
Extracranial Germ Cell Tumors in Children: Ten Years of Experience in Three Children’s Medical Centers in Shanghai


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Diagnosis and Staging of Patients
2.2. Treatment, Monitoring, and Follow-Up
- PEB regimen: cisplatin, etoposide, bleomycin (one dose of bleomycin per cycle).
- JEB regimen: carboplatin, etoposide, bleomycin.
- BEP regimen: bleomycin, etoposide, cisplatin (3 doses of bleomycin per cycle).
- AVCP/IEV regimen: AVCP, adriamycin, vincristine, cyclophosphamide, cisplatin; IEV, isocyclophosphamide, etoposide, vincristine.
2.3. Statistical Methods
2.4. Ethical Approval
3. Results
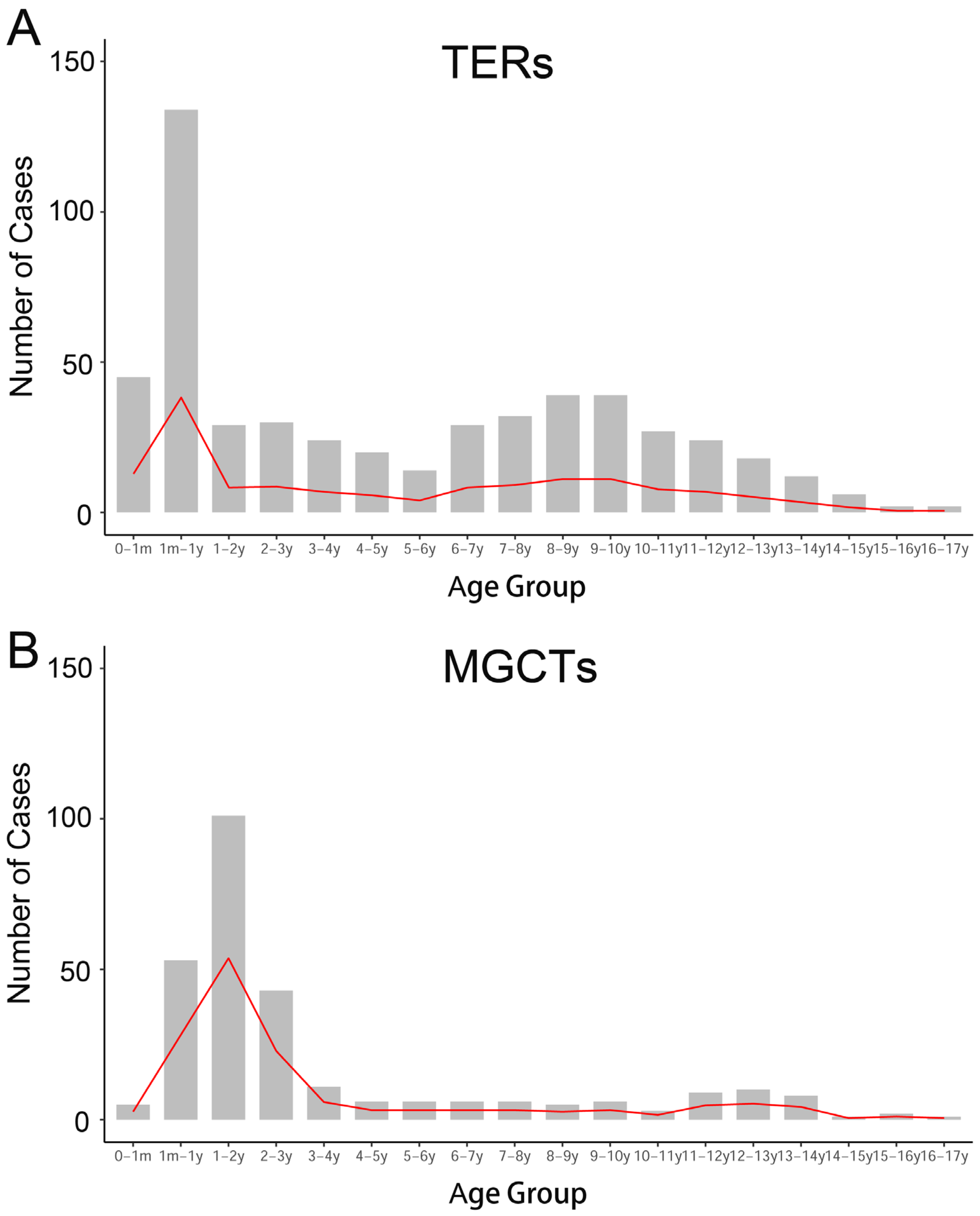
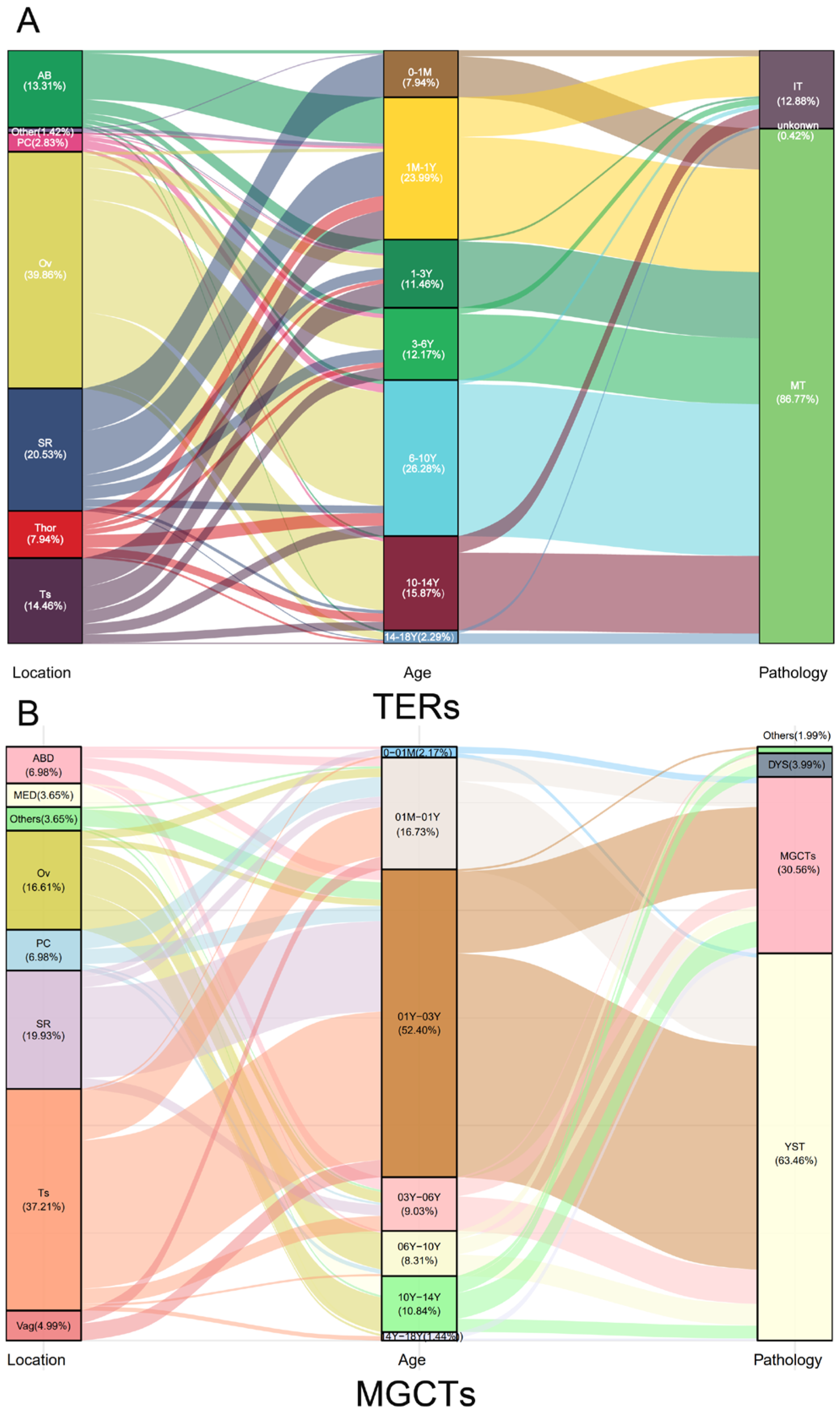
3.1. Clinical Characteristics and Age Distribution by Pathological Type and Anatomical Location
3.2. Tumor Markers in MGCTs
3.3. Survival and Prognostic Indicators of MGCTs
3.4. Chemotherapy for MGCTs
4. Discussion
4.1. Prognosis-Related Factors
4.2. AFP
4.3. Platinum-Based Chemotherapy Regimen
4.4. Age Distribution of GCTs Reflects Pathological Origin
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GCTs | Germ cell tumors |
| TER | Teratoma |
| MGCT | Malignant germ cell tumor |
| AFP | Alpha fetoprotein |
| hCG | human chorionic gonadotropin |
| IT | Immature teratoma |
| MT | Mature teratoma |
| EFS | Event free survival |
| OS | Overall survival |
| PGCs | Primordial germ cells |
| YST | Yolk sac tumor |
| Mix | Mixed germ cell tumor |
| DYS | Dysgerminoma |
| ABD | Abdomen |
| MED | Mediastinum |
| Ov | Ovaries |
| PC | Pelvic cavity |
| SR | Sacrococcygeal region |
| Thor | Thorax |
| Ts | Testicles |
| Vag | Vagina |
References
- Fonseca, A.; Frazier, A.L.; Shaikh, F. Germ Cell Tumors in Adolescents and Young Adults. J. Oncol. Pract. 2019, 15, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, F.; Murray, M.J.; Amatruda, J.F.; Coleman, N.; Nicholson, J.C.; Hale, J.P.; Pashankar, F.; Stoneham, S.J.; Poynter, J.N.; Olson, T.A.; et al. Paediatric Extracranial Germ-Cell Tumours. Lancet Oncol. 2016, 17, e149–e162. [Google Scholar] [CrossRef] [PubMed]
