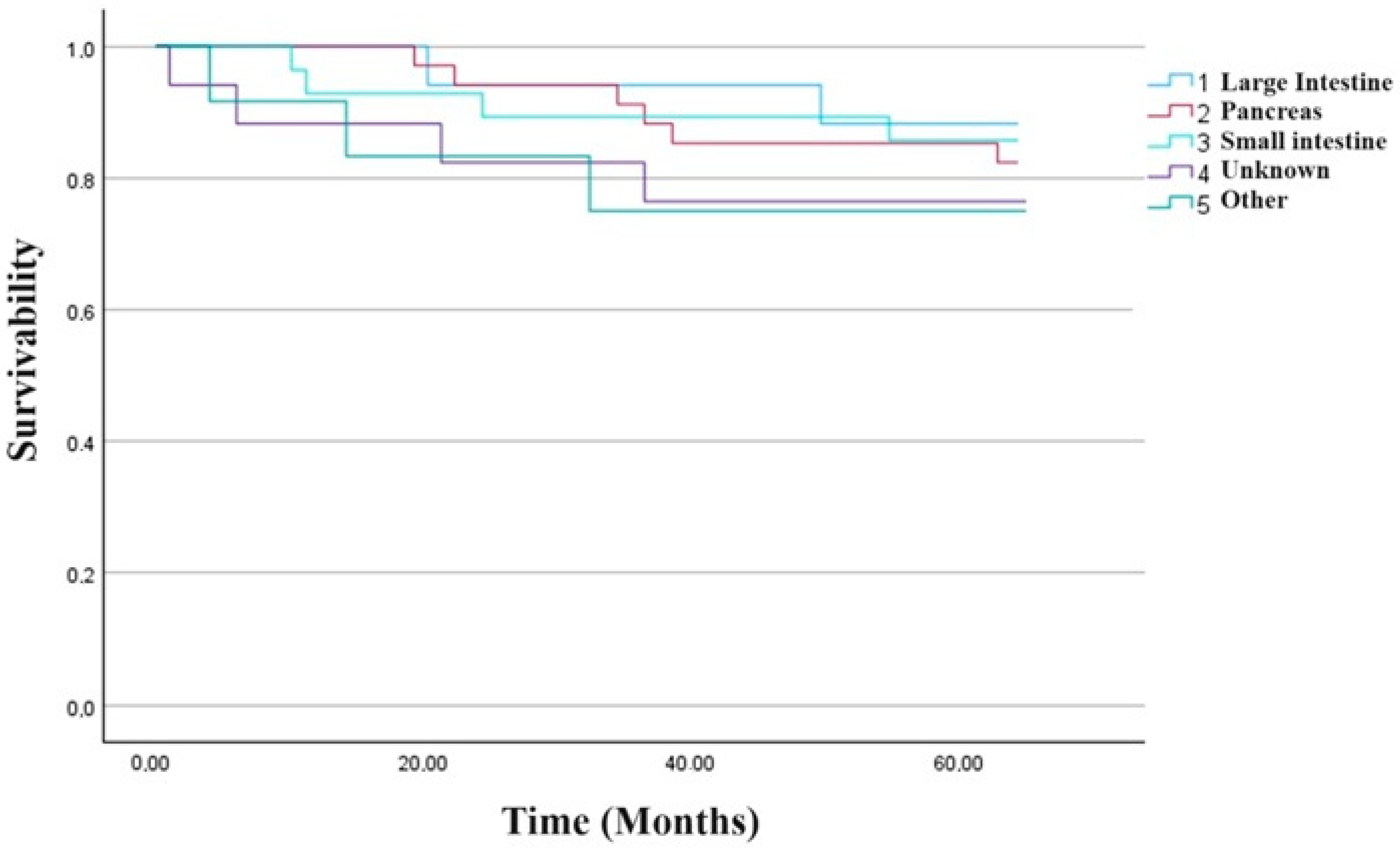
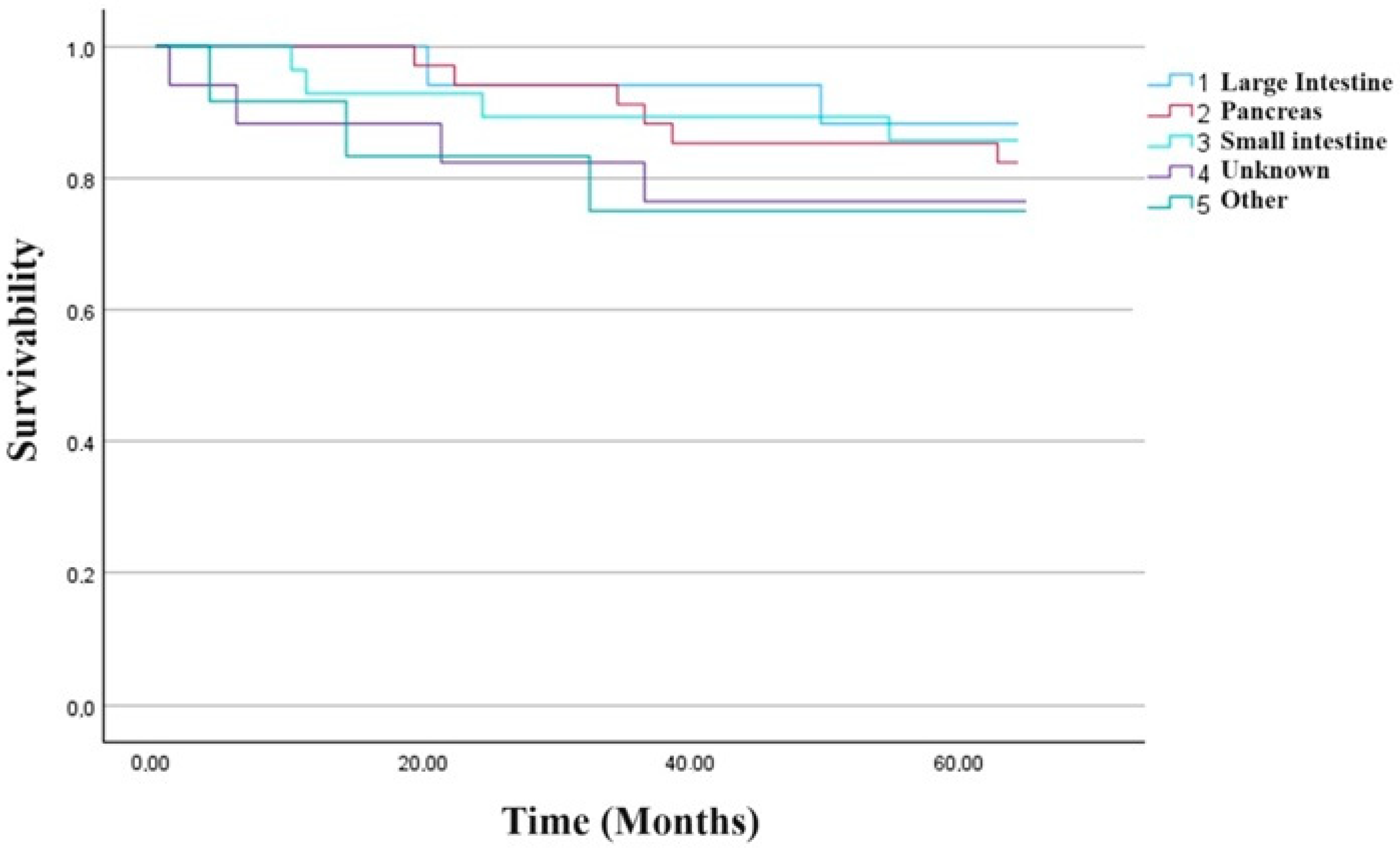
3.9. Treatment Outcomes
4. Discussion
5. Conclusions
6. Study Limitations
7. Study Strengths
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leotlela, P.D.; Jauch, A.; Holtgreve-Grez, H.; Thakker, R.V. Genetics of neuroendocrine and carcinoid tumours. Endocr.-Relat. Cancer 2003, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Raphael, M.J.; Chan, D.L.; Law, C.; Singh, S. Principles of diagnosis and management of neuroendocrine tumours. Can. Med. Assoc. J. 2017, 189, E398–E404. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Mete, O.; Uccella, S.; Basturk, O.; La Rosa, S.; Brosens, L.A.A.; Ezzat, S.; de Herder, W.W.; Klimstra, D.S.; Papotti, M.; et al. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocr. Pathol. 2022, 33, 115–154. [Google Scholar] [CrossRef] [PubMed]
- Kos-Kudła, B.; Foltyn, W.; Malczewska, A.; Bednarczuk, T.; Bolanowski, M.; Borowska, M.; Chmielik, E.; Ćwikła, J.B.; Gisterek, I.; Handkiewicz-Junak, D.; et al. Update of the diagnostic and therapeutic guidelines for gastro-entero-pancreatic neuroendocrine neoplasms (recommended by the Polish Network of Neuroendocrine Tumours). Endokrynol. Pol. 2022, 73, 387–454. [Google Scholar] [CrossRef]
- Spigel, D.R.; Hainsworth, J.D.; Greco, F.A. Neuroendocrine Carcinoma of Unknown Primary Site. Semin. Oncol. 2009, 36, 52–59. [Google Scholar] [CrossRef]
- Yao, J.C.; Hassan, M.M.; Phan, A.T.; Dagohoy, C.G.; Leary, C.C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.-N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef]
- Juhlin, C.C.; Zedenius, J.; Höög, A. Metastatic Neuroendocrine Neoplasms of Unknown Primary: Clues from Pathology Workup. Cancers 2022, 14, 2210. [Google Scholar] [CrossRef]
- Urso, L.; Nieri, A.; Rambaldi, I.; Castello, A.; Uccelli, L.; Cittanti, C.; Panareo, S.; Gagliardi, I.; Ambrosio, M.R.; Zatelli, M.C.; et al. Radioligand therapy (RLT) as neoadjuvant treatment for inoperable pancreatic neuroendocrine tumors: A literature review. Endocrine 2022, 78, 255–261. [Google Scholar] [CrossRef]
- Kolasińska-Ćwikła, A.; Łowczak, A.; Maciejkiewicz, K.M.; Ćwikła, J.B. Peptide Receptor Radionuclide Therapy for Advanced Gastroenteropancreatic Neuroendocrine Tumors—From oncology perspective. Nucl. Med. Rev. Cent. East Eur. 2018, 21, 115–124. [Google Scholar] [CrossRef]
- Piwowarska-Bilska, H.; Kurkowska, S.; Birkenfeld, B. Optimized method for normal range estimation of standardized uptake values (SUVmax, SUVmean) in liver SPECT/CT images with somatostatin analog [99mTc]-HYNIC-TOC (Tektrotyd). Nucl. Med. Rev. Cent. East Eur. 2022, 25, 37–46. [Google Scholar] [CrossRef]
