
Time Trends in the Treatment and Survival of 5036 Uveal Melanoma Patients in The Netherlands over a 30-Year Period

 , , , , and
, , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Retrieval
2.2. Definitions
2.3. Outcome Measures
2.4. Survival
2.5. Statistical Analysis
3. Results
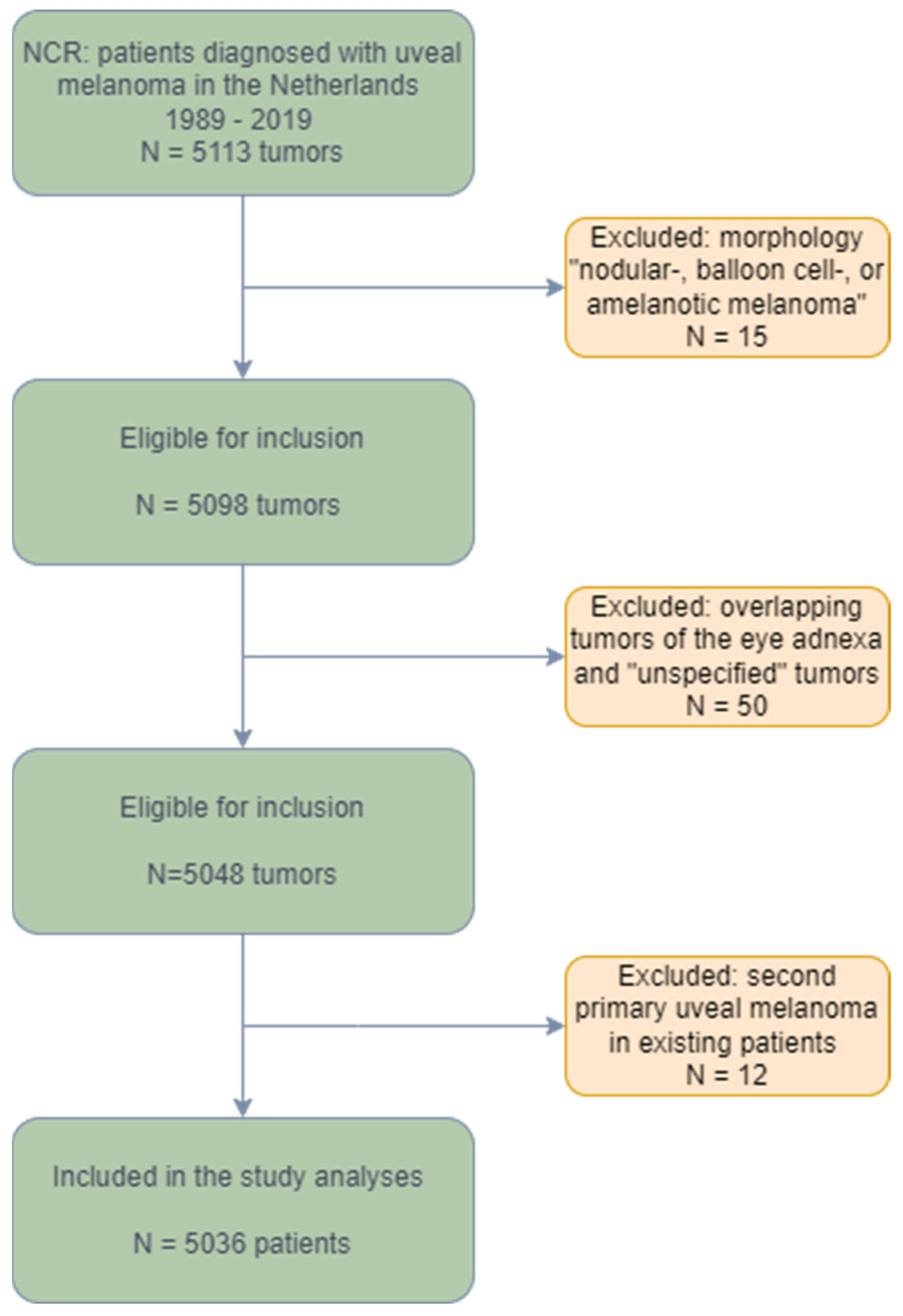
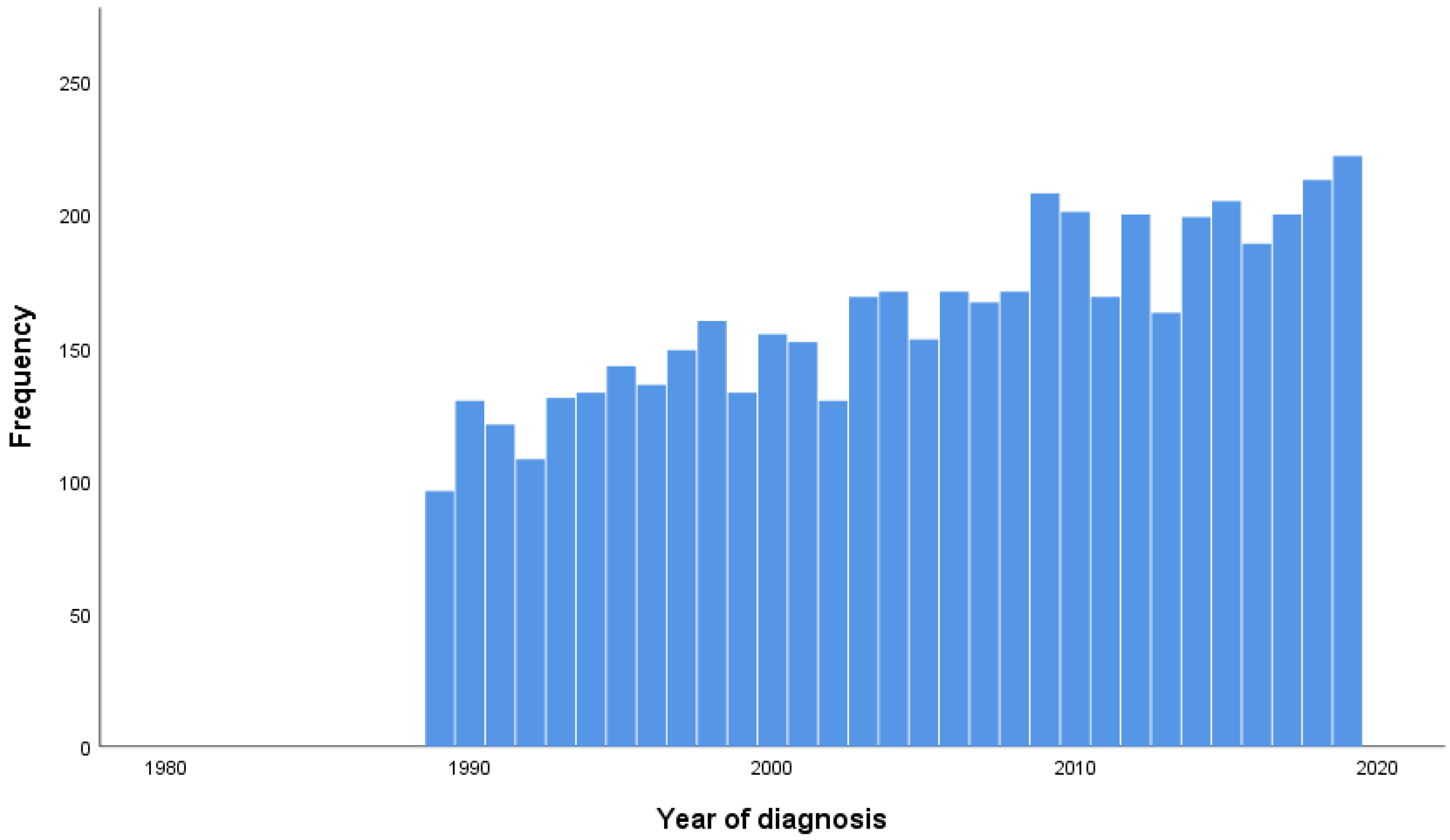
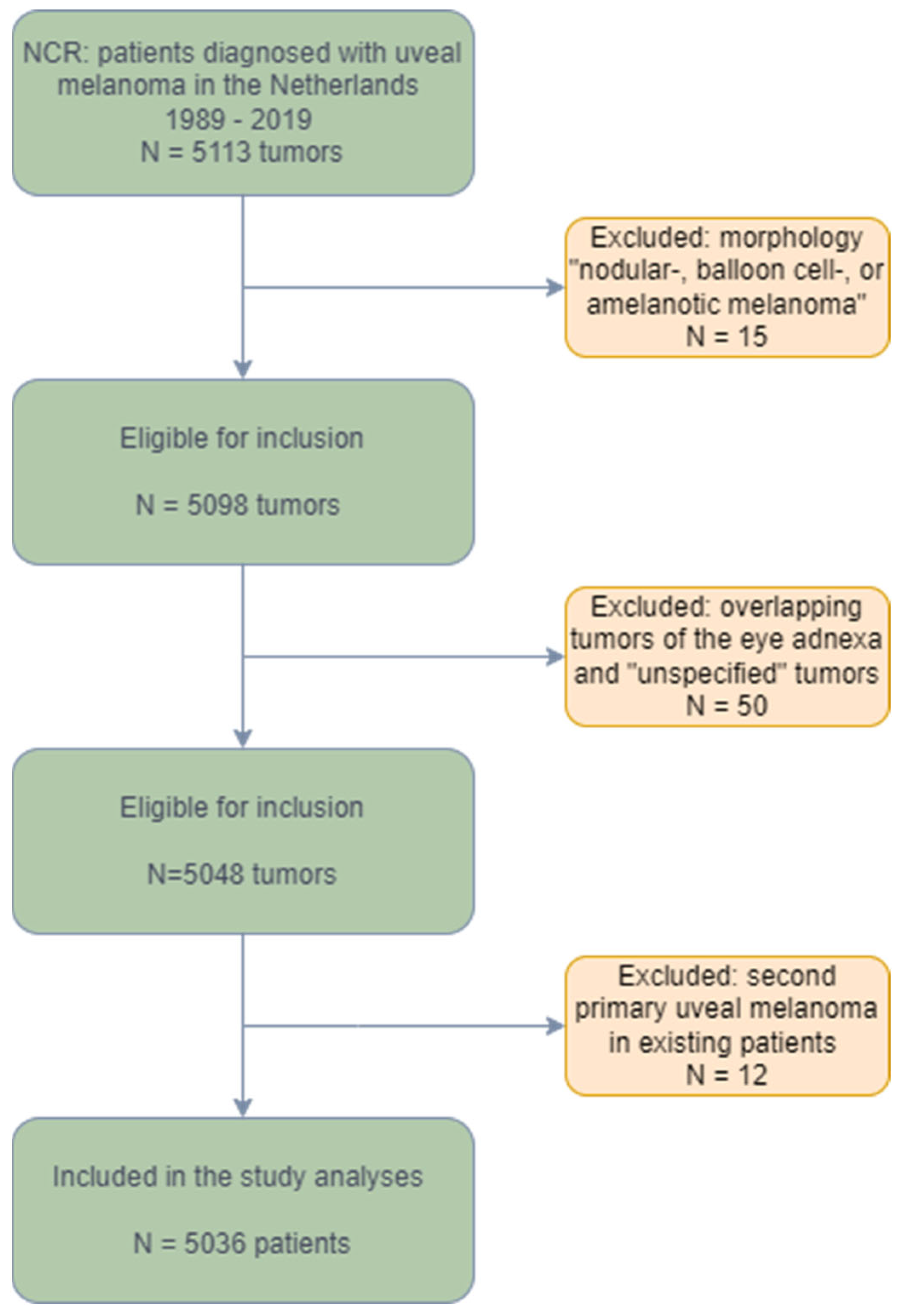
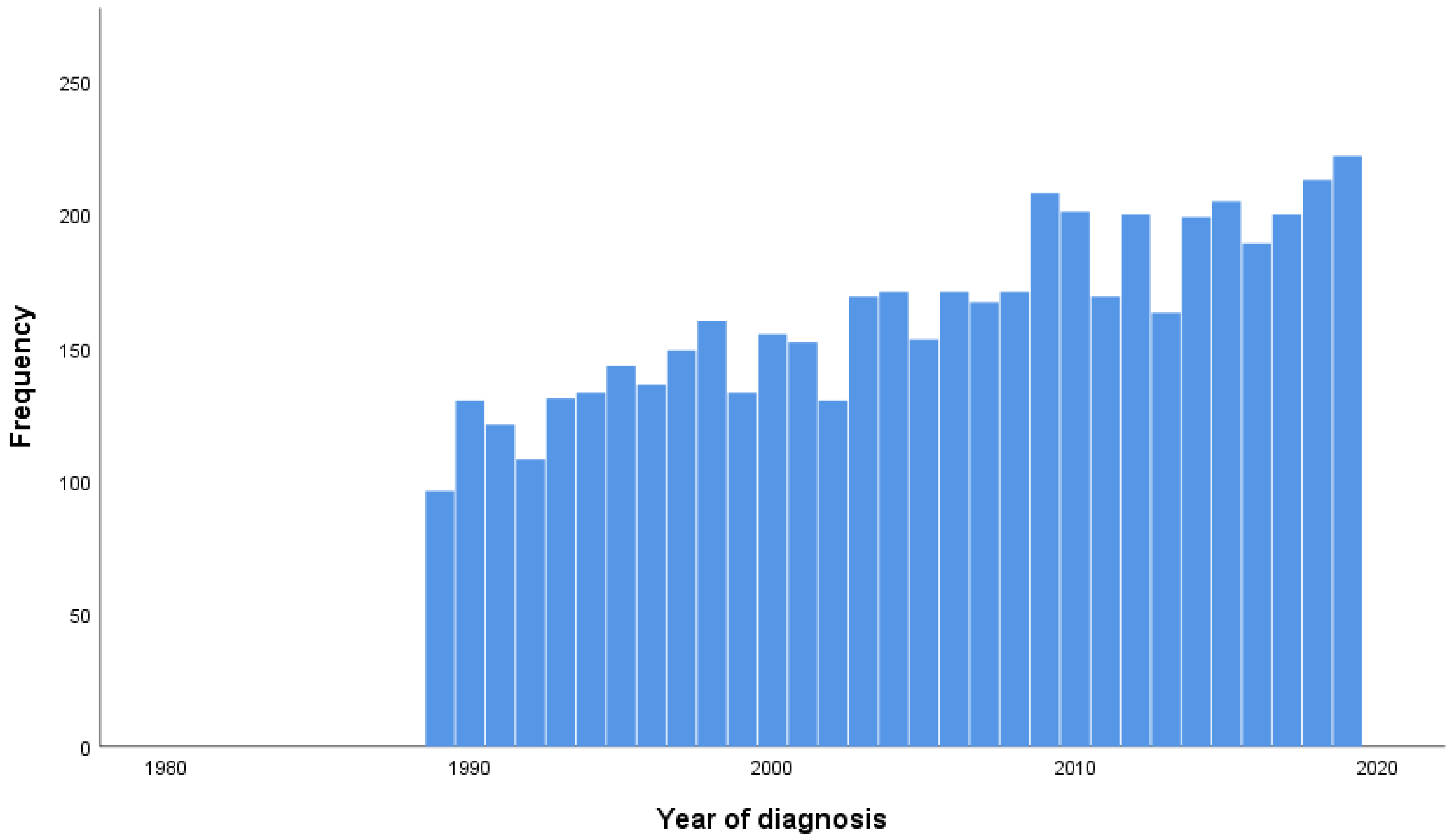
3.1. Study Population
3.2. Treatments
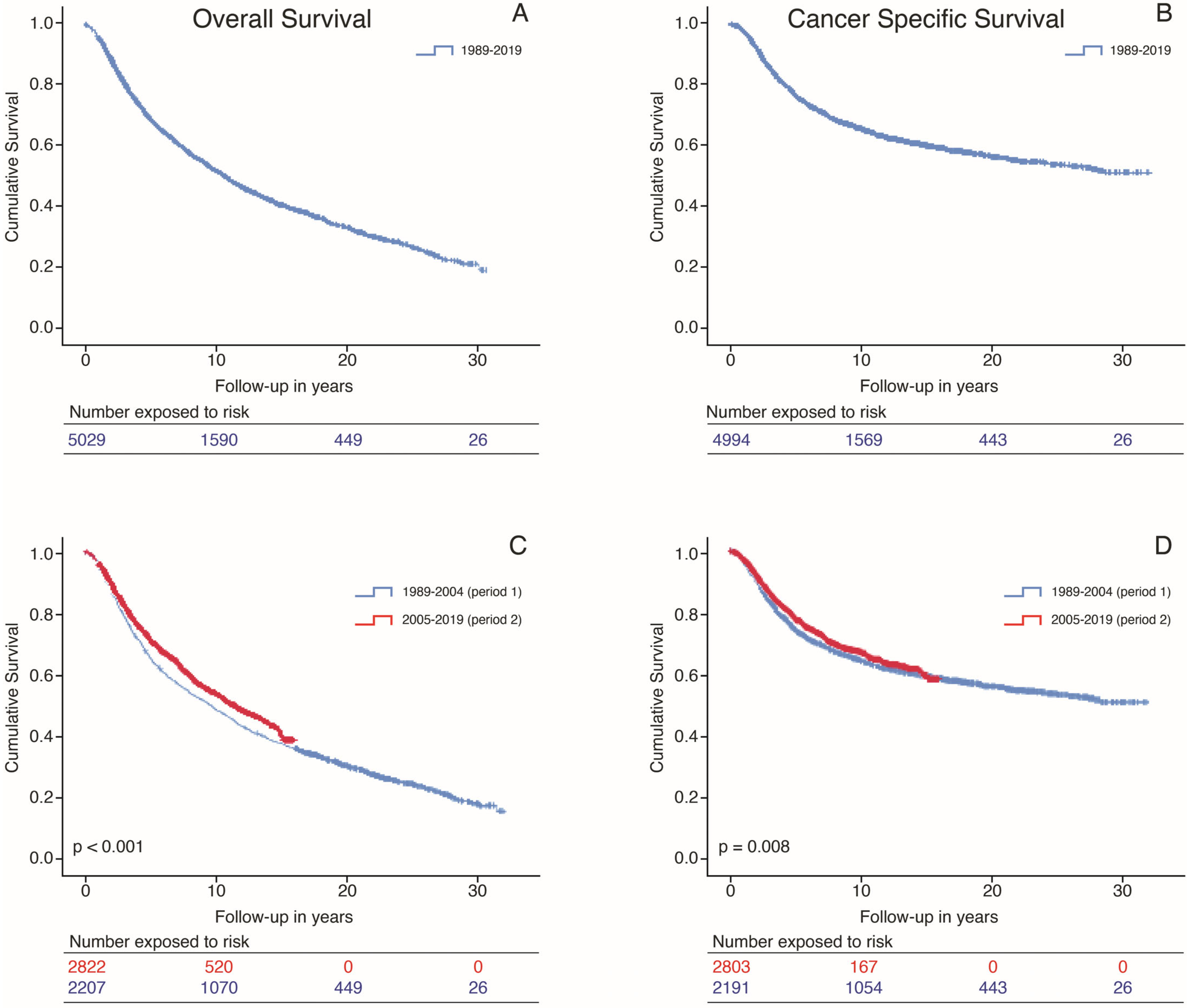
3.3. Overall Survival and Cancer-Specific Survival
3.4. Variables Associated with OS and CSS in UVA
3.5. Variables Associated with OS and CSS in MVA
3.6. Adjusted Models for Period of Diagnosis in MVA
4. Discussion
4.1. Survival over Time
4.2. Treatment over Time
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Damato, B. Treatment of primary intraocular melanoma. Expert Rev. Anticancer Ther. 2006, 6, 493–506. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.M.; Paci, E.; EUROCARE Working Group. Incidence of uveal melanoma in Europe. Ophthalmology 2007, 114, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Aronow, M.E.; Topham, A.K.; Singh, A.D. Uveal Melanoma: 5-Year Update on Incidence, Treatment, and Survival (SEER 1973–2013). Ocul. Oncol. Pathol. 2018, 4, 145–151. [Google Scholar] [CrossRef]
- Damato, B. Does ocular treatment of uveal melanoma influence survival? Br. J. Cancer 2010, 103, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Souto, E.B.; Zielinska, A.; Luis, M.; Carbone, C.; Martins-Gomes, C.; Souto, S.B.; Silva, A.M. Uveal melanoma: Physiopathology and new in situ-specific therapies. Cancer Chemother. Pharmacol. 2019, 84, 15–32. [Google Scholar] [CrossRef]
- Jager, M.J.; Shields, C.L.; Cebulla, C.M.; Abdel-Rahman, M.H.; Grossniklaus, H.E.; Stern, M.H.; Carvajal, R.D.; Belfort, R.N.; Jia, R.; Shields, J.A.; et al. Uveal melanoma. Nat. Rev. Dis. Primers 2020, 6, 24. [Google Scholar] [CrossRef]
- Gragoudas, E.; Li, W.; Goitein, M.; Lane, A.M.; Munzenrider, J.E.; Egan, K.M. Evidence-based estimates of outcome in patients irradiated for intraocular melanoma. Arch. Ophthalmol. 2002, 120, 1665–1671. [Google Scholar] [CrossRef]
- Caujolle, J.P.; Paoli, V.; Chamorey, E.; Maschi, C.; Baillif, S.; Herault, J.; Gastaud, P.; Hannoun-Levi, J.M. Local recurrence after uveal melanoma proton beam therapy: Recurrence types and prognostic consequences. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1218–1224. [Google Scholar] [CrossRef]