- Oosterhuis, J.W.; Looijenga, L.H.J. Testicular Germ-Cell Tumours in a Broader Perspective. Nat. Rev. Cancer 2005, 5, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Calaminus, G.; Schneider, D.T.; von Schweinitz, D.; Jürgens, H.; Infed, N.; Schönberger, S.; Olson, T.A.; Albers, P.; Vokuhl, C.; Stein, R.; et al. Age-Dependent Presentation and Clinical Course of 1465 Patients Aged 0 to Less than 18 Years with Ovarian or Testicular Germ Cell Tumors; Data of the MAKEI 96 Protocol Revisited in the Light of Prenatal Germ Cell Biology. Cancers 2020, 12, 611. [Google Scholar] [CrossRef] [PubMed]
- Sievers, S.; Alemazkour, K.; Zahn, S.; Perlman, E.J.; Gillis, A.J.M.; Looijenga, L.H.J.; Göbel, U.; Schneider, D.T. IGF2/H19 Imprinting Analysis of Human Germ Cell Tumors (GCTs) Using the Methylation-Sensitive Single-Nucleotide Primer Extension Method Reflects the Origin of GCTs in Different Stages of Primordial Germ Cell Development. Genes. Chromosomes Cancer 2005, 44, 256–264. [Google Scholar] [CrossRef]
- Oosterhuis, J.W.; Looijenga, L.H.J. Human Germ Cell Tumours from a Developmental Perspective. Nat. Rev. Cancer 2019, 19, 522–537. [Google Scholar] [CrossRef]
- Einhorn, L.H.; Donohue, J.P. Improved Chemotherapy in Disseminated Testicular Cancer. J. Urol. 1977, 117, 65–69. [Google Scholar] [CrossRef]
- Peckham, M.J.; Barrett, A.; Liew, K.H.; Horwich, A.; Robinson, B.; Dobbs, H.J.; McElwain, T.J.; Hendry, W.F. The Treatment of Metastatic Germ-Cell Testicular Tumours with Bleomycin, Etoposide and Cis-Platin (BEP). Br. J. Cancer 1983, 47, 613–619. [Google Scholar] [CrossRef]
- Horwich, A.; Sleijfer, D.T.; Fosså, S.D.; Kaye, S.B.; Oliver, R.T.; Cullen, M.H.; Mead, G.M.; de Wit, R.; de Mulder, P.H.; Dearnaley, D.P.; et al. Randomized Trial of Bleomycin, Etoposide, and Cisplatin Compared with Bleomycin, Etoposide, and Carboplatin in Good-Prognosis Metastatic Nonseminomatous Germ Cell Cancer: A Multiinstitutional Medical Research Council/European Organization for Research and Treatment of Cancer Trial. J. Clin. Oncol. 1997, 15, 1844–1852. [Google Scholar] [CrossRef]
- Frazier, A.L.; Hale, J.P.; Rodriguez-Galindo, C.; Dang, H.; Olson, T.; Murray, M.J.; Amatruda, J.F.; Thornton, C.; Arul, G.S.; Billmire, D.; et al. Revised Risk Classification for Pediatric Extracranial Germ Cell Tumors Based on 25 Years of Clinical Trial Data from the United Kingdom and United States. J. Clin. Oncol. 2015, 33, 195–201. [Google Scholar] [CrossRef]
- Hendricks, M.; Cois, A.; Geel, J.; du Plessis, J.; Bassingthwaighte, M.; Naidu, G.; Rowe, B.; Büchner, A.; Omar, F.; Thomas, K.; et al. Malignant Extracranial Germ Cell Tumours: A First National Report by the South African Children’s Cancer Study Group. Pediatr. Blood Cancer 2022, 69, e29543. [Google Scholar] [CrossRef] [PubMed]