- Paiella, S.; Landoni, L.; Tebaldi, S.; Zuffante, M.; Salgarello, M.; Cingarlini, S.; D’Onofrio, M.; Parisi, A.; Deiro, G.; Manfrin, E.; et al. Dual-Tracer (68Ga-DOTATOC and 18F-FDG-)-PET/CT Scan and G1-G2 Nonfunctioning Pancreatic Neuroendocrine Tumors: A Single-Center Retrospective Evaluation of 124 Nonmetastatic Resected Cases. Neuroendocrinology 2022, 112, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-H.; Chang, Y.-C.; Hwang, T.-L.; Chen, J.-S.; Chou, W.-C.; Hsieh, C.-H.; Yeh, T.-S.; Hsu, J.-T.; Yeh, C.-N.; Tseng, J.-H.; et al. 68Ga-DOTATOC and 18F-FDG PET/CT for identifying the primary lesions of suspected and metastatic neuroendocrine tumors: A prospective study in Taiwan. J. Formos. Med. Assoc. 2018, 117, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Sowa-Staszczak, A.; Pach, R.; Kunikowska, J.; Krolicki, L.; Stefanska, A.; Tomaszuk, M.; Buziak-Bereza, M.; Mikolajczak, R.; Matyja, M.; Gilis-Januszewska, A.; et al. Efficacy and safety of 90Y-DOTATATE therapy in neuroendocrine tumours. Endokrynol. Pol. 2011, 62, 392–400. [Google Scholar] [PubMed]
- Bodei, L.; Kidd, M.; Paganelli, G.; Grana, C.M.; Drozdov, I.; Cremonesi, M.; Lepensky, C.; Kwekkeboom, D.J.; Baum, R.P.; Krenning, E.P.; et al. Long-term tolerability of PRRT in 807 patients with neuroendocrine tumours: The value and limitations of clinical factors. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 5–19. [Google Scholar] [CrossRef]
- Kunikowska, J.; Królicki, L.; Hubalewska-Dydejczyk, A.; Mikołajczak, R.; Sowa-Staszczak, A.; Pawlak, D. Clinical Results of Radionuclide Therapy of Neuroendocrine Tumours with 90Y-DOTATATE and Tandem 90Y/177LuDOTATATE: Which Is a Better Therapy Option? Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1788–1797. [Google Scholar] [CrossRef]
- Ramage, J.; De Herder, W.; Fave, G.D.; Ferolla, P.; Ferone, D.; Ito, T.; Ruszniewski, P.; Sundin, A.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines Update for Colorectal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103, 139–143. [Google Scholar] [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A.; ESMO Guidelines Committee. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Öberg, K.; Castellano, D. Current knowledge on diagnosis and staging of neuroendocrine tumors. Cancer Metastasis Rev. 2011, 30 (Suppl. S1), 3–7. [Google Scholar] [CrossRef]
- Luchini, C.; Pantanowitz, L.; Adsay, V.; Asa, S.L.; Antonini, P.; Girolami, I.; Veronese, N.; Nottegar, A.; Cingarlini, S.; Landoni, L.; et al. Ki-67 assessment of pancreatic neuroendocrine neoplasms: Systematic review and meta-analysis of manual vs. digital pathology scoring. Mod. Pathol. 2022, 35, 712–720. [Google Scholar] [CrossRef]