- Kowal, J.; Markiewicz, A.; Debicka-Kumela, M.; Bogdali, A.; Jakubowska, B.; Karska-Basta, I.; Romanowska-Dixon, B. Analysis of local recurrence causes in uveal melanoma patients treated with (125)I brachytherapy—A single institution study. J. Contemp. Brachytherapy 2019, 11, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Diener-West, M.; Reynolds, S.M.; Agugliaro, D.J.; Caldwell, R.; Cumming, K.; Earle, J.D.; Hawkins, B.S.; Hayman, J.A.; Jaiyesimi, I.; Jampol, L.M.; et al. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2005, 123, 1639–1643. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Mäkitie, T.; Kivelä, T. Very long-term prognosis of patients with malignant uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, M.; Horeweg, N.; Fiocco, M.; Peters, F.P.; Sommers, L.W.; Laman, M.S.; Bleeker, J.C.; Ketelaars, M.; Luyten, G.P.; Creutzberg, C.L. Ruthenium-106 brachytherapy for choroidal melanoma without transpupillary thermotherapy: Similar efficacy with improved visual outcome. Eur. J. Cancer 2016, 68, 106–113. [Google Scholar] [CrossRef]
- Gelmi, M.C.; Bas, Z.; Malkani, K.; Ganguly, A.; Shields, C.L.; Jager, M.J. Adding the Cancer Genome Atlas Chromosome Classes to American Joint Committee on Cancer System Offers More Precise Prognostication in Uveal Melanoma. Ophthalmology 2022, 129, 431–437. [Google Scholar] [CrossRef]
- Eskelin, S.; Pyrhönen, S.; Hahka-Kemppinen, M.; Tuomaala, S.; Kivelä, T. A prognostic model and staging for metastatic uveal melanoma. Cancer 2003, 97, 465–475. [Google Scholar] [CrossRef]
- Rietschel, P.; Panageas, K.S.; Hanlon, C.; Patel, A.; Abramson, D.H.; Chapman, P.B. Variates of survival in metastatic uveal melanoma. J. Clin. Oncol. 2005, 23, 8076–8080. [Google Scholar] [CrossRef]
- Rowcroft, A.; Loveday, B.P.T.; Thomson, B.N.J.; Banting, S.; Knowles, B. Systematic review of liver directed therapy for uveal melanoma hepatic metastases. HPB 2020, 22, 497–505. [Google Scholar] [CrossRef]
- Gonsalves, C.F.; Adamo, R.D.; Eschelman, D.J. Locoregional Therapies for the Treatment of Uveal Melanoma Hepatic Metastases. Semin. Interv. Radiol. 2020, 37, 508–517. [Google Scholar] [CrossRef]