- Cushing, B.; Giller, R.; Cullen, J.W.; Marina, N.M.; Lauer, S.J.; Olson, T.A.; Rogers, P.C.; Colombani, P.; Rescorla, F.; Billmire, D.F.; et al. Randomized Comparison of Combination Chemotherapy with Etoposide, Bleomycin, and Either High-Dose or Standard-Dose Cisplatin in Children and Adolescents with High-Risk Malignant Germ Cell Tumors: A Pediatric Intergroup Study--Pediatric Oncology Group 9049 and Children’s Cancer Group 8882. J. Clin. Oncol. 2004, 22, 2691–2700. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.R.; Gray, E.S.; Thornton, C.; Raafat, F.; Robinson, K.; Collins, G.S.; Gornall, P.; Huddart, S.N.; Hale, J.P.; Oakhill, A.; et al. Mature and Immature Extracranial Teratomas in Children: The UK Children’s Cancer Study Group Experience. J. Clin. Oncol. 2008, 26, 3590–3597. [Google Scholar] [CrossRef] [PubMed]
- Olson, T.A.; Murray, M.J.; Rodriguez-Galindo, C.; Nicholson, J.C.; Billmire, D.F.; Krailo, M.D.; Dang, H.M.; Amatruda, J.F.; Thornton, C.M.; Arul, G.S.; et al. Pediatric and Adolescent Extracranial Germ Cell Tumors: The Road to Collaboration. J. Clin. Oncol. 2015, 33, 3018–3028. [Google Scholar] [CrossRef]
- Hulsker, C.C.C.; El Mansori, I.; Fiocco, M.; Zsiros, J.; Wijnen, M.H.W.; Looijenga, L.H.J.; Mavinkurve-Groothuis, A.M.C.; van der Steeg, A.F.W. Treatment and Survival of Malignant Extracranial Germ Cell Tumours in the Paediatric Population: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 3561. [Google Scholar] [CrossRef]
- Grabski, D.F.; Pappo, A.S.; Krasin, M.J.; Davidoff, A.M.; Rao, B.N.; Fernandez-Pineda, I. Long-Term Outcomes of Pediatric and Adolescent Mediastinal Germ Cell Tumors: A Single Pediatric Oncology Institutional Experience. Pediatr. Surg. Int. 2017, 33, 235–244. [Google Scholar] [CrossRef]
- Terenziani, M.; Bisogno, G.; Boldrini, R.; Cecchetto, G.; Conte, M.; Boschetti, L.; De Pasquale, M.D.; Biasoni, D.; Inserra, A.; Siracusa, F.; et al. Malignant Ovarian Germ Cell Tumors in Pediatric Patients: The AIEOP (Associazione Italiana Ematologia Oncologia Pediatrica) Study. Pediatr. Blood Cancer 2017, 64, e26568. [Google Scholar] [CrossRef]