- Farrell, J.M.; Pang, J.C.; Kim, G.E.; Tabatabai, Z.L. Pancreatic neuroendocrine tumors: Accurate grading with Ki-67 index on fine-needle aspiration specimens using the WHO 2010/ENETS criteria. Cancer Cytopathol. 2014, 122, 770–778. [Google Scholar] [CrossRef]
- Tacelli, M.; Bina, N.; Crinò, S.F.; Facciorusso, A.; Celsa, C.; Vanni, A.S.; Fantin, A.; Antonini, F.; Falconi, M.; Monica, F.; et al. Reliability of grading preoperative pancreatic neuroendocrine tumors on EUS specimens: A systematic review with meta-analysis of aggregate and individual data. Gastrointest. Endosc. 2022, 96, 898–908.e23. [Google Scholar] [CrossRef] [PubMed]
- Heidsma, C.M.; Tsilimigras, D.I.; Rocha, F.; Abbott, D.E.; Fields, R.; Smith, P.M.; Poultsides, G.A.; Cho, C.; van Eijck, C.; van Dijkum, E.N.; et al. Clinical relevance of performing endoscopic ultrasound-guided fine-needle biopsy for pancreatic neuroendocrine tumors less than 2 cm. J. Surg. Oncol. 2020, 122, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Hijioka, S.; Nagashio, Y.; Maruki, Y.; Ohba, A.; Takeshita, K.; Takasaki, T.; Agarie, D.; Hagiwara, Y.; Hara, H.; et al. Efficacy of endoscopic ultrasound-guided tissue acquisition for solid pancreatic lesions 20 mm or less in diameter suspected as neuroendocrine tumors or requiring differentiation. J. Gastroenterol. 2023, 58, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Mastrosimini, M.G.; Manfrin, E.; Remo, A.; De Bellis, M.; Parisi, A.; Pedron, S.; Luchini, C.; Brunelli, M.; Ammendola, S.; Bernardoni, L.; et al. Endoscopic ultrasound fine-needle biopsy to assess DAXX/ATRX expression and alternative lengthening of telomeres status in non-functional pancreatic neuroendocrine tumors. Pancreatology 2023, 23, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Baudin, E.; Gigliotti, A.; Ducreux, M.; Ropers, J.; Comoy, E.; Sabourin, J.; Bidart, J.; Cailleux, A.; Bonacci, R.; Ruffié, P.; et al. Neuron-specific enolase and chromogranin A as markers of neuroendocrine tumours. Br. J. Cancer 1998, 78, 1102–1107. [Google Scholar] [CrossRef]
- Fuksiewicz, M.; Kowalska, M.; Kolasińska-Ćwikła, A.; Ćwikła, J.B.; Sawicki, Ł.; Roszkowska-Purska, K.; Drygiel, J.; Kotowicz, B. Prognostic value of chromogranin A in patients with GET/NEN in the pancreas and the small intestine. Endocr. Connect. 2018, 7, 803–810. [Google Scholar] [CrossRef]
- Dąbkowski, K.; Starzyńska, T. Management of small, asymptomatic, non-functioning pancreatic neuroendocrine tumours: Follow-up, ablation, or surgery? Endokrynol. Pol. 2023, 74, 25–30. [Google Scholar] [CrossRef]