- Meijer, T.S.; Burgmans, M.C.; de Leede, E.M.; de Geus-Oei, L.F.; Boekestijn, B.; Handgraaf, H.J.M.; Hilling, D.E.; Lutjeboer, J.; Vuijk, J.; Martini, C.H.; et al. Percutaneous Hepatic Perfusion with Melphalan in Patients with Unresectable Ocular Melanoma Metastases Confined to the Liver: A Prospective Phase II Study. Ann. Surg. Oncol. 2021, 28, 1130–1141. [Google Scholar] [CrossRef]
- Nathan, P.; Hassel, J.C.; Rutkowski, P.; Baurain, J.-F.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N. Engl. J. Med. 2021, 385, 1196–1206. [Google Scholar] [CrossRef]
- Netherlands Cancer Registry (NCR). Available online: https://iknl.nl/nkr-cijfers (accessed on 1 March 2023).
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Roelofsen, C.D.M.; Wierenga, A.P.A.; van Duinen, S.; Verdijk, R.M.; Bleeker, J.; Marinkovic, M.; Luyten, G.P.M.; Jager, M.J. Five Decades of Enucleations for Uveal Melanoma in One Center: More Tumors with High Risk Factors, No Improvement in Survival over Time. Ocul. Oncol. Pathol. 2021, 7, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Khoja, L.; Atenafu, E.G.; Suciu, S.; Leyvraz, S.; Sato, T.; Marshall, E.; Keilholz, U.; Zimmer, L.; Patel, S.P.; Piperno-Neumann, S.; et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: An international rare cancers initiative (IRCI) ocular melanoma study. Ann. Oncol. 2019, 30, 1370–1380. [Google Scholar] [CrossRef] [PubMed]
- Rantala, E.S.; Hernberg, M.; Kivela, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef]
- Beasley, A.B.; Preen, D.B.; McLenachan, S.; Gray, E.S.; Chen, F.K. Incidence and mortality of uveal melanoma in Australia (1982–2014). Br. J. Ophthalmol. 2021, 107, 406–411. [Google Scholar] [CrossRef]
- Stålhammar, G.; Herrspiegel, C. Long-term relative survival in uveal melanoma: A systematic review and meta-analysis. Commun. Med. 2022, 2, 18. [Google Scholar] [CrossRef]
- Reichstein, D.; Brock, A.; Lietman, C.; McKean, M. Treatment of metastatic uveal melanoma in 2022: Improved treatment regimens and improved prognosis. Curr. Opin. Ophthalmol. 2022, 33, 585–590. [Google Scholar] [CrossRef]
- Greene, F.L.; Page, D.L.; Fleming, I.D.; Fritz, A.G.; Balch, C.M.; Haller, D.G.; Morrow, M. (Eds.) AJCC Cancer Staging Manual, 6th ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Feinstein, A.R.; Sosin, D.M.; Wells, C.K. The Will Rogers phenomenon—Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N. Engl. J. Med. 1985, 312, 1604–1608. [Google Scholar] [CrossRef]