- Necchi, A.; Pond, G.R.; Nicolai, N.; Giannatempo, P.; Raggi, D.; Adra, N.; Hanna, N.H.; Salvioni, R.; Einhorn, L.H.; Albany, C. A Suggested Prognostic Reclassification of Intermediate and Poor-Risk Nonseminomatous Germ Cell Tumors. Clin. Genitourin. Cancer 2017, 15, 306–312.e3. [Google Scholar] [CrossRef]
- Lavi, A.; Winquist, E.; Nair, S.M.; Chin, J.L.; Izawa, J.; Fernandes, R.; Ernst, S.; Power, N.E. Primary Mediastinal Germ Cell Tumors-The University of Western Ontario Experience. Curr. Oncol. 2020, 28, 78–85. [Google Scholar] [CrossRef]
- Schneider, D.T.; Schuster, A.E.; Fritsch, M.K.; Calaminus, G.; Göbel, U.; Harms, D.; Lauer, S.; Olson, T.; Perlman, E.J. Genetic Analysis of Mediastinal Nonseminomatous Germ Cell Tumors in Children and Adolescents. Genes. Chromosomes Cancer 2002, 34, 115–125. [Google Scholar] [CrossRef]
- Mann, J.R.; Raafat, F.; Robinson, K.; Imeson, J.; Gornall, P.; Sokal, M.; Gray, E.; McKeever, P.; Hale, J.; Bailey, S.; et al. The United Kingdom Children’s Cancer Study Group’s Second Germ Cell Tumor Study: Carboplatin, Etoposide, and Bleomycin Are Effective Treatment for Children with Malignant Extracranial Germ Cell Tumors, with Acceptable Toxicity. J. Clin. Oncol. 2000, 18, 3809–3818. [Google Scholar] [CrossRef] [PubMed]
- Depani, S.; Stoneham, S.; Krailo, M.; Xia, C.; Nicholson, J. Results from the UK Children’s Cancer and Leukaemia Group Study of Extracranial Germ Cell Tumours in Children and Adolescents (GCIII). Eur. J. Cancer 2019, 118, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Frazier, A.L.; Rumcheva, P.; Olson, T.; Giller, R.; Cushing, B.; Cullen, J.; Marina, N.; London, W.B. Children’s Oncology Group Application of the Adult International Germ Cell Classification System to Pediatric Malignant Non-Seminomatous Germ Cell Tumors: A Report from the Children’s Oncology Group. Pediatr. Blood Cancer 2008, 50, 746–751. [Google Scholar] [CrossRef] [PubMed]
- International Germ Cell Cancer Collaborative Group. International Germ Cell Consensus Classification: A Prognostic Factor-Based Staging System for Metastatic Germ Cell Cancers. J. Clin. Oncol. 1997, 15, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Taskinen, S.; Fagerholm, R.; Lohi, J.; Taskinen, M. Pediatric Ovarian Neoplastic Tumors: Incidence, Age at Presentation, Tumor Markers and Outcome. Acta Obstet. Gynecol. Scand. 2015, 94, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, F.; Cullen, J.W.; Olson, T.A.; Pashankar, F.; Malogolowkin, M.H.; Amatruda, J.F.; Villaluna, D.; Krailo, M.; Billmire, D.F.; Rescorla, F.J.; et al. Reduced and Compressed Cisplatin-Based Chemotherapy in Children and Adolescents With Intermediate-Risk Extracranial Malignant Germ Cell Tumors: A Report From the Children’s Oncology Group. J. Clin. Oncol. 2017, 35, 1203–1210. [Google Scholar] [CrossRef]