- Crinò, S.F.; Napoleon, B.; Facciorusso, A.; Lakhtakia, S.; Borbath, I.; Caillol, F.; Pham, K.D.-C.; Rizzatti, G.; Forti, E.; Palazzo, L.; et al. Endoscopic Ultrasound-guided Radiofrequency Ablation Versus Surgical Resection for Treatment of Pancreatic Insulinoma. Clin. Gastroenterol. Hepatol. 2023, 21, 2834–2843.e2. [Google Scholar] [CrossRef]
- Elkelany, O.O.; Karaisz, F.G.; Davies, B.; Krishna, S.G. An Overview of Pancreatic Neuroendocrine Tumors and an Update on Endoscopic Techniques for Their Management. Curr. Oncol. 2023, 30, 7566–7580. [Google Scholar] [CrossRef]
- Armellini, E.; Facciorusso, A.; Crinò, S.F. Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis. Medicina 2023, 59, 359. [Google Scholar] [CrossRef]
- Ebbers, S.C.; Braat, A.J.A.T.; Moelker, A.; Stokkel, M.P.M.; Lam, M.G.E.H.; Barentsz, M.W. Intra-arterial versus standard intravenous administration of lutetium-177-DOTA-octreotate in patients with NET liver metastases: Study protocol for a multicenter, randomized controlled trial (LUTIA trial). Trials 2020, 21, 141. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.L.; Singh, S. Current Chemotherapy Use in Neuroendocrine Tumors. Endocrinol. Metab. Clin. N. Am. 2018, 47, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Bardasi, C.; Spallanzani, A.; Benatti, S.; Spada, F.; Laffi, A.; Antonuzzo, L.; Lavacchi, D.; Marconcini, R.; Ferrari, M.; Rimini, M.; et al. Irinotecan-based chemotherapy in extrapulmonary neuroendocrine carcinomas: Survival and safety data from a multicentric Italian experience. Endocrine 2021, 74, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Andreetti, C.; Ibrahim, M.; Gagliardi, A.; Poggi, C.; Maurizi, G.; Armillotta, D.; Peritone, V.; Teodonio, L.; Rendina, E.A.; Venuta, F.; et al. Adjuvant chemotherapy, extent of resection, and immunoistochemical neuroendocrine markers as prognostic factors of early-stage large-cell neuroendocrine carcinoma. Thorac. Cancer 2022, 13, 900–912. [Google Scholar] [CrossRef]
- Oziel-Taieb, S.; Zemmour, C.; Raoul, J.-L.; Mineur, L.; Poizat, F.; Charrier, N.; Piana, G.; Cavaglione, G.; Niccoli, P. Efficacy of FOLFOX Chemotherapy in Metastatic Enteropancreatic Neuroendocrine Tumors. Anticancer. Res. 2021, 41, 2071–2078. [Google Scholar] [CrossRef] [PubMed]
- Cierniak-Piotrowska, M.; Dąbrowska, A.; Stelmach, K.; Statistics Poland, Demographic Surveys Department. Population. Size and Structure and Vital Statistics in Poland by Territorial Division in 2022. As of 30 June. Available online: https://stat.gov.pl/en/topics/population/population/population-size-and-structure-and-vital-statistics-in-poland-by-territorial-division-in-2022-as-of-30-june-2022,3,32.html (accessed on 28 September 2023).