- Al-Jamal, R.T.; Cassoux, N.; Desjardins, L.; Damato, B.; Konstantinidis, L.; Coupland, S.E.; Heimann, H.; Petrovic, A.; Zografos, L.; Schalenbourg, A.; et al. The Pediatric Choroidal and Ciliary Body Melanoma Study: A Survey by the European Ophthalmic Oncology Group. Ophthalmology 2016, 123, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.K., Jr.; Di Nicola, M. Ocular Oncology-Primary and Metastatic Malignancies. Med. Clin. N. Am. 2021, 105, 531–550. [Google Scholar] [CrossRef] [PubMed]
- Piperno-Neumann, S.; Kapiteijn, E.; Larkin, J.M.G.; Carvajal, R.D.; Luke, J.J.; Seifert, H.; Roozen, I.; Zoubir, M.; Yang, L.; Choudhury, S.; et al. Phase I dose-escalation study of the protein kinase C (PKC) inhibitor AEB071 in patients with metastatic uveal melanoma. J. Clin. Oncol. 2014, 32, 9030. [Google Scholar] [CrossRef]
- Carvajal, R.D.; Piperno-Neumann, S.; Kapiteijn, E.; Chapman, P.B.; Frank, S.; Joshua, A.M.; Piulats, J.M.; Wolter, P.; Cocquyt, V.; Chmielowski, B.; et al. Selumetinib in Combination With Dacarbazine in Patients with Metastatic Uveal Melanoma: A Phase III, Multicenter, Randomized Trial (SUMIT). J. Clin. Oncol. 2018, 36, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Piperno-Neumann, S.; Larkin, J.; Carvajal, R.D.; Luke, J.J.; Schwartz, G.K.; Hodi, F.S.; Sablin, M.P.; Shoushtari, A.N.; Szpakowski, S.; Chowdhury, N.R.; et al. Genomic Profiling of Metastatic Uveal Melanoma and Clinical Results of a Phase I Study of the Protein Kinase C Inhibitor AEB071. Mol. Cancer Ther. 2020, 19, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Amaral, T.; Kähler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined immune checkpoint blockade for metastatic uveal melanoma: A retrospective, multi-center study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef]
- Bol, K.F.; Ellebaek, E.; Hoejberg, L.; Bagger, M.M.; Larsen, M.S.; Klausen, T.W.; Køhler, U.H.; Schmidt, H.; Bastholt, L.; Kiilgaard, J.F.; et al. Real-World Impact of Immune Checkpoint Inhibitors in Metastatic Uveal Melanoma. Cancers 2019, 11, 1489. [Google Scholar] [CrossRef]
- Najjar, Y.G.; Navrazhina, K.; Ding, F.; Bhatia, R.; Tsai, K.; Abbate, K.; Durden, B.; Eroglu, Z.; Bhatia, S.; Park, S.; et al. Ipilimumab plus nivolumab for patients with metastatic uveal melanoma: A multicenter, retrospective study. J. Immunother. Cancer 2020, 8, e000331. [Google Scholar] [CrossRef]