- Pinkerton, C.R.; Pritchard, J.; Spitz, L. High Complete Response Rate in Children with Advanced Germ Cell Tumors Using Cisplatin-Containing Combination Chemotherapy. J. Clin. Oncol. 1986, 4, 194–199. [Google Scholar] [CrossRef]
- Cangir, A.; Smith, J.; van Eys, J. Improved Prognosis in Children with Ovarian Cancers Following Modified VAC (Vincristine Sulfate, Dactinomycin, and Cyclophosphamide) Chemotherapy. Cancer 1978, 42, 1234–1238. [Google Scholar] [CrossRef]
- Marina, N.; Fontanesi, J.; Kun, L.; Rao, B.; Jenkins, J.J.; Thompson, E.I.; Etcubanas, E. Treatment of Childhood Germ Cell Tumors. Review of the St. Jude Experience from 1979 to 1988. Cancer 1992, 70, 2568–2575. [Google Scholar] [CrossRef]
- Zubizarreta, P.; Rossa, A.; Bailez, M.; Gil, S.; Rose, A.; Cacciavillano, W. Malignant Extra-Cranial Germ Cell Tumors in Children and Adolescents. Results Following the Guidelines of SFOP/SFCE 95 Protocol. Medicina 2016, 76, 265–272. [Google Scholar]
- Frazier, A.L.; Stoneham, S.; Rodriguez-Galindo, C.; Dang, H.; Xia, C.; Olson, T.A.; Murray, M.J.; Amatruda, J.F.; Shaikh, F.; Pashankar, F.; et al. Comparison of Carboplatin versus Cisplatin in the Treatment of Paediatric Extracranial Malignant Germ Cell Tumours: A Report of the Malignant Germ Cell International Consortium. Eur. J. Cancer 2018, 98, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Billmire, D.F.; Cullen, J.W.; Rescorla, F.J.; Davis, M.; Schlatter, M.G.; Olson, T.A.; Malogolowkin, M.H.; Pashankar, F.; Villaluna, D.; Krailo, M.; et al. Surveillance after Initial Surgery for Pediatric and Adolescent Girls with Stage I Ovarian Germ Cell Tumors: Report from the Children’s Oncology Group. J. Clin. Oncol. 2014, 32, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Pavone, R.; Pacquement, H.; Pasquet, M.; Sudour-Bonnange, H.; Hameury, F.; Sarnacki, S.; Chastagner, P.; Faure-Conter, C.; Poirée, M.; Taque, S.; et al. Childhood Ovarian Nonseminomatous Germ Cell Tumors: A Highly Curable Disease with Few Long-Term Treatment-Related Toxicities-Results of the French TGM95 Study. Int. J. Cancer 2021, 149, 1705–1712. [Google Scholar] [CrossRef]