- Das, S.; Dasari, A. Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms: Are There Global Differences? Curr. Oncol. Rep. 2021, 23, 43. [Google Scholar] [CrossRef]
- Lawrence, B.; Gustafsson, B.I.; Chan, A.; Svejda, B.; Kidd, M.; Modlin, I.M. The Epidemiology of Gastroenteropancreatic Neuroendocrine Tumors. Endocrinol. Metab. Clin. N. Am. 2011, 40, 1–18. [Google Scholar] [CrossRef]
- Hallet, J.; Law, C.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar]
- Scherübl, H.; Streller, B.; Stabenow, R.; Herbst, H.; Höpfner, M.; Schwertner, C.; Zappe, S.M. Clinically detected gastroenteropancreatic neuroendocrine tumors are on the rise: Epidemiological changes in Germany. World J. Gastroenterol. 2013, 19, 9012–9019. [Google Scholar] [CrossRef]
- Hauso, O.; Gustafsson, B.I.; Kidd, M.; Waldum, H.L.; Drozdov, I.; Chan, A.K.C.; Modlin, I.M. Neuroendocrine tumor epidemiology. Cancer 2008, 113, 2655–2664. [Google Scholar] [CrossRef]
- Tsai, H.-J.; Wu, C.-C.; Tsai, C.-R.; Lin, S.-F.; Chen, L.-T.; Chang, J.S. The Epidemiology of Neuroendocrine Tumors in Taiwan: A Nation-Wide Cancer Registry-Based Study. PLoS ONE 2013, 8, e62487. [Google Scholar] [CrossRef]
- Chang, J.S.; Chen, L.-T.; Shan, Y.-S.; Chu, P.-Y.; Tsai, C.-R.; Tsai, H.-J. An updated analysis of the epidemiologic trends of neuroendocrine tumors in Taiwan. Sci. Rep. 2021, 11, 7881. [Google Scholar] [CrossRef]
- Koizumi, T.; Otsuki, K.; Tanaka, Y.; Kanda, S. Epidemiology of neuroendocrine neoplasmas in Japan: Based on analysis of hospital-based cancer registry data, 2009–2015. BMC Endocr. Disord. 2022, 22, 105. [Google Scholar] [CrossRef]
- Gauci, J.; Azzopardi, N.; Babic, D.; Cortis, K.; Axisa, B. Neurofibromatosis Type 1. Pancreas 2022, 51, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Effraimidis, G.; Knigge, U.; Rossing, M.; Oturai, P.; Rasmussen, K.; Feldt-Rasmussen, U. Multiple endocrine neoplasia type 1 (MEN-1) and neuroendocrine neoplasms (NENs). Semin. Cancer Biol. 2022, 79, 141–162. [Google Scholar] [CrossRef] [PubMed]
- Binderup, M.L.M.; Smerdel, M.; Borgwadt, L.; Nielsen, S.S.B.; Madsen, M.G.; Møller, H.U.; Kiilgaard, J.F.; Friis-Hansen, L.; Harbud, V.; Cortnum, S.; et al. von Hippel-Lindau disease: Updated guideline for diagnosis and surveillance. Eur. J. Med. Genet. 2022, 65, 104538. [Google Scholar] [CrossRef]
- Zwolak, A.; Świrska, J.; Tywanek, E.; Dudzińska, M.; Tarach, J.S.; Matyjaszek-Matuszek, B. Pancreatic neuroendocrine tumours in patients with von Hippel-Lindau disease. Endokrynol. Pol. 2020, 71, 256–259. [Google Scholar] [CrossRef]
- Evans, L.M.; Geenen, K.R.; O’Shea, A.; Hedgire, S.S.; Ferrone, C.R.; Thiele, E.A. Tuberous sclerosis complex-associated nonfunctional pancreatic neuroendocrine tumors: Management and surgical outcomes. Am. J. Med. Genet. Part A 2022, 188, 2666–2671. [Google Scholar] [CrossRef]
- Sorbye, H.; Kong, G.; Grozinsky-Glasberg, S. PRRT in high-grade gastroenteropancreatic neuroendocrine neoplasms (WHO G3). Endocr.-Relat. Cancer 2020, 27, R67–R77. [Google Scholar] [CrossRef]
- de Mestier, L.; Walter, T.; Evrard, C.; de Boissieu, P.; Hentic, O.; Cros, J.; Ruszniewski, P. Temozolomide alone or combined with capecitabine for the treatment of advanced pancreatic neuroendo-crinetumor. Neuroendocrinology 2020, 110, 83–91. [Google Scholar] [CrossRef]
- Borga, C.; Businello, G.; Murgioni, S.; Bergamo, F.; Martini, C.; De Carlo, E.; Trevellin, E.; Vettor, R.; Fassan, M. Treatment personalization in gastrointestinal neuroendocrine tumors. Curr. Treat. Options Oncol. 2021, 22, 29. [Google Scholar] [CrossRef] [PubMed]
- Kohno, S. Diagnosis and Surgical Treatment of Gastroenteropancreatic Neuroendocrine Neoplasms: A Literature Review. Cancer Diagn. Progn. 2022, 2, 115–125. [Google Scholar] [CrossRef]