- Pelster, M.S.; Gruschkus, S.K.; Bassett, R.; Gombos, D.S.; Shephard, M.; Posada, L.; Glover, M.S.; Simien, R.; Diab, A.; Hwu, P.; et al. Nivolumab and Ipilimumab in Metastatic Uveal Melanoma: Results From a Single-Arm Phase II Study. J. Clin. Oncol. 2021, 39, 599–607. [Google Scholar] [CrossRef]
- Piulats, J.M.; Espinosa, E.; de la Cruz Merino, L.; Varela, M.; Alonso Carrion, L.; Martin-Algarra, S.; Lopez Castro, R.; Curiel, T.; Rodriguez-Abreu, D.; Redrado, M.; et al. Nivolumab Plus Ipilimumab for Treatment-Naive Metastatic Uveal Melanoma: An Open-Label, Multicenter, Phase II Trial by the Spanish Multidisciplinary Melanoma Group (GEM-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef]
- Koch, E.A.T.; Petzold, A.; Wessely, A.; Dippel, E.; Erdmann, M.; Heinzerling, L.; Hohberger, B.; Knorr, H.; Leiter, U.; Meier, F.; et al. Clinical determinants of long-term survival in metastatic uveal melanoma. Cancer Immunol. Immunother. 2022, 71, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.N.; Carvajal, R.D. Tebentafusp for the treatment of HLA-A*02:01-positive adult patients with unresectable or metastatic uveal melanoma. Expert Rev. Anticancer. Ther. 2022, 22, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Gibson, T.; Vigneswaran, G.; Patel, S.; Wheater, M.; Karydis, I.; Gupta, S.; Takhar, A.; Pearce, N.; Ottensmeier, C.; et al. Chemosaturation with percutaneous hepatic perfusion of melphalan for metastatic uveal melanoma. Melanoma. Res. 2022, 32, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.M.L.; Samim, M.; Kapiteijn, E.; Meijer, T.S.; Speetjens, F.M.; Bruning, R.; Schroeder, T.H.; El-Sanosy, S.; Maschke, H.; Wacker, F.K.; et al. Predictive Parameters in Patients Undergoing Percutaneous Hepatic Perfusion with Melphalan for Unresectable Liver Metastases from Uveal Melanoma: A Retrospective Pooled Analysis. Cardiovasc. Interv. Radiol. 2022, 45, 1304–1313. [Google Scholar] [CrossRef]
- Vogel, A.; Ochsenreither, S.; Zager, J.S.; Wacker, F.; Saborowski, A. Chemosaturation for primary and secondary liver malignancies: A comprehensive update of current evidence. Cancer Treat. Rev. 2022, 113, 102501. [Google Scholar] [CrossRef]