- Kaatsch, P.; Häfner, C.; Calaminus, G.; Blettner, M.; Tulla, M. Pediatric Germ Cell Tumors from 1987 to 2011: Incidence Rates, Time Trends, and Survival. Pediatrics 2015, 135, e136–e143. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.T.; Calaminus, G.; Koch, S.; Teske, C.; Schmidt, P.; Haas, R.J.; Harms, D.; Göbel, U. Epidemiologic Analysis of 1,442 Children and Adolescents Registered in the German Germ Cell Tumor Protocols. Pediatr. Blood Cancer 2004, 42, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Jn, P.; Jf, A.; Ja, R. Trends in Incidence and Survival of Pediatric and Adolescent Patients with Germ Cell Tumors in the United States, 1975 to 2006. Cancer 2010, 116, 4882–4891. [Google Scholar] [CrossRef]
- Runyan, C.; Gu, Y.; Shoemaker, A.; Looijenga, L.; Wylie, C. The Distribution and Behavior of Extragonadal Primordial Germ Cells in Bax Mutant Mice Suggest a Novel Origin for Sacrococcygeal Germ Cell Tumors. Int. J. Dev. Biol. 2008, 52, 333–344. [Google Scholar] [CrossRef]
- Suita, S.; Shono, K.; Tajiri, T.; Takamatsu, T.; Mizote, H.; Nagasaki, A.; Inomata, Y.; Hara, T.; Okamura, J.; Miyazaki, S.; et al. Malignant Germ Cell Tumors: Clinical Characteristics, Treatment, and Outcome. A Report from the Study Group for Pediatric Solid Malignant Tumors in the Kyushu Area, Japan. J. Pediatr. Surg. 2002, 37, 1703–1706. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Ters (n = 706) | MGCTs (n = 301) | ||
|---|---|---|---|
| Gender | Gender | ||
| Male/Female | 1/2.66 | Male/Female | 1.13/1 |
| Age (M) | 68.40 (3 day–202 month) | Age (M) | 41 (3 day–213 month) |
| Primary site | Proportion (number) | Primary site | Proportion (number) |
| ovary | 39.86% (281) | testis | 37.21%(112) |
| sacrococcygeal | 20.53% (145) | ovary | 16.61% (50) |
| testis | 14.46% (102) | sacrococcygeal | 19.93% (60) |
| abdomen | 13.05% (92) | abdomen | 6.98% (21) |
| pelvic cavity | 2.83% (20) | pelvic cavity | 6.98% (21) |
| thorax | 7.94% (56) | Thorax(mediastinum) | 3.65% (11) |
| Others (nasopharynx, neck, hip, thymus, femur) | 0.008% (6) | Vagina | 4.99% (15) |
| unknown | 0.005% (4) | Others (orbit, upper lip, etc.) | 2.66% (8) |
| Pathology | Proportion (number) | unknown | 0.10% (3) |
| Mature teratoma | 86.77% (612) | ||
| Immature teratoma | 12.88% (91) | Pathology | |
| Unknown | 0.42% (3) | Yolk sac tumor | 63.45% (191) |