- Juhlin, C.C.; Skoglund, S.; Juntti-Berggren, L.; Karlberg, M.; Calissendorff, J. Non-functioning neuroendocrine pancreatic tumors transforming to malignant insulinomas - four cases and review of the literature. Neuro Endocrinol. Lett. 2019, 40, 175–183. [Google Scholar] [PubMed]
- Fang, J.M.; Li, J.; Shi, J. An update on the diagnosis of gastroenteropancreatic neuroendocrine neoplasms. World J. Gastroenterol. 2022, 28, 1009–1023. [Google Scholar] [CrossRef]
- de Herder, W.W.; Zandee, W.T.; Hofland, J. Insulinoma. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Portela-Gomes, G.M.; Stridsberg, M.; Grimelius, L.; Rorstad, O.; Janson, E.T. Differential Expression of the Five Somatostatin Receptor Subtypes in Human Benign and Malignant Insulinomas—Predominance of Receptor Subtype 4. Endocr. Pathol. 2007, 18, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.M.; Topliss, D.J.; Hamblin, P.S. Successful medical management of insulinoma with diazoxide for 27 years. Endocrinol. Diabetes Metab. Case Rep. 2020, 2020, 20-0132. [Google Scholar] [CrossRef]
- Rossi, R.E.; Elvevi, A.; Citterio, D.; Coppa, J.; Invernizzi, P.; Mazzaferro, V.; Massironi, S. Gastrinoma and Zollinger Ellison syndrome: A roadmap for the management between new and old therapies. World J. Gastroenterol. 2021, 27, 5890–5907. [Google Scholar] [CrossRef]
- Broder, M.S.; Beenhouwer, D.; Strosberg, J.R.; Neary, M.P.; Cherepanov, D. Gastrointestinal neuroendocrine tumors treated with high dose octreotide-LAR: A systematic literature review. World J. Gastroenterol. 2015, 21, 1945–1955. [Google Scholar] [CrossRef]
- Pavel, M.; Borson-Chazot, F.; Cailleux, A.; Hörsch, D.; Lahner, H.; Pivonello, R.; Tauchmanova, L.; Darstein, C.; Olsson, H.; Tiberg, F.; et al. Octreotide SC depot in patients with acromegaly and functioning neuroendocrine tumors: A phase 2, multicenter study. Cancer Chemother. Pharmacol. 2019, 83, 375–385. [Google Scholar] [CrossRef]
- Lepage, C.; Phelip, J.-M.; Lievre, A.; Le-Malicot, K.; Dahan, L.; Tougeron, D.; Toumpanakis, C.; Di-Fiore, F.; Lombard-Bohas, C.; Borbath, I.; et al. Lanreotide as maintenance therapy after first-line treatment in patients with non-resectable duodeno-pancreatic neuroendocrine tumours: An international double-blind, placebo-controlled randomised phase II trial—Prodige 31 REMINET: An FFCD study. Eur. J. Cancer 2022, 175, 31–40. [Google Scholar] [CrossRef]
- Paulson, S.; Ray, D.; Aranha, S.; Scales, A.; Wang, Y.; Liu, E. Lanreotide Depot to Treat Gastroenteropancreatic Neuroendocrine Tumors in a US Community Oncology Setting: A Prospective, Observational Study. Oncol. Ther. 2022, 10, 463–479. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.; McBride, A.; Ray, D.; Pulgar, S.; Ramirez, R.; Elquza, E.; Favaro, J.; Dranitsaris, G. Lanreotide vs octreotide LAR for patients with advanced gastroenteropancreatic neuroendocrine tumors: An observational time and motion analysis. J. Oncol. Pharm. Prat. 2019, 25, 1425–1433. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Caplin, M.E.; Kunz, P.L.; Ruszniewski, P.B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. 177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): Final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1752–1763. [Google Scholar] [CrossRef] [PubMed]
- Saracyn, M.; Durma, A.D.; Bober, B.; Kołodziej, M.; Lubas, A.; Kapusta, W.; Niemczyk, S.; Kamiński, G. Long-Term Complications of Radioligand Therapy with Lutetium-177 and Yttrium-90 in Patients with Neuroendocrine Neoplasms. Nutrients 2023, 15, 185. [Google Scholar] [CrossRef]