- Hughes, M.S.; Zager, J.; Faries, M.; Alexander, H.R.; Royal, R.E.; Wood, B.; Choi, J.; McCluskey, K.; Whitman, E.; Agarwala, S.; et al. Results of a Randomized Controlled Multicenter Phase III Trial of Percutaneous Hepatic Perfusion Compared with Best Available Care for Patients with Melanoma Liver Metastases. Ann. Surg. Oncol. 2016, 23, 1309–1319. [Google Scholar] [CrossRef]
- Zager, J.S.; Orloff, M.M.; Ferrucci, P.F.; Glazer, E.S.; Ejaz, A.; Richtig, E.; Ochsenreither, S.; Lowe, M.C.; Reddy, S.A.; Beasley, G.; et al. FOCUS phase 3 trial results: Percutaneous hepatic perfusion (PHP) with melphalan for patients with ocular melanoma liver metastases (PHP-OCM-301/301A). J. Clin. Oncol. 2022, 40, 9510. [Google Scholar] [CrossRef]
- Tong, T.M.L.; van der Kooij, M.K.; Speetjens, F.M.; van Erkel, A.R.; van der Meer, R.W.; Lutjeboer, J.; van Persijn van Meerten, E.L.; Martini, C.H.; Zoethout, R.W.M.; Tijl, F.G.J.; et al. Combining Hepatic Percutaneous Perfusion with Ipilimumab plus Nivolumab in advanced uveal melanoma (CHOPIN): Study protocol for a phase Ib/randomized phase II trial. Trials 2022, 23, 137. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total N = 5036 (%) | 1989–2004 N = 2209 (%) | 2005–2019 N = 2827 (%) | p-Value | |
|---|---|---|---|---|
| Gender | 0.72 | |||
| Male | 2589 (51) | 1142 (512) | 1447 (51) | |
| Female | 2447 (49) | 1067 (48) | 1380 (49) | |
| Age at diagnosis | <0.001 | |||
| <50 | 857 (17) | 467 (21) | 390 (14) | |
| 50–70 | 2580 (51) | 1085 (49) | 1495 (53) | |
| >70 | 1599 (32) | 657 (30) | 942 (33) | |
| Affected eye | <0.001 * | |||
| Right | 2496 (49.6) | 1077 (49) | 1419 (50) | |
| Left | 2519 (50) | 1113 (50) | 1406 (50) | |
| Unknown | 21 (0.4) | 19 (0.9) | ||
| Diagnosis confirmation | <0.001 | |||
| Clinical and diagnostic assessment | 2220 (44) | 698 (32) | 1522 (54) | |
| Cytological analysis | 24 (0.5) | 9 (0.4) | 15 (0.5) | |
| Histological analysis | 2782 (55) | 1492 (68) | 1290 (46) | |
| Other/unknown | 10 (0.2) | 10 (0.5) | ||
| Tumor location in the eye | 0.006 | |||
| Choroid | 4305 (86) | 1854 (84) | 2451 (87) | |
| Eyeball | 731 (14) | 355 (16) | 376 (13) | |
| TNM/AJCC Stage | <0.001 | |||
| I | 946 (19) | 427 (19) | 519 (18) | |
| II | 2355 (47) | 686 (31) | 1669 (59) | |
| III | 1169 (23) | 727 (33) | 442 (16) | |
| IV | 163 (3) | 120 (5.4) | 43 (1.5) | |
| N/A or unknown | 403 (8) | 249 (11) | 154 (5.4) |
| Total N = 5036 (%) | 1989–2004 N = 2209 (%) | 2005–2019 N = 2827 (%) | p-Value | |
|---|---|---|---|---|
| Surgery | <0.001 | |||