| Mixed germ cell tumor | 30.56% (92) | ||
| dysgerminoma | 3.99% (12) | ||
| gonadoblastoma | 0.10% (3) | ||
| seminoma | 0.33% (1) | ||
| Embryonal carcinoma | 0.33% (1) | ||
| Choriocarcinoma | 0.33% (1) | ||
| Staging | |||
| I | 37.21 (112) | ||
| II | 11.63 (35) | ||
| III | 27.57 (83) | ||
| IV | 23.59 (71) |
| N | AFP (No./%) | CMH Statistics | p | ||||
|---|---|---|---|---|---|---|---|
| S0 | S1 | S2 | S3 | ||||
| Total | 217 | 24/11.06 | 37/17.05 | 66/30.41 | 91/41.94 | ||
| Pathology | 81.32 | <0.0001 | |||||
| Yolk sac tumor | 137 | 4/2.92 | 25/18.25 | 53/38.69 | 55/40.15 | ||
| Mixed germ cell tumour | 67 | 8/11.94 | 11/16.42 | 12/17.91 | 36/53.73 | ||
| Choriocarcinoma | 1 | 1 | 0 | 0 | 0 | ||
| Embryonal carcinoma | 1 | 0 | 0 | 1 | 0 | ||
| Dysgerminoma | 11 | 11/4.72 | 0 | 0 | 0 | ||
| Seminoma | 1 | 1/0.43 | 0 | 0 | 0 | ||
| Staging | 33.21 | <0.0001 | |||||
| Ⅰ | 70 | 6/8.57 | 22/31.43 | 33/47.14 | 9/12.86 | ||
| Ⅱ | 25 | 7/28.00 | 6/24.00 | 8/32.00 | 6/24.00 | ||
| Ⅲ | 59 | 9/15.25 | 4/6.78 | 18/30.51 | 32/54.24 | ||
| Ⅳ | 58 | 2/3.45 | 5/13.79 | 6/10.34 | 45/77.59 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, S.; Dong, K.; Li, K.; Liu, J.; Du, X.; Huang, C.; Jiao, Y.; Han, Y.; Yang, J.; Liao, X.; et al. Extracranial Germ Cell Tumors in Children: Ten Years of Experience in Three Children’s Medical Centers in Shanghai. Cancers 2023, 15, 5412. https://doi.org/10.3390/cancers15225412
Jiang S, Dong K, Li K, Liu J, Du X, Huang C, Jiao Y, Han Y, Yang J, Liao X, et al. Extracranial Germ Cell Tumors in Children: Ten Years of Experience in Three Children’s Medical Centers in Shanghai. Cancers. 2023; 15(22):5412. https://doi.org/10.3390/cancers15225412
Chicago/Turabian StyleJiang, Shayi, Kuiran Dong, Kai Li, Jiangbin Liu, Xin Du, Can Huang, Yangyang Jiao, Yali Han, Jingwei Yang, Xuelian Liao, and et al. 2023. "Extracranial Germ Cell Tumors in Children: Ten Years of Experience in Three Children’s Medical Centers in Shanghai" Cancers 15, no. 22: 5412. https://doi.org/10.3390/cancers15225412
APA StyleJiang, S., Dong, K., Li, K., Liu, J., Du, X., Huang, C., Jiao, Y., Han, Y., Yang, J., Liao, X., Li, Y., Zhang, T., Li, S., Lv, Z., & Gao, Y. (2023). Extracranial Germ Cell Tumors in Children: Ten Years of Experience in Three Children’s Medical Centers in Shanghai. Cancers, 15(22), 5412. https://doi.org/10.3390/cancers15225412