- Bober, B.; Saracyn, M.; Zaręba, K.; Lubas, A.; Mazurkiewicz, P.; Wilińska, E.; Kamiński, G. Early Complications of Radioisotope Therapy with Lutetium-177 and Yttrium-90 in Patients with Neuroendocrine Neoplasms—A Preliminary Study. J. Clin. Med. 2022, 11, 919. [Google Scholar] [CrossRef]
- Hörsch, D.; Ezziddin, S.; Haug, A.; Gratz, K.F.; Dunkelmann, S.; Miederer, M.; Schreckenberger, M.; Krause, B.J.; Bengel, F.M.; Bartenstein, P.; et al. Effectiveness and side-effects of peptide receptor radionuclide therapy for neuroendocrine neoplasms in Germany: A multi-institutional registry study with prospective follow-up. Eur. J. Cancer 2016, 58, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Brabander, T.; van der Zwan, W.A.; Teunissen, J.J.; Kam, B.L.; Feelders, R.A.; de Herder, W.W.; van Eijck, C.H.; Franssen, G.J.; Krenning, E.P.; Kwekkeboom, D.J. Long-Term Efficacy, Survival, and Safety of [177Lu-DOTA0,Tyr3]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin. Cancer Res. 2017, 23, 4617–4624. [Google Scholar] [CrossRef]
- Paganelli, G.; Sansovini, M.; Nicolini, S.; Grassi, I.; Ibrahim, T.; Amadori, E.; Di Iorio, V.; Monti, M.; Scarpi, E.; Bongiovanni, A.; et al. 177Lu-PRRT in advanced gastrointestinal neuroendocrine tumors: 10-year follow-up of the IRST phase II prospective study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 152–160. [Google Scholar] [CrossRef]
- Jiang, Y.; Liu, Q.; Wang, G.; Sui, H.; Wang, R.; Wang, J.; Zhang, J.; Zhu, Z.; Chen, X. Safety and efficacy of peptide receptor radionuclide therapy with 177Lu-DOTA-EB-TATE in patients with metastatic neuroendocrine tumors. Theranostics 2022, 12, 6437–6445. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Banegas, J.; Gijón-Conde, T. Epidemiología de la hipertensión arterial. Hipertens. Riesgo Vasc. 2017, 34 (Suppl. S2), 2–4. [Google Scholar] [CrossRef] [PubMed]
- Al Ghorani, H.; Götzinger, F.; Böhm, M.; Mahfoud, F. Arterial hypertension—Clinical trials update 2021. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 21–31. [Google Scholar] [CrossRef]
- Hisamatsu, T.; Segawa, H.; Kadota, A.; Ohkubo, T.; Arima, H.; Miura, K. Epidemiology of hypertension in Japan: Beyond the new 2019 Japanese guidelines. Hypertens. Res. 2020, 43, 1344–1351. [Google Scholar] [CrossRef] [PubMed]
- Saracyn, M.; Durma, A.D.; Bober, B.; Lubas, A.; Kołodziej, M.; Kapusta, W.; Dmochowska, B.; Kamiński, G. Renal Disturbances during and after Radioligand Therapy of Neuroendocrine Tumors—Extended Analysis of Potential Acute and Chronic Complications. Int. J. Mol. Sci. 2023, 24, 7508. [Google Scholar] [CrossRef] [PubMed]
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.A.; Ramaiya, K.L. Diabetes in developing countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef]
- Cappellani, D.; Urbani, C.; Sardella, C.; Scattina, I.; Marconcini, G.; Lupi, I.; Manetti, L.; Marcocci, C.; Bogazzi, F. Diabetes mellitus induced by somatostatin analogue therapy is not permanent in acromegalic patients. Endocrinol. Diabetes Metab. 2018, 2, e00033. [Google Scholar] [CrossRef]
- Teunissen, J.J.M.; Krenning, E.P.; de Jong, F.H.; de Rijke, Y.B.; Feelders, R.A.; van Aken, M.O.; de Herder, W.W.; Kwekkeboom, D.J. Effects of therapy with [177Lu-DOTA0,Tyr3]octreotate on endocrine function. Eur. J. Nucl. Med. 2009, 36, 1758–1766. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Guijarro, C.; Cosín-Sales, J. LDL cholesterol and atherosclerosis: The evidence. Clin. Investig. Arterioscler. 2021, 33 (Suppl. S1), 25–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Female (n = 85) | Male (n = 82) | Total (n = 167) | |
|---|---|---|---|---|
| Diagnosis | M | 56.95 | 57.51 | 57.23 |