| Yes | 2584 (51) | 1437 (65) | 1147 (41) | |
| No | 2452 (49) | 772 (35) | 1680 (59) | |
| Radiotherapy | <0.001 | |||
| Yes | 2250 (45) | 716 (32) | 1534 (54) | |
| No | 2786 (55) | 1493 (68) | 1293 (46) | |
| Systemic chemotherapy | 0.73 | |||
| Yes | 20 (0.4) | 8 (0.4) | 12 (0.4) | |
| No | 5016 (99.6) | 2201 (99.6) | 2815 (99.6) | |
| Targeted therapy | 0.03 | |||
| Yes | 6 (0.1) | 6 (0.2) | ||
| No | 5030 (99.9) | 2209 (100) | 2821 (99.8) | |
| Other curative treatment * | 0.87 | |||
| Yes | 13 (0.3) | 6 (0.3) | 7 (0.2) | |
| No | 5023 (99.7) | 2203 (99.7) | 2820 (99.8) | |
| Unknown treatment | 0.67 | |||
| Yes | 12 (0.2) | 6 (0.3) | 6 (0.2) | |
| No | 5024 (99.8) | 2203 (99.7) | 2821 (99.8) | |
| Active surveillance | 324 (6.4) | 147 (6.7) | 177 (6.3) |
| Factor | Univariate Analyses | Multivariate Analyses | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age | Cont. | 1.05 | 1.05–1.05 | <0.001 | 1.05 | 1.05–1.06 | <0.001 |
| <50 | Ref. | ||||||
| Age | 50–70 | 2.32 | 2.03–2.65 | <0.001 | |||
| >70 | 5.28 | 4.60–6.06 | <0.001 | ||||
| Gender | Male | Ref. | Ref. | ||||
| Female | 0.91 | 0.84–0.98 | 0.01 | 0.85 | 0.79–0.92 | <0.001 | |
| Tumor stage | I | Ref. | Ref. | ||||
| II | 1.38 | 1.23–1.55 | <0.001 | 1.58 | 1.40–1.79 | <0.001 | |
| III | 2.20 | 1.95–2.49 | <0.001 | 2.07 | 1.82–2.34 | <0.001 | |
| IV | 3.73 | 3.06–4.55 | <0.001 | 2.88 | 2.35–3.54 | <0.001 | |
| M/Unknown | 1.32 | 1.12–1.55 | 0.001 | 1.44 | 1.22–1.71 | <0.001 | |
| Tumor location | Choroid(ref)/ | 1.02 | 0.92–1.14 | 0.69 | 1.02 | 0.91–1.14 | 0.789 |
| Eyeball | |||||||
| Period | 1989–2004 | Ref. | Ref. | ||||
| 2005–2019 | 0.86 | 0.79–0.93 | <0.001 | 0.94 | 0.72–1.26 | 0.15 | |
| Surgery | No (ref)/Yes | 1.88 | 1.74–2.04 | <0.001 | 1.39 | 1.22–1.60 | <0.001 |
| Radiotherapy | No (ref)/Yes | 0.52 | 0.48–0.57 | <0.001 | 0.73 | 0.64–0.83 | <0.001 |
| Other curative treatment | No (ref)/Yes | 3.75 | 2.02–6.99 | <0.001 | 4.29 | 2.30–8.01 | <0.001 |
| Factor | Univariate Analyses | Multivariate Analyses | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age | Cont. | 1.02 | 1.02–1.03 | <0.001 | 1.03 | 1.02–1.04 | <0.001 |
| <50 | Ref. | ||||||
| Age | 50–70 | 1.67 | 1.44–1.95 | <0.001 | |||
| >70 | 2.28 | 1.93–2.68 | <0.001 | ||||
| Gender | Male | Ref. | Ref. | ||||
| Female | 0.88 | 0.80–0.98 | 0.01 | 0.92 | 0.83–1.02 | 0.12 | |
| Tumor stage | I | Ref. | Ref. | ||||
| II | 2.20 | 1.83–2.64 | <0.001 | 2.20 | 1.79–2.64 | <0.001 | |
| III | 3.83 | 3.19–4.59 | <0.001 | 3.15 | 2.62–3.80 | <0.001 | |
| IV | 7.72 | 5.99–9.95 | <0.001 | 5.53 | 4.27–7.17 | <0.001 | |
| M/Unknown | 1.51 | 1.17–1.96 | 0.002 | 1.72 | 1.33–2.23 | <0.001 | |
| Tumor location | Choroid(ref)/ | 1.02 | 0.89–1.18 | 0.74 | 1.02 | 0.88–1.18 | 0.83 |
| Eyeball | |||||||
| Period | 1989–2004 | Ref. | Ref. | ||||
| 2005–2019 | 0.08 | 0.74–0.94 | 0.003 | 1.09 | 0.97–1.22 | 0.13 | |
| Surgery | No (ref)/Yes | 2.74 | 1.74–2.04 | <0.001 | 1.84 | 1.52–2.25 | <0.001 |
| Radiotherapy | No (ref)/Yes | 0.41 | 0.48–0.57 | <0.001 | 0.74 | 0.61–0.90 | 0.002 |
| Other curative treatment | No (ref)/Yes | 5.34 | 2.87–9.95 | <0.001 | 4.46 | 2.38–8.33 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, T.M.L.; Bastiaannet, E.; Speetjens, F.M.; Blank, C.U.; Luyten, G.P.M.; Jager, M.J.; Marinkovic, M.; Vu, T.H.K.; Rasch, C.R.N.; Creutzberg, C.L.; et al. Time Trends in the Treatment and Survival of 5036 Uveal Melanoma Patients in The Netherlands over a 30-Year Period. Cancers 2023, 15, 5419. https://doi.org/10.3390/cancers15225419
Tong TML, Bastiaannet E, Speetjens FM, Blank CU, Luyten GPM, Jager MJ, Marinkovic M, Vu THK, Rasch CRN, Creutzberg CL, et al. Time Trends in the Treatment and Survival of 5036 Uveal Melanoma Patients in The Netherlands over a 30-Year Period. Cancers. 2023; 15(22):5419. https://doi.org/10.3390/cancers15225419
Chicago/Turabian StyleTong, Thaïs M. L., Esther Bastiaannet, Frank M. Speetjens, Christian U. Blank, Gregorius P. M. Luyten, Martine J. Jager, Marina Marinkovic, T. H. Khanh Vu, Coen R. N. Rasch, Carien L. Creutzberg, and et al. 2023. "Time Trends in the Treatment and Survival of 5036 Uveal Melanoma Patients in The Netherlands over a 30-Year Period" Cancers 15, no. 22: 5419. https://doi.org/10.3390/cancers15225419
APA StyleTong, T. M. L., Bastiaannet, E., Speetjens, F. M., Blank, C. U., Luyten, G. P. M., Jager, M. J., Marinkovic, M., Vu, T. H. K., Rasch, C. R. N., Creutzberg, C. L., Beenakker, J.-W. M., Hartgrink, H. H., Bosch, J. J. J., Kiliç, E., Naus, N. C., Yavuzyigitoglu, S., van Rij, C. M., Burgmans, M. C., & Kapiteijn, E. H. W. (2023). Time Trends in the Treatment and Survival of 5036 Uveal Melanoma Patients in The Netherlands over a 30-Year Period. Cancers, 15(22), 5419. https://doi.org/10.3390/cancers15225419