| SD | 13.51 | 11.81 | 12.69 | |
| Treatment | M | 59.80 | 60.01 | 59.90 |
| SD | 12.85 | 11.83 | 12.36 |
| CgA before RLT | CgA after RLT | p | |||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | ||
| Carcinoid (n = 33) | 466.0 | 5050.6 | 383.5 | 7840.8 | 0.509 |
| * Functioning (n = 43) | 298.1 | 1941.7 | 227.6 | 5425.8 | 0.659 |
| Non-functioning (n = 79) | 96.9 | 240.1 | 82.8 | 187.6 | 0.018 |
| Total (n = 122) | 133.1 | 359.4 | 102.9 | 395.0 | 0.034 |
| No Surgery | Feature | Results |
|---|---|---|
| Age | M | 61.8 y.o. |
| SD | 10.2 y.o. | |
| Gender | Female | n = 25 |
| Male | n = 26 | |
| Location | pancreas | n = 20 |
| unknown | n = 20 | |
| other | n = 7 | |
| small intestine | n = 4 |
| I | capecitabine + temozolomide | CAPTEM | n = 7 |
| etoposide + cisplatin | E/P | n = 6 | |
| everolimus | EVR | n = 5 | |
| unknown | UNK | n = 4 | |
| sunitinib | SU | n = 2 | |
| capecitabine + oxaliplatin | XELOX | n = 2 | |
| 5-fluorouracil | 5FU | n = 1 | |
| 5-fluorouracil + leucovorin | 5FU/LV | n = 1 | |
| gemcitabine | GEM | n = 1 | |
| cisplatin + vinorelbine | PN | n = 1 | |
| folinic acid, fluorouracil and irinotecan | FOLFIRI | n = 1 | |
| Etoposide + carboplatin | E/CP | n = 1 | |
| II | docetaxel | DTX | n = 1 |
| 5-fluorouracil + leucovorin | 5FU/LV | n = 1 | |
| III | capecitabine + temozolomide | CAPTEM | n = 1 |
| n | Med. [Months] | IQR | |
|---|---|---|---|
| OS | 13 | 34.0 | 16.0 |
| PFS | 28 | 29.3 | 23.9 |
| OTS | 67 | 29.8 | 22.6 |
| UNK | 19 | NA | |
| Radioisotope | [177Lu]Lu-DOTA-TATE (n = 99) | [177Lu]Lu-DOTA-TATE/[90Y]Y-DOTA-TATE (n = 28) | |||||
|---|---|---|---|---|---|---|---|
| Parameter | n | Med. | IQR | n | Med. | IQR | p |
| OS | 10 | 30.0 | 21.5 | 3 | 34.0 | 15.0 | 0.469 |
| PFS | 22 | 29.3 | 21.1 | 34 | 28.2 | 27.7 | 0.935 |
| OTs | 54 | 29.8 | 21.1 | 15 | 29.2 | 27.7 | 0.868 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durma, A.D.; Saracyn, M.; Kołodziej, M.; Jóźwik-Plebanek, K.; Dmochowska, B.; Kapusta, W.; Żmudzki, W.; Mróz, A.; Kos-Kudła, B.; Kamiński, G. Epidemiology of Neuroendocrine Neoplasms and Results of Their Treatment with [177Lu]Lu-DOTA-TATE or [177Lu]Lu-DOTA-TATE and [90Y]Y-DOTA-TATE—A Six-Year Experience in High-Reference Polish Neuroendocrine Neoplasm Center. Cancers 2023, 15, 5466. https://doi.org/10.3390/cancers15225466
Durma AD, Saracyn M, Kołodziej M, Jóźwik-Plebanek K, Dmochowska B, Kapusta W, Żmudzki W, Mróz A, Kos-Kudła B, Kamiński G. Epidemiology of Neuroendocrine Neoplasms and Results of Their Treatment with [177Lu]Lu-DOTA-TATE or [177Lu]Lu-DOTA-TATE and [90Y]Y-DOTA-TATE—A Six-Year Experience in High-Reference Polish Neuroendocrine Neoplasm Center. Cancers. 2023; 15(22):5466. https://doi.org/10.3390/cancers15225466
Chicago/Turabian StyleDurma, Adam Daniel, Marek Saracyn, Maciej Kołodziej, Katarzyna Jóźwik-Plebanek, Beata Dmochowska, Waldemar Kapusta, Wawrzyniec Żmudzki, Adrianna Mróz, Beata Kos-Kudła, and Grzegorz Kamiński. 2023. "Epidemiology of Neuroendocrine Neoplasms and Results of Their Treatment with [177Lu]Lu-DOTA-TATE or [177Lu]Lu-DOTA-TATE and [90Y]Y-DOTA-TATE—A Six-Year Experience in High-Reference Polish Neuroendocrine Neoplasm Center" Cancers 15, no. 22: 5466. https://doi.org/10.3390/cancers15225466
APA StyleDurma, A. D., Saracyn, M., Kołodziej, M., Jóźwik-Plebanek, K., Dmochowska, B., Kapusta, W., Żmudzki, W., Mróz, A., Kos-Kudła, B., & Kamiński, G. (2023). Epidemiology of Neuroendocrine Neoplasms and Results of Their Treatment with [177Lu]Lu-DOTA-TATE or [177Lu]Lu-DOTA-TATE and [90Y]Y-DOTA-TATE—A Six-Year Experience in High-Reference Polish Neuroendocrine Neoplasm Center. Cancers, 15(22), 5466. https://doi.org/10.3390/cancers15